


Introduction
To ensure optimal utilization of the pharmaceutical budget amidst constrained healthcare resources, monitoring the effectiveness and performance of commercialized drugs is imperative. This is particularly relevant for rare disease therapies that have the potential to improve morbidity and mortality but often enter the market with high costs and limited clinical evidence. This is usually due to small patient populations, disease heterogeneity, and a lack of adequate alternative treatment (1–Reference Blonda, Barcina Lacosta, Toumi and Simoens5).
Overview of the procedure for the HTA/reimbursement of rare disease therapies in Belgium.
In Belgium, a decision on the reimbursement of a health technology must be reached within 180 days following a manufacturer’s application (6). Throughout this process, technical experts from the National Institute for Health and Disability Insurance (NIHDI) prepare health technology assessment (HTA) reports at key milestones (day 60, day 90, day 120, and the final proposal on day 150) based on the manufacturer’s dossier and the conclusions of the Drug Reimbursement Committee (Commissie Tegemoetkoming Geneesmiddelen/Commission de Remboursement des Médicaments [CTG/CRM]). These reports should be publicly accessible along with a letter detailing the Minister of Health’s final decision, to ensure transparency of the process (Reference Le Polain, Franken, Koopmanschap and Cleemput7;Reference Neyt, Gerkens and San Miguel8).
To address affordability concerns and mitigate the financial risk of reimbursing high-priced therapies with uncertain benefits, many health systems – including Belgium – increasingly employ managed entry agreements (MEAs). MEAs enable temporary and conditional reimbursement, coupled with confidential discounts and requirements for additional clinical or real-world evidence (Reference Neyt, Gerkens and San Miguel8;Reference Moes, Houwaart, Delnoij and Horstman9). However, their use has raised concerns. Several studies have highlighted that MEAs often fail to meet their contract terms, leaving clinical uncertainties unresolved and price negotiations incomplete (Reference Pontes, Zara and Torrent-Farnell10–Reference Trotta, Maria, Aurora and Cangini14).
In Belgium, MEA use has expanded rapidly, increasing from 13 new MEAs concluded in 2013 to 43 new MEAs concluded in 2023, with a cumulative total of over 183 MEAs established between 2013 and 2023 (15). MEAs are typically introduced when the Belgian Drug Reimbursement Committee (Commissie Tegemoetkoming Geneesmiddelen/Commission de Remboursement des Médicaments [CTG/CRG]) cannot reach consensus on reimbursement conditions at the end of the appraisal process (see Box 1).
In such cases, the applicant negotiates confidentially with the Minister of Social Affairs and Public Health to define the terms of the MEA. These agreements usually last up to 3 years, after which the agreement is either extended or a health technology reassessment (HTR) is performed. If evidence remains insufficient to justify continued reimbursement at the negotiated price, decision-makers may negotiate a new agreement – for example, including larger (confidential) discounts on the list price or revising requirements for evidence generation. Alternatively, the CTG/CRM may recommend that the Ministry of Health (MoH) discontinue the conditional reimbursement through disinvestment (16;Reference Makady, van Veelen and de Boer17). However, this option is less common due to the controversial nature of disinvesting in treatments for rare diseases, which are often associated with a large unmet need.
Disinvestment can be passive, for example, by restricting reimbursement to certain subgroups with demonstrated benefit (Reference Parkinson, Sermet and Clement18). Examples include the implementation of subgroup restrictions for ineffective anti-Alzheimer medications in France and Belgium (19;Reference Figaro20) and the restricted prescribing of duloxetine in Sweden due to concerns over its value in practice following the availability of generic venlafaxine (Reference Godman, Persson and Miranda21). However, this approach may be less suitable for orphan drugs, as patients often have no effective alternatives. Another form of passive disinvestment is the so-called “extinction scenario,” in which current (subgroups of) patients are allowed to continue treatment, but no new patients are initiated. In Belgium, this approach was applied to decitabine for acute myeloid leukemia patients with 20–30 percent blasts (22).
An alternative strategy is active disinvestment (or delisting), which involves the complete withdrawal of reimbursement for a disease therapy, requiring patients to pay the full cost if they wish to continue treatment. In Belgium, passive approaches are more common for rare diseases, whereas active disinvestment is avoided due to the lack of alternatives and the emotive nature of rare diseases (Reference van de Wetering, van Exel and Brouwer23). A notable example occurred in the Netherlands, when the College of Health Insurers recommended removing agalsidase alfa and alglucosidase alfa – used to treat Fabry and Pompe disease, respectively – from the basic reimbursement package. Despite an estimated incremental cost-effectiveness ratio of €15 million for alglucosidase alfa, the recommendation faced strong resistance from patients and physicians, and disinvestment plans were ultimately halted (Reference Zorginstituut24–Reference Simoens, Picavet, Dooms, Cassiman and Morel26).
Nonetheless, as healthcare systems in high-income countries face growing financial pressures – driven in part by aging populations – active disinvestment of orphan drugs may become inevitable. This is to ensure the efficient and equitable allocation of resources to treatments that provide demonstrable value.
Previous research highlights that effective communication with stakeholders – including healthcare providers, payers, patients, and industry – is critical for successful disinvestment (Reference Maloney, Schwartz, O’Reilly and Levine27;Reference Rotteveel, Lambooij and van de Rijt28). In Belgium, a structured communication procedure exists only for ultra-rare diseases reimbursed on a case-by-case basis (29). In these cases, an Orphan Drug College provides an opinion on the individual prescription and reimbursement of the orphan drug (Reference Denis, Simoens, Fostier, Mergaert and Cleemput30). This College is composed of physicians and specialists knowledgeable about a specific rare disease (treatable by the orphan drug) and advisory physicians who are members of the reimbursement committee (CTG/CRM) at the National Institute for Health and Disability Insurance (NIHDI). They first deliver their opinion to the advising physician of the health insurance fund, who then informs the concerned patient. For other rare disease therapies, communication is often delayed, informal, or incomplete, leading to confusion and, at times, public controversy.
To our knowledge, this study develops the first structured, context-specific communication roadmap for the disinvestment of rare disease therapies. This roadmap is intended for situations in which the payer determines that the added value of a therapy – compared to the standard of care – has not been sufficiently demonstrated (or is considered insufficient relative to its additional cost). It seeks to address the clinical, financial, ethical, psychological, and social dimensions of orphan drug disinvestment. Moreover, it provides practical tools to guide communication with all stakeholders, especially patients and the wider public. While rooted in the Belgian system, the proposed principles and tools are designed to be adaptable to other jurisdictions with similar challenges in orphan drug disinvestment.
Methods
Study design
This qualitative, exploratory study used stakeholder engagement to develop a structured communication roadmap for the disinvestment of rare disease therapies. We applied grounded theory – an inductive methodology that facilitates the creation of frameworks based on collected data (Reference Corbin and Strauss31) – to capture actionable insights from expert knowledge. Grounded theory was chosen for its suitability in generating practical guidance for complex and sensitive decision-making contexts, making it highly suited to the study’s objectives.
Study conduct
An advisory board was convened to guide the roadmap’s development. To prepare for the board meetings, we conducted a targeted literature review of disinvestment cases and strategies in healthcare, with a focus on rare disease therapies. Relevant peer-reviewed studies, legal and policy texts, and gray literature were identified through targeted searches in PubMed, Google Scholar, and snowballing. Search terms included synonyms for “disinvestment,” “delisting,” “discontinuation,” “reassessment,” and “defunding.” While not systematic, this review provided essential foundations to inform the discussion points for the meetings.
Three advisory board meetings (in Dutch) were held on 14 December 2022 and 22 and 30 May 2023. Feedback and insights from each meeting were integrated into subsequent discussions. The first meeting took place in person at the KU Leuven Department of Pharmaceutical and Pharmacological Sciences. The final two meetings were teleconferences to accommodate experts’ schedules. Figure 1 outlines the roadmap development process and the scope of each meeting.
Overview of the roadmap development process and the scope of each meeting. Numbers in superscript indicate that the same expert participated in multiple meetings.

The first meeting identified critical elements and values for effectively communicating disinvestment decisions to rare disease patients. Moreover, it determined which stakeholders should be involved, and at which stages, in developing and disseminating communication materials. Building on the results of this first meeting, a preliminary set of recommendations and a communication flow were developed and shared with participants ahead of the second advisory board meeting.
The second meeting produced a preliminary roadmap that was tested in three fictional cases. The third meeting validated the roadmap’s feasibility and practicality by discussing it in the context of two additional cases.
Based on these discussions, we created a five-step communication roadmap with supportive communication materials (see Supplementary Tables S1–S3), which include:
-
1) A template for the lay summary of the HTR report (Supplementary Table S2), modeled after the health technology assessment (HTA) reports from the Dutch Zorginstituut Nederland (ZIN) (Reference Nederland32), the National Institute for Health and Clinical Excellence (NICE) (33), and the German Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen (34).
-
2) A template for letters communicating the disinvestment decision to patients and the wider public (Supplementary Table S3). It defines components to be included during, for example, a patient consultation, a press release, or the website of the national health authority.
-
3) A roles and responsibilities form for defining deadlines and stakeholders’ responsibilities (identify, inform, communicate, and publish; see Supplementary Table S3).
Participants
We purposively sampled experts with experience in the Belgian (orphan) drug reimbursement process (Reference Palinkas, Horwitz and Green35). Potential participants were identified through the investigators’ professional networks, scientific publications, and official websites or social media (e.g., LinkedIn) of national healthcare authorities. Experts were invited via email between 15 October and 30 November 2022.
The final advisory board included representatives from academia, health insurance funds, clinical practice, and the CTG/CRM. Recruitment ensured at least one representative from each stakeholder group and geographic diversity across Belgium.
Data analysis
The focus groups were moderated by the principal researchers and transcribed verbatim by KU Leuven-affiliated coworkers. We followed the Qualitative Analysis Guide of Leuven to guide the process of qualitative data analysis (Reference Dierckx de Casterle, Gastmans, Bryon and Denier36). The same researchers analyzed the transcripts independently, by performing a two-stage analysis.
In the coding stage, a predefined (complementary deductive) coding framework, based on the specific study topics, was assigned to various text fragments. Additionally, inductive open coding was applied for emerging themes such as ethical values and prerequisites for disinvestment communication. Coding was performed in NVivo 1.7 by both researchers independently.
In the synthesis stage, the researchers compared their analyses to develop an overarching code structure, which was used to detail the roadmap steps. The two principal researchers then drafted the roles and responsibilities guide, lay summary template, and communication letter template. The full research team reviewed and validated the roadmap, principles, guides, and recommendations.
Ethical considerations
The research protocol was approved by the Ethical Committee Research University Hospitals Leuven (14/10/2022, S66927). All participants provided written informed consent. Participant anonymity was maintained unless explicit permission for attribution was given. Data were handled confidentially throughout the study.
Results
Participant characteristics
Nine experts (four females and five males) participated in the advisory board meetings, of whom four attended sessions twice (see Figure 1). All were Belgian senior-level professionals with >10 years of experience in their respective fields, spanning academia, health insurance funds, clinical practice, and prior roles at the NIHDI (including the CTG/CRM).
Principles for a successful communication roadmap
During the meetings, experts identified several bottlenecks that could hinder a smooth implementation of a communication roadmap – such as media controversies and inconsistent messaging. These challenges were synthesized into key principles essential for ensuring feasibility and effectiveness (see Table 1).
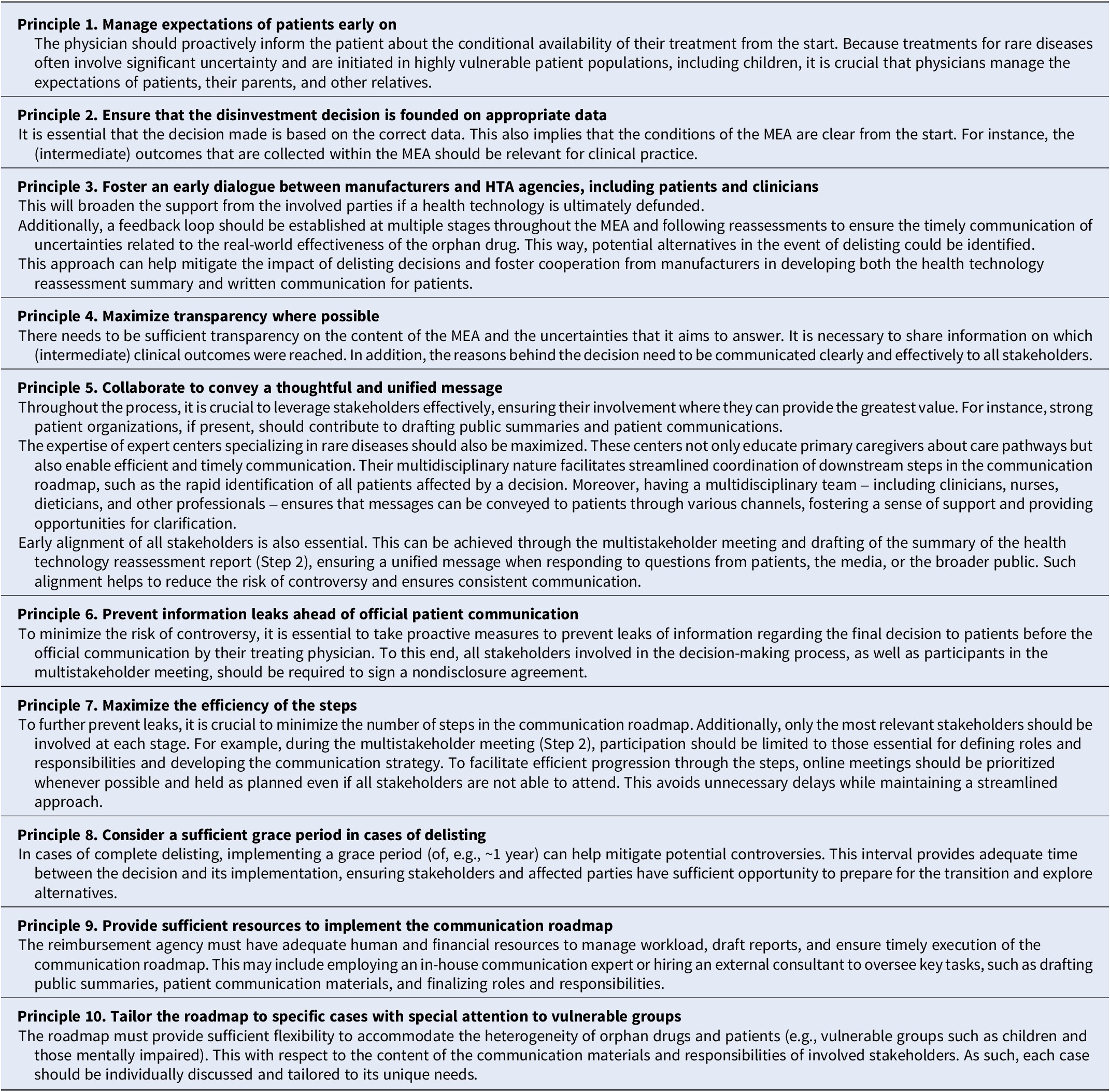
Key principles for an effective communication roadmap for the disinvestment of orphan drugs

Abbreviations: HTA, health technology assessment; MEA, managed entry agreement.
Currently, Belgium has no formal system for communicating the disinvestment of a rare disease therapy that is conditionally or formally reimbursed by the NIHDI. Experts highlighted that clinicians often learn about such decisions informally or through delayed communication from manufacturers. Decision letters from the Minister of Health may provide only a brief rationale, often without a clear explanation of the evidence base. In some cases, patients first learn of a drug’s unavailability from their pharmacist.
The five-step communication roadmap
The roadmap (see Figure 2) presumes that the competent authority or MoH formally communicates a decision to withdraw reimbursement to the manufacturer. The roadmap also presumes that the disinvestment decision is evidence-based and appropriate and, therefore, solely focuses on how the decision should be communicated. While the timelines are specific to Belgium, the structure can be adapted to healthcare contexts of other jurisdictions.
The five-step disinvestment communication roadmap. Abbreviations: D, day; HTR, health technology reassessment; MoH, Minister of Health; NIHDI, National Institute for Health and Disability Insurance; RD, rare disease; T, time.

Step 1: prepare – compile the comprehensive HTR report
In Belgium, HTA reports are often available only upon formal request and may be difficult to interpret, even for those familiar with the process. The justifications provided in these reports are frequently unclear, lacking clarity in terms of language, scientific reasoning, and structure, which further complicates their accessibility and usability.
The first step is therefore to produce a publicly accessible HTR report that consolidates all relevant, nonconfidential evidence and clearly explains the reimbursement committee’s scientific conclusions. This report, prepared by NIHDI technical experts and tailored to the public, follows a format like the European Public Assessment Report of the European Medicines Agency (37), which avoids excessive technicality while maintaining sufficient detail. It aims to provide maximum clarity and transparency within the boundaries set by the confidentiality of CTG/CRM deliberations and price negotiations. Manufacturers may provide feedback on the draft. The compilation of this report should be completed within 3 days of initiating the procedure.
Step 2: discuss & complete – develop the public summary and communication guide
A NIHDI technical expert convenes a confidential multistakeholder meeting to prepare the communication to physicians, the patients, and the public. This step is best conducted as an online, rather than face-to-face, meeting to enable the earliest possible discussion. The goal of the meeting is to produce
-
(i) A public summary of the HTR report to the patient and public, including information on alternative treatment options (see guide for drafting the HTR report in Supplementary Table S1.
-
(ii) A detailed communication letter for patients and the public (see guide for drafting communication letters in Supplementary Table S2) and
-
(iii) A completed roles and responsibilities template, outlining actions, responsible stakeholders, and timelines for downstream communication and patient outreach (see template in Supplementary Table S3).
The NIHDI technical expert – who coordinates the meeting – invites participants via email or phone. All participants sign a nondisclosure agreement before the meeting to prevent premature leaks. The meeting requires the presence of various stakeholders, as detailed in Table 2.
Stakeholders involved in drafting the disinvestment communication and their roles

Abbreviations: NIHDI, National Institute for Health and Disability Insurance; CTG/CRM, Commissie Tegemoetkoming Geneesmiddelen/Commission de Remboursement des Médicaments; HTR, health technology reassessment.
The duration of this meeting can range from an hour to half a day, depending on the complexity of the arguments behind the decision and the characteristics of the patient group. The scientific writer finalizes the public summary within 1 day after the meeting; feedback from attendees and approval from the MoH (or delegate, if the MoH was absent during the meeting) should be obtained within 3 days. Final documents are circulated within 5 days of the meeting.
Step 3: inform – prepare relevant stakeholders for patient contact
The public summary and communication letter are shared with physicians responsible for informing patients, as well as with stakeholders who may be approached by patients (e.g., health insurance funds and hospital pharmacists). The clinical expert (e.g., physician from the expert center, Council of Rare Diseases of Functional Hospitals, or College for Genetics and Rare Diseases), who was present in the virtual meeting, informs the multidisciplinary team of the reference center, or, where not applicable, the treating physician. Simultaneously, the NIHDI technical expert informs health insurance funds, the hospital, and/or local pharmacists. These parties should, above all, avoid confusion by providing appropriate and consistent messaging to patients or referring them to their treating physician. This step runs in parallel with Step 4 and should be completed within 3 days of finalizing the public summary.
Step 4: communicate – inform affected patients
Depending on the size of the target population, different actors should be involved in personally communicating the message to the concerned patient(s). In case of disinvestment in the form of a cohort restriction, both patients who are already receiving therapy as well as de novo or formerly eligible patients – who will no longer be able to initiate the treatment – should be informed. Patients already receiving therapy will be able to continue therapy, contingent on signing a form specifying that the treatment is no longer recommended. The message must be delivered empathetically by a trusted person, clearly stating that the treatment is no longer effective or beneficial. It should also reassure the patient (and their caregivers or relatives) by discussing alternative treatments and providing room for dialogue. Initially, this message should be conveyed verbally, followed by the delivery of the public summary of the HTR report (see supplemental guide).
For patient numbers below 50, the message can be personally delivered during a consultation with their treating physician (and the broader multidisciplinary team), who is responsible for personally reaching out and inviting the patients for a consultation. However, for patient numbers larger than 50, it becomes logistically challenging to communicate the message to everyone in a timely manner. In this instance, the multidisciplinary team of the reference center and the patient organization, if professional and well-organized, may invite concerned patients to an explanatory session. This session could be hosted on a video conferencing platform provided by NIHDI, or physically in the respective reference center. If there is no reference center or patient organization available, health insurance funds could alternatively organize such a session, in conjunction with advising physicians (and treating physicians). This session should conclude with a message urging patients to reach out to their treating physician for more specific and detailed information and refer to the HTR report and public summary. This step should occur simultaneously with step 3 and be completed within 1 week of receiving the written documents conveying the disinvestment decision.
Step 5: publish – release public statement and supporting documents
NIHDI publishes an official public statement, together with the HTR report, the public summary, and a communication letter to the patient, on an accessible and user-friendly NIHDI webpage. The official statement is concise, factual, and written in nontechnical language, specifying the decision and effective date, the principal reasons for disinvestment in lay terms, and links to the full HTR report and the public summary.
The webpage should be modeled after best-practice examples from the ZIN (The Netherlands) and NICE (The United Kingdom and Wales) (Reference Nederland32;33). Simultaneously, the HTR report and letter to the patient are also shared with relevant patient organizations, national and regional agencies responsible national drug registration, pharmacovigilance and medical information provision – such as the Belgian Federal Agency for Medicines and Health Products and the Belgian Centre for Pharmacotherapeutic Information – and with other healthcare bodies likely to receive queries from clinicians or patients. A well-trained NIHDI spokesperson is appointed to answer any media questions regarding the decision, ensuring that all public messaging is consistent and accurate. Where possible, the timing of publication is coordinated so that patients receive the information directly from their treating physician prior to media reporting.
Discussion
Several publications have described frameworks for prioritizing healthcare interventions or low-value care for disinvestment, de-adoption, or de-implementation (Reference Parkinson, Sermet and Clement18;Reference Niven, Mrklas and Holodinsky38–Reference Kamaruzaman, Grieve and Wu43). However, to our knowledge, this paper is the first to present a comprehensive roadmap specifically for communicating the disinvestment of rare disease therapies after conditional reimbursement. A particular strength of the roadmap lies in the practical guides and templates – such as the guide for drafting the public summary of the HTR report (see Supplementary Table S1), the guide for drafting the communication to patients and the public (see Supplementary Table S2), and the roles and responsibilities template (see Supplementary Table S3). These were developed bottom-up by a multistakeholder advisory board, which included patient representatives. While the timelines and specific stakeholders identified in the roadmap (e.g., the Orphan Drug College and the Council of Rare Diseases of Functional Hospitals) are a projection specific to the Belgian context, the general principles (Table 1) and supporting tools are transferable to other high-income countries with similar healthcare systems.
We also believe that our roadmap could be extended beyond pharmaceutical products to high-cost drugs or other health technologies. For example, considering new European Union quality control regulations, which are believed to be so stringent that they may prompt manufacturers to withdraw certain (orphan) medical devices from the market, our roadmap could provide guidance for decision-makers to inform patients about such market withdrawals (Reference Westermark, Holm and Söderholm44;Reference Dooms45).
Principles underpinning a successful communication roadmap
Given the growing number of conditionally approved rare disease therapies and increasing concerns about the affordability of premium-priced biological medicines, there is a need for clear and transparent communication to patients and the public (Reference Godman, Hill and Simoens13). This study identified 10 basic principles for successful communication of a disinvestment decision. These principles are likely to be applicable to the disinvestment of other health technologies in high-income settings, given the methodology used to develop them.
First, our findings showed that the disinvestment process and its rationale must be structured, evidence-based, and transparent. These characteristics are consistently identified in the literature as key facilitators of successful disinvestment strategies (Reference Parkinson, Sermet and Clement18;Reference Maloney, Schwartz, O’Reilly and Levine27;Reference Niven, Mrklas and Holodinsky38;Reference Mayer and Nachtnebel39;Reference Walsh-Bailey, Tsai and Tabak42;Reference Elshaug, Watt, Mundy and Willis46–Reference Mitchell, Bowles, O’Brien, Bardoel and Haines52).
Second, fostering collaboration among key stakeholders – particularly clinicians and patients – is crucial for gaining acceptance of disinvestment decisions. Stakeholders should be engaged early and kept informed throughout the reassessment that precedes disinvestment (Reference Parkinson, Sermet and Clement18;Reference Niven, Mrklas and Holodinsky38;Reference Mayer and Nachtnebel39;Reference Walsh-Bailey, Tsai and Tabak42;Reference Elshaug, Watt, Mundy and Willis46;Reference Soril, Niven, Esmail, Noseworthy and Clement48;Reference Embrett, Randall, Lavis and Dion50;Reference Esandi, Gutiérrez-Ibarluzea, Ibargoyen-Roteta and Godman51). Patient engagement is essential to improve the acceptability of the decision (Reference Polisena, Clifford and Elshaug47;Reference de Lemos, Guerra Júnior and Santos49). In the Belgian context, rare disease expertise centers play an essential role. Although there are currently eight such centers (53), they do not cover all rare diseases. Expanding their role and coverage, possibly by centralizing expertise per therapeutic area and formalizing responsibilities of key parties involved, could enhance the efficiency of communication and stakeholder engagement. Such approaches would facilitate timely inclusion of all relevant parties, reduce procedural delays, and minimize information leaks that could fuel public controversy.
Third, a communication roadmap should be practical, context-specific (Reference Elshaug, Watt, Mundy and Willis46), and customized to the key parties affected by the decision (Reference Mayer and Nachtnebel39;Reference Esmail, Hanson, Holroyd-Leduc, Niven and Clement41). While we tested the feasibility and applicability of our roadmap in fictional cases, the heterogeneity of rare diseases requires flexible implementation of the roadmap and case-by-case adjustments. For example, the roles and responsibilities template (see Supplementary Table S3) should be expanded as needed to include parties essential for specific cases. Future adaptations of the roadmap should also incorporate tailored communication strategies for vulnerable populations, such as children and individuals with cognitive impairments. In such cases, communication might be directed first to their parents or primary caregivers.
Finally, a media response strategy should be built into the roadmap from the outset of conditional reimbursement. Highly publicized disinvestment cases – especially those involving treatments with no adequate alternatives – can generate strong media and public reactions. While healthcare payers typically appoint a spokesperson, our guides (see Supplementary Tables S1–S3) help ensure that the message is clear and transparent, and that all stakeholders are prepared to respond consistently to media queries.
Limitations
This study has several limitations. We aimed to include experts from countries with relevant disinvestment experience and healthcare systems similar to Belgium. Of the 44 invited experts, eight were from France, six from the Netherlands, and four from the Walloon region. However, due to scheduling constraints in the post-pandemic period, only Belgian experts participated. Similarly, although we initially had commitments from five experts per advisory board meeting, last-minute cancellations resulted in smaller group discussions. Despite this, all major stakeholder groups were represented, and the risk of Flemish overrepresentation was mitigated by including experts active in national-level patient organizations and healthcare decision-making. Furthermore, while the roadmap was developed with consideration for vulnerable populations, time constraints during meetings prevented discussion of specific cases involving these groups. Given the exploratory nature of this study, future research should expand the advisory board to include a broader range of national and international experts and pilot the roadmap in real-world disinvestment cases.
Conclusion
This study provides a comprehensive roadmap for communicating the withdrawal of funding for rare disease therapies after conditional reimbursement. It also identifies core principles essential for effective communication of disinvestment decisions. Although designed for the Belgian context, the roadmap’s principles and tools can be adapted to other jurisdictions. By applying evidence-based, transparent, collaborative, and adaptable approaches, policymakers can improve the communication of disinvestment decisions, ultimately benefiting patients, clinicians, and the public.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/S0266462326103444.
Acknowledgments
The authors would like to thank all advisory board members for their time, insights, and constructive feedback throughout the development of the communication roadmap. The authors are especially grateful to the patient representatives for sharing their experiences and perspectives, which were invaluable to ensuring the patient-centered nature of the roadmap. The authors would also like to thank Marc Dooms for his valuable insights and contributions throughout the entire study process, and Egbert de Groot (ZIN) and Beth (NICE) for sharing useful links on their HTA scientific reports and communication guidelines.
Author contribution
KA, AB, and SS conceived and designed the study. KA and AB led the design of the roadmap, coordinated the multistakeholder advisory board meetings, and performed the primary data collection and analysis. BG provided expertise on disinvestment practices. SS, IH, KC, and YD contributed to the study design, data interpretation, and critical revision of the manuscript. All authors approved the final version for submission.
Funding statement
This research was funded by the Scientific Research Foundation Flanders (FWO) (grant number G0B9819N).
Competing interests
The authors declare none.






 Open access
Open access