


Introduction
Ectopic atrial tachycardia in the neonatal period is an uncommon arrhythmia that may be difficult to control with standard antiarrhythmic therapy. It is typically related to increased automaticity and may be incessant, with a risk of tachycardia-induced cardiomyopathy. We report a case of refractory neonatal ectopic atrial tachycardia successfully treated with ivabradine.
Case report
A term neonate was prenatally diagnosed with persistent foetal tachycardia from 12 weeks of gestation, with a constant heart rate of approximately 200 beats per minute. There were no signs of cardiac failure or extracardiac abnormalities. The arrhythmia showed no variability or spontaneous termination. Foetal rhythm analysis suggested a regular tachycardia with a long ventriculoatrial interval (Supplementary file 1), consistent with an automatic atrial mechanism.
Maternal transplacental treatment with flecainide was initiated at 20 weeks of gestation and progressively increased due to incomplete control, reaching 200 mg every 12 hours. This resulted in partial reduction of the foetal heart rate to approximately 160 beats per minute. The remainder of the pregnancy was uneventful, without evidence of foetal haemodynamic compromise. Delivery occurred at 38 weeks of gestation.
After birth, the neonate was haemodynamically stable, with Apgar scores of 9 at 1 and 5 minutes. Electrocardiography demonstrated a regular atrial tachycardia with abnormal P-wave morphology and normal axis, suggestive of an ectopic atrial origin (Figure 1).
Electrocardiogram at birth. Regular atrial tachycardia with abnormal P-wave morphology and normal axis, suggestive of an ectopic atrial origin.

Figure 1. Long description
Panel A: A line graph showing lead I with regular atrial tachycardia. The horizontal axis represents time, and the vertical axis represents electrical activity. The graph shows abnormal P-wave morphology and normal axis, suggestive of an ectopic atrial origin. Panel B: A line graph showing lead II with similar characteristics. Panel C: A line graph showing lead III with regular atrial tachycardia. Panel D: A line graph showing lead aVR with regular atrial tachycardia. Panel E: A line graph showing lead aVL with regular atrial tachycardia. Panel F: A line graph showing lead aVF with regular atrial tachycardia. Panel G: A line graph showing lead V1 with regular atrial tachycardia. Panel H: A line graph showing lead V2 with regular atrial tachycardia. Panel I: A line graph showing lead V3 with regular atrial tachycardia. Panel J: A line graph showing lead V4 with regular atrial tachycardia. Panel K: A line graph showing lead V5 with regular atrial tachycardia. Panel L: A line graph showing lead V6 with regular atrial tachycardia.
Treatment with oral flecainide was continued despite partial efficacy and subsequently combined with digoxin in an attempt to optimise conventional therapy before considering alternative treatments. Despite this, heart rate remained persistently elevated, with average values above 160 beats per minute. At 9 days of life, despite combination therapy, mean heart rate was 171 beats per minute.
An adenosine test was performed to further clarify the mechanism of tachycardia. Transient atrioventricular block revealed persistent atrial activity with a consistent morphology, supporting the diagnosis of ectopic atrial tachycardia. This finding is consistent with an automatic atrial mechanism.
Given the inadequate response to conventional therapy, treatment was discontinued and ivabradine was initiated at a dose of 0.2 mg/kg/day in two divided doses. A rapid reduction in heart rate was observed within hours, without evidence of arrhythmia termination, with values decreasing to 135–150 beats per minute. This improvement was sustained over the following days.
The patient was discharged with outpatient follow-up and remained asymptomatic, with appropriate growth. There was no evidence of ventricular dysfunction or signs of heart failure during follow-up. At 3 months of age, Holter monitoring showed a mean heart rate of 139 beats per minute, with persistence of ectopic atrial tachycardia under ivabradine treatment. The patient remained asymptomatic, with no evidence of ventricular dysfunction on echocardiography.
Discussion
Ectopic atrial tachycardia is a rare neonatal arrhythmia caused by increased automaticity of an atrial focus. Reference Ge, Li, Liu and Jiang1 Its incessant nature may lead to tachycardia-induced cardiomyopathy if not adequately controlled. Reference Karmegaraj, Balaji and Raju2
Management is often challenging, as conventional antiarrhythmic drugs may be limited by incomplete efficacy and potential haemodynamic side effects. Reference Ge, Li, Liu and Jiang1 In our case, the arrhythmia was already present in foetal life and showed only partial response to transplacental and postnatal therapy, highlighting these limitations.
Ivabradine selectively inhibits the hyperpolarisation-activated cyclic nucleotide-gated channels responsible for the pacemaker current, reducing phase 4 depolarisation and suppressing abnormal automaticity. Reference Brugada, Katritsis and Arbelo3 Importantly, it does not affect myocardial contractility or blood pressure, making it particularly attractive in neonates.
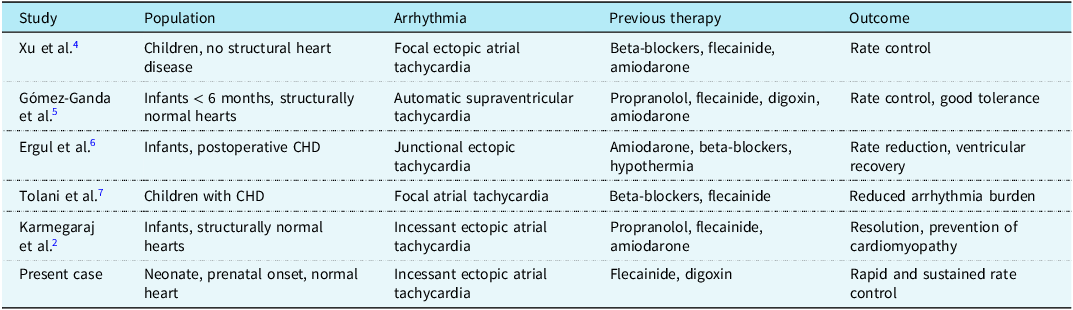
Growing evidence supports the use of ivabradine in paediatric automatic tachycardias.( Reference Karmegaraj, Balaji and Raju 2 , Reference Xu, Guo and Gao 4 – Reference Tolani, Ramdat Misier and Alqahtani 7 ) As summarised in Table 1, previous reports have demonstrated its efficacy in reducing heart rate and improving outcomes in infants and children, particularly in refractory cases.
Published reports of ivabradine use in paediatric automatic atrial tachycardias

Table 1. Long description
A table summarizing studies on ivabradine use in paediatric automatic atrial tachycardias. The table has five columns: Study, Population, Arrhythmia, Previous therapy, and Outcome. It contains six rows of data. Row 1: Study, Xu et al.4; Population, Children, no structural heart disease; Arrhythmia, Focal ectopic atrial tachycardia; Previous therapy, Beta-blockers, flecainide, amiodarone; Outcome, Rate control. Row 2: Study, Gómez-Ganda et al.5; Population, Infants < 6 months, structurally normal hearts; Arrhythmia, Automatic supraventricular tachycardia; Previous therapy, Propranolol, flecainide, digoxin, amiodarone; Outcome, Rate control, good tolerance. Row 3: Study, Ergul et al.6; Population, Infants, postoperative CHD; Arrhythmia, Junctional ectopic tachycardia; Previous therapy, Amiodarone, beta-blockers, hypothermia; Outcome, Rate reduction, ventricular recovery. Row 4: Study, Tolani et al.7; Population, Children with CHD; Arrhythmia, Focal atrial tachycardia; Previous therapy, Beta-blockers, flecainide; Outcome, Reduced arrhythmia burden. Row 5: Study, Karmegaraj et al.2; Population, Infants, structurally normal hearts; Arrhythmia, Incessant ectopic atrial tachycardia; Previous therapy, Propranolol, flecainide, amiodarone; Outcome, Resolution, prevention of cardiomyopathy. Row 6: Study, Present case; Population, Neonate, prenatal onset, normal heart; Arrhythmia, Incessant ectopic atrial tachycardia; Previous therapy, Flecainide, digoxin; Outcome, Rapid and sustained rate control.
In our case, ivabradine achieved effective rate control without complete rhythm conversion, which is consistent with its mechanism of action targeting automaticity rather than arrhythmia termination. Reference Gómez-Ganda, Parramón-Teixidó and Giralt-García5 Early initiation may help avoid escalation to more aggressive therapies and reduce the risk of myocardial dysfunction. Reference Karmegaraj, Balaji and Raju2 These findings support early consideration of ivabradine in neonatal automatic tachycardias refractory to conventional therapy, particularly when haemodynamic tolerance is a concern.
Conclusion
Ivabradine may represent a safe and effective therapeutic option in neonatal ectopic atrial tachycardia refractory to conventional treatment. Its favourable haemodynamic profile and mechanism of action make it particularly attractive in this population. Further studies are required to define its role in clinical practice.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S104795112612352X.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
None.
Ethical standard
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation and with the Helsinki Declaration.




 Open access
Open access