
Microbial and host cellular biology and interactions dictate the breadth of clinical infection practice, from colonisation to invasion to infection. Understanding the classifications used for bacteria, viruses, fungi and parasites aids clinical and laboratory diagnosis and ultimately patient management. Understanding the common host responses to infective agents at the cellular level enables appropriate clinical management both with direct acting anti-infectives and other supportive therapy.
Questions
Q1.1 A 21-year-old female presents with a fever, and a novel viral infection is suspected. Electron microscopy is performed. Which of the following might be present in a virus?
Q1.2 A 46-year-old male presents with a fever of unknown origin, and a whole blood sample is sent to the virology laboratory for polymerase chain reaction testing. The test identifies a DNA virus. Which of the following class of viruses contain DNA?
Q1.3 A 1-year-old male awaiting repair of a ventricular septal defect is being considered for palivizumab prophylactic therapy for respiratory syncytial virus (RSV). What type of virus is RSV?
Q1.4 A 21-year-old female presents with a fever and leucopaenia, and a viral infection is suspected. Which of the following is a paramyxovirus?
Q1.5 A 25-year-old female is recalled after cervical screening. Which of the following is true regarding human papillomavirus (HPV)-associated malignancy?
Q1.6 A 27-year-old female with sickle cell anaemia presents in aplastic crisis with a fever. Her blood results demonstrate:
Haemoglobin 50 g/L
Reticulocyte count 0.1%
White cell count 12.3 × 109/L
Lymphocytes 8.6 × 109/L
CRP 34
Which genus is the most likely causative virus from?
Q1.7 A 31-year-old female is referred from occupational health. A chronic infective carrier state may occur in which viral infection?
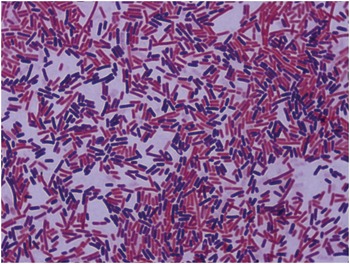
Q1.8 A 54-year-old male presents with fever, tachycardia and hypotension. A blood culture is taken and becomes positive in 12 hours. The Gram stain is shown in Figure 1.1.
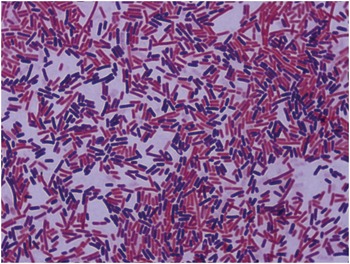
Figure 1.1 Gram stain from a positive blood culture.
Which of the components of the Gram stain is a fixative?
Q1.9 A 54-year-old male presents with fever, tachycardia and hypotension. A blood culture is taken and becomes positive in 12 hours, and Escherichia coli is identified. It is demonstrated to have in vitro resistance to many penicillins and cephalosporins. Through what mechanism is an extended-spectrum beta-lactamase gene most likely to be present in this E. coli?
Q1.10 A 28-year-old male presents with diarrhoea. A non-lactose fermenting coliform is isolated from faeces, and serological investigation of the isolate is performed. The “O” antigen is positive, but the “H” antigen is negative. What is the most likely explanation for this?
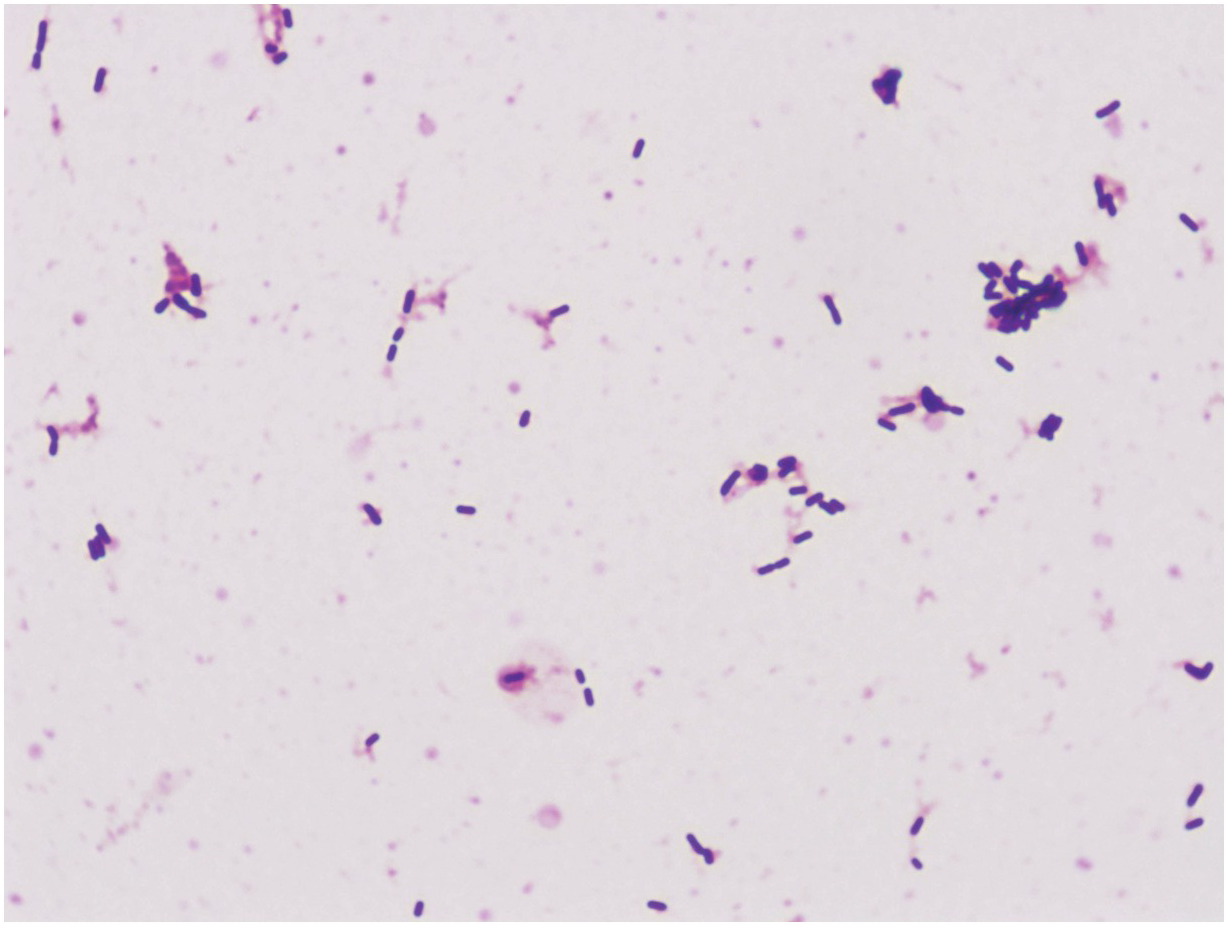
Q1.11 A 35-week pregnant female recalled a flu-like illness 2 days prior to delivery. She was treated for peri-partum sepsis, and her new-born child was born in poor condition and admitted to the neonatal intensive care department. Blood cultures (and subsequently cerebrospinal fluid) grew the organism depicted in Figure 1.2.

Figure 1.2 Gram stain of cerebrospinal fluid.
Which laboratory test would be the most useful to confirm identification?
Q1.12 A 34-year-old man presents with a fever, and an aerobic blood culture bottle grows a Gram-negative rod. Which one of the following organisms is a strict aerobe?
Q1.13 A 42-year-old patient presents with septic shock and is found to have a soft tissue infection. Which component of the cell wall of Gram-positive bacteria may contribute to the development of septic shock in Gram-positive infections?
Q1.14 A 23-year-old female presents with a urinary tract infection. Which of the following is true about urease producing bacteria?
Q1.15 A 63-year-old female is diagnosed with urosepsis. She is profoundly hypotensive. What is the most important endotoxin component leading to septic shock from Gram-negative bacteria?
Q1.16 A 21-year-old female presents with necrotising fasciitis. Which of the following is not a virulence factor of Staphylococcus aureus?
Q1.17 A 31-year-old male returns from Ethiopia and presents with a recurrent febrile illness. What is the cause of the relapsing nature of fever in Borrelia recurrentis infection?
Q1.18 A 16-year-old male presents with respiratory distress. Which organism produces a toxin similar in action to that of Corynebacterium diphtheriae?
Q1.19 An 18-year-old female presents with difficulty swallowing. A throat swab demonstrates club-shaped organisms with differential staining. Corynebacterium diphtheriae is suspected. What are Corynebacterium diphtheriae volutin granules made of?
Q1.20 A 45-year-old female presents with a heart block following a minor dog bite to the palm of her hand (Figure 1.3).

Figure 1.3 Clinical appearance of the right hand following a minor dog bite.
Corynebacterium ulcerans is isolated from the wound, and an Elek test is positive. How does diphtheria toxin act?
Q1.21 A 50-year-old male who underwent traumatic splenectomy two years ago presents with tachypnoea, tachycardia and hypoxia. A mucoid Streptococcus pneumoniae is subsequently grown (Figure 1.4).

An avirulent, non-capsulate strain of pneumococcus can change to virulent capsulate strains through which mechanism?
Q1.22 A 56-year-old male is diagnosed with native valve endocarditis. A blood culture grows a Gram-positive cocci on both blood agar and MacConkey agar, which is ampicillin resistant. What is the likely identification of this organism?
Q1.23 A 14-month-old child is admitted with a two-week history of coughing and is admitted with severe paroxysms of coughing leading to hypoxia. Pertussis is suspected. Which of the following is true about Bordetella pertussis?
Q1.24 A 56-year-old female with urosepsis is not improving despite treatment with an intravenous third-generation cephalosporin. Which bacteria are most likely to harbour an extended-spectrum beta-lactamase gene?
Q1.25 A 49-year-old homeless patient attends the emergency department complaining of itching and fever. He describes the onset of fever approximately 7 days ago. On examination, he has a widespread rash and excoriation marks. What is the most likely vector for this illness?
Q1.26 A 54-year-old male presents with a flitting rash and an eosinophilia eight weeks after return from the tropics. Which of the following infections require an intermediate snail host?
Q1.27 A 31-year-old male presents with diarrhoea several days after return from Nigeria. Entamoeba is seen on stool microscopy. Which of the following is a non-pathogenic variant of Entamoeba histolytica?
Q1.28 A 21-year-old female presents with a fever, adenopathy and a rash. Blood tests demonstrate a lymphocytosis. Serological diagnosis of a primary viral infection may be made by detection of which viral-specific immunoglobulin?
Q1.29 A 23-year-old male student has been recently admitted with invasive meningococcal disease. He has made a good recovery but gives a history of a previous episode of meningococcal septicaemia when he was 15 years old. There is no history of other recurrent infections. Which immunodeficiency is most likely in this patient?
Q1.30 An 18-year-old male with chronic granulomatous disease (CGD) has recurrent staphylococcal infection. What is the mechanism behind this?
Answers
Answer B: An envelope
Viruses (Latin for toxin) contain DNA or RNA but not both. The central ribonucleic core is surrounded by a protective shell (not a cell wall) of repeating protein units called capsomeres. This has a symmetry which is either helical or icosahedral. Viral particles contain polymerases and integrases but no true metabolic pathways. As completed virions move from the host cell nucleus to the cytoplasm or from the cytoplasm to the extracellular space, an external lipid-containing envelope may be added to the nucleocapsid.
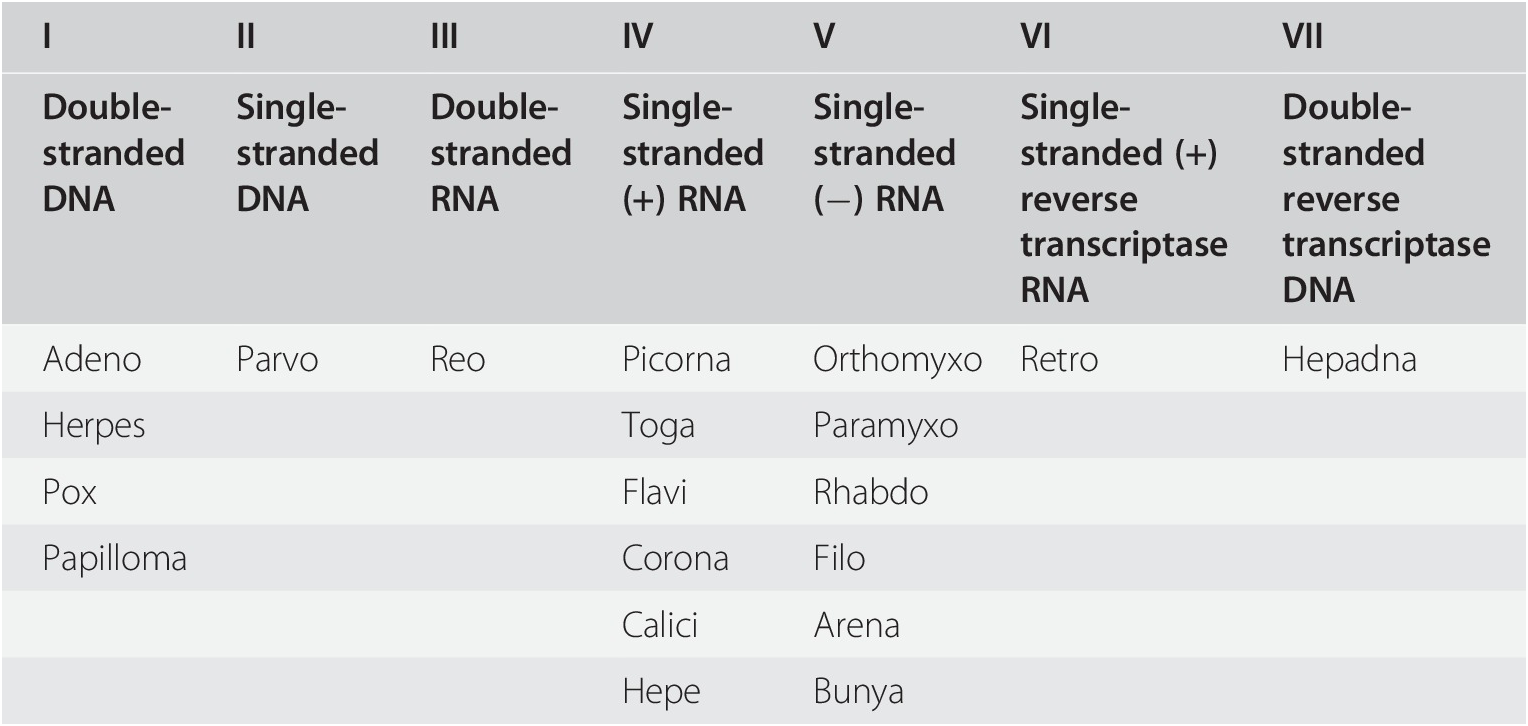
Answer E: Parvoviridae
There are several methods of classifying viruses, but perhaps the most widely used is the Baltimore system developed in 1971, which designates viruses into one of seven groups depending on the nature of the nucleic acid within the virus. Four aspects are considered: (i) whether the nucleic acid is DNA or RNA, (ii) whether it is single stranded or double stranded, (iii) whether it is positive or negative sense, and (iv) the method of replication.
| I | II | III | IV | V | VI | VII |
|---|---|---|---|---|---|---|
| Double-stranded DNA | Single-stranded DNA | Double-stranded RNA | Single-stranded (+) RNA | Single-stranded (−) RNA | Single-stranded (+) reverse transcriptase RNA | Double-stranded reverse transcriptase DNA |
| Adeno | Parvo | Reo | Picorna | Orthomyxo | Retro | Hepadna |
| Herpes | Toga | Paramyxo | ||||
| Pox | Flavi | Rhabdo | ||||
| Papilloma | Corona | Filo | ||||
| Calici | Arena | |||||
| Hepe | Bunya |
Answer A: Single-stranded (−) RNA
RSV is a single-stranded (−) RNA virus of the family Paramyxoviridae. Infection with this virus usually produces only mild symptoms, often indistinguishable from common cold and minor illnesses. It is, however, also the most common cause of bronchiolitis and pneumonia in children less than 1 year of age and can also cause croup. These syndromes are more likely to occur in patients that are immunocompromised or infants born prematurely. No antivirals are effective – the mainstay of therapy is oxygen. Palivizumab (a monoclonal antibody against RSV surface fusion protein) can be given as monthly injections begun just prior to the RSV season (usually for five months) as RSV prophylaxis for infants that are premature or have either cardiac or lung disease.
Answer D: Nipah virus
The paramyxoviridae (ss(−)RNA) family includes viruses causing many common infections. However, it has a complex taxonomy:
Subfamily Paramyxovirinae
Genus Henipavirus (Hendra virus and Nipah virus)
Genus Morbillivirus (Measles virus)
Genus Respirovirus (Human parainfluenza viruses 1 and 3)
Genus Rubulavirus (Mumps virus and Human parainfluenza viruses 2 and 4)
Subfamily Pneumovirinae
Genus Pneumovirus (Human respiratory syncytial virus)
Genus Metapneumovirus (Human metapneumovirus)
Rubella virus is of the genus Rubivirus from the Togaviridae family (ss(+)RNA). Influenza B virus is a genus of the Orthomyxoviridae family (ss(−)RNA). Polio virus is of the genus Enterovirus from the Picornaviridae family (ss(+)RNA). Parvovirus B19 is of the genus Erythrovirus from the Parvoviridae family.
Answer B: HPV-16 and HPV-18 are associated with genital cancers
HPV is a DNA virus from the papillomavirus family, of which there are numerous serotypes. Serotypes 6 and 11 most frequently cause ano-genital warts, while serotypes 16 and 18 are linked with ano-genital cancers. The E6 and E7 early viral proteins are considered oncogenic, inhibiting tumour suppression genes: E6 inhibits p53, while E7 inhibits p53, p21 and RB. Diagnosis is through PCR on sample obtained during colposcopy.
Answer E: Erythrovirus
Humans can be infected by viruses from three genera from the Parvoviridae family, but no members of the genus Parvovirus are currently known to infect humans. This creates a confusion of terms because the human parvoviruses are not in genus Parvovirus. They are from the genera: Dependoviruses (e.g. Adeno-Associated Virus), Erythroviruses (e.g. Parvovirus B19) and Bocaviruses. In healthy individuals, the major presentation of B19 infection is erythema infectiosum, but in patients with underlying haematological disorders, infection can lead to aplastic crisis. In immunosuppressed patients, persistent infection may develop that presents as pure red cell aplasia and subsequent chronic anaemia. In utero infection may result in hydrops fetalis, miscarriage or congenital anaemia.
Answer D: Hepatitis C virus
Viruses typically have one of three natural histories; acute infection (e.g. influenza, hepatitis A, Hanta, Nipah, hepatitis E), latent infection (e.g. herpes simplex, varicella zoster, cytomegalovirus) or chronic infection (e.g. hepatitis B, hepatitis C, HIV).
The global annual incidence of hepatitis C is estimated at four million, of whom 18–34% will spontaneously clear the virus. Acute infection with hepatitis C is clinically mild and may even be unrecognised or undiagnosed; acute resolution is not associated with any long-term sequelae. The remainder of the patients are deemed to have chronic hepatitis C, which is now the leading cause of end-stage liver diseases and liver-related deaths in much of the world. Progression of liver fibrosis in chronic hepatitis C is extremely variable, and is influenced by viral, host and environmental factors.
Answer E: Iodide
Clinical samples requiring a Gram stain, such as sterile fluids and positive blood cultures, must be heat fixed to a slide. A Gram stain can then be undertaken to determine the presence of Gram-positive or Gram-negative bacteria and to enable morphological characterisation. The slide should be flooded with crystal violet for 1 minute, which penetrates through cells and cell membrane. This is then followed by addition of iodide for a further minute, which also enters the cell wall and then binds with the crystal violet, forming larger molecules which are insoluble in water and are therefore fixed in place. A decolouriser is then washed over the slide for a few seconds, in the form of either acetone or alcohol, and the slide is then rinsed with water. This dehydrates and therefore tightens the cell wall of Gram-positive organisms, stopping the large crystal violate-iodine complexes from exiting the cells. Contemporaneously the decolouriser degrades the outer membrane of Gram-negative organisms and the thin cell wall cannot retain the crystal violet-iodine solution. A counterstain is then applied for 1 minute, usually safranin or carbol fuchsin, which cannot stain the dehydrated Gram-positive organisms, but does adhere to Gram-negative organisms.
Gram-positive organisms have a single cell membrane, around which is a thick peptidoglycan cell wall. Gram-negative organisms have a thin peptidoglycan cell wall, but have two cell membranes, one on either side of the cell wall. Cell wall deficient bacteria cannot be readily characterised by the Gram stain.
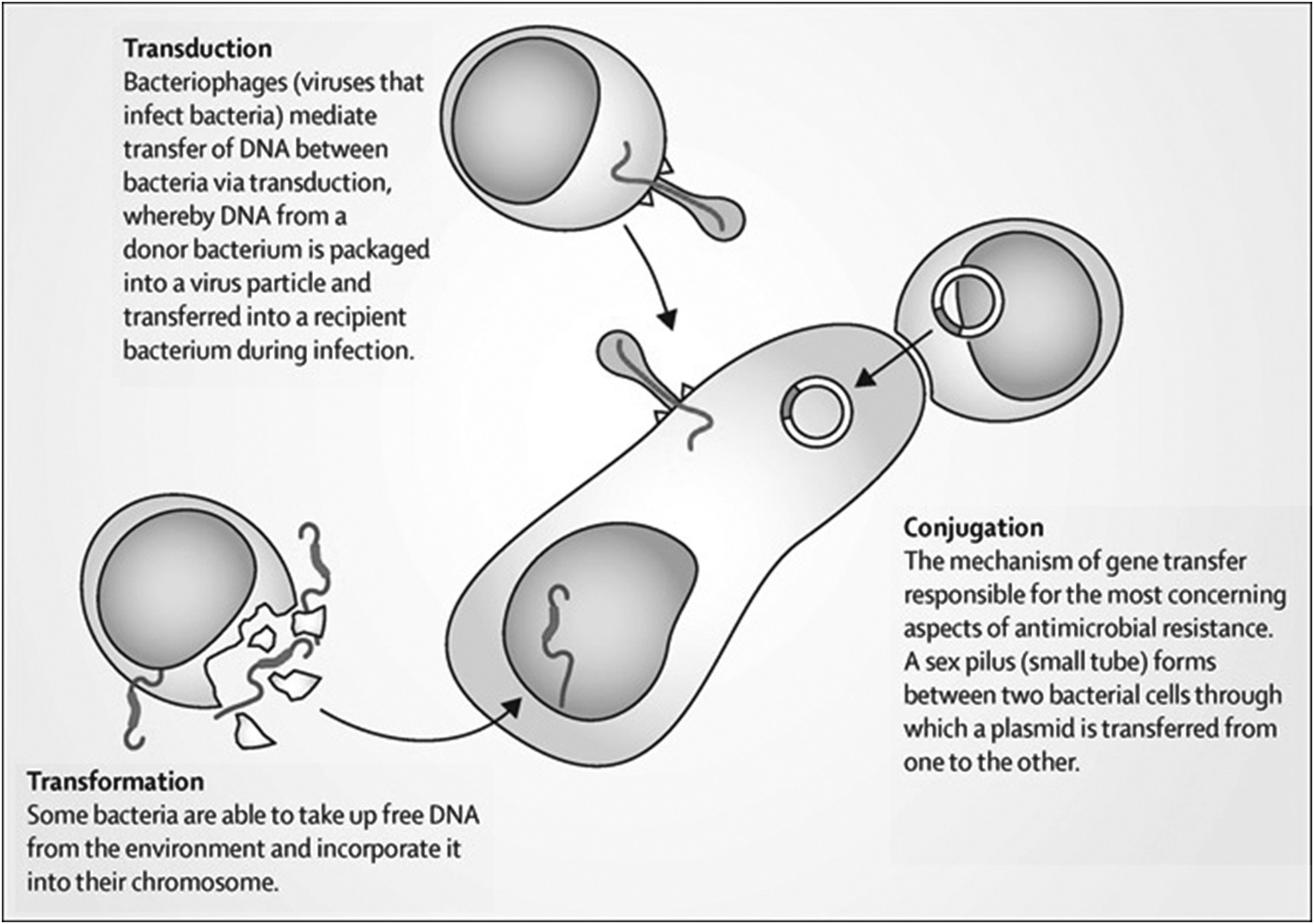
Answer C: Conjugation
Bacteria can demonstrate resistance to antimicrobials through a number of mechanisms, including target alteration, enzymatic destruction, porin loss and efflux pumps. The different genes which dictate these cellular mechanisms can be constitutively present in some genera and species of bacteria, or, more rarely may arise through de novo mutations in those organisms which did not previously harbour them. More usually however, genetic material encoding antimicrobial resistance mechanisms is transferred between organisms, either of the same species, of different species in the same genera, or less frequently between genera. This transfer of genetic material can occur through three main mechanisms: transduction, transformation and conjugation (Figure 1.5).
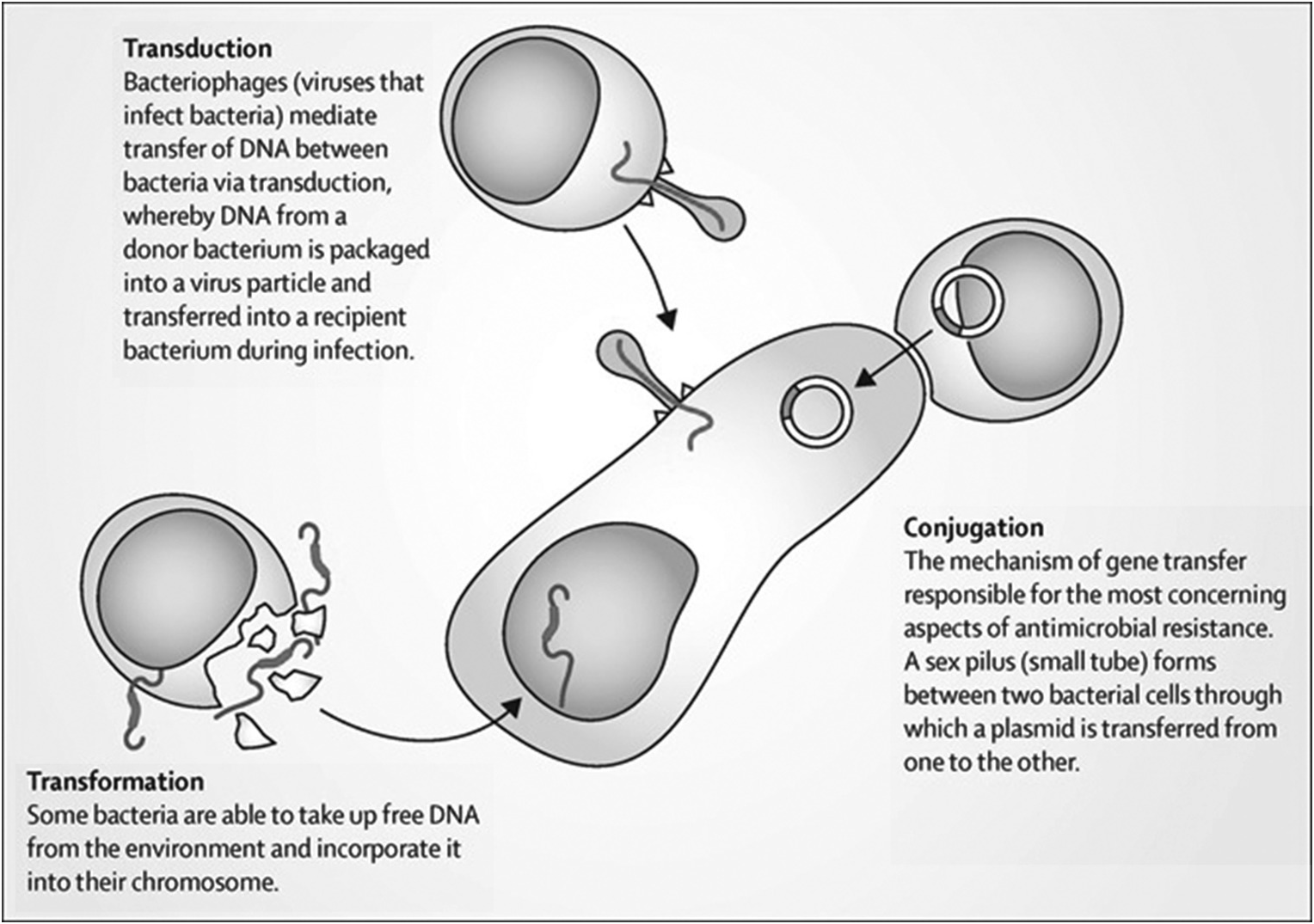
In this case, Escherichia coli does not constitutively harbour an extended-spectrum beta-lactamase (ESBL) gene in their chromosomal genetic material, and the development of a de novo ESBL gene would be rare. Similarly, in the context of both this organism (E. coli) and this family of resistance genes (ESBL), transduction and transformation is unlikely. Instead, it is conjugation, and the transmission of plasmids with their additional genetic material, which will bring to the host E. coli lineage the ability to produce ESBL proteins and confer resistance to many penicillins and cephalosporins.
Answer A: The isolate is non-motile
Salmonella species are non-lactose fermenting (with the exception of Salmonella Arizonae and Salmonella Indiana) coliforms which produce hydrogen sulphide (with the exception of some isolates of Salmonella Paratyphi A and Salmonella Typhi) when sub-cultured in the presence of sulphur-containing amino acids (on agar plates such as xylose-lysine-desoxycholate agar (XLD) or desoxycholate citrate (DCA)).
Two antigens are examined when identifying serovars of clinical Salmonella isolates; somatic (oligosaccharide) “O” antigens and flagella “H” antigens. Variations in these antigens aid identification for clinical and epidemiological purposes; however, laboratory identification can be complex. Salmonella isolates can exist in two “H” phases; phase I being motile and phase II being non-motile (the latter as in this case). Isolates that are non-motile on primary culture may be switched to a motile phase using a Cragie tube or the Jameson plate.
Somatic “O” antigens are heat stable and alcohol-resistant, but flagellar “H” antigens are heat-labile. Some surface antigens in Salmonella may mask somatic antigens, meaning bacteria will not agglutinate with somatic “O” antisera – one specific surface antigen is the “Vi” antigen. The “Vi” antigen may only occur in three Salmonella serovars (out of over 2000): Typhi, Paratyphi C and Dublin, but is variably detected. Other non-lactose fermenting coliforms can cause diarrhoea, including Shigella species, but as a rule these do not produce hydrogen sulphide.
Answer E: Tumbling motility
Neonates are at a greater risk of sepsis and meningitis than other age groups due to deficiencies in humoral and cellular immunity and in phagocytic function. Infants younger than 32 weeks’ gestation receive little maternal immunoglobulin. Inefficiency in the neonates’ alternative complement pathway compromises their defence against encapsulated bacteria and poor migration and phagocytic function of neutrophils is apparent. Group B Streptococcus is the most commonly identified organism, implicated in roughly 50% of cases, with Escherichia coli accounting for a further 20%, meaning identification and treatment of maternal genitourinary infections is an important prevention strategy. Listeria monocytogenes is the third most common pathogen, causing 5–10% of cases. Patients exposed to L. monocytogenes in pregnancy often describe a mild flu-like illness but the organism exhibits transplacental transmission leading to sepsis in both mother and neonate. Listeria is a catalase-positive, haemolytic Gram-positive rod that exhibits tumbling motility at 25°C but not at 37°C. Tumbling motility is specific to Listeria and identified by the hanging drop test. The cerebrospinal fluid response usually reflects the intracellular nature of Listeria with a predominant mononuclear pleocytosis.
Answer E: Pseudomonas aeruginosa
P. aeruginosa is an obligate aerobe. It is a Gram-negative, non-lactose fermenting organism which is oxidase positive. It is a common commensal in wounds, but can become an opportunistic pathogen.
Bacteroides spp. (Gram negative) and Clostridium spp. (Gram positive) are examples of non-spore-forming and spore-forming strict anaerobes, respectively. Other obligate anaerobes include Peptostreptococcus spp. and Veillonella spp. Bacteroides melaninogenicus has recently been reclassified as Prevotella melaninogenica while Porphyromonas gingivalis (commonly found in the oral cavity) were originally classified in the Bacteroides genus. Kluyvera spp. has been put forward as a new member of the Enterobacteriales and as such is only a facultative anaerobe. P. aeruginosa is an obligate aerobe.
Answer E: Teichoic acid
The outside of a Gram-positive cell wall is covered with a thick layer consisting of peptidoglycan (PGN) and lipoteichoic acid (LTA), which resembles Gram-negative lipopolysaccharide (LPS). LTA and PGN are able to induce the release of nitric oxide, IL-1, IL-6 and TNF-α by monocytes and macrophages and to activate the oxidative burst in vitro. Furthermore, the effects of LTA and PGNs may be synergistic. Lipoteichoic acid can bind to CD14 and to TLR – binding to TLR-2 has shown to induce NF-kB expression (a central transcription factor), elevating expression of both pro- and anti-apoptotic genes. Its activation also induces mitogen-activated protein kinases (MAPK) activation. LTA bound to targets can interact with circulating antibodies and activate the complement cascade to induce a passive immune kill phenomenon. It also triggers the release from neutrophils and macrophages of reactive oxygen and nitrogen species and cytotoxic cytokines. Therefore, LTA shares many pathogenic similarities with endotoxins.
Answer D: Morganella morganii is potentially a urea-splitting bacteria
Bacterial urease alkalinises urine, and urease-producing bacteria play a prominent role in the formation of infection-induced urinary stones. Struvite stone formation occurs when ammonia production increases and urine pH elevates to decrease the solubility of phosphate. Proteus spp., M. morganii and Klebsiella pneumoniae are all potentially urea-splitting bacteria, whereas while E. coli is the most common cause of lower urinary tract infections, it is not associated with significant alkalinisation, nor is infection with Pseudomonas aeruginosa. Hyperammonaemia can result from the production of excessive amounts of ammonia due to bacterial urease, and its subsequent re-absorption into the systemic circulation, which is implicated in hepatic encephalopathy.
Answer C: Lipid A
Endotoxins are part of the outer membrane of the cell wall of Gram-negative bacteria. Lipopolysaccharide (LPS) is a major component of the outer membrane, contributing greatly to the structural integrity and protecting the membrane from chemical attack. LPS comprises three parts: O antigen, core oligosaccharide and Lipid A. Lipid A is associated with the toxicity of Gram-negative bacteria. It is the innermost of the three regions of the lipopolysaccharide molecule, and its hydrophobic nature allows it to anchor the LPS to the outer membrane. Lipid A (and LPS) is believed to activate cells via the Toll-like receptor system. The polysaccharide components produce immunogenicity.
Answer A: Lecthinase
S. aureus is a common skin commensal, but can cause skin and skin structure infections, including cellulitis and necrotising fasciitis. Different strains of S. aureus produce various different exotoxins, some of which are associated with differing disease presentations and differing severity.
Panton-Valentine leukocidin (PVL) is a cytotoxin produced by S. aureus which destroys neutrophils and causes tissue necrosis, recurrent skin and soft tissue infections and necrotising pneumonia. Toxic shock syndrome toxin-1 (TSST-1) is a superantigen produced by S. aureus which stimulates IL1, IL2 and tumour necrosis factor leading to toxic shock syndrome. Enterotoxin A can result in the emetic response seen in S. aureus food poisoning, but in addition staphylococcal enterotoxins A, B and C are also associated with toxic-shock syndrome presentations. DNase (deoxyribonuclease) production is often used in microbiology laboratories to differentiate S. aureus from other species of staphylococci (which can hydrolyse DNA for a source of carbon).
Several bacteria produce phospholipases including Listeria monocytogenes but not S. aureus. Lecithinase is a type of phospholipase produced by Clostridium perfringens causing myonecrosis and haemolysis.
Answer D: Antigenic variation
Borrelia recurrentis (louse-borne relapsing fever) are spirochaetes. A single spirochaete can lead to infection and multiply every 6–12 hours in the blood. The organism can invade the brain, eye, liver, heart and other organs. Each febrile episode is characterised by marked spirochaete-aemia following which there is clearance of the circulating microbes and a development of antibodies against the antigens displayed during the episode. Later episodes will involve spirochaetes displaying a different antigen, similar to trypanosomes, enabling reappearance in the blood. This is accomplished through a process of antigenic variation – specifically site-specific recombination.
Antigenic shift and antigenic drift are the mechanisms through which influenza changes its genetic structure and epitopes over time. Slipped strand mispairing can function as mechanism for phase variation in Escherichia coli. Transposons have varied roles in infectious diseases, but perhaps of most clinical relevance are responsible for transfer of anti-microbial resistance genes.
Answer B: Pseudomonas aeruginosa
Diphtheria toxin is an exotoxin which is encoded by a bacteriophage. It catalyses the ADP-ribosylation of eukaryotic elongation factor-2 (eEF2), inactivating this protein. In this way, it acts as a RNA translational inhibitor. The exotoxin A of P. aeruginosa uses a similar mechanism of action. It is an extremely potent exotoxin with only a single toxin molecule required to kill a human cell.
Answer D: Phosphate
Corynebacterium is named from the Greek word ‘Coryne’ which refers to the club shape of bacteria. Volutin, or metachromatic granules, are cytoplasmic granules located in bacterial cytoplasm. These contain polymerised metaphosphate and represents a storage form for inorganic phosphate and energy. These metachromatic granules stain red with methylene blue dye and forms the basis of Albert’s stain for the microbiological identification of C. diphtheria.
Answer A: ADP ribosylation of EF2
Diphtheria toxin is an exotoxin which is encoded by a bacteriophage. It catalyses the ADP-ribosylation of eukaryotic elongation factor-2 (eEF2), inactivating this protein. Toxin-mediated systemic sequelae occur in up to 15% of cases, predominantly in respiratory diphtheria but also in those with cutaneous diphtheria where disease is extensive. These manifest in two ways; myocarditis or peripheral neuropathy. Myocarditis can lead to complete heart block and cardiomyopathies. Toxin-mediated neuropathies can manifest as bulbar dysfunction, limb weakness or respiratory failure. Symptoms can be protracted – one series found symptoms persisted for a median of 49 days.
Answer C: Naked DNA transformation
S. pneumoniae is a Gram-positive cocci which is a common upper respiratory tract commensal. It has the ability to become pathogenic however, and has several virulence factors to aid this. One such virulence factor is the extracellular capsule, which resists phagocytosis by host immune cells. S. pneumoniae can alter its production of such capsules through phase variation; a switch between all or none protein expression which is usually reversible. This system can be used to adapt to more than one environment and provides mechanisms to evade the host immune system. Across different genera, phase variation occurs through several mechanisms: slip strand mispairing (e.g. meningococcal capsule formation), homologous recombination, site-specific recombination (e.g. DNA inversion in type 1 fimbrial variation in Escherichia coli ), epigenic regulation (e.g. altered methylation of regulatory DNA regions in E. coli outer membrane protein formation) or transformation of exogenous DNA (e.g. pneumococcal opacity, as in this case).
Answer B: Enterococcus faecium
Enterococci grow well on MacConkey agar unlike streptococci. E. faecalis are generally sensitive to ampicillin and resistant to quinupristin/dalfopristin (synercid®). E. faecium are resistant to ampicillin and sensitive to quinupristin/dalfopristin. These characteristics are useful in laboratory identification of enterococci, however quinupristin/dalfopristin is difficult to obtain for clinical use and is not universally tested in laboratory practice.
Answer C: Organism is isolated from throat for several days following infection
Bordetella spp. are small Gram-negative coccobacilli of the phylum proteobacteria and are highly fastidious obligate aerobes. Bordetella pertussis is an exclusive human pathogen. Transmission occurs by direct contact or respiratory aerosol droplets. It is highly contagious with over 90% of household contacts developing disease. The incubation period averages 7–10 days (range 5–21 days). Activity tends to peak at the ages of 3–4 years. Bacteria initially adhere to ciliated epithelial cells in the nasopharynx causing an initial catarrhal phase, which lasts for 1–2 weeks during which large numbers of bacteria can be recovered from the pharynx. Paroxysms of cough increase in frequency and severity as illness progresses for 2–6 weeks. During this stage toxins cause ciliostasis and facilitate the entry of bacteria to tracheal/bronchial ciliated cells. B. pertussis also produces a lymphocytosis-promoting factor, which causes a decrease in the entry of lymphocytes into lymph nodes and leads to a marked lymphocytosis. Complications include pneumonia, seizures and encephalitis.
Diagnosis can be made via culture of the organism, serology or molecular detection. A nasopharyngeal swab can be cultured on Bordet-Gengou agar to select for the organism, which shows mercury-drop colonies. Culture lacks sensitivity, decreasing with age and specimen quality. It is unlikely to culture positive after 2 weeks of illness. Serology testing detects anti-pertussis toxin IgG antibody levels using ELISA. This is used in older children and adults at least 14 days after onset of cough. Serology is not recommended within a year of vaccination. Genomic detection by PCR improves sensitivity. This can be performed on nasopharyngeal swabs or aspirates and is recommended on any acutely unwell child <12 months of age.
Macrolide antibiotics are first line treatment. Antibiotic therapy has limited effect on improving the clinical course but prevents secondary transmission. In 2007, a Cochrane review showed short course are as effective. Clarithromycin is recommended for neonates, erythromycin in pregnancy and azithromycin for infants, older children and adults. Neither vaccination nor natural disease confers complete or lifelong protective immunity against pertussis with immunity waning after 5–10 years. In 2012, a national UK outbreak was declared due to increase case detection. In response the Department of Health introduced an immunisation programme for pregnant women between 28 and 38 weeks gestation. Boosting maternal antibodies would thus lead to higher neonatal antibody levels.
Answer A: Klebsiella pneumoniae
K. pneumoniae is a Gram-negative member of the Enterobacteriales family. It is a lactose-fermenting coliform and is a common commensal of the gastrointestinal tract. It has the ability to acquire resistance mechanisms including plasmid mediated ESBLs. The spread of metallo-beta-lactamases such as KPC (Klebsiella producing carbapenemases) and NDM (New Delhi Metallo-beta-lactamase) within K. pneumoniae is of worldwide concern. Enterobacter spp., C freundii and M. morganii can acquire such plasmid-mediated mechanisms, but more commonly clinically relevant antimicrobial resistance is due to Ambler class C AmpC type beta-lactamases.
Answer C: Pediculus humanus humanus
Epidemic typhus (louse-borne typhus) causes epidemics following wars and natural disasters. The causative organism is Rickettsia prowazekii, transmitted by the human body louse (Pediculus humanus humanus also known as Pediculosis humanus corporis) in its faeces. The body louse is 2–4 mm in length, lives in clothes and lays eggs along the seams. The incubation period of epidemic typhus is 1–2 weeks. Symptoms include severe headache, a sustained high fever, cough, rash, severe myalgia, hypotension and delirium. The rash begins on the chest about five days after the fever appears, and spreads to the trunk and extremities. Louse infestation is often sufficiently treated by bathing the patient and heat treating the clothes and bed linen. Permethrin topically and oral ivermectin can be used in persistent cases. A randomised trial using permethrin impregnated underwear in homeless individuals failed to show sustained benefit.
Glossina spp. are known as Tsetse flies and transmit trypanosomiasis. Aedes aegypti is the vector for viruses such as dengue, chikungunya, Zika and yellow fever. A. gambiae is the vector for malaria. Culex spp. are the vectors for West Nile virus, Japanese encephalitis and Western and Eastern Equine encephalitis.
Answer B: Schistosomiasis
The Diphyllobothrium latum intermediate host is a copepod (freshwater crustacean) then a fish. Paragonamus spp. intermediate host is a crab or crayfish. Echinococcus spp. (hydatid disease) has an intermediate host of sheep, goats and swine with the definitive host of canines. Strongyloides stercoralis a free-living organism. Each human infecting schistosome has a specific snail species for an intermediate host: Schistosoma mansoni with Biomphalaria spp.; Schistosoma haematobium and Schistosoma intercalatum with Bulinus spp.; Schistosoma japonicum with Oncomelania spp.; Schistosoma mekongi with Tricula spp.
Answer A: E. dispar
E. histolytica is the causative agent of intestinal amoebiasis leading to clinical manifestations of amoebic dysentery or amoebic liver abscesses. E. histolytica has microscopic morphological similarity with two other species: E. dispar and Entamoeba moshkovskii. Entamoeba dispar is non-pathogenic but Entamoeba moshkovskii is reportedly associated with diarrhoea, but its pathogenic potential remains unclear. These can be diagnosed by stool samples but it is impossible to distinguish the three species by microscopy alone. Trophozoites may be seen in a fresh faecal smear and cysts in an ordinary stool sample. Antigen tests can distinguish between pathogenic and non-pathogenic species. Molecular techniques, such as PCR, can be used but are not widely available in clinical practice.
Answer D: IgM
Immunoglobulins, composed of two heavy chains and two light chains in a Y shape, bind antigens in a variable domain and effect functions through a constant domain. There are five classes of constant domain, defining the five isotypes of immunoglobulins: IgA, IgD, IgE, IgG, IgM. IgM immunoglobulins are the first isotypes expressed during B-cell development; naïve B-cells express IgM as a monomer on their cell surface, then once stimulated by an antigen IgM is produced as a pentamer early in a primary viral infection. However, the heavy chains in IgM have not undergone much somatic mutation in response to antigens, and tend to be more poly-reactive than other immunoglobulin isotypes. IgG is the predominant isotype and are produced by activated B-cells (i.e. plasma cells) either part way through a primary viral infection (replacing IgM production) or upon activation of memory B-cells in response to later re-exposures or reactivation of viral infections. IgA occurs as a monomer in serum but as a dimer when secreted at mucosal surfaces and in breast milk where it acts to protect these mucosal surfaces from viruses, bacteria and toxins. IgE binds with high affinity to mast cells, basophils and eosinophils once activated by an antigen – typically a helminth, although it is also associated with hypersensitivity and allergic reactions. IgD functions as an antigen receptor on naïve B-cells and can also bind basophils and mast cells in respiratory immune defence.
Answer B: C7 deficiency
Adenosine deaminase deficiency is an autosomal recessive metabolic disorder. It leads to severe combined immunodeficiency (SCID) in 90% cases with T, B and natural killer cell dysfunction. It causes an accumulation of deoxyadenosine, which causes an increase in S-adenosylhomocysteine; both of which are toxic to immature lymphocytes leading to a complete lack of both T- and B-cells. Prognosis is poor and acute recurrent infections occur in particular Pneumocystis jirovecii (PCP) pneumonia, candidiasis, herpetic infections (CMV, EBV, VZV), parainfluenza and enterovirus. Job syndrome (autosomal dominant hyperimmunoglobulin E syndrome) is characterised by abnormally high levels of immunoglobulin E. It clinically appears with recurrent skin abscesses, cystic lung infections (primarily Staphylococcus aureus and Candida), eczematous dermatitis, eosinophilia and elevated IgE levels. Patients with C7 deficiency have markedly diminished total haemolytic complement activity and little if any C7 is in their serum. Serum bactericidal activity is markedly reduced and is responsible for the increased risk of Neisseria spp. (especially Neisseria meningitidis) infections. The cause of IgM deficiency is unknown but is characterised by an absence of IgM in the presence of normal levels of IgG and IgA. Serious recurrent bacterial infections can occur from Staphylococcus aureus, encapsulated organisms (Streptococcus pneumoniae, Haemophilius influenzae) and viral infections.
Answer B: Defect in phagocyte oxidase
Phagocytes use nicotinamide adenine dinucleotide phosphate (NADPH) oxidase to generate reactive species of oxygen. CGD is caused by mutations resulting in loss of function in this process. Neutrophils, monocytes and macrophages are unable to phagocytose bacteria such as Staphylococcus aureus leading to recurrent bacterial infections.
Answer B: TLR4
TLRs are surface molecules on cells that detect and react to microbial antigens. The ligands for these receptors are parts of microbes and often called pathogen-associated molecular patterns (PAMPs). TLR4 is the principle receptor for LPS of the Gram-negative bacterium. TLR3 binds double-stranded RNA produced by many viruses. TLR5 recognises flagella of bacteria. TLR7 is similar to TLR8 and bind single-stranded RNA from viruses such as influenza and HIV. TLR10 function is not yet known.
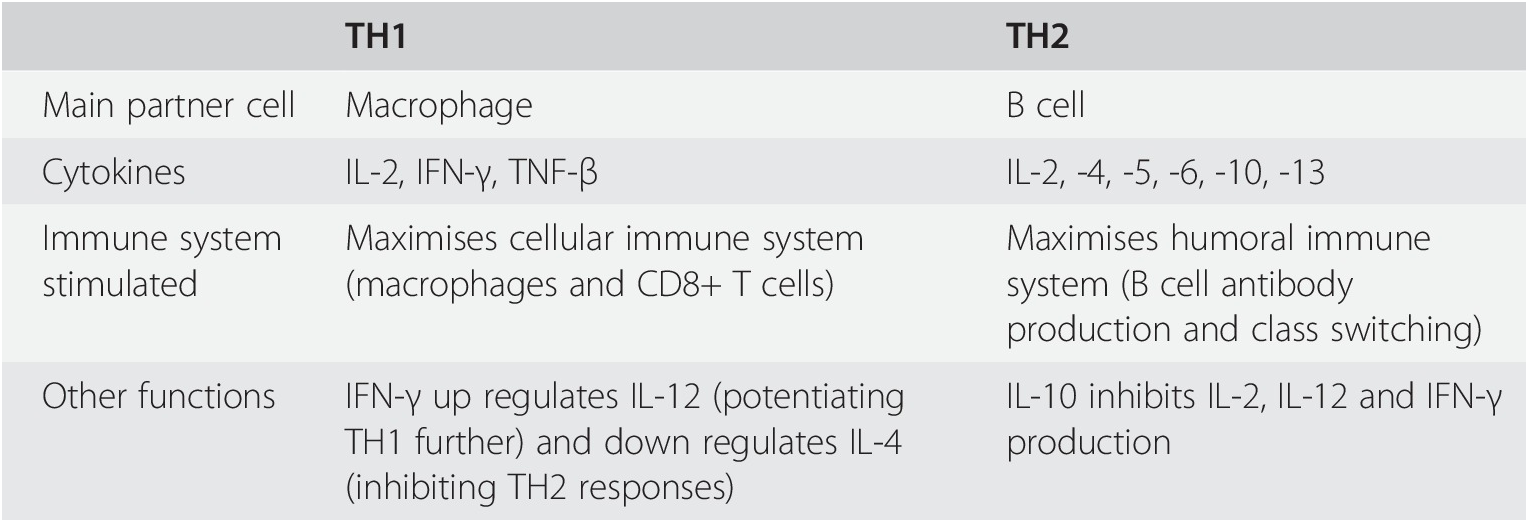
Answer C: IL2 and IFN-γ
A TH1-type response is generally associated with killing of intracellular organisms, either viruses or bacteria. Cytokines associated with a TH1 response are, therefore, typically pro-inflammatory and activate macrophages and induce opsonising/complement-fixing immunoglobulin production by B-lymphocytes. Interferon gamma is one of the main TH1 cytokines.
A TH2-type response occurs typically to combat extracellular bacteria and parasite. This leads to activation of eosinophils, basophils and dendritic cells through cytokines including interleukins 4, 5 and 13, and a degree of anti-inflammatory response through interleukin-10.
In hepatitis C, both IL-2 and IFN-γ are key cytokines associated with clearance of acute and chronic HCV. The impact of IL-2 is likely due to its role in differentiation of CD8+ T-lymphocytes into effector and long lived memory cells. The activity of IFN-γ in hepatitis C is likely attributable to its direct role in inhibiting viral replication. Untreated patients with hepatitis C who have primary clearance of the virus display high magnitude IL-2 and IFN-γ responses. Treated hepatitis C patients who display sustained virological response have a higher magnitude and maintenance levels of IL-2 and IFN-γ. Null-responder patients may have high magnitude IFN-γ responses early in infection but lack high maintenance levels.