

Key messages
Chapter 2.3 reports on low-value care and how to reduce waste. Decommissioning or disinvesting from low-value care means taking money away from health care services that give poor value for money. Key learning includes that:
Ending investment in health technologies or treatments that are ineffective releases resources for more effective high-value care, increases efficiency and quality and contributes to sustainability.
Disinvesting from or decommissioning low-value care often faces institutional barriers.
Health technology assessment (HTA) and the continuous monitoring of peer-reviewed evidence and administrative health care data are key in identifying low-value care and prioritizing what should be decommissioned.
Combining financial and nonfinancial mechanisms can help influence both the supply of and demand for low-value care and stop its provision.
Broad stakeholder consultation and engagement is a key part of ending the use of low-value care because patients, clinicians, health-related organizations and health system norms and structures can all create barriers to change.
Decision-makers need to address how resources released by disinvestment can best be reinvested to strengthen efficiency, quality and access.
Introduction
There has been significant attention afforded to the challenges associated with assessing the value and introduction of novel health technologies, but much less attention afforded to how to disinvest from or decommission pre-existing health technologies or treatments which may be considered as low value. This is an important consideration for the sustainability of health care financing, particularly as this disinvestment or decommissioning has the potential to release resources which can be invested elsewhere, thereby improving the overall efficiency of the health care system.
The potential rewards are significant. For example, it has been estimated that approximately 30% of the USA’s health expenditure is on treatments and services considered as low value (Shrank, Rogstad & Parekh, 2019). However, defining what is meant by “low value” is challenging and context dependent. A common definition used in the literature is the “use of an intervention where evidence suggests it confers no or very little benefit on patients, or risk of harm exceeds likely benefit, or, more broadly, the added costs of the intervention do not provide proportional added benefits” (Scott & Duckett, 2015). While this may seem relatively straightforward, it is important to understand that whether a health technology or treatment is considered low value or not is usually determined by the specific indication, patient characteristics and preferences (Verkerk et al., 2018). With some understanding of the challenges in defining instances of low-value care, one will begin to understand the difficulties in developing strategies to disinvest from low-value care and monitoring implementation. In the simplest scenario, there may be broad consensus among the clinical and patient community that a health technology is not effective or has been superseded by a novel health technology that is more effective or cheaper. In this case, commissioners and policy-makers often chose to reduce coverage of the low-value health technology and remove it completely from relevant benefits packages. However, this scenario rarely exists and instead in most cases the classification of health technologies as low value is more nuanced and dependent upon specific circumstances. In these cases, a broader set of financial and nonfinancial approaches is needed to encourage disinvestment.
This chapter discusses these challenges in detail, and presents a conceptual framework for disinvestment from low-value care.
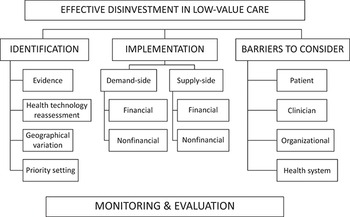
Fig. 2.3.1 details the conceptual framework. We begin by outlining approaches to identify potential instances of low-value care which may be candidates for disinvestment. We then discuss strategies to disinvest from low-value care and classify them as demand-side, supply-side, financial or nonfinancial interventions. We also consider what barriers to implementation exist from the patient, clinician, organizational and health system perspectives. Finally, we present a case study of a programme which has attempted to overcome these barriers and draw upon learnings from different approaches to disinvestment from low-value care over the last two decades: the NHS England Evidence-Based Interventions (EBI) programme.
Conceptual framework for disinvestment from low-value care

Figure 2.3.1 Long description
The Effective disinvestment in low-value care has 3 parts: Identification (Evidence, Health technology reassessment, Geographical variation, and Priority setting), Implementation (Demand and supply-side, each with financial and non-financial considerations), and Barriers to consider (Patient, Clinician, Organisational, and Health system). This is followed by monitoring and evaluation.
Identifying candidates for disinvestment
The first stage of disinvestment from low-value care is the identification and classification of certain health technologies as low-value. Various approaches have been tried. The most prominent methods discussed in the literature include appraising published evidence, health technology (re)assessment and exploring variation (Elshaug, McWilliams & Landon, 2013; Malik et al., 2018; Public Health England, 2016). While these are sometimes discussed as distinct approaches, in reality the principles which underlie these three approaches overlap and they are conducted in parallel. Once instances of low-value care have been identified, a process of prioritization to identify targets for disinvestment is then undertaken at either the national or local level.
Appraising published evidence
The initial step to identifying potential candidates for disinvestment is typically systematic searches of the published evidence to find instances of low-value care (Brook, 2010; NHS England, 2018; NICE, 2014). Ideally, the development of the search criteria should be transparent and involve multiple stakeholders including patients, commissioners and health care professionals. Searches must also include strict inclusion and exclusion criteria, and to narrow the scope searches are often conducted on a specialty or indication basis with the involvement of professional societies. The Cochrane Library is a particularly useful resource for such searches, as it incorporates a repository of systematic reviews of the comparative clinical and cost–effectiveness of health technologies. It has been shown to include many recommendations for disinvestment suitable for translation into practice (Garner et al., 2013).
One practical demonstration of this approach took place in Australia, where a team of academics was commissioned by the Australian Government to draw up recommendations for disinvestment, and subsequently identified over 150 low-value care interventions in the Australian Medicare Benefits Schedule based on a review of the literature, the Cochrane Library, and nominations from both clinical and non-clinical stakeholders (Elshaug et al., 2012). The BMJ Rapid Recommendations series is another useful resource, combining systematic literature reviews with economic evaluations to develop recommendations on disinvestment from low-value care (Siemieniuk et al., 2017).
Health technology (re)assessments
While appraising already published evidence is an essential component of identifying potential candidates for disinvestment, comparative HTA processes are sometimes required to establish whether a pre-existing or established health technology is no longer cost-effective compared to other health technologies or against a relative cost–effectiveness threshold. This requires the calculation of costs per quality-adjusted life-year. However, there is considerable variation in the role of HTA agencies internationally with regards to disinvestment. These agencies are typically focused on evaluating novel health technologies rather than providing disinvestment recommendations for pre-existing health technologies. A review of 62 HTA agencies conducted in 2015 found evidence of methodological frameworks for disinvestment from only four countries, specifically Austria, Italy, Spain and the United Kingdom (Calabrò et al., 2018). The same review also commented how most HTA activities in disinvestment were in the field of research and not widely applied in practical clinical settings.
England’s National Institute for Health and Care Excellence (NICE) has the most experience of encouraging disinvestment from low-value care. In 2005, the government requested that NICE pilot an “ineffective treatment programme”, and following consultation, this led to the belief that the best approach to disinvestment was through the publication of clinical guidance and associated “do not do” lists. NICE subsequently reviewed all pre-existing HTA recommendations and guidance, and identified over 2000 clinical interventions as candidates for disinvestment (Garner & Littlejohns, 2011). However, this programme has subsequently been replaced by national initiatives, such as the EBI programme (see the Evidence in practice: the NHS England Evidence-Based Interventions (EBI) programme section), that are more focused on co-development and ownership with clinicians with hopes of increased engagement. Other HTA agencies have come to similar conclusions: that their efforts may be enhanced with improved collaboration with specialty organizations. For example, the Canadian Agency for Drugs and Technologies in Health has recently published recommendations of low-value care in conjunction with Choosing Wisely Canada, a grass roots movement encouraging clinicians to abstain from unnecessary interventions (Basharat & Born, 2021).
Variations in level of use
A key component of identifying potential candidates for disinvestment is to analyse administrative health care data to explore to what extent there is current variation in utilization. Low volumes of an ineffective health technology suggest that disinvestment is feasible, best practice is being achieved and learning can be shared with areas that are not achieving low volumes. In contrast, high volumes suggest an area of high resource use and potentially unwarranted clinical variation. However, it must be remembered that substantial variation may either demonstrate inequity of care (underuse of high-value health technology) or inappropriate use of resources (overuse of low-value health technology). Therefore, while broad geographical variation implies inappropriate care, whether it constitutes overuse or underuse requires further assessment (Appleby et al., 2011; Public Health England, 2016; Wennberg & Gittelsohn, 1973).
Making that assessment requires some level of understanding of what an appropriate or expected level of utilization should be for relevant health technologies for specific populations based upon characteristics such as age, gender and comorbidities. However, challenges with data availability and suitability are common and identifying a suitable threshold for when variation may warrant further investigation is not straightforward. Many countries, including Australia, Canada, Germany, the Netherlands, New Zealand, Spain, the United Kingdom and the USA, have focused on establishing Atlases of Variation, which use data on geographical variation to benchmark health care providers and guide efforts to reduce unwarranted clinical variation (DaSilva & Gray, 2016; Harrison et al., 2020; Health Quality & Safety Commission New Zealand, 2021; World Bank, 2015). A review of the effectiveness of these programmes found that providing feedback on variation was associated with reductions in overuse of tests and treatments, and improvements in adherence to guidelines and protocols (Harrison et al., 2020). However, more evidence is needed on the relative effectiveness of particular feedback approaches.
Prioritizing candidates for disinvestment
Once candidates for investment are identified, a major challenge is prioritizing which low-value health technologies should be targeted for disinvestment. This is a complex process which needs to consider the relative trade-offs between alternative candidates for disinvestment, including potential savings, certainty of evidence on lack of clinical and cost–effectiveness and the potential unintended consequences, such as substitution by other types of care or inequity in access. If there is significant heterogeneity in clinical practice and patient needs between regions, these trade-offs may be very different at national and local levels.
In England, local efforts to prioritize candidates for disinvestment are common, for example through listing Procedures of Limited Clinical Effectiveness or Procedures of Limited Clinical Value (Coronini-Cronberg et al., 2015). These typically involve an evidence review and a local resource impact assessment, but have been criticized for a lack of transparency and accountability, and for resulting in a so-called “postcode lottery” whereby patients are confronted with sometimes unexplained variations in eligibility criteria to access different treatments based upon where they live (Russell et al., 2013). Other countries such as Wales (Charles et al., 2016) and Canada (Smith et al., 2016) have focused on utilizing resource management frameworks such as programme budgeting and marginal analysis to establish systematic approaches to disinvestment at the local level that improve transparency, accountability and public participation in decision-making. This typically involves mapping candidates for investment or disinvestment, and evaluation of the relative benefits and drawbacks of alternative candidates based upon stakeholder perspectives, and the economic concepts of opportunity cost and marginal gain (Donaldson et al., 2010). However, there is significant variation in engagement and approach to public involvement, and these frameworks are often only utilized sporadically or for research purposes rather than routinely in practice (Tsourapas & Frew, 2011).
Evidence on approaches to disinvestment from low-value care
Financial and nonfinancial mechanisms exist, both on the demand and supply side. Once low-value interventions are identified, several approaches to disinvestment can be utilized; there is now growing evidence on the effectiveness of these alternative approaches. Colla et al. (2017) classified these according to demand-side (i.e. patients and consumers) and supply-side (i.e. health care providers) interventions. We offer a similar approach encompassing more recent studies, and further categorize these interventions according to which are financial or nonfinancial mechanisms (Table 2.3.1).

Table 2.3.1 Long description
The first part of the table is Demand-side interventions. It has 2 columns: Nonfinancial and Financial. It reads as follows. Nonfinancial: Educational interventions (public awareness campaigns and patient information leaflets) - strong evidence. Shared decision-making between patients and clinicians - mixed evidence. Public reporting of variation in provisions of low-value care between health care providers - weak evidence. Financial: Cost-sharing for low-value health technologies and treatments (co-payments, deductibles, and co-insurance) - strong evidence. Removal of low-value health technologies and treatments from a benefits package (that is, delisting or negative lists) - strong evidence. Reference pricing to improve generic prescribing - strong evidence.
The second part of the table is Supply-side interventions. It has 2 columns: Nonfinancial and Financial. It reads as follows. Nonfinancial: Clinical decision support tools (embedded in health information technology systems, patient pathways and policies) - strong evidence. Educational interventions (awareness campaigns, continuing professional development) - mixed evidence. Feedback to providers (cycles of audit and feedback, individual feedback to prescribers) - mixed evidence. Financial: Pay for performance (financial incentives to reduce provision of low-value health technologies and treatments) - strong evidence. Penalties or fines for overprescribing or providing unnecessary care - weak evidence. Payer restrictions (through gatekeeping, or prior approval mechanisms) - strong evidence. Risk sharing (through capitation or global budgets) - mixed evidence.
Evidence on demand-side financial disinvestment interventions
Evidence of financial disinvestment mechanisms on the demand side shows promising impacts; however, it also exposes potential unintended consequences.
Demand-side interventions aim to curb the provision of low-value care through influencing patient or consumer behaviour. The predominant financial mechanism utilized for this purpose is cost-sharing, whereby costs of unnecessary procedures are shared between patients and payers through different co-payments, deductibles and co-insurance in an attempt to communicate value to patients. The introduction of targeted co-payments (ranging from US$ 100–500 in the fiscal year 2011/2012) for several low-value diagnostics (sleep studies, computed tomography scans, magnetic resonance imaging scans, positron emission tomography scans and upper gastrointestinal endoscopies) and surgical procedures (spine surgeries for pain, shoulder and knee arthroscopies, and hip and knee replacements) by a large insurer in the USA found significantly reduced use of targeted services, with a price elasticity of −0.22 (Gruber et al., 2020). Crucially, the same study found no impact of substitution between targeted and non-targeted services. However, when non-targeted, there is a risk that patients will forgo both high-value and low-value care, with several studies concluding that patients may not necessarily be able to distinguish between the two (Lohr et al., 1986; Wharam et al., 2011). Moreover, there is a risk that cost-sharing will have differential impacts between socioeconomic groups, with cost-sharing disproportionately impacting people of lower socioeconomic groups (Wharam et al., 2011). Reference pricing is an example of cost-sharing commonly utilized in Europe to discourage the use of brand-name medicines – which can be understood to be an example of low-value care when equivalent generic versions exist – in favour of generic medicines. Evidence suggests that reference pricing can generate higher generic medicine use, but also unintended consequences such as the complete discontinuation of cost-effective treatments for chronic diseases (Gibson, McLaughlin & Smith, 2010).
Cost-sharing is different to the complete removal of low-value health technologies or treatments from a defined benefits package, as when this strategy is adopted costs are not shared between the patient and payer and the patient is exposed to 100% of the costs. This type of financial intervention, sometimes called “delisting” or creating “negative lists”, is most easily applied to pharmaceuticals which have clear indications. This strategy has been applied to hundreds of pharmaceuticals in France and has reduced relevant prescriptions by up to 50% (Pichetti & Sermet, 2011), but has been controversial for some pharmaceuticals such as the use of acetylcholinesterase inhibitors for patients with dementia (Walsh, King & Brayne, 2019). Delisting or removal from the benefits package has also been used effectively in many other European countries including Czechia (Chytilová & Šebesta, 2015), Denmark (Hesse et al., 2013), Italy (Rocchi et al., 2004) and the Netherlands (Kroneman & de Jong, 2015).
Evidence on demand-side nonfinancial disinvestment interventions
There are several nonfinancial demand-side mechanisms that have been used to influence patient or consumer demand for low-value care including improved education, shared decision-making and public reporting. Excess antibiotic use is a key example of low-value care, and there are many pre-post studies which demonstrate that large-scale multimodal public awareness campaigns can change knowledge, behaviours and usage of antibiotics (Price et al., 2018). There is also evidence for other pharmaceuticals: for example, a patient information leaflet on the indication, harms and drug interactions of benzodiazepines, as well as visual tapering recommendations, has been shown to increase discussions around cessation, and numbers of patients achieving full cessation (Tannenbaum et al., 2014). Shared decision-making involves patients and clinicians having a focused and detailed discussion regarding the low-value treatment in question, thereby enabling the patient to make a fully informed choice regarding their care (Elwyn et al., 2012). A review of the public’s role in reducing low-value care found that decision-making tools that supported shared decision-making between clinicians and patients, such as the educational materials produced by the international Choosing Wisely initiative, were effective (Reyes et al., 2020), although rarely utilized in practice (Sypes et al., 2020). Increasingly, public reporting is used to show variation in provision of low-value care between health care providers (Maratt et al., 2019; Reyes et al., 2017). In theory, this has the potential to alter the behaviour of health care providers if patients make choices based upon this information. However, this is dependent upon patients being able to easily view and understand this information, as well as being able to change which health care providers they access. In reality, largely because these conditions are often not met, evidence suggests that public reporting generally may have negligible or limited impact on health care quality (Joynt et al., 2012; Ryan, Nallamothu & Dimick, 2012). However, more research is needed to understand the impact on the provision of low-value care specifically (Maratt et al., 2019).
Evidence on supply-side financial disinvestment mechanisms
Supply-side interventions aim to change the behaviour of health care providers at either the organizational or individual level. The four financial mechanisms commonly utilized to incentivize health care providers to reduce provision of low-value care are: pay for performance (P4P); penalties; payer restrictions; and risk sharing. P4P programmes provide financial incentives to health care providers to reduce the provision of inappropriate care – for example, excess antibiotic prescriptions or unnecessary laboratory tests. Evidence from the United Kingdom has indicated that a nationwide P4P programme, the Quality Premium, has been effective at reducing inappropriate antibiotic prescribing (Bou-Antoun et al., 2018). Evidence from the USA has also shown that a financial incentive scheme for residents reduced unnecessary blood tests and adherence to clinical guidance (Han et al., 2014). In contrast to P4P programmes which reward health care providers, penalties have been used to fine clinicians who overprescribe unnecessary or potentially harmful treatments. These were used in France between 1994 and 1996, when approximately 13 000 doctors were surveyed over two years and ultimately 75 were fined for inappropriate prescribing (Busse et al., 2015). However, in 1999 the sanctions were declared illegal and the policy was abandoned. A systematic review of measures in six high-income countries for curbing overprescribing also found that penalties are rarely used (Rashidian et al., 2015).
Payer restriction involves only providing reimbursement for certain indications and contexts, and is often implemented and monitored through some form of prior approval or gatekeeping mechanism to access the relevant low-value health technology or treatment. One study demonstrated that introducing a gatekeeping policy based upon patient symptoms for an autoimmune blood test reduced inappropriate testing (Sinclair, Saas & Stevens, 2004). Similarly, another study demonstrated that introducing an infectious disease consultation requirement for parenteral antibiotic therapy in the outpatient setting reduced inappropriate prescribing (Conant, Erdman & Osterholzer, 2014). Risk sharing involves utilizing reimbursement mechanisms that expose health care providers to the financial cost of services provided. These typically involve some form of global budget or capitation payment, and in theory, could encourage the provider to disinvest from low-value care, thereby maximizing the value for patients from restricted funds. In the USA, Blue Cross Blue Shield introduced an Alternative Quality Contract in 2009 for health care providers, which incorporated global payments and found that cardiovascular services reduced by 7.4% and imaging services reduced by 6.1%, but colonoscopies increased by 5.2% (Song et al., 2013). However, another study from the USA found no association between capitation payments and low-value imaging for low back pain and headache in the primary care setting (Liao et al., 2020). Moreover, other studies have commented that reimbursement mechanisms such as capitation or global budgets are unlikely to incentivize disinvestment from low-value care in isolation, and they must be utilized as part of multicomponent strategies (Lee et al., 2016; Mafi et al., 2019).
Evidence on supply-side nonfinancial disinvestment mechanisms
There are three nonfinancial supply-side mechanisms utilized to encourage health care providers to reduce provision of low-value care; clinical decision support tools; education; and feedback to providers. Clinical decision support tools aim to reduce unnecessary tests and unsafe prescribing while promoting compliance with guidelines on evidence-based care, and can be embedded into health information technology systems, patient pathways or policies. Prompts integrated into health information technology systems that alert clinicians they are potentially non-compliant with guidance or ordering unnecessary tests have been shown to be effective in reducing the provision of unnecessary blood transfusions (Baer et al., 2011), inappropriate use of imaging (Aston, 2010; Solberg et al., 2010) and duplicate blood tests (Levick et al., 2013; Niès et al., 2010). Moreover, other studies have demonstrated that adapting prescription order displays to show only generic medicines (Patel et al., 2014), or incorporating infection disease specialist reviews into a computerized antibiotic authorization system can reduce low-value prescribing (Potasman, Naftal & Grupper, 2012). However, it is important to consider the risk of alert fatigue in clinicians who can then choose to ignore or override notifications. The evidence regarding education for clinicians, who may be reluctant to engage with such efforts, is mixed. Evidence on trends in the provision of 32 low-value services for Medicare recipients between 2014 and 2018 (Mafi et al., 2021) concluded there were only marginal reductions in provision of low-value care despite a national education campaign to limit the provision of these services in collaboration with specialty societies. It appears that educational programmes may be more effective if more targeted and multimodal. For example, a continuing medical education programme involving tutorials and an interactive seminar on shared decision-making has been shown to result in lower levels of inappropriate antibiotic use, with 52% of patients in the control group and 27% of those in the intervention group deciding to use antibiotics’ after consultation (Légaré et al., 2012). Similarly, lectures and the introduction of a medicines reconciliation form have been shown to reduce inappropriate acid suppression therapy during hospital admission from 51% to 22% (Gupta et al., 2013). Feedback to providers on the extent of the provision of low-value care can also reduce its provision. Cycles of audit and feedback at the local level have been associated with significant reductions in low-value care, with a systematic review on this topic highlighting reductions achieved in inappropriate polypharmacy, antibiotic use and imaging (Ivers et al., 2012). Results at the national level are more mixed. A study from the United Kingdom which evaluated the use of feedback to individual practices that were in the top 20% of antibiotic prescribers was shown to reduce antibiotic prescriptions by 3.7% (Ratajczak et al., 2019). However, two other studies from Switzerland and Denmark respectively, which evaluated the use of individual provider feedback alongside a nationwide antibiotic stewardship programme, found no associated change in antibiotic use (Hemkens et al., 2017; Søndergaard et al., 2003).
Evidence on multicomponent disinvestment interventions
Evidence on multicomponent interventions shows that by combining different approaches, sustainable reductions in the provision of low-value care are possible.
Colla and colleagues concluded that multicomponent interventions are more likely to achieve sustainable reductions in the provision of low-value care (Colla et al., 2017). These multicomponent interventions typically involve a combination of nonfinancial supply-side mechanisms, incorporating clinical decision support tools, education and feedback to providers. For example, a study found that an educational programme involving a lecture, information card and twice weekly feedback on individual ordering behaviour reduced inappropriate echocardiography use (Bhatia et al., 2013). Similarly, another study focusing on the impact of audit and feedback, lectures and participation of pharmacists in ward rounds, found significant reductions in inappropriate acid suppression therapy (Khudair et al., 2011). Other examples involving the combining of educational campaigns, clinical decision support systems and cycles of audit and feedback have been shown to reduce prevalence of inappropriate use of blood transfusions (Arnold et al., 2011; Rothschild et al., 2007).
Barriers to the implementation of disinvestment strategies
There is a growing literature base on the barriers to implementation to consider when developing strategies to disinvest from low-value care.
Despite growing efforts to reduce the provision of low-value care, the evidence on many supply- and demand-side mechanisms is mixed. Below we discuss these barriers from a patient, clinician, organization and health system perspective.
Barriers to disinvestment at patient level
At the patient level, information asymmetry, lack of trust and limited patient involvement can get in the way of disinvestment efforts.
From a patient perspective, patients often lack the capability to differentiate between high- and low-value care (Lohr et al., 1986). Patients may therefore be reluctant to forgo unnecessary screening or testing due to fear of delayed diagnosis. Moreover, it has been emphasized that patients may mistrust the medical establishment, and feel that care is being withdrawn or restricted unfairly (Norton & Chambers, 2020). This can be particularly damaging to the patient-clinician relationship, and clinicians may therefore be unwilling to restrict access to low-value care. These tensions are intensified when disinvestment initiatives are developed with limited public involvement (Sypes et al., 2020), or lack of engagement from either patients or clinicians in shared decision-making (Allen et al., 2019). While disinvestment initiatives such as Choosing Wisely have focused on developing patient decision aids to promote awareness and shared decision-making, a review of these materials found few provided balanced information on the benefits and harms of alternative interventions and therefore may be misleading or confusing for patients (Légaré et al., 2016).
Barriers to disinvestment at clinician level
From the clinician perspective, disinvestment from low-value care is often perceived as a cost-cutting exercise rather than for quality improvement (Embrett & Randall, 2018), and many clinicians fear lost revenue (Zadro et al., 2019). Other barriers discussed in qualitative interviews are time constraints, which prevent clinicians from engaging in shared decision-making with patients (Kool et al., 2020; Zikmund-Fisher et al., 2017), and fear of patient dissatisfaction or litigation that may result from withdrawing or restricting access to care (Lin et al., 2017; Osorio et al., 2020; Pausch et al., 2020; Zikmund-Fisher et al., 2017). Clinicians also discussed difficulties in overcoming patients’ preferences (Smith et al., 2020), and emphasized there is a lack of tools available to support shared decision-making. Most surveys indicated there was a high awareness among clinicians of low-value care initiatives and the need to manage limited resources efficiently (Buist et al., 2016; Kool et al., 2020), but most clinicians nonetheless reported they would still order unnecessary tests or procedures if a patient insisted.
Barriers to disinvestment at the organization level
From the organizational perspective, lack of resources to implement disinvestment initiatives, for example to create additional clinic time to facilitate shared decision-making, is discussed frequently in the literature (Dulmen et al., 2020; Ellen et al., 2018; Norton & Chambers, 2020). Concern about resources is exacerbated by the perception that engagement with disinvestment initiatives could further reduce available resources if they lead to lost revenues and increased litigation. Organizations may also resist collaborating with other organizations if they are perceived as having competing interests or priorities (Ellen et al., 2018). Other barriers discussed within the literature include the risk of change fatigue if organizations are exposed to repeated quality improvement efforts (McMillan & Perron, 2020), and inadequate infrastructure – in particular, health information technology systems – to implement, monitor and evaluate disinvestment initiatives (Dulmen et al., 2020).
Barriers to disinvestment at the health system level
From a health system perspective, reimbursement mechanisms that reward volume of care, such as fee-for-service payments, rather than those which incentivize the reduction of unnecessary care, such as capitation or global payments, were repeatedly emphasized as a barrier to disinvesting from low-value care (Dulmen et al., 2020). Other barriers discussed in the literature include poor awareness or commitment on the part of policy-makers and leadership regarding the need to address low-value care (Ellen et al., 2018); difficulties in coordination and building consensus between stakeholders at different levels of the health care system (Ellen et al., 2018); and a lack of resources to undertake the academic work required to identify low-value care (Garner et al., 2013). A review of involvement by HTA agencies in disinvestment initiatives in Europe also identified a lack of guidelines for the identification of obsolete technologies (Calabrò et al., 2018), and discussed how disinvestment remains a relatively new concept within these agencies. Moreover, a lack of data or suitable measures for monitoring and evaluation has been highlighted (Chalmers et al., 2018).
Evidence in practice: the NHS England Evidence-Based Interventions (EBI) programme
Most recently, the National Health Service (NHS) in England has accelerated efforts to disinvest from low-value care by developing the EBI programme, which aims to reduce avoidable harm to patients, maximize value and avoid waste by reducing unnecessary interventions. Statutory guidance for the EBI programme was published in November 2018 (NHS England, 2018), and the programme was officially launched in April 2019.
Identification of candidates for disinvestment
To identify potential candidates for disinvestment, the programme first undertook a thorough review of published evidence and HTA recommendations and explored variation between local commissioning bodies. The team developing the programme was conscious of how previous initiatives to disinvest from low-value care – in particular, the NICE “do not do” lists and locally developed procedures – had failed to engage with relevant stakeholders. Therefore, the EBI team launched a consultation aimed at the public, commissioners and health care professionals (the latter through their specialty organizations). As a result, the first phase of the EBI programme identified 17 low-value procedures within two categories (Table 2.3.2).
Category 1: not clinically or cost-effective
Surgical intervention for snoring (not obstructive sleep apnoea)
Dilatation & curettage for heavy menstrual bleeding
Knee arthroscopy with osteoarthritis
Injection for nonspecific low back pain without sciatica
Category 2: clinically and cost-effective only in certain circumstances
Breast reduction
Removal of benign skin lesions
Grommets
Tonsillectomy
Haemorrhoid surgery
Hysterectomy for heavy bleeding
Chalazia removal
Shoulder decompression
Carpal tunnel syndrome release
Dupuytren’s contracture release
Ganglion excision
Trigger finger release
Varicose vein surgery
Category 1 interventions have been shown not to be clinically or cost-effective and there is consensus among health care professionals that the procedures should no longer routinely be offered to patients. Category 2 interventions are only clinically or cost-effective for certain types of indication and/or patients.
Implementing the disinvestment
The EBI programme draws upon learning from many previous initiatives undertaken to disinvest from low-value care, and uses a multicomponent approach to encourage disinvestment from these low-value procedures. The programme has set targets for each local commissioning body to reduce the number of category 1 interventions to “near zero” and category 2 interventions to 25% of current levels nationally. The latter target involved calculating an expected rate for each local commissioning body based on population characteristics. They delisted category 1 interventions, introducing a zero tariff, with health care providers no longer reimbursed by the NHS for these interventions. Local commissioning bodies were asked to implement a prior approval process for category 2 interventions, with clinicians now expected to seek approval from local commissioning bodies for appropriate indications and/or patients. Progress in meeting agreed targets continues to be monitored and shared with hospitals and clinical commissioning groups by means of a publicly available dashboard to allow benchmarking (NHS Business Services Authority, n.d.). The identification of low-value procedures is based upon combinations of operation and diagnostic codes that are continually refined based upon feedback from commissioners, hospitals and health care providers. Crucially, this allows the identification of low-value procedures according to specific indications, and relevant exclusion criteria for other indications when the procedure is considered as high-value. To support improved awareness, education and shared decision-making between patients and clinicians, a series of patient information leaflets and videos was also developed (AMRC, 2022). The EBI programme has since expanded to a second phase, with a further 31 low-value procedures, diagnostics and treatments, and the statutory guidance was published in November 2020 (AMRC, 2020).
Evaluation of the EBI programme
Conclusive evaluation of the EBI programme is not yet complete, as this has been hampered by the emergence of the COVID-19 pandemic.
A preliminary analysis of the first 11 months following implementation, against a control group of other yet to be identified low-value procedures, concluded that the EBI programme encouraged a general culture of disinvestment from low-value care but did not accelerate disinvestment for the low-value procedures under its remit (Anderson et al., 2022). Nevertheless, the EBI programme remains the most robust and comprehensive approach to disinvestment from low-value care in England to date. The EBI programme draws upon learning from many previous initiatives to disinvest from low-value care, and uses several financial and nonfinancial supply and demand-side approaches to encourage disinvestment. The EBI programme also attempts to overcome many barriers to implementation through a broad consultation process, transparent monitoring and evaluation mechanisms, feedback to individual hospitals and commissioners, and public reporting. Despite this, Anderson and colleagues (2022) conclude that the EBI programme may have taken an approach to implementation that it is too top-down, and that the success of the programme is also heavily dependent upon successful collaborations between local commissioning bodies, hospitals and clinicians at the local level.
Policy relevance and conclusions
While there is broad consensus that disinvestment from low-value care is crucial to the financial sustainability of health care systems, there continues to be disagreement among relevant stakeholders about how best to identify potential candidates for disinvestment and what approaches should be taken to encourage disinvestment. The complexity of these challenges is further compounded by uncertainties in defining in what circumstances specific health technologies or interventions may be considered low-value, and technical difficulties in the monitoring and evaluation of initiatives. The resulting lack of clarity has often led to differing levels of success and fractured relationships between policy-makers, clinicians and patients. One thing is clear: no perfect mechanism for disinvestment has been identified to date – highlighting how great the challenge of disinvestment from low-value care is.
As we look to the future, lessons can be drawn from the experience acquired over the past two decades. Disinvestment must be sensitive to the opinions of all stakeholders, in particular those who drive the persistent use of low-value care; it must be rigorous and transparent in the identification and prioritization of potential candidates for disinvestment; and its implementation must draw upon multiple approaches that consider both demand- and supply-side perspectives. The implementation of disinvestment needs to be understood as a dynamic process that involves continual monitoring and evaluation, with concomitant feedback to individual clinicians and health care providers. Finally, released resources need to be reinvested into other areas of high-value care so patients, clinicians and policy-makers can see the benefits of engaging with these initiatives, and to ensure that disinvestment from low-value care is not perceived as a cost-cutting exercise.Footnote 1



 Open access
Open access