

INTRODUCTION
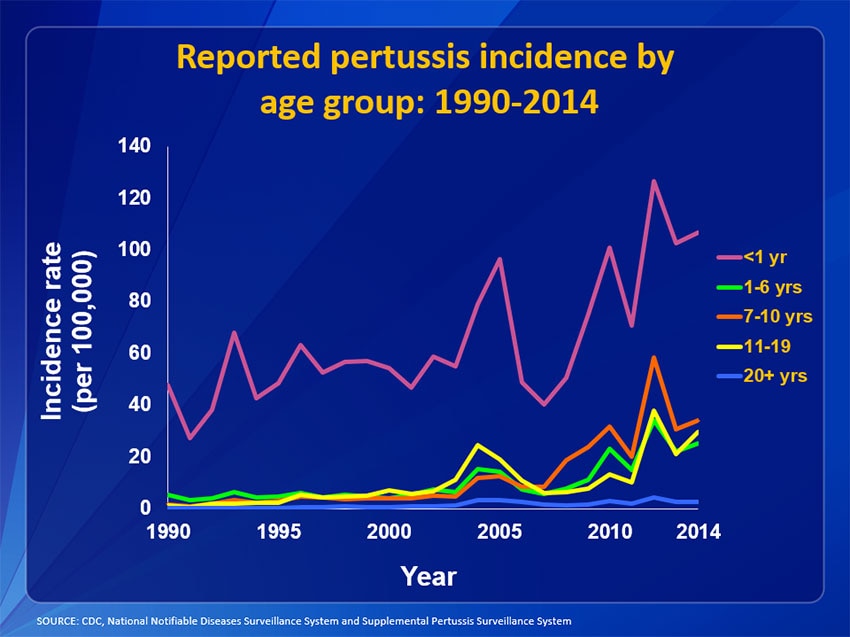
Pertussis is a highly communicable respiratory illness caused by the Bordetella pertussis bacterium, characterized by a prolonged paroxysmal cough and inspiratory whoop. After the introduction of the pertussis vaccine, the incidence of pertussis in the USA dropped substantially (from 150 cases per 100 000 persons between 1940 and 1945 to a low of approximately 1 per 100 000 persons in 1980–1990) [Reference Atkinson, Wolfe and Hamborsky1]. However, recent surveillance statistics indicate a resurgence of pertussis in communities nationwide. In 2012, more than 48 000 cases of pertussis (incidence: 15·4 per 100 000 persons) were reported to the Centers for Disease Control and Prevention (CDC), an increase from 2011 (incidence: 6·1 per 100 000 population) [Reference Adams2]. Infants younger than 12 months of age had the highest incidence (126·7 cases per 100 000 persons), followed by adolescents aged 11–14 years (59·2 per 100 000). Despite the high incidence of pertussis in infants and children, more than half of all reported cases in 2012 occurred in persons aged 11 years and older [3].
Research has shown that the clinical presentation of pertussis in adolescents and adults is characterized by symptoms including paroxysm, whoop, posttussive apnea, and posttussive vomiting [Reference Long4]. Among adolescents and adults, complications such as pneumonia, fainting, urinary incontinence, and hospitalization have been shown to increase with age [Reference De Serres5]. Furthermore, costs associated with pertussis in adults are substantial, with previous studies estimating costs per pertussis episode among patients aged 50 years and older in the USA to be between $1800 and $14 500, depending on the treatment setting [Reference McGuiness6].
As pertussis is an infection of the respiratory tract, patients with chronic respiratory conditions such as asthma or chronic obstructive pulmonary disease (COPD) may be at increased risk for pertussis. There is some evidence showing that patients with asthma have a higher incidence of pertussis than patients without asthma [Reference De Serres5, Reference Capili7, Reference Liu8]. In addition, a small case–control study (N = 90) found that anti-pertussis toxin immunoglobulin G seropositivity was significantly higher in patients with COPD than in control patients [Reference Hashemi9]; however, the burden of pertussis in patients with COPD requires further characterization. To bridge this research gap and provide important information on the burden of pertussis in potential high-risk groups, the objective of this study was to generate US-specific data on the incidence and economic burden of diagnosed pertussis among adolescents and adults with a pre-existing diagnosis of asthma or COPD.
METHODS
Study design and data source
A retrospective cohort study using US administrative claims (i.e., inpatient, outpatient, and pharmacy claims) was conducted. The data sources were the MarketScan Commercial Claims and Encounters and Medicare Supplemental and Coordination of Benefits (1/2006–6/2014) and Medicaid Multi-State (1/2007–12/2013) databases. The authors’ data access was restricted to the HIPAA (Health Insurance Portability and Accountability Act)-compliant de-identified data.
Patient selection criteria and study cohorts
Patients were selected for the study cohorts based on standard claims-based algorithms. Specifically, patients were identified for inclusion in the analysis if they had a primary or secondary diagnosis of pertussis (defined by International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes 033·0x, 033·9x, and 484·3x [Reference McGuiness6]). To allow for inclusion of health care resources related to the workup of the pertussis diagnosis (e.g., initial office visits and laboratory tests), the index date was defined as the date of the first observed pertussis diagnosis minus 15 days. Patients were required to have at least 6 months of continuous enrollment before and after the index date and to be aged 11 years or older.
The pre-existing COPD and pertussis (COPD + PERT) cohort included patients with at least two claims (i.e., inpatient, emergency department, or outpatient) spaced at least 14 days apart with a COPD diagnosis (ICD-9-CM codes 491.xx, 492.xx, or 496.xx) and at least one COPD diagnosis in the 6 months before the index date. A previous study required multiple COPD claims to define exposure status [Reference Mapel10], and the specificity and sensitivity of multiple claims with COPD diagnoses have been estimated at approximately 80% [Reference Gershon11, Reference Ajmera12]. The pre-existing asthma and pertussis (ASTHMA + PERT) cohort included patients with one inpatient or emergency department visit with a diagnosis of asthma or two outpatient visits with a diagnosis of asthma and at least one prescription for an asthma medication, with the first observed asthma diagnosis occurring in the 6 months before the index date. A variety of algorithms have been used to identify patients with asthma in health care claims data (e.g., [Reference Yang13, Reference Dombkowski, Wasilevich and Lyon-Callo14]); the algorithm used in this analysis was based on common themes of identifying patients with encounters for severe asthmatic events (inpatient or emergency department visits) or encounters for managing asthma (outpatient visits plus medication). All qualified patients identified from the database and meeting the study eligibility criteria were included in the analysis. To control for differences in underlying demographic and clinical characteristics, patients with pre-existing COPD or asthma and pertussis were matched 1:1 to patients with pertussis and no pre-existing COPD or asthma using direct covariate matching. The covariates included were patient age, sex, insurance payer, categorical Charlson Comorbidity Index (CCI) score excluding COPD (i.e., 0, 1, 2, and ⩾3), year of pertussis diagnosis, and costs in the 6 months pre-index date by quartile.
Study measures
All-cause health care costs were calculated for three time periods: 45 days pre-index date and 45 days post-index date; 3 months pre-index date and 3 months post-index date; and 6 months pre-index date and 6 months post-index date. Pertussis-related health care costs were calculated for the post-index date time periods only. All-cause health care costs included all medical and pharmacy costs, regardless of the corresponding diagnoses or prescriptions. Pertussis-related health care costs included inpatient or emergency department visits with a primary diagnosis of pertussis; outpatient visits with a primary or secondary diagnosis of pertussis; and pharmacy claims for azithromycin, clarithromycin, erythromycin, or trimethoprim-sulfamethoxazole. Cost analyses were conducted from the total burden of disease perspective and included all payments made by the insurance provider, third parties (e.g., Medicare), and the patient. Cost data were adjusted to 2014 US dollars using the medical care component of the US Consumer Price Index [15].
Data analyses
The incidence of diagnosed pertussis among patients with pre-existing COPD and among patients with pre-existing asthma, as well as among patients without pre-existing conditions, was calculated. Person-time (reported as person-years) accumulated during the follow-up period served as the denominator in assessing the incidence rate. The follow-up period started on the enrollment date of patients without pre-existing asthma or COPD or the exposure index date among patients with pre-existing asthma or pre-existing COPD and ended with the pertussis index date among patients with pertussis, or the end of enrollment or end of the study period (whichever came first) among patients who were not diagnosed with pertussis. Estimation of 95% confidence intervals (CIs) was based on the Poisson distribution [Reference Buchan16, Reference Ulm17]. The incidence of diagnosed pertussis was calculated for patients with and without pre-existing asthma or COPD and was stratified by age. In addition, the relative risk of diagnosed pertussis among patients with each pre-existing condition compared with those without pre-existing conditions was computed and stratified by age.
Regression models were estimated to determine the adjusted excess costs during the 45-day and 3- and 6-month periods after the study index date. Adjusted health care costs were reported for each post-index date time period using a generalized estimating equation model with a log-link for the mean and a γ distribution for the residuals. The covariates included in the model were pre-existing COPD or asthma, sex, geographic region, health plan type, payer type, CCI score, year of diagnosis, age, and baseline costs. Missing values for certain variables (e.g., region) were treated as a separate category but were not excluded from the analysis. From the model estimations, predicted costs were generated and reported for the COPD + PERT cohort, the ASTHMA + PERT cohort, and the respective matched cohorts. Adjusted excess health care costs were reported as the adjusted costs for the COPD + PERT cohort or the ASTHMA + PERT cohort minus the adjusted costs for the respective matched cohort.
RESULTS
Incidence of diagnosed pertussis
Table 1 presents the incidence of diagnosed pertussis in the MarketScan database population. The overall incidence of pertussis among patients with pre-existing COPD was 0·176 (95% CI 0·166–0·185) per 1000 person-years (relative risk, 2·533 (95% CI 2·396–2·678) vs. patients without asthma or COPD). Among patients with pre-existing COPD, the relative risk of pertussis was highest among patients aged 19–64 years (relative risk, 3·588 (95% CI 3·353–3·840)). The overall incidence of pertussis among patients with pre-existing asthma was 0·274 (95% CI 0·265–0·285) per 1000 person-years (relative risk, 3·959 (95% CI 3·808–4·115) vs. patients without asthma or COPD). Among patients with pre-existing asthma, the relative risk of pertussis was also highest among patients aged 19–64 years (relative risk 4·060 (95% CI 3·861–4·269)).
Incidence of diagnosed pertussis among adolescents and adults with pre-existing COPD or asthma

CI, confidence interval; COPD, chronic obstructive pulmonary disease.
Sample characteristics
A total of 441 patients who qualified for the cohort with pre-existing COPD and pertussis (i.e., the COPD + PERT cohort) and 1157 patients who qualified for cohort with pre-existing asthma and pertussis (i.e., the ASTHMA + PERT cohort) were identified. Matching resulted in 343 patients in the COPD + PERT cohort and 1041 patients in the ASTHMA + PERT cohort. Table 2 presents the sample characteristics.
Sample characteristics
COPD, chronic obstructive pulmonary disease; s.d., standard deviation.
a Charlson comorbidities measured in the 6-month pre-study index date period, and excluding COPD. The comorbidities presented affected more than 7% of any cohort or more than 2% of all cohorts. The comorbidities not presented included congestive heart failure, myocardial infarction, dementia, connective tissue disease, ulcer disease, use of warfarin, hemiplegia, moderate or severe renal disease, diabetes with end-organ damage, mild liver disease, metastatic cancer, and AIDS.
The mean (standard deviation (s.d.)) age of the COPD + PERT cohort was 53·2 (18·4) years, and approximately two-thirds of this cohort was female. The mean (s.d.) CCI score was 1·7 (2·2) for the COPD + PERT cohort vs. 1·8 (2·4) for the matched cohort. For both the COPD + PERT cohort and the matched cohort, the highest proportion of pertussis diagnoses occurred in 2012. Mean (s.d.) costs during the 6-month pre-index date period were slightly higher for the COPD + PERT cohort ($12 230 ($34 058)) than for the matched cohort ($10 413 ($22 142)).
The mean (s.d.) age of the ASTHMA + PERT cohort was 32·1 (19·5) years, and approximately two-thirds of this cohort was female. The mean (s.d.) CCI score was 0·6 (1·3) for patients with pre-existing asthma and pertussis vs. 0·7 (1·4) for matched patients. For both the ASTHMA + PERT cohort and the matched cohort, the highest proportion of pertussis diagnoses occurred in 2012. Mean (s.d.) costs during the 6-month pre-index date period were slightly higher among the ASTHMA + PERT cohort ($7360 ($14 464)) than for the matched cohort ($6095 ($11 052)).
Hospitalizations
During the 45 days, 3 months and 6 months post-index date, the difference in the percentage of patients with at least one all-cause hospitalization was greater in the COPD + PERT cohort than in the matched cohort relative to the respective periods pre-index date (Table 3). Likewise, during all three post-index date periods, the differences in the percentage of patients with at least one all-cause hospitalization were greater in the ASTHMA + PERT cohort than in the matched cohort relative to the respective periods pre-index date.
Difference in likelihood of hospitalizations after pertussis diagnosis, by time period and cohort
COPD, chronic obstructive pulmonary disease.
a All-cause hospitalizations reflect the difference in the percentage of patients with ⩾1 hospitalization during the 45-day, 3-month, and 6-month periods post-pertussis index date, respectively, relative to the 45-day, 3-month, and 6-month periods pre-pertussis index date.
b Pertussis-related hospitalizations reflect the percentage of patients with ⩾1 hospitalization related to pertussis in the 45 days, 3 months, and 6 months post-pertussis index date.
Similar patterns were observed for pertussis-related hospitalization patterns: across all three post-index date periods, the percentage of patients with at least one pertussis-related hospitalization were greater in the COPD + PERT and ASTHMA + PERT cohorts than in the respective matched cohorts.
Unadjusted costs
Unadjusted all-cause costs
During the 45 days post-index date, the COPD + PERT cohort accrued $4150 more than they accrued during the 45 days pre-index date, whereas the matched-control cohort accrued $1201 more during the 45 days post-index date, resulting in an excess cost of pertussis in patients with COPD of $2950 (P = 0·009) compared with patients with pertussis without COPD (Table 4). For the 3-month and 6-month periods, the excess costs of pertussis in the COPD + PERT cohort compared with the matched-control cohort were $3499 (P = 0·026) and $5657 (P = 0·012), respectively. During the 45 days post-index date, the ASTHMA + PERT cohort accrued $1746 more than they accrued during the 45 days pre-index date, whereas the matched-control cohort accrued $1084 more during the 45 days post-index date, resulting in an excess cost of pertussis in patients with asthma compared with patients with pertussis without asthma of $662 (P = 0·079). For the 3- and 6-month periods, the excess costs of pertussis in the ASTHMA + PERT cohort compared with the matched-control cohort were $591 (P = 0·244) and $1386 (P = 0·129), respectively.
Unadjusted mean difference in all-cause and pertussis-related costs, by time period and cohort

COPD, chronic obstructive pulmonary disease.
a Due to rounding, the difference may not correspond to the difference between the individual values presented for the COPD + pertussis cohort and the matched cohort.
b All-cause costs reflect the difference in costs (i.e., all medical and pharmacy costs, regardless of the corresponding diagnoses or prescriptions) incurred during the 45-day, 3-month, and 6-month periods post-pertussis index date (including pertussis-related costs), respectively, relative to the 45-day, 3-month, and 6-month periods pre-pertussis index date.
c Pertussis-related costs reflect costs associated with pertussis in the 45 days, 3 months, and 6 months post-pertussis index date.
Unadjusted pertussis-related costs
Compared with the matched cohort, the COPD + PERT cohort accrued $956 more in pertussis-related unadjusted costs during the 45 days post-index date (P = 0·128), $972 more during the 3 months post-index date (P = 0·121), and $979 more during the 6 months post-index date (P = 0·119) (Table 4). Compared with the matched cohort, the ASTHMA + PERT cohort accrued $175 more in pertussis-related unadjusted costs during the 45 days post-index date (P = 0·032), $188 more during the 3 months post-index date (P = 0·021), and $197 more during the 6 months post-index date (P = 0·016).
Adjusted costs
Adjusted all-cause costs
In the 45-day period after the index date, the COPD + PERT cohort accrued $4751 in all-cause adjusted health care costs, whereas the matched cohort accrued $1057 in all-cause adjusted health care costs. This resulted in $3694 more in all-cause adjusted costs associated with the COPD + PERT cohort compared with the matched cohort (P < 0·0001) (Fig. 1). The difference in all-cause adjusted costs of the COPD + PERT cohort vs. the matched cohort increased to $4173 in the 3 months post-index date and to $6154 in the 6 months post-index date (both P < 0·0001). The difference in all-cause adjusted costs between the COPD + PERT cohort vs. the matched cohort was found to increase with age during the 45-day post-index date period ($1474 among patients aged 11–18 years, $3356 among patients aged 19–64 years, and $5295 among patients aged 65 + years; all P < 0·0001). The trend of increasing differences in all-cause adjusted costs with increasing patient age continued during the 3-month period ($1643 among patients aged 11–18 years, $4092 among patients aged 19–64 years, and $5184 among patients aged 65 + years; all P < 0·0001) and the 6-month period ($2276 among patients aged 11–18 years, $6110 among patients aged 19–64 years, and $7491 among patients aged 65 + years; all P < 0·0001).
Adjusted all-cause health care costs for patients with pre-existing COPD and pertussis and matched patients with pertussis only in the 45 days, 3 months, and 6 months following the index date. COPD = chronic obstructive pulmonary disease. *P < 0·0001 for all differences.

In the 45-day period after the index date, the ASTHMA + PERT cohort accrued $2007 in all-cause adjusted health care costs, whereas the matched cohort accrued $814 in all-cause adjusted health care costs. This resulted in $1193 more in all-cause adjusted costs associated with the ASTHMA + PERT cohort compared with the matched cohort (P < 0·0001) (Fig. 2). The difference in all-cause adjusted costs between the ASTHMA + PERT cohort vs. the matched cohort increased slightly to $1301 in the 3 months post-index date and to $1639 in the 6 months post-index date (both P < 0·0001). The difference in all-cause adjusted costs between the ASTHMA + PERT cohort vs. the matched cohort was found to increase with increasing patient age during the 45-day post-index date period ($746 among patients aged 11–18 years, $1460 among patients aged 19–64 years, and $2510 among patients aged 65 + years; all P < 0·0001). The trend of increasing differences in all-cause adjusted costs with increasing patient age continued during the 3-month period ($794 among patients aged 11–18 years, $1632 among patients aged 19–64 years, and $2436 among patients aged 65 + years; all P < 0·0001) and the 6-month period ($1021 among patients aged 11–18 years, $2087 among patients aged 19–64 years, and $2475 among patients aged 65 + years; all P < 0·0001).
Adjusted all-cause health care costs for patients with pre-existing asthma and pertussis and matched patients with pertussis only in the 45 days, 3 months, and 6 months following the index date. *P < 0·0001 for all differences.

Adjusted pertussis-related costs
The difference in pertussis-related adjusted costs between the COPD + PERT cohort and the matched cohort was $369 in the 45-day period after the index date, $435 during the 3-month period, and $463 during the 6-month period (all P < 0·0001) (Fig. 3). The difference in pertussis-related adjusted costs between the COPD + PERT cohort vs. the matched cohort during the 45-day period was found to increase with increasing patient age ($264 among patients aged 11–18 years, $361 among patients 19–64 years, and $423 among patients aged 65 + years; all P < 0·01). The trend of increasing differences in pertussis-related adjusted costs with age continued during the 3-month period ($281 among patients aged 11–18 years, $428 among patients aged 19–64 years, and $500 among patients aged 65 + years; all P < 0·01) and the 6-month period ($285 among patients aged 11–18 years, $459 among patients aged 19–64 years, and $528 among patients aged 65 + years; all P < 0·01).
Adjusted pertussis-related health care costs for patients with pre-existing COPD and pertussis and matched patients with pertussis only in the 45 days, 3 months, and 6 months following the index date. COPD = chronic obstructive pulmonary disease. *P < 0·0001 for all differences.

The difference in pertussis-related adjusted costs between the ASTHMA + PERT cohort and the matched cohort was $230 in the 45-day period after the index date, $241 during the 3-month period, and $251 during the 6-month period (all P < 0·0001) (Fig. 4). The differences in pertussis-related adjusted costs between the ASTHMA + PERT cohort vs. the matched cohort were similar across age groups during the 45-day period ($183 among patients aged 11–18 years, $267 among patients aged 19–64 years, and $255 among patients aged 65 + years; all P < 0·0001). Similar differences in pertussis-related adjusted costs between the ASTHMA + PERT cohort vs. the matched cohort were also observed across age groups during the 3-month period ($193 among patients aged 11–18 years, $278 among patients aged 19–64 years, and $266 among patients aged 65 + years; all P < 0·0001) and during the 6-month period ($204 among patients aged 11–18 years, $289 among patients aged 19–64 years, and $276 among patients aged 65 + years; all P < 0·0001).
Adjusted pertussis-related health care costs for patients with pre-existing asthma and pertussis and matched patients with pertussis only in the 45 days, 3 months, and 6 months following the index date. *P < 0·0001 for all differences.

DISCUSSION
This retrospective database analysis compared patients with diagnosed pertussis and pre-existing asthma or COPD with matched patients who had diagnosed pertussis but no pre-existing asthma or COPD, and reported on the incidence of diagnosed pertussis as well as all-cause and pertussis-related costs. The results for the 2006–2014 study period may be generalizable to a large insured US population. The observed incidence rates varied considerably across age groups, with the highest incidence occurring among adolescents aged 11–18 years in both the PERT + COPD and the PERT + ASTHMA populations. Similar variations in incidence by age have been reported by the CDC during this time frame [18], but, to our knowledge, there is limited evidence on the incidence of pertussis among individuals with pre-existing asthma or COPD.
Respiratory infections such as pertussis are associated with an increase in acute exacerbations in patients with asthma and COPD [Reference Kumar and Grayson19–Reference De Serres22]. Furthermore, some research has suggested that patients with asthma or COPD may be at increased risk for pertussis compared with patients without either of these conditions [Reference De Serres5, Reference Capili7, Reference Liu8, Reference Hashemi9]. Our study builds upon the current literature and shows that, regardless of the age group, the incidence of ICD-9-CM-diagnosed pertussis was higher among patients with a diagnosis of COPD or asthma compared with patients without either of these conditions.
Additionally, limited published data exist regarding costs associated with pertussis in adolescents and adults. A small US survey study evaluating the economic impact of pertussis among adolescents found societal costs, including direct medical and indirect costs, to be in excess of $315 per affected household [Reference Varan23]. Further, a study by McGuiness and colleagues [Reference McGuiness6] evaluated US patients with pertussis aged 50 years and older and reported on inpatient and outpatient health care costs using a retrospective database. Their study found that patients with pertussis accrued between $1835 and $14 428 in all-cause costs, depending on whether they received treatment in the inpatient or outpatient setting. Results from this study are not directly comparable with our analysis, which included adolescents and adults of all ages and stratified patients with pertussis by COPD and asthma status. Nevertheless, average adjusted per-patient all-cause costs in our analysis were within the range of all-cause costs identified by McGuiness and colleagues [Reference McGuiness6], ranging from $3143 for patients with asthma to $6478 for patients with COPD in the 6 months post-index date.
Our study supports previous findings that pertussis may be associated with worsening COPD and asthma symptoms, thereby increasing the overall economic burden of the diseases. Among patients with pre-existing COPD in particular, all-cause costs increased with time following a diagnosis of pertussis, whereas all-cause costs decreased over time for matched patients without COPD. These findings suggest that patients with pre-existing COPD can experience negative consequences from pertussis for at least 6 months. Specifically, matched patients without COPD accrued $1057 in adjusted costs (while controlling for costs in the pre-index date period) in the 45 days after the index date. However, adjusted costs for matched patients without COPD were found to decrease over time, with matched patients without COPD having just $324 in adjusted costs in the 6 months after the index date. This indicates that patients without COPD did not experience lingering symptoms and that the pertussis diagnosis did not have long-term health consequences for patients without pre-existing asthma or COPD. Contrasting this with patients with COPD, the burden of pertussis increased over time even after controlling for baseline health care costs, from adjusted costs of $4751 in the 45-day post-index date to $6478 in the 6-month post-index date, indicating that patients with pertussis and COPD experienced longer term negative consequences from pertussis compared to patients with pertussis without COPD. This conclusion is further supported by the fact that pertussis-related spending remained constant between the 45-day and 6-month period for patients with COPD (i.e., adjusted pertussis-related costs of $1083 in the 45-day period and $1158 in the 6-month period). Thus, patients were not accruing additional pertussis-related care after the 45-day post-index date period, and all subsequent health care expenditures causing the increase in adjusted all-cause costs over time were not directly related to the treatment of pertussis but rather were associated with increased health care costs due to other concomitant conditions. Similar findings were also observed for asthma patients with pertussis; however, the economic consequences were not as large (range: adjusted all-cause costs of $2007 in the 45-day post-study index period to adjusted all-cause costs of $3143 in the 6-month post-study index period).
Tetanus, diphtheria, and acellular pertussis (Tdap) vaccination remains the most effective strategy against infection and in reducing disease severity among adolescents and adults. Protective benefits of Tdap vaccination have ranged from an estimated effectiveness of 53·0% among patients aged 11 years or older in the community setting [Reference Baxter24] to an estimated efficacy of 92% among adults participating in the Adult Pertussis Trial [Reference Ward25]; however, recent research has found that this protection from pertussis wanes over time [Reference Acosta26, Reference Koepke27]. Although there are no studies specifically examining Tdap vaccine efficacy among patients with COPD or asthma, whole-cell pertussis vaccination has been shown to have a protective effect against allergic asthma exacerbations [Reference Ennis, Cassidy and Mahon28]. In addition, other vaccines, such as the influenza vaccine, are associated with a reduction in acute exacerbations among patients with COPD [Reference Varkey, Varkey and Varkey29]. Therefore, incorporating compliance with the Advisory Committee on Immunization Practice (ACIP) Tdap recommendations into COPD and asthma management plans may aid in reducing morbidity and mortality among these patients. The ACIP currently recommends one dose of Tdap vaccine for non-pregnant adolescents (preferred at ages 11 or 12 years) and adults [30]. However, compliance in the general adult population is low; in 2014, an estimated 20·1% of adults had received the Tdap vaccine in the previous 9 years [Reference Williams31]. Given the lack of information on the effectiveness of Tdap in patients with COPD and asthma, further research on the measurable effect of vaccination on infection and disease severity is warranted.
This study has several limitations common to retrospective database analyses, including the potential for coding errors in the administrative claims data and for selection bias. In particular, some of the 27 adolescent patients (aged 11–18 years) in the study sample who had COPD may have been subject to diagnostic coding errors. Although observable measures were used to alleviate the effect of selection bias by conducting direct covariate matching, unmeasured or unknown factors may have affected the outcome differently. Moreover, data on laboratory-confirmed pertussis are unavailable in the MarketScan databases; therefore, pertussis cases were identified using diagnosis codes, which likely resulted in an underestimation of the number of patients with pertussis, especially in adults. Similarly, spirometry testing results were not available, and identification of COPD and asthma also relied on established claims-based algorithms. Additionally, this analysis may have underestimated the incidence and burden of pertussis, as some patients may not have sought care with a health care provider. Finally, some non-pertussis-related illnesses were included when calculating all-cause costs (although because the analysis evaluated the change in costs between the pre- and post-index date periods, any non-pertussis-related costs that occurred in the post-index period would reasonably have been expected to be balanced out by those in the pre-index date period).
To conclude, this study identified the potential for long-term complications from pertussis among patients with pre-existing respiratory conditions. Additional explorations of disease course and specific outcomes following pertussis infection, including complications and resource-use patterns, in individuals with respiratory comorbidities are warranted. During the 6-month follow-up window after a diagnosis of pertussis, patients with pertussis and COPD accrued approximately $6154 more in adjusted health care costs compared with matched patients with pertussis without COPD or asthma, while patients with pertussis and asthma accrued approximately $1639 more in adjusted health care costs compared with matched patients with pertussis without COPD or asthma. Additionally, this study found that patients with pre-existing asthma or COPD were more likely to have diagnosed pertussis compared with patients without pre-existing asthma or COPD. Focused interventions to prevent pertussis infection among these high-risk patients, including targeted Tdap vaccination strategies, could aid in reducing exacerbation of asthma and COPD, resulting in long-term health care savings.
AUTHOR CONTRIBUTION
All authors participated in the design, implementation, or analysis of the study and in the interpretation of the study. All authors had full access to the data, contributed to the development of this manuscript, and gave final approval before submission.
ACKNOWLEDGEMENTS
The authors acknowledge Mayank Ajmera (RTI Health Solutions) for assistance with the preliminary analysis of the study data and Kate Lothman (RTI Health Solutions) for medical writing support. The authors would like to thank Business & Decision Life Sciences platform for editorial assistance and manuscript coordination, on behalf of GSK Vaccines. Marie Cloes coordinated manuscript development and provided editorial support. GlaxoSmithKline Biologicals SA funded this study (GSK study identifier: HO-15-15543) and was involved in all stages of study conduct, including analysis of the data. GlaxoSmithKline Biologicals SA also took in charge all costs associated with the development and publication of this manuscript.
DECLARATION OF INTEREST
P.O.B. and L.-D.G. are employees of the GSK group of companies. P.O.B. owns shares in the GSK group of companies as part of his employee remuneration. J.L.M., R.P., S.K.K., and K.L.D. are employees of RTI Health Solutions, which received funding from the GSK group of companies for the conduct of the study. S.K.K. has received contract research funding from Eli Lilly, Pfizer Inc., and LEO Pharma, and K.L.D. has received contract research funding from Merck through their institution.








 Open access
Open access
{kind=link}