


Introduction
Social anxiety disorder (SAD) is characterized by a fear of negative evaluation (e.g. embarrassment, humiliation, rejection) in one or more social situations, which are consequently avoided or endured with excessive anxiety (American Psychiatric Association, 2013). SAD is linked to substantial functional impairment across domains such as work, social life, and family life (Aderka et al., Reference Aderka, Hofmann, Nickerson, Hermesh, Gilboa-Schechtman and Marom2012; Stein et al., Reference Stein, Lim, Roest, de Jonge, Aguilar-Gaxiola, Al-Hamzawi, Alonso, Benjet, Bromet, Bruffaerts, de Girolamo, Florescu, Gureje, Haro, Harris, He, Hinkov, Horiguchi, Hu and Karam2017). Indeed, SAD is associated with a much higher unemployment rate compared with other anxiety and mood disorders, low self-reported quality of life, and is prevalent globally, with a 12-month prevalence of 2.4% (Dryman et al., Reference Dryman, Gardner, Weeks and Heimberg2016; Moitra et al., Reference Moitra, Beard, Weisberg and Keller2011; Stein et al., Reference Stein, Lim, Roest, de Jonge, Aguilar-Gaxiola, Al-Hamzawi, Alonso, Benjet, Bromet, Bruffaerts, de Girolamo, Florescu, Gureje, Haro, Harris, He, Hinkov, Horiguchi, Hu and Karam2017).
Cognitive behavioural therapy (CBT) largely based on models by Clark and Wells (Reference Clark, Wells, Heimberg, Liebowitz, Hope and Schneier1995) and Heimberg et al. (Reference Heimberg, Juster, Hope, Mattia and Stein1995) is widely regarded as first-line treatment for SAD (Katzman et al., Reference Katzman, Bleau, Blier, Chokka, Kjernisted, Van Ameringen, Antony, Bouchard, Brunet, Flament, Grigoriadis, Mendlowitz, O’Connor, Rabheru, Richter, Robichaud and Walker2014; Pelissolo et al., Reference Pelissolo, Abou Kassm and Delhay2019), demonstrating large effect size improvements in SAD symptoms (Mayo-Wilson et al., Reference Mayo-Wilson, Dias, Mavranezouli, Kew, Clark, Ades and Pilling2014). Group CBT (CBGT) has also been associated with medium to large effect size improvements in SAD symptoms, which are maintained at long-term follow-up (Fogarty et al., Reference Fogarty, Hevey and McCarthy2019; Mayo-Wilson et al., Reference Mayo-Wilson, Dias, Mavranezouli, Kew, Clark, Ades and Pilling2014; McCarthy et al., Reference McCarthy, Hevey, Brogan and Kelly2013). While some randomized controlled trials suggest that individual CBT is more effective than CBGT (Mörtberg et al., Reference Mörtberg, Clark, Sundin and Åberg Wistedt2007; Stangier et al., Reference Stangier, Heidenreich, Peitz, Lauterbach and Clark2003), others find these modalities equally effective (Dogaheh et al., Reference Dogaheh, Mohammadkhani and Dolatshahi2011; Neufeld et al., Reference Neufeld, Palma, Caetano, Brust-Renck, Curtiss and Hofmann2020) and a meta-analysis failed to establish significant differences in their efficacy for SAD treatment (Barkowski et al., Reference Barkowski, Schwartze, Strauss, Burlingame, Barth and Rosendahl2016). In both individual CBT and CBGT for SAD, participants engage in core CBT skills, while in CBGT participants have the added opportunity to interact with other treatment participants, and may benefit from their support, encouragement, accountability, and modeling (Taube-Schiff et al., Reference Taube-Schiff, Suvak, Antony, Bieling and McCabe2007). These positive group member interactions may generate group processes, such as group cohesion, which may in turn contribute to positive therapeutic outcomes (Taube-Schiff et al., Reference Taube-Schiff, Suvak, Antony, Bieling and McCabe2007).
Group cohesion can be described as the attraction or belonging members feel for their group, and conceptualizations of group cohesion have involved dimensions such as a sense of bonding, working together towards shared goals, engagement, and acceptance, support, and identification with one’s group (Marziali et al., Reference Marziali, Munroe-Blum and McCleary1997; Yalom and Leszcz, Reference Yalom and Leszcz2020). Recent meta-analytic and systematic reviews have demonstrated that group cohesion is reliably related to and predictive of treatment outcomes both across psychotherapy approaches and diagnostic categories (Burlingame et al., Reference Burlingame, McClendon and Yang2018) as well as in CBT for anxiety and related disorders (Luong et al., Reference Luong, Drummond and Norton2020). The limited research in SAD suggests that group connection and collaboration in CBGT for SAD can be present and have a positive impact on outcomes. For example, Bonsaksen et al. (Reference Bonsaksen, Borge and Hoffart2013) demonstrated that high engagement (a component of group cohesion consisting of mutual liking, collaborative problem-solving, and active participation within the group) is linked to decreased social anxiety symptoms both during treatment and at 12-month follow-up. Taube-Schiff et al. (Reference Taube-Schiff, Suvak, Antony, Bieling and McCabe2007) showed that increased group cohesion scores across CBGT for SAD sessions are associated with improved depression, general anxiety, and social anxiety symptoms. Most recently, McEvoy et al. (Reference McEvoy, Bendlin, Johnson, Kazantzis, Campbell, Bank and Egan2023) found that group cohesion is significantly and positively associated with post-treatment SAD symptoms in CBGT.
The COVID-19 pandemic led to a rapid scale-up of videoconference-based psychotherapies, which presented opportunities to expand our knowledge on the efficacy of this treatment delivery method. Research that focuses on CBGT, especially for anxiety and related disorders, is scarce but encouraging. In a pilot study, Khatri et al. (Reference Khatri, Marziali, Tchernikov and Shepherd2014) found that the proportion of participants that experienced a positive change in symptoms and symptom classification (e.g. from moderate to low symptoms) was identical across face-to-face and videoconference CBGT for mood and/or anxiety disorders. It should be noted, however, that this study only assessed depressive symptoms. In a non-clinical sample of university students who completed videoconference CBGT, participants reported a significant decrease in anxiety and depression symptoms, as well as high treatment satisfaction (Bantjes et al., Reference Bantjes, Kazdin, Cuijpers, Breet, Dunn-Coetzee, Davids, Stein and Kessler2021). Nauphal et al. (Reference Nauphal, Swetlitz, Smith and Rosellini2021) demonstrated that videoconference CBGT for SAD was feasible, acceptable, and successful in reducing symptoms; however, these results are preliminary and based on a very small sample. Most recently, Milosevic et al. (Reference Milosevic, Cameron, Milanovic, McCabe and Rowa2022) found similar improvement in symptoms when comparing in-person and videoconference CBGT for SAD and other anxiety and related disorders.
Studies investigating group processes in videoconference delivered CBGT are even more sparse. In a sample of participants with clinically significant symptoms of depression, Arrow et al. (Reference Arrow, Yap and Chester2021) demonstrated that group climate developed similarly across in-person and videoconference CBGT, and that it played a role in predicting therapeutic outcomes. In contrast, Lopez et al. (Reference Lopez, Rothberg, Reaser, Schwenk and Griffin2020) found that participants with depression, bipolar disorder, or anxiety who completed group dialectical behaviour therapy (DBT) using videoconference felt less connected to other group members compared with those in an in-person DBT group. To our knowledge, Nauphal et al. (Reference Nauphal, Swetlitz, Smith and Rosellini2021) is the only study to have evaluated group dynamics in videoconference CBGT for SAD. This study assessed group climate, and results indicated high engagement, low avoidance (i.e. of one’s responsibility in the group), and low conflict (i.e. among group members) in their group; however, their sample included only five participants.
While these results are promising, studies specific to SAD are warranted, especially because bonding and collaborating with one’s group via videoconference may be particularly challenging for the SAD population. Non-verbal communication, such as small gestures and eye contact, are important cues for comfortable conversation flow (Peros et al., Reference Peros, Webb, Fox, Bernstein and Hoffman2021). When these cues are difficult to see and feel, as they are over videoconference, it may be challenging for people who are already anxious in social situations to connect with their videoconference group (Peros et al., Reference Peros, Webb, Fox, Bernstein and Hoffman2021). Moreover, whenever one speaks in a videoconference, they can be seen and heard by the entire group and may feel as if they are ‘on stage’, which can be distressing for people with SAD and may discourage them from engaging with the group. When CBGT is conducted in-person, participants often take part in quiet side conversations with only one or a few of their fellow group members, which is invaluable to fostering relationships with one another. In videoconference CBGT, these opportunities are absent. In addition, videoconferencing software shows participants their own camera feed during sessions, which for people with SAD, may be particularly distracting and shift their focus away from therapy and their group (Payne et al., Reference Payne, Flannery, Kambakara Gedara, Daniilidi, Hitchcock, Lambert, Taylor and Christie2020). As such, further research is necessary to better understand whether group cohesion and positive treatment outcomes can be meaningfully developed in videoconference CBGT for individuals with SAD.
Therefore, the primary aim of the present study was to investigate the development of group cohesion in videoconference CBGT for SAD, in comparison with two groups: (1) in-person CBGT for SAD and (2) videoconference CBGT for other anxiety disorders (e.g. generalized anxiety disorder (GAD), obsessive-compulsive disorder (OCD), and panic disorder (PD)). A secondary aim was to compare treatment outcomes (i.e. reduction in SAD and related symptoms (e.g. depression, anxiety, and stress) from pre- to post-treatment) across all three groups.
We predicted that the videoconference CBGT for SAD group would report lower cohesion scores at both mid- and post-treatment when compared with the comparison groups due to the potential unique challenges this population may experience in videoconference-based treatment. We also predicted that group cohesion would develop, to some extent, in all three groups with an increase from mid- to post-treatment in each group. Finally, due to previous evidence demonstrating the efficacy of CBGT both in-person and using videoconference, we hypothesized that all three treatment groups would report significant symptom reduction.
Method
Participants
Participants were recruited retrospectively from the Anxiety Treatment and Research Clinic (ATRC) at St. Joseph’s Healthcare Hamilton and were assessed for DSM-5 diagnoses at pre-treatment using the Diagnostic Assessment Research Tool – a semi-structured diagnostic tool that can be used for a range of DSM-5 disorders (DART; McCabe et al., Reference McCabe, Milosevic, Rowa, Shnaider, Pawluk and Antony2017) – a psychiatric consult, or a nursing assessment. See Table 1 for assessment method details.
Demographics of videoconference SAD, in-person SAD, and videoconference other anxiety disorders groups
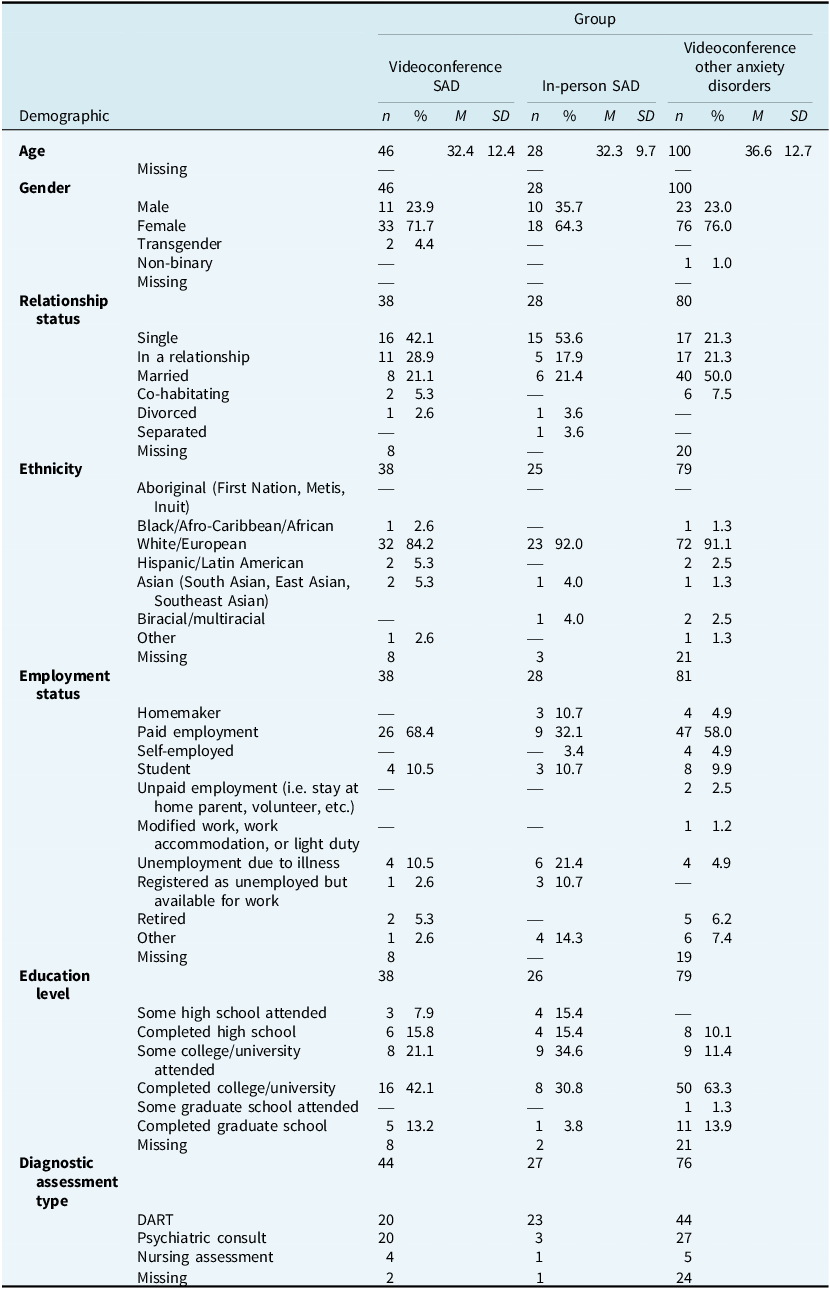
SAD, social anxiety disorder; n, number of participants; M, mean; SD, standard deviation; DART, Diagnostic Assessment Research Tool.
Inclusion criteria for the two SAD groups required a primary diagnosis of social anxiety disorder. For the other anxiety disorders groups, inclusion criteria required both a primary diagnosis of GAD, OCD, or PD and no co-morbid SAD diagnosis. All participants consented to their data being used for research. Data for the in-person SAD group was collected between January 2019 and December 2019 (prior to the onset of the COVID-19 pandemic) and data for the two videoconference groups were collected from participants using Zoom Video Communications’ platform between May 2020 and August 2022 (following the onset of the COVID-19 pandemic).
The present study used naturalistic data collection, which expectedly yielded low response rates. In the present study, ‘completers’ refers to those who, for at least one study measure, provided data at two time points, whereas ‘non-completers’ refers to those who did not provide data at two time points for any study measure. Chi-square analyses found no significant difference in the number of completers versus non-completers across mode of delivery (χ2(1,N=349)=.295, p=.587). There was a significant difference in the number of completers versus non-completers between all three treatment groups (χ2(2,N=349)=19.8, p<.001), where videoconference CBGT for SAD group members were more likely to be non-completers and videoconference CBGT for other anxiety disorders group members were more likely to be completers.
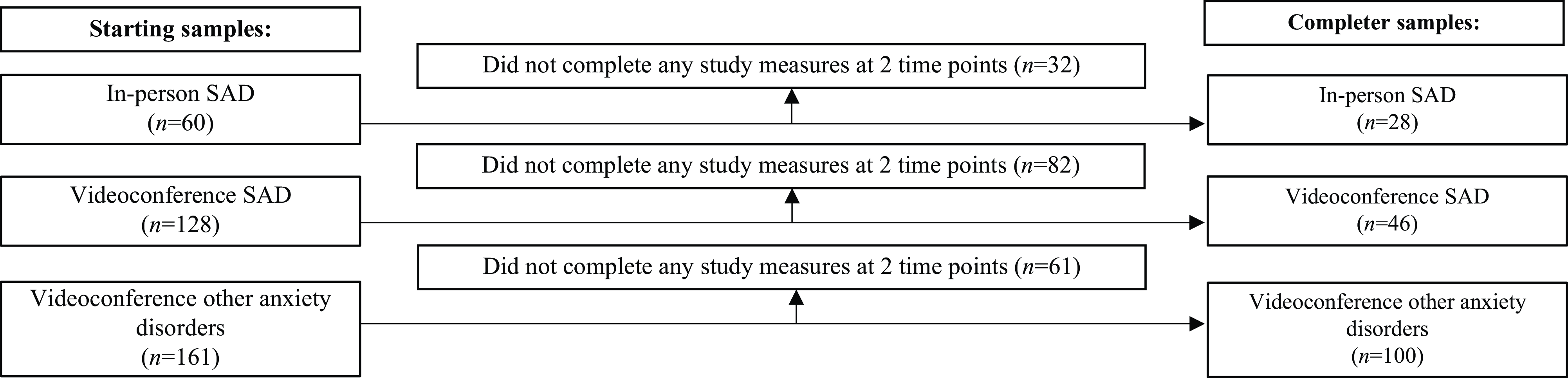
Chi-square and t-test analyses revealed no significant differences between completers and non-completers’ gender (χ2(5,N=349)=1.4, p=.920) and pre-treatment symptom scores (SPIN: mean difference (MD)=.124, p=.937; DASS-21-D: MD=1.05, p=.361; DASS-21-A: MD=1.35, p=.208; DASS-21-S: MD=.024, p=.981). A t-test indicated that completers were on average older than non-completers (MD=4.25 years, p=.001). Sixty individuals who completed in-person CBGT for SAD were eligible for inclusion in this study; however, 32 of these participants did not complete any of the study measures at both pre- or mid-treatment and post-treatment and were therefore omitted from all analyses and demographic reports. Therefore, the final in-person SAD group included 28 participants, with a mean age of 32.3 (SD=9.7), where 64.3% of participants self-identified as female. Including their primary diagnosis, 64.3% of this group had two diagnoses, 42.9% had three diagnoses, and 32.1% had four diagnoses. The most common co-morbid diagnoses were depressive disorders (28.8%) and other anxiety disorders (28.8%). In the videoconference SAD group, 128 participants who completed CBGT were eligible for inclusion in this study; however, 82 of these participants did not complete any of the study measures at both pre- or mid-treatment and post-treatment and were therefore omitted from all analyses and demographic reports, leaving a final sample of 46 participants, with a mean age of 32.4 (SD=12.4), where 71.7% of participants self-identified as female. Including their primary diagnosis, 63.0% of this group had two diagnoses, 32.6% had three diagnoses, and 13.0% had four diagnoses. The most common co-morbid diagnoses were depressive disorders (37.0%) and other anxiety disorders (29.6%). For the videoconference other anxiety and related disorders group, 161 participants who completed CBGT were eligible for inclusion in this study, however 61 of these participants did not complete any of the study measures at both pre- or mid-treatment and post-treatment and were therefore omitted from all analyses and demographic reports, leaving a final sample of 100 participants, with a mean age of 36.6 (SD=12.7), where 76.0% of participants self-identified as female. Including their primary diagnosis, 29.0% of this group had two diagnoses, 10.0% had three diagnoses, and 4.0% had four diagnoses. The most common co-morbid diagnoses were depressive disorders (21.3%). Of the participants in the other anxiety and related disorder group, 48 completed CBT for GAD, 31 completed CBT for OCD, and 21 completed CBT for PD. See Fig. 1 for participant flow diagram and Table 1 for additional demographic information.
Flow diagram of participant omissions. Any participant who completed treatment during the study data period but completed none of the study measures at more than one time point (i.e. completed a maximum of every study measure at only one time point) was automatically omitted from 2×3 ANOVA analyses in SPSS and was therefore also removed from demographic reports, so as to accurately characterize the included sample. n, sample size.
Interventions
All treatment groups were disorder-specific and were conducted using treatment manuals, which were developed based on existing CBGT protocols for SAD, GAD, OCD, and PD, respectively. The in-person SAD group came from 10 different therapy groups, the videoconference SAD group came from 13 different therapy groups, and the videoconference other anxiety disorders group came from 40 different therapy groups (20 GAD, 13 OCD, and 7 PD). Treatment components included psychoeducation, cognitive restructuring, exposure exercises, elimination of safety behaviours, the completion of homework between sessions, and other disorder-specific lessons and skill building customized for each disorder-specific treatment (e.g. response prevention in OCD, interoceptive exposure in PD). The CBGT for SAD treatment manual is primarily adapted from the model of Heimberg et al. (Reference Heimberg, Juster, Hope, Mattia and Stein1995) with content from the model of Clark and Wells (Reference Clark, Wells, Heimberg, Liebowitz, Hope and Schneier1995) regarding the elimination of safety behaviours.
Groups of 8–12 participants led by at least two therapists (including one or more experienced clinicians (e.g. psychologist) and one or more clinical learners (e.g. graduate student in psychology)) met for 2-hour weekly sessions for 12 weeks, either in-person or remotely using videoconference via a secure network. In the videoconference groups, participants were required to keep their cameras on, but participants chose whether to hide their own image. Breakout rooms were used for exposure exercises so participants could carry out exposures in smaller groups as is done in in-person treatment. No other adaptations were made to content in the videoconference groups.
Participants in all treatment groups completed self-report questionnaires at pre-, mid-, and post-treatment.
Measures
Group Cohesion Scale-Revised (GCS-R; Treadwell et al., 2001)
The GCS-R is a 25-item self-report questionnaire used to assess cohesion among group members in terms of various dimensions such as: interaction and communication, member retention, decision making, vulnerability among group members, and consistency between group and individual goals. Items are rated on a 4-point Likert-type scale, ranging from strongly disagree to strongly agree, which are summed to provide a single total score, with higher scores indicating higher group cohesion. The scale has demonstrated acceptable to good internal consistency reliability, with scores ranging from .48 to .89 on a pre-test assessment, and from .77 to .90 on a post-test assessment (Treadwell et al., Reference Treadwell, Lavertue, Kumar and Veeraraghavan2001). The GCS-R was completed by all participants at session 5 of treatment and again at post-treatment, and Cronbach’s alpha for completers in this sample ranged from .84 to .90.
Social Phobia Inventory (SPIN; Connor et al., 2000)
The SPIN is a 17-item self-report questionnaire used to assess the symptoms and severity of social anxiety disorder. The SPIN consists of three subscales: fear, avoidance, and physiological discomfort. Items on the SPIN are rated on a 5-point Likert-type scale, ranging from 0 (not at all) to 4 (extremely), which are summed to produce a total score and/or three individual subscale scores. Higher total scores on the SPIN indicate more severe and distressing social anxiety symptoms. The scale has demonstrated strong psychometric properties (Antony et al., Reference Antony, Coons, McCabe, Ashbaugh and Swinson2006; Connor et al., Reference Connor, Davidson, Churchill, Sherwood and Weisler2000). The SPIN was completed by all participants in the two SAD groups pre- and post-treatment. Cronbach’s alpha for completers in this sample ranged from .83 to .94.
Depression Anxiety Stress Scales, 21-item version (DASS-21; Lovibond and Lovibond, 1995)
The DASS-21 is a 21-item self-report questionnaire used to assess depression, anxiety, and stress symptoms. The DASS-21 consists of three subscales. The DASS-21-D measures depressive symptoms such as low positive affect, hopelessness, and feelings of worthlessness, the DASS-21-A measures characteristics of anxiety such as physical arousal and fear, and the DASS-21-S measures symptoms of stress such as tension and irritability. Items on the DASS-21 are rated on a 4-point Likert-type scale, ranging from 0 (did not apply to me at all) to 3 (applied to me very much or most of the time). Items are then summed to produce three individual subscale scores, where a higher score indicates more severe symptoms. The DASS-21 has demonstrated high internal consistency and factor analysis of the total scale has repeatedly produced three factors (Antony et al., Reference Antony, Bieling, Cox, Enns and Swinson1998; Lovibond and Lovibond, Reference Lovibond and Lovibond1995). The DASS-21 demonstrates strong convergent and divergent validity (Lee, Reference Lee2019). The DASS-21 was completed by all participants pre- and post-treatment, and Cronbach’s alpha for completers in this sample ranged from .91 to .95.
Diagnostic Assessment Research Tool (DART; McCabe et al., 2017)
The DART is a modular semi-structured interview used to diagnose a wide range of DSM-5 mental disorders. The DART has demonstrated excellent convergent validity with corresponding disorder-specific measures and excellent discriminant validity from a measure assessing general symptoms of depression and anxiety, as well as good to excellent construct validity (Schneider et al., Reference Schneider, Pawluk, Milosevic, Shnaider, Rowa, Antony, Musielak and McCabe2022).
Data analysis
Participants who did not complete one or more of the measures were omitted only from analyses involving those specific measures, which resulted in varying sample sizes across analyses. For the purposes of this study, any score on any measure that was greater than 1.5 times the interquartile range above the 75th percentile or below the 25th percentile of scores for that group on that measure was considered an outlier. In the videoconference SAD group, two outliers were found on the pre-treatment SPIN and two outliers were found on the post-treatment SPIN. In the other anxiety and related disorders group, one outlier was found on the pre-treatment DASS-21-D subscale, one outlier was found on the pre-treatment DASS-21-A subscale, and three outliers were found on the post-treatment DASS-21-D subscale. No outliers were found in the in-person SAD group on any of the measures. Outlier scores were adjusted to the lowest (SPIN) or highest (DASS-21) non-outlier score reported in their group and the participant’s data was retained.
A 2×3 repeated measures analysis of variance (ANOVA), with time as the within-subjects factor and treatment group as the between-subjects factor, was used to assess differences in group cohesion (mid- vs post-treatment GCS-R scores) and symptom improvement (pre- vs post-treatment DASS-21 scores) between all three treatment groups (videoconference SAD, in-person SAD, and videoconference other anxiety disorders), as well as differences in pre- vs post-treatment SPIN scores between the videoconference and in-person SAD groups. Interaction effects between scores and times were also examined.
Partial eta-squared and Cohen’s d were used to calculate effect sizes for the DASS-21 and GCS-R within and between all three treatment groups, and for the SPIN within and between both the SAD groups. A series of independent samples t-tests and Pearson chi-squares were also performed to assess differences between groups’ demographics. An alpha value of .05 was used for statistical analyses, and all analyses were conducted using version 27 of IBM SPSS Statistics.
Results
Descriptive statistics
Descriptive statistics for demographic variables are provided in Table 1. Chi-square and t-test analyses revealed no significant differences between groups’ average age (MD between SAD-IP and SAD-VC=.048 years, p=.986; MD between SAD-IP and OAD-VC=4.30 years, p=.100; MD between SAD-VC and OAD-VC=4.25 years, p=.061), genders (χ2(6,N=174)=8.18, p=.226), and ethnicities (χ2(2,N=142)=1.5, p=.469). Analyses did, however, reveal significant differences between groups’ relationship statuses (χ2(2,N=146)=16.4, p<.001), where the in-person SAD group had a significantly larger single population and the videoconference other anxiety disorders group had significantly more individuals in a relationship. There were also differences in employment statuses (χ2(2,N=147)=10.7, p=.005), where the in-person SAD group had a significantly larger unemployed population than the other groups, and education levels (χ2(2,N=143)=18.3, p<.001), where the in-person SAD group had a significantly larger population who did not graduate college and the videoconference other anxiety disorders group had a significantly larger college graduate population.
Analyses
Means and standard deviations for all measures for all three treatment groups, as well as the results of the repeated measures ANOVA comparing treatment outcomes and group cohesion scores within and between all three treatment groups are shown in Table 2.
Treatment outcome and group cohesion means, standard deviations, and ANOVA comparisons between in-person SAD, videoconference SAD, and videoconference OAD groups
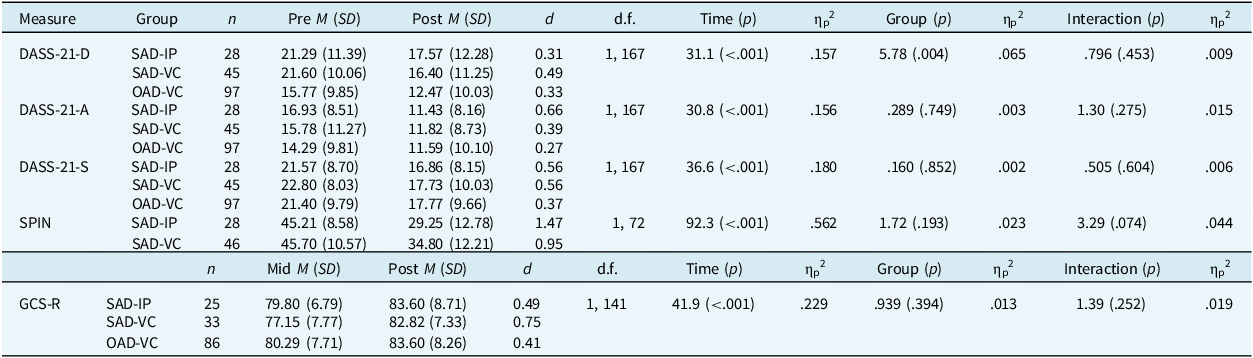
ANOVA, analysis of variance; SAD, social anxiety disorder; OAD, other anxiety disorders; n, sample size; M, mean; SD, standard deviation; d, Cohen’s d; d.f., degrees of freedom; ηp 2, partial eta squared; DASS-21-D, depression anxiety stress scales depression subscale; DASS-21-A, depression anxiety stress scales anxiety subscale; DASS-21-S, depression anxiety stress scales stress subscale; SPIN, social phobia inventory; GCS-R, group cohesion scale revised; IP, in-person; VC, videoconference.
No significant main effect of group was found for the GCS-R, suggesting that the videoconference CBGT for SAD group reported similar cohesion to both comparison groups at mid-treatment and post-treatment. Significant main effects of time were found for the GCS-R, F 1,141=41.9, p<.001, ηp 2=.229, the SPIN, F 1,72=92.3, p<.001, ηp 2=.562, the DASS-21-D, F 1,167=31.1, p<.001, ηp 2=.157, the DASS-21-A, F 1,167=30.8, p<.001, ηp 2=.156, and the DASS-21-S, F 1,167=36.6, p<.001, ηp 2=.180, indicating that cohesion increased and symptoms decreased over time regardless of treatment condition (see Fig. 2) with effect sizes ranging from small to large across variables (see Table 2 for details).
Graphs of in-person SAD, videoconference SAD, and videoconference other anxiety and related disorders groups’ pre-treatment and post-treatment mean DASS-21-D, DASS-21-A, DASS-21-S, SPIN, and GCS-R scores. SAD, social anxiety disorder; DASS-21-D, depression anxiety stress scales depression subscale; DASS-21-A, depression anxiety stress scales anxiety subscale; DASS-21-S, depression anxiety stress scales stress subscale; SPIN, social phobia inventory; GCS-R, group cohesion scale revised. Graph bars represent standard error.
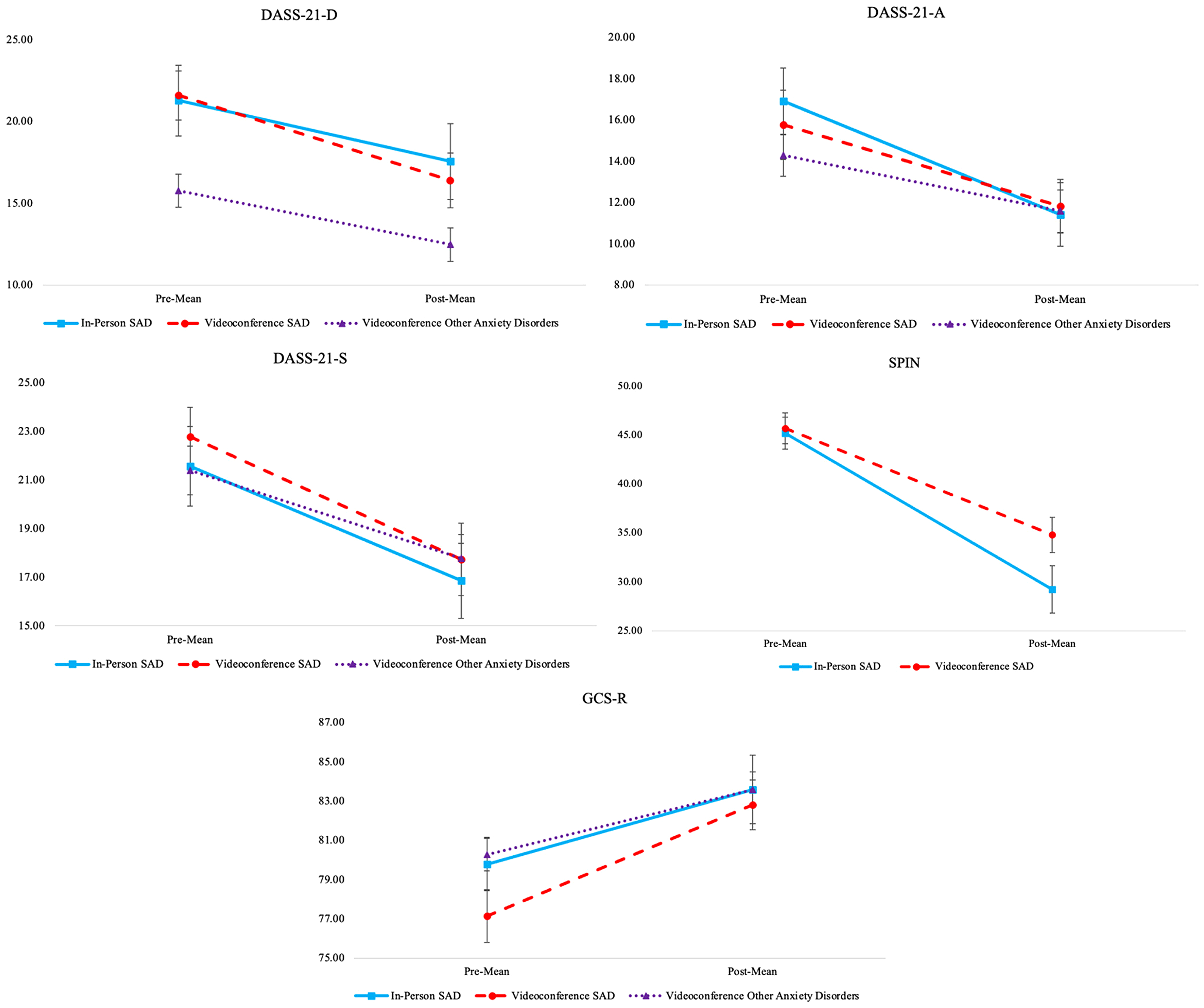
A significant main effect of group with a medium effect size was found for the DASS-21-D, F 1,167=5.78, p=.004, ηp 2=.065, indicating that the videoconference other anxiety and related disorders group had lower depressive symptoms at both pre-and post-treatment compared with both SAD groups (see Fig. 2), which was an incidental finding not included in our hypotheses.
Power
Given that the present study used retrospectively collected data, a priori power analyses were precluded. Instead, post-hoc power analyses were completed using G*Power for the primary study outcomes (interaction effects on the DASS-21-D, DASS-21-A, DASS-21-S, SPIN, and GCS-R). Analyses confirmed that there was sufficient power to detect interaction effects on these measures (α=0.81–0.94), except for the DASS-21-S (α=0.49). As such, the results of the analysis for the DASS-21-S should be interpreted with caution.
Discussion
The present study compared group cohesion development and symptom change between videoconference CBGT for SAD and both in-person CBGT for SAD and videoconference CBGT for other anxiety disorders. As hypothesized, results demonstrated that group cohesion increased and symptoms decreased over the course of treatment for all groups. Contrary to our hypothesis, results revealed no significant difference in mid- or post-treatment group cohesion between groups.
Symptom findings suggest that videoconference was a successful mode of treatment delivery for social anxiety disorder and other anxiety disorder-specific CBT groups, which adds to a small but growing literature on the efficacy of videoconference CBGT for anxiety disorders (Milosevic et al., Reference Milosevic, Cameron, Milanovic, McCabe and Rowa2022; Nauphal et al., (Reference Nauphal, Swetlitz, Smith and Rosellini2021). Symptom reductions were not only statistically significant but also clinically meaningful. Although residual symptoms remained at post-treatment, mean DASS-21 subscale scores changed from severe or moderate at pre-treatment to moderate or mild at post-treatment for all three treatment groups. Furthermore, although post-treatment mean SPIN scores for both SAD groups were above a widely used clinical SPIN cut-off score of 19 (Connor et al., Reference Connor, Davidson, Churchill, Sherwood and Weisler2000), they were either below or approaching 30, an alternative cut-off score used in clinical research where symptoms tend to be more severe than in community or undergraduate samples (Moscovitch et al., Reference Moscovitch, Gavric, Merrifield, Bielak and Moscovitch2011; Moser et al., Reference Moser, Hajcak, Huppert, Foa and Simons2008). Along with large effect sizes on the SPIN and small to medium effect sizes on the DASS-21 subscales, it appears that participants experienced meaningful clinical change in all three treatment groups. The finding that group cohesion develops similarly in videoconference and in-person CBGT for SAD, although in contrast to Lopez et al. (Reference Lopez, Rothberg, Reaser, Schwenk and Griffin2020), strengthens support for the use of videoconference treatment with respect to this aspect of group process and aligns with pilot work by Arrow et al. (Reference Arrow, Yap and Chester2021) and Nauphal et al. (Reference Nauphal, Swetlitz, Smith and Rosellini2021). Although videoconference CBGT for SAD may involve unique connection-building barriers, results found that levels of reported cohesion were similar to both comparison groups. It is possible that the barriers were counteracted by unique connection-building enablers, therefore resulting in similar group cohesion development. For example, therapists, or even participants, may work harder to generate group connection in videoconference treatment groups (e.g. spending increased time drawing similarities between group member examples, ice breakers) because they perceive it to be a more difficult environment in which to do so. Additionally, because participants are attending treatment from their homes or other personal environments (e.g. office, car) they may experience a greater sense of comfort during sessions than those attending treatment in-person at a clinic, leaving them more at ease and therefore more capable of connecting with other group members. Due to the growing popularity of videoconference-hosted social interactions participants may already be similarly proficient in building and maintaining relationships over video as they are in person and are thus not especially deterred by interactions with limited body language and eye contact, even for those with SAD. Furthermore, study participants in the videoconference groups completed treatment during earlier phases of the COVID-19 pandemic, in which they may have been experiencing intense isolation and loneliness, causing the relative value of social bonds to increase, leading to extra effort put forth to bond with fellow CBGT members. Future research investigating how group cohesion may be uniquely developed in videoconference CBGT compared with in-person CBGT, as well as how group cohesion and other factors (e.g. homework engagement, working alliance, attendance) specifically contribute to therapeutic outcomes in videoconference CBGT, is necessary to build our confidence in, and improve the delivery of videoconference CBGT for anxiety and related disorders.
An incidental finding in the present study was that both the in-person and videoconference SAD groups experienced greater pre- and post-treatment depressive symptoms compared with the videoconference other anxiety and related disorders group. Research suggests that major depressive disorder (MDD) is a common co-morbidity in SAD, and SAD symptoms tend to precede depressive symptoms and are associated with a much greater risk of developing MDD (Kalin, Reference Kalin2020; Koyuncu et al., Reference Koyuncu, İnce, Ertekin and Tükel2019). The connection between SAD and associated depressive symptoms may be even stronger than that for other anxiety disorders. On the other hand, this finding could reflect something unique about our sample, with ancillary depressive symptoms perhaps increasing the chance that individuals with SAD seek treatment. Further research on this relationship is necessary.
Anecdotally, clinicians who led the videoconference groups shared observations about the perceived advantages and challenges presented by videoconference-delivered treatment, which we believe are vital to this discussion and to advising future studies. With respect to advantages, some clinicians noted that participants tended to address one another by name more frequently in videoconference treatment, which likely resulted from members’ names being clearly displayed on screen throughout sessions. Also, clinicians remarked that the use of virtual breakout rooms for individual exposures and experiments improved efficiency in therapy sessions. In terms of disadvantages, clinicians inferred that the lack of pre- and post-session transition time spent having individual conversations with fellow participants in a physical waiting room environment may mean that videoconference groups are missing out on valuable opportunities to bond with one another. Clinicians also observed some clients engaging in screen-based distractions (e.g. playing a video game, checking their email) during sessions. Finally, as noted previously, it can be difficult for more than one person to speak and be heard at one time when using videoconference software. As a result, group sessions may have felt more formal, and when one member of the group was sharing, other participants could only reinforce by nodding their heads or using gestures, rather than verbally reinforcing as is commonly used during in-person sessions. As the videoconference-delivered group therapy literature grows, considering observations such as these will be an important part of deepening our understanding of the mechanisms impacting this mode of treatment delivery.
This study had some limitations. Most importantly, the in-person CBGT for SAD group completed treatment before the COVID-19 pandemic, whereas the videoconference groups completed treatment during the COVID-19 pandemic. Unfortunately, randomization was not possible because in-person CBGT was not occurring at our clinic at the time of this study’s videoconference data collection and vice versa. Given that participants were not randomly assigned to either videoconference or in-person CBGT for SAD, uncontrolled differences between these groups are possible. For example, participants beginning treatment during the COVID-19 pandemic may be experiencing less severe SAD symptoms than the range of patients typically attending our clinic because individuals with very severe SAD symptoms may have been accommodated by the pandemic’s isolation requirements and were therefore less likely to seek treatment during the study period. Future research will be necessary to determine if our findings hold true outside of the context of the COVID-19 pandemic.
Retrospectively collected data also prevented us from using a standardized diagnostic assessment method. It is also important to note that the sample in the present study was noticeably homogenous, consisting of predominantly white, educated, female participants, and analyses revealed some significant differences between the groups’ demographics. Future research with diverse participants will increase generalizability. The findings of this study should also be interpreted cautiously considering the small sample size of the in-person SAD group.
The poor rate of questionnaire completion across groups as well as the differences found in the number of completers versus non-completers between groups is another limitation. It is possible that the final completer sample used for analyses was biased towards those who were more motivated to improve their symptoms or bond with their treatment group, thus skewing study findings. Additionally, the possibility that some therapists – or specific behaviours – may be more effective at facilitating group cohesion or symptom change than others (Bryde Christensen et al., Reference Bryde Christensen, Riis, Wahrén, Reinholt, Skov, Poulsen, Simonsen and Arnfred2022) may also have affected study findings. When planning future research on this topic, attention should be given to addressing these limitations a priori.
Future research could include a follow-up period, which was regrettably beyond the scope of our current study but could provide insights into the long-term effectiveness of videoconference CBGT. Another intriguing avenue for future investigation would involve employing structural equation modeling to enhance our understanding of the interplay between symptom improvement and group cohesion. A prospective randomized controlled trial with a large sample size and data collection at more than two time points would enable these analyses to yield robust findings that comprehensively delineate the role of group cohesion in CBGT.
Results from the present study demonstrate that participation in videoconference CBGT leads to similar reductions in disorder-related symptoms and development of group cohesion when compared with in-person CBGT for SAD and videoconference CBGT for other anxiety disorders. These findings can increase confidence in the efficacy of videoconference CBGT for SAD and encourage widespread dissemination of this mode of treatment.
Data availability statement
The anonymous datasets generated during and/or analysed during the current study can be made available from the corresponding author upon reasonable request.
Acknowledgements
We wish to express our gratitude to Ashleigh Elcock for her assistance with data collection.
Author contributions
Isabel Shapiro: Conceptualization (equal), Data curation (lead), Formal analysis (lead), Investigation (lead), Methodology (equal), Project administration (lead), Writing - original draft (lead), Writing - review & editing (equal); Jenna Boyd: Conceptualization (equal), Formal analysis (supporting), Investigation (supporting), Methodology (equal), Project administration (supporting), Supervision (supporting), Writing - review & editing (equal); Randi McCabe: Project administration (supporting), Resources (lead); Karen Rowa: Conceptualization (equal), Formal analysis (supporting), Investigation (supporting), Methodology (equal), Project administration (supporting), Supervision (lead), Writing - review & editing (equal).
Financial support
The authors of this manuscript received no financial support for the research, authorship, or publication of this article.
Competing interests
The authors declare that they have no known competing interests regarding the research, authorship, or publication of this article.
Ethical standards
This research was reviewed by the Hamilton Integrated Research Ethics Board (HiREB) and received approval (07-2955). Participants provided informed consent to the inclusion of their demographic and clinical information in a research database used for retrospective studies at the ATRC. Authors abided by the Ethical Principles of Psychologists set out by the BABCP and BPS.





 Open access
Open access
Comments
No Comments have been published for this article.