


Introduction
Body dysmorphic disorder (BDD) is a serious and often debilitating condition characterised by an excessive pre-occupation with perceived flaws in physical appearance that are typically unobservable to others (American Psychiatric Association, 2013; World Health Organization, 2022). This leads to intense anxiety, self-disgust and shame, which sufferers attempt to neutralise by engaging in time-consuming repetitive behaviours often aiming at checking, concealing or correcting their perceived flaws (American Psychiatric Association, 2013; World Health Organization, 2022). Although not widely recognised, BDD affects approximately 2% of adolescents and adults at any point in time (Krebs et al., Reference Krebs, Clark, Ford and Stringaris2025; Veale et al., Reference Veale, Gledhill, Christodoulou and Hodsoll2016), equating to around 1.2 million people in the United Kingdom (UK). This means that BDD is at least as prevalent as many related conditions that receive greater clinical attention, such as obsessive-compulsive disorder (OCD), which has an estimated prevalence of 1–2% (Torres et al., Reference Torres, Prince, Bebbington, Bhugra, Brugha, Farrell and Singleton2006; Ruscio et al., Reference Ruscio, Stein, Chiu and Kessler2010). BDD is associated with substantial functional impairment including impoverished relationships, social isolation, school absenteeism, and unemployment (Phillips et al., Reference Phillips, Menard, Fay and Pagano2005; Rautio et al., Reference Rautio, Jassi, Krebs, Andrén, Monzani, Gumpert, Lewis, Peile, Sevilla-Cermeño, Jansson-Fröjmark, Lundgren, Hillborg, Silverberg-Morse, Clark, Fernández de la Cruz and Mataix-Cols2020). The disorder has also been shown to be associated with poorer mental health-related quality of life than depression, bipolar disorder, and schizophrenia (Phillips et al., Reference Phillips, Menard, Fay and Pagano2005), and an estimated one in four people with BDD attempt suicide (Angelakis et al., Reference Angelakis, Gooding and Panagioti2016). Without effective treatment, BDD typically persists and often worsens over time. This is concerning, not least since longer duration of illness is associated with poorer prognosis including a lower likelihood of recovery and an elevated risk of suicide attempts (Bjornsson et al., Reference Bjornsson, Didie, Grant, Menard, Stalker and Phillips2013; Phillips et al., Reference Phillips, Menard, Quinn, Didie and Stout2013).
Effective psychological treatments exist for BDD, particularly specifically tailored cognitive behaviour therapy (CBT) (Zhao et al., Reference Zhao, Guo, Bo, Feng and Zhao2024). CBT for BDD is associated with large effects sizes relative to waitlist control (Harrison et al., Reference Harrison, de la Cruz, Enander, Radua and Mataix-Cols2016) and active comparators such as anxiety management (Veale et al., Reference Veale, Anson, Miles, Pieta, Costa and Ellison2014). However, this treatment is rarely available and in practice BDD frequently goes undiagnosed and untreated, with only a small minority of sufferers receiving evidence-based care. Survey-based studies show that only about 15% of those with BDD report having received a formal diagnosis (Schulte et al., Reference Schulte, Schulz, Wilhem and Buhlmann2020) or evidence-based treatment (McCausland et al., Reference McCausland, Paparo and Wootton2021), and this is likely to be an over-estimate given sampling bias. Recent studies utilising health record data indicate that only 0.03–0.08% of cases within mental health services are diagnosed with BDD (Addison et al., Reference Addison, James, Borschmann, Costa, Jassi and Krebs2024; Olaomi et al., Reference Olaomi, Khenechukwu, Udegbe, Uwumiro, Okafor, Obijuru, Yayehyirad and Opeyemi2024; Rautio et al., Reference Rautio, Isomura, Rück, Lichtestein, Kuja-Halkla, Larsson, Chang, D’Onofrio, Brikell, Sidorchuck, Mataix-Cols and Férnandez2024). This is strikingly lower than the estimated prevalence of 6–7% in these settings (McGrath et al., Reference McGrath, Oey and McDonald2023; Veale et al., Reference Veale, Gledhill, Christodoulou and Hodsoll2016), suggesting considerable under-diagnosis.
Multiple factors contribute to the under-diagnosis and under-treatment of BDD, including individual factors such as shame and limited insight, as well as systemic barriers such as limited resources in services and a shortage of clinical expertise (Marques et al., Reference Marques, Weingarden, Leblanc and Wilhelm2011; Schulte et al., Reference Schulte, Schulz, Wilhem and Buhlmann2020). A critical issue, as highlighted in a recent UK parliamentary inquiry (Health and Social Care Committee, 2022), is the lack of adequate training and education on BDD among mental health professionals. This knowledge gap may result in clinicians overlooking BDD symptoms or failing to ask targeted screening questions, which is particularly problematic in BDD given that most individuals do not disclose their symptoms unless directly asked (Veale et al., Reference Veale, Akyüz and Hodsoll2015). Consequently, BDD is frequently misdiagnosed as other conditions such as social anxiety disorder or depression, leading to inappropriate or ineffective treatment.
To quantify this issue, the current study aimed to examine the extent and nature of BDD training currently provided to mental health practitioners enrolled on professional psychological therapy courses in the UK. Specifically, we sought to assess the frequency, content, and perceived barriers to BDD training. To contextualise findings, we compared BDD training with that on OCD, a related condition with comparable prevalence and impact. We hypothesised that BDD would be less frequently and extensively covered in training than OCD.
Method
Design
Data were collected via a survey circulated to all UK-based Doctorate in Clinical Psychology (DClinPsy) programmes (n=32) and all MSc and Postgraduate Diploma (PgDip) in Cognitive Behaviour Therapy for Adults courses, collectively referred to as PgDip hereafter (n=30). The latter is the formal qualification for High Intensity Therapists in NHS Talking Therapies (NHS TTad), the largest provider of psychological therapies in England. The DClinPsy and PgDip courses were selected because together they train the majority of psychological therapists in the UK (estimated as over 2000 clinicians per year, combined).
Measure
The survey was delivered online via Qualtrics. The survey asked courses to report whether they provided training on BDD (yes/no), how much time was dedicated to BDD training (less than half a day, half a day, a full day, more than a full day), the format of delivery (didactic lecture, skills-based workshop, seminars, other), and the topics covered (assessment, treatment, other). If training on BDD was not included in the curriculum, participants were asked to select the reason(s) from the following options: (i) BDD is not as common as other disorders, (ii) BDD is not as serious as other disorders; (iii) teaching on related topics covers relevant skills; (iv) insufficient space in the timetable; (v) teaching staff do not have the relevant expertise; (vi) placement supervisors are not trained in BDD; and (vii) course tutors are not trained in BDD. The full set of questions were repeated in relation to teaching provided on OCD.
Procedure
We adopted a two-phase approach to recruitment. We first emailed courses between August 2024 and March 2025, inviting them to complete the full survey, with the opportunity to register for a free online training workshop on BDD following completion. Where possible, the survey was sent directly to course curriculum leads or academic directors. Where this information was not available, the survey was sent to course administrators. The recruitment email included the survey link, where participants were first provided with an information sheet and consent form. After consent was obtained, participants were presented with the survey, which took approximately 5–10 minutes to complete (see Supplementary material for full survey).
Response rates in the first phase were low (29.0%, n=18) and therefore in the second phase we recontacted courses requesting responses under the Freedom of Information Act 2000 (FOIA), in keeping with a previous training mapping study (Ayton and Ibrahim, Reference Ayton and Ibrahim2018). The FOIA grants the public the right to access recorded information held by public bodies, including details about postgraduate courses. In line with the FOIA, we requested only objective information about course content and structure and did not ask about perceived barriers to BDD training provision (see Supplementary material for FOIA request). The FOIA requests yielded a 100% response rate (n=62).
Statistical analyses
BDD and OCD teaching offered by DClinPsy and PGDip courses was summarised descriptively. Statistical comparisons were made used z-tests of proportions. Analyses were conducted in base R.
Results
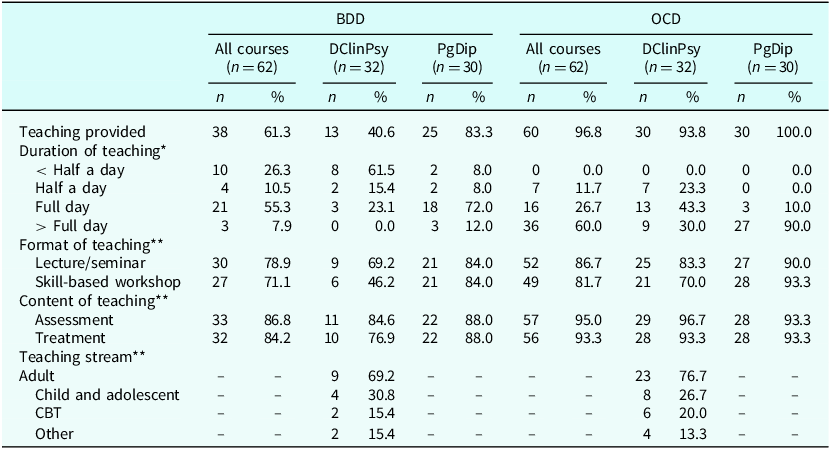
Table 1 provides a summary of training provided by DClinPsy and PgDip courses. Of the 62 courses, 61.3% (n=38) provided training on BDD versus 96.8% (n=60) on OCD, a statistically significant difference (z=4.85, p<.001). This difference was largely driven by DClinPsy courses, with significantly fewer DClinPsy courses providing BDD training than PgDip courses (40.6% vs 83.3%, z=3.45, p<.001). Of note, the vast majority of PgDip courses delivered training on both BDD and OCD, with no significant difference in frequency (83.3% vs 100%, respectively; z=2.34, p=.019). In contrast, significantly fewer DClinPsy courses delivered training on BDD than OCD (40.6% vs 93.7%, respectively; z=4.53, p<.001).
Descriptives of training provided on BDD and OCD in both the DClinPsy and PGDip courses

* One response for OCD in a DClinPsy course was marked as ‘unable to quantify’, thus the total number of courses for the duration of teaching of OCD for both DClinPsy and ‘All courses’ do not add up to the total number of courses that provided OCD teaching and percentages do not add up to 100%. **Data only provided for DClinPsy courses as the PGDip courses that were included focus exclusively on CBT for adults. Values in corresponding columns add up to more than the respective n (or 100%) as participants could select more than one answer per question.
Duration and format of teaching
Among the courses that taught BDD (n=38), the majority (55%, n=21) provided a day of training, and only 7.9% (n=3) provided more than one day of training. In contrast, the majority of courses that taught OCD (n=60) provided more than one day of training (60.0%, n=36). Most courses provided OCD and BDD teaching through lectures/seminars and skill-based workshops. The exception was BDD teaching on DClinPsy courses, where fewer than half (46%, 6 out of 13) offered skills-based workshops.
Teaching content
Of the courses offering BDD training (n=38), most covered the assessment (86.6%, n=33) and treatment (84.2%, n=32) within their curricula. This was similar for OCD, where almost all courses covered assessment (95.0%, n=57) and treatment (93.3%, n=56). DClinPsy and PgDip courses were equivalent with respect to their BDD and OCD teaching content.
Barriers to teaching delivery
Eighteen courses (29.0%; 9 DClinPsy and 9 PgDip) provided full survey responses and therefore reported on perceived barriers to training. Among these, five did not provide BDD training and the main perceived barriers were that there was insufficient space in the teaching timetable (80%, n=4,) and that there was already teaching on related topics, such as eating disorders and OCD, which was perceived as covering relevant skills (80%, n=4).
Sixteen courses (88.9%) were interested in further BDD teaching being offered in their curriculum, 12 (75.0%) of which already had some BDD teaching and four (25.0%) did not. Notably, all 16 courses (100%) expressed a specific interest in including teaching on the challenges and complexities of working with individuals with BDD. This was followed by interest in working with BDD in adults (68.8%, n=11), BDD treatment (68.8%, n=11), BDD assessment (56.3%, n=9) and BDD in adolescents (43.8%, n=7).
Discussion
The current study represents the first effort to systematically map the provision of BDD training among mental health professionals. Despite being prevalent and impairing, our findings show that BDD remains under-represented in psychological therapy training programmes in the UK. This is especially evident within DClinPsy courses, where only a minority provide any BDD-specific teaching. This training gap is likely to contribute to the widespread under-recognition and under-treatment of BDD in clinical practice (Addison et al., Reference Addison, James, Borschmann, Costa, Jassi and Krebs2024; Olaomi et al., Reference Olaomi, Khenechukwu, Udegbe, Uwumiro, Okafor, Obijuru, Yayehyirad and Opeyemi2024; Rautio et al., Reference Rautio, Isomura, Rück, Lichtestein, Kuja-Halkla, Larsson, Chang, D’Onofrio, Brikell, Sidorchuck, Mataix-Cols and Férnandez2024), and underscores a pressing need to improve BDD education for mental health professionals.
Importantly, our findings show that across DClinPsy and PgDip programmes BDD is not only taught less frequently than OCD, but also for shorter durations. Few courses reported offering more than one day of BDD training, whereas most said that they provided more than one day of OCD training, suggesting a further lack of parity in training provision. BDD is a complex disorder that requires specialised CBT. Indeed, randomised controlled trials (RCTs) have shown that generic therapies such as support psychotherapy and anxiety management are less effective than BDD-specific CBT (Enander et al., Reference Enander, Andersson, Mataix-Cols, Lichtenstein, Alström, Andersson and Rück2016; Veale et al., Reference Veale, Anson, Miles, Pieta, Costa and Ellison2014), which includes various specialist techniques such as mirror retraining, imagery rescripting, and reduction of self-focused attention (Veale and Neziroglu, Reference Veale and Neziroglu2010; Wilhelm et al., Reference Wilhelm, Phillips and Steketee2012). In a similar vein, although BDD is viewed as closely related to OCD (American Psychiatric Association, 2013; World Health Organization, 2022), it is a distinct disorder with different aetiological influences, underlying cognitive processes, and clinical features (Malcolm et al., Reference Malcolm, Labuschagne, Castle, Terrett, Rendell and Rossell2018), and therefore treating BDD simply as a variant of OCD (e.g. using CBT for OCD) may not adequately address BDD-specific factors. For example, insight is typically poorer in individuals with BDD than those with OCD (Malcolm et al., Reference Malcolm, Labuschagne, Castle, Terrett, Rendell and Rossell2018). Many individuals with BDD are firmly convinced that they have a genuine physical defect (Phillips et al., Reference Phillips, Pinto, Hart, Coles, Eisen, Menard and Rasmussen2012), leading to ambivalence about the value of psychological treatment and posing a significant challenge to therapeutic engagement. Less than one day of training is likely to be insufficient to adequately equip clinicians with the necessary skills required to engage and treat individuals with BDD.
Interestingly, in contrast to DClinPsy programmes we found that most PgDip in CBT courses reported inclusion of some training on BDD. This may reflect the introduction of BDD as a core module in the most recent version of the NHS Talking Therapies curriculum for high intensity therapists (Health Education England, 2022). While this represents a positive development, it is notable that 17% of PgDip courses still do not offer BDD teaching, despite it being included in the curriculum. Gaining a clearer understanding of the barriers to implementation may help inform more effective strategies to improve uptake.
Another key finding of the current study is that even when BDD is taught, within DClinPsy courses the teaching typically focuses on adult populations, even though the disorder usually emerges in adolescence. Approximately two-thirds of adults with BDD report an onset prior to the age of 18, with an average age at onset of 16 years (Bjornsson et al., Reference Bjornsson, Didie, Grant, Menard, Stalker and Phillips2013). Furthermore, BDD onset is often insidious with symptoms first emerging in early adolescence, around the age of 12–13 years (Bjornsson et al., Reference Bjornsson, Didie, Grant, Menard, Stalker and Phillips2013), which may be linked with normative developmental processes such as onset of puberty and the development of self-concept. Therefore, training clinicians in recognising, formulating, and treating BDD in youth is essential to aid earlier detection and intervention efforts. Of note, the focus on adult populations was also evident in teaching provision for OCD, which often has a childhood onset, and may therefore represent a broader issue rather than being specific to BDD.
The current findings have several implications for education, training and clinical practice. First and foremost, our findings highlight the need for BDD education to be embedded within curricula across mental health training pathways. Encouragingly, many courses expressed interest in incorporating BDD training, citing the complexity of the disorder and the challenges it presents. Although the current study focused on DClinPsy and PgDip courses, it is likely that BDD is also under-represented in other mental health professionals training courses. For example, BDD teaching is not mandated in the curriculum for Psychological Wellbeing Practitioners (PWPs), who conduct a large proportion of initial assessments within NHS TTad. There is a need to train this workforce in simple BDD screening questions and use of validated self-report measures, in order to promote detection and facilitate timely access to treatment. Additionally, BDD screening should be integrated into the newly emerging ‘digital front door’ technologies to ensure that it is not overlooked early in the care pathway (National Institute for Health and Care Excellence, 2025).
Second, in addition to updating training course curricula, there is also a need to develop less resource-intensive and scalable educational programmes for mental health professionals. This approach is particularly important given that training courses have limited time in their teaching curricula, as highlighted by the current findings, and may therefore be unable to provide comprehensive training in BDD. Technology-enabled training programmes have been shown to be associated with improvements in knowledge, self-efficacy, and therapeutic skills in relation to a variety of mental health conditions (Singh and Reyes-Portillo, Reference Singh and Reyes-Portillo2020), with effects generally enhanced when training includes an element of case supervision (Rakovshik et al., Reference Rakovshik, McManus, Vazquez-Montes, Muse and Ougrin2016). Recently, an online therapist training programme for BDD has been developed and evaluated in an initial pilot study (Gumpert et al., Reference Gumpert, Rautio, Birovecz, Jolstedt, Lundgren, Fernández de la Cruz and Jansson-Fröjmark2025). Thirty clinicians from child and adolescent mental health services in Sweden completed a supervised online education programme over 4–7 weeks, with supervision provided by a BDD expert throughout. Clinicians’ knowledge, understanding and self-efficacy in assessing and treating paediatric BDD improved significantly. Additionally, clinicians reported using the acquired skills in their practice at 6-month follow-up. Although further evaluation with a control comparator is required, these findings are nevertheless encouraging and offer one potential solution for disseminating BDD training.
Third, although improving access to BDD training for clinicians should be prioritised, clinicians can also draw on published, evidence-based assessment and treatment tools to enhance their clinical practice. A range of self-report questionnaires have been developed to aid assessment of BDD (Hogg et al., Reference Hogg, Causier, Del Prete Ferrucci, Gupta, Stringaris and Krebs2026), including the Body Image Questionnaire (BIQ; Veale et al., Reference Veale, Ellison, Werner, Dodhia, Serfaty and Clarke2012) and its adapted version for young people, the BIQ-C (Blacker et al., Reference Blacker, Gupta, Quinn, Monzani, Jassi, Veale and Krebs2024). Such tools are quick and easy to administer and can be used to inform a clinical assessment and promote identification of BDD. Similarly, treatment manuals are widely considered to be a useful vehicle for disseminating evidence-based practices beyond research settings. Several CBT for BDD protocols have been evaluated in RCTs and since published as therapist manuals (Veale and Neziroglu, Reference Veale and Neziroglu2010; Wilhelm et al., Reference Wilhelm, Phillips and Steketee2012), providing a valuable resource for therapists and opportunity to develop knowledge of evidence-based practice.
A key strength of the current study is its comprehensive coverage of all DClinPsy and PgDip (CBT) courses across the UK, coupled with a 100% response rate to the core survey questions, ensuring a robust overview of current BDD training provision. However, several limitations should be considered. First, most courses responded only to the FOIA request, and the low response rate to the full survey limits insights into perceived barriers to BDD teaching. Second, most courses were only able to provide high level information preventing detailed analysis of teaching content. Third, while we focused on two of the largest psychological therapy training programmes in the UK, future studies should examine other pathways such as psychiatry training programmes or those designed specifically for children and young people’s mental health practitioners.
In conclusion, this study provides the first national overview of BDD training within UK psychological therapy programmes and identifies a critical shortfall, particularly in DClinPsy courses where provision is limited and largely adult-focused. This training gap may contribute to the widespread under-recognition and under-treatment of BDD. Addressing this disparity is likely to require both curricula reform as well as scalable training solutions, such as supervised online programmes, to ensure clinicians are equipped to detect and treat BDD effectively.
Key practice points
-
(1) Body dysmorphic disorder (BDD) is under-recognised and under-treated, and this may be partly due to limited training among psychological therapists, especially within Doctorate in Clinical Psychology (DClinPsy) programmes in the UK.
-
(2) Training provision for BDD is significantly lower than for obsessive-compulsive disorder (OCD), despite similar prevalence and impact of these two disorders.
-
(3) Shorter duration and limited skills-based teaching on BDD may hinder clinicians’ ability to accurately assess and treat the disorder, underscoring the importance of integrating more comprehensive BDD training into curricula.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1754470X26100518
Data availability statement
Aggregate data will be made available on request. The full study dataset will be made available on reasonable request and subject to appropriate data sharing agreements.
Acknowledgements
None.
Author contributions
Georgina Krebs: conceptualised and supervised the study, and wrote the original draft; Shyn Phua: contributed to project administration, formal analyses, and reviewing and editing the manuscript; Gaia Del Prete Ferrucci: contributed to project administration, formal analyses, and reviewing and editing the manuscript; Angela Lewis: contributed to methodology and reviewing and editing the manuscript; David M. Veale: contributed to interpretation of findings and writing the draft; Elizabeth Hogg: contributed to study design and methodology, project administration, formal analyses and reviewing and editing the manuscript.
Financial support
Professor Krebs has received research funding from the Wellcome Trust, the British Academy, and honoraria from Elsevier for editorial work. This study represents independent research part funded by the National Institute for Health Research (NIHR) Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London.
Competing interests
Professor Krebs receives honoraria from Elsevier for editorial work. The authors have no other competing interests to declare.
Ethical standards
The study was approved by the UCL Division of Psychology and Language Sciences (PALS) Low Risk Research Ethics Committee (reference: CEHP/2024/595), and abided by the Ethical Principles of Psychologists and Code of Conduct as set out by the British Association of Behavioural and Cognitive Psychotherapies and the British Psychological Society.



 Open access
Open access
Comments
No Comments have been published for this article.