

1. Introduction
Additive Manufacturing (AM), commonly known as 3D printing, offers designers unique capabilities for creating components with geometric, hierarchical, and material complexity (Reference Gibson, Rosen, Stucker and KhorasaniGibson et al., 2020). These capabilities enable personalised healthcare solutions, particularly when patient-specific customisation, complex geometries, and lightweight structures can improve patient outcomes (Reference Alrasheedi, Tlija, Elloumi and LouhichiAlrasheedi et al., 2025; Reference Huang, Liu and MokasdarHuang et al., 2013). Orthotic design is inherently multidisciplinary. Clinicians define therapeutic objectives, prosthetists-orthotists translate them into solutions through an assess–design–fit process, and engineers develop and fabricate the devices, together ensuring anatomically appropriate and clinically effective devices (Reference Alrasheedi, Tlija, Elloumi and LouhichiAlrasheedi et al., 2025). Conventional manufacturing, however, imposes limitations on shape complexity, material efficiency, and lead time, often resulting in generic, ill-fitting medical devices (Reference CronskärCronskär, 2014; Reference Raheem, Hameed, Whenish, Elsen, Aswin, Jaiswal, Prashanth and ManivasagamRaheem et al., 2021).
Traditional orthosis fabrication, which has long relied on plaster casting and manual shaping, is undergoing a digital transformation toward workflows based on 3D scanning, computer-aided modelling, and AM. Such workflows can reduce production time from weeks to days while improving comfort and patient compliance (Reference Hale, Linley and KalaskarHale et al., 2020). Reference Farhan, Wang, Bray, Burns and ChengFarhan et al. (2021) found that 3D scanning is faster and comparably reliable to traditional casting, although it is still dependent on operator expertise. Yet current systems remain semi-automated and rely on human interpretation to adjust designs for factors such as pressure distribution and gait dynamics, as most software still relies on static anatomical data rather than biomechanically informed models, limiting their ability to fully account for the dynamic interaction between the orthosis and the human body (Reference Alrasheedi, Tlija, Elloumi and LouhichiAlrasheedi et al., 2025). As a result, clinicians must interpret biomechanical requirements and iteratively adjust device geometry based on patient-specific needs (Reference Hale, Linley and KalaskarHale et al., 2020). These challenges highlight the need for more flexible and process-aware design methods. AM offers valuable design freedoms, including part consolidation, topology optimisation, and lattice structures, that can support the development of lightweight, patient-specific devices (Reference Gibson, Rosen, Stucker and KhorasaniGibson et al., 2020). However, the immaturity of orthosis-tailored AM design methods, sensitivity to process parameters, and the difficulty of predicting part behaviour under patient-specific loading hinder broad adoption in healthcare (Reference Abdulhameed, Al-Ahmari, Ameen and MianAbdulhameed et al., 2019). These issues complicate repeatable fit and function and increase the effort required for verification, validation, and regulatory qualification, an effect compounded by persistent gaps in regulatory guidance for medical AM (Reference Javaid and HaleemJavaid & Haleem, 2018). From a research perspective, AM’s unique design freedom has given rise to the field of Design for Additive Manufacturing (DfAM), which has emerged to help engineers harness the technology’s potential. Most DfAM prioritise performance and manufacturability and can be integrated into generative design tools.
Generative design tools provide one such pathway by synthesising multiple alternative geometries, integrating numerical optimisation with design heuristics to automatically generate designs optimised for different objectives and constraints (Reference Plocher and PanesarPlocher & Panesar, 2019). When enhanced with artificial intelligence (AI), which employs machine-learning models to recognise patterns and autonomously generate new geometries, generative design can expand the capabilities of traditional Computer-Aided Design (CAD) workflows (Reference Junk and BurkartJunk & Burkart, 2021). Generative design is described as a computational design approach based on explicit constraints, optimisation objectives, and physics-based simulations. While such methods are sometimes labelled as ‘AI-enabled’ in commercial tools, they typically do not involve learning or data-driven adaptation. In this paper, Artificial Intelligence refers specifically to machine-learning-based methods capable of learning from data and generalising beyond predefined rules. Generative AI refers to data-driven machine-learning models that learn from training data and can generate new, previously unseen outputs. This distinction is critical in the context of orthotic design, where biomechanical variability, clinical expertise, and qualification requirements exceed the expressive capacity of rule-based optimisation alone. In an engineering design context, this includes models that can synthesise geometries and help in supporting design exploration and decision-making. Although promising, the application of Generative AI to orthotic design remains underexplored (Reference Harale, Jadhav, Jadhav, Mohite and UndeHarale et al., 2025). Designers lack the structured tools and evidence-based processes to systematically explore the multifunctional design space of AM, encompassing biomechanics, ergonomics, aesthetics, validation, and certification. Hence, the purpose of this paper is to identify how designers can create a structured framework that uses AI and DfAM to enable the design, validation, and qualification of high-performance, patient-specific orthoses.
The contribution of this paper is a structured synthesis of how Generative AI could be integrated into the DfAM of orthotic devices, highlighting the opportunities, gaps, and future directions for this emerging field. To achieve this, the paper outlines the landscape of AM, DfAM, CAD, generative design and AI within orthotic design, establishing the technological foundations and challenges that motivate the review. The research method, including search strategy, screening procedures, and thematic classification, is then detailed (Section 2). The findings of the systematic review are presented across four dimensions within orthosis development (Section 3). Finally, the paper discusses the implications for future research and practice, identifies opportunities to advance Generative AI–enabled DfAM workflows, and concludes with recommendations for future work (Sections 4 and 5).
2. Method
The literature review was conducted in four stages based on the PRISMA approach (Reference Moher, Liberati, Tetzlaff and AltmanMoher et al., 2009) as illustrated in Figure 1. The review followed four PRISMA-recommended phases: article identification, duplicate screening, eligibility assessment, and qualitative synthesis. No restriction was placed on publication year.
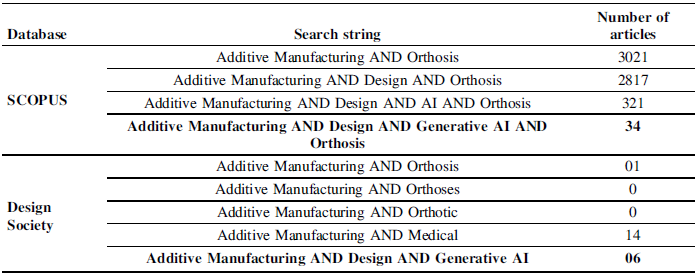
STAGE 1: SCOPUS and the Design Society Library were selected as the databases for the search. In both databases, the queries were executed using an all-fields search configuration to maximise coverage, while slightly different search strings were used to reflect each platform’s indexing and search behaviour, as shown in Table 1. For SCOPUS, the search string was (Additive Manufacturing AND Design AND Generative AI AND Orthosis), whereas for the Design Society library, the search string (Additive Manufacturing AND Design AND Generative AI) was applied. These search terms were selected to identify research that explicitly referenced the use of Generative AI within DfAM. The search strings were tailored to each database’s characteristics to balance specificity and comprehensiveness.
The search string (Additive Manufacturing AND Design AND Generative AI AND Orthosis) was used to target literature that was directly relevant to the review’s scope. However, applying this narrow search across all platforms risked missing relevant work in sources with different indexing or narrower subject coverage. The same search string was applied in the Design Society database, yielding no results. Therefore, the search string was broadened to (Additive Manufacturing AND Design AND Generative AI), without the precise keyword “Orthosis”, to capture related research, as shown in Table 1.
The results of the systematic literature search

This broader search string was used to capture relevant studies, as the narrow search returned no records in the Design Society database. In all searches, “Additive Manufacturing” was treated inclusively to encompass all major AM processes, and no restrictions were placed on materials, ensuring that studies using polymers, metals, and composites were all captured.
Flow diagram of the systematic review process (based on Reference Moher, Liberati, Tetzlaff and AltmanMoher et al., 2009)

STAGE 2: Once the database searches were completed, the initial article lists were compiled in Microsoft Excel. Conditional formatting was used to identify duplicates, which were then manually verified and removed.
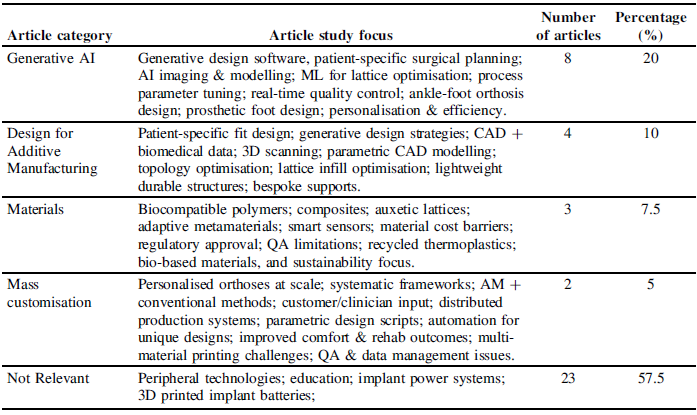
STAGE 3: The initial purpose of the review was to identify studies explicitly addressing Generative AI within the context of Design for Additive Manufacturing of orthotic devices. After compiling the articles, each was scanned and cursorily read to determine its main theme and the article’s study focus based on its title and abstract. Articles were then categorised into one of five thematic groups to understand the distribution of research related to Generative AI in DfAM of orthotic devices: Generative AI, Design for Additive Manufacturing, Materials, Mass Customisation, and Not Relevant. The final category was used to exclude studies not directly related to the research focus, such as those addressing peripheral technologies, educational applications, implant power systems, and 3D-printed implant batteries. Relevance was assessed according to whether each article directly addresses any of the following: AM applied to orthotic or medical devices; design for AM (DfAM); generative design or topology optimisation for wearable healthcare devices; Artificial Intelligence applied to AM, design, qualification and quality control for personalised medical devices; usability considerations for wearable devices; and clinical, qualification, or regulatory aspects of such products. One author performed the initial eligibility assessment and categorisation, and the other authors subsequently reviewed, approved, and/or reclassified. Table 2 provides a summary of the paper categorisations and an overview of the article study focuses identified.
Paper categorisation, definitions, number of articles, and percentage of articles

STAGE 4: After completing the eligibility assessment, 17 articles were retained for qualitative synthesis. One week after the initial search, follow-up searches were conducted by repeating the original searches in both databases, yielding one additional article, which was excluded after assessment.
The number and proportion of articles at each stage of the review process are presented in Figure 1. The findings from this synthesis are discussed in the following section, which examines how Generative AI is being integrated with AM in the design and production of orthotic devices.
3. Findings – generative AI in the design for AM of orthotic devices
The review identified 40 relevant articles in the screening phase published between 2015 and 2025, with publication activity steadily increasing, particularly from 2022 onwards. This growth reflects rising interest in the combined use of Generative AI and AM within orthotic design. Recent work suggests that Generative AI is being increasingly integrated with AM to support the creation of patient-specific orthoses and supportive devices (Reference Harale, Jadhav, Jadhav, Mohite and UndeHarale et al., 2025). Reference Harale, Jadhav, Jadhav, Mohite and UndeHarale et al. (2025) highlight how AI-driven methods are being utilised in conjunction with the geometric freedom of AM to automate design steps, enhance personalisation, and deliver functionally optimised orthotic solutions. Similar observations are made by Reference Mikołajewska, Mikołajewski, Mikolajczyk and PaczkowskiMikołajewska et al. (2025), who report that combining AI-based design approaches with AM enables the production of highly customised, functionally optimised orthotic devices.
The following review is structured into four sections that examine key dimensions of this convergence. Generative AI discusses how AI techniques, such as predictive modelling and generative design algorithms, are being used to enhance AM processes and outcomes in orthosis development. Design for additive manufacturing explores design methodologies that combine advanced CAD tools, topology optimisation strategies, and biomechanical data to fully leverage AM’s geometric freedom, enabling the creation of patient-specific orthoses. Materials reviews development in printable materials, ranging from new polymers and metamaterials to biocompatibility and regulatory considerations, that influence the performance and clinical adoption of 3D-printed orthoses. Mass customisation examines how AM facilitates the scalable production of patient-specific orthotic devices, highlighting frameworks, challenges and enablers for implementing patient-specific orthoses at scale; materials and mass customisation govern feasibility and clinical adoption. Together, these sections illustrate that the combination of Generative AI and AM has the potential to accelerate orthosis design, moving from universal to data-driven, individually optimised devices.
3.1. Generative AI
Research indicates a strong interaction between AI and AM in advancing orthosis design and fabrication (Reference Liu, Tian and KanLiu et al., 2022). Clinically, AI has been used to enhance medical imaging, modelling, and decision-making for 3D-printed orthopaedics (Reference Harale, Jadhav, Jadhav, Mohite and UndeHarale et al., 2025). Reference Harale, Jadhav, Jadhav, Mohite and UndeHarale et al. (2025) highlight that combining AI algorithms with 3D printing enables patient-specific surgical planning, the fabrication of custom implants and orthoses, and improved outcomes, such as faster recovery and reduced complications. From an engineering perspective, AI is transforming the design and production workflows of AM products (Reference Pancholi, Gupta, Bartoszuk, Vashishtha, Ross, Korkmaz, Krolczyk and PetruPancholi, 2025). An overview of Generative AI highlights that machine learning and generative design techniques are being applied at multiple stages, from optimising complex lattice designs and topology for weight reduction to automating process parameter tuning and real-time quality control during printing. While the former emphasises AI’s role in personalised patient care, the latter focuses on manufacturing efficiency and precision, together highlighting AI’s broad impact (Reference Pancholi, Gupta, Bartoszuk, Vashishtha, Ross, Korkmaz, Krolczyk and PetruPancholi et al., 2025). Reference Jhunjhunwala and NarayanJhunjhunwala and Narayan (2025) outline generative design strategies for wearable assistive devices, showing that generative methods can address objectives such as lightweighting, adjustability, and actuator load reduction relevant to orthoses. Their work presents a “selection philosophy” that connects design goals to generative algorithms, represented through AI-based ankle-foot orthosis (AFO) design. Similarly, Reference Morano-Okuno, Esqueda, Chong-Quero, Sandoval-Benitez, Murano-Labastida and Jaramillo-GodinezMorano-Okuno et al. (2024) applied AI-powered software to generate complex prosthetic foot designs that a human designer might not have conceived. The success of such a generative design tool in creating an AFO demonstrates the potential of AI to innovate orthosis geometries as well (Reference Morano-Okuno, Esqueda, Chong-Quero, Sandoval-Benitez, Murano-Labastida and Jaramillo-GodinezMorano-Okuno et al., 2024). Collectively, these findings show that AI can significantly enhance AM for orthotics by augmenting design creativity, personalisation, and production efficiency. Taken together, these studies suggest that integrating AI into AM can produce orthotic devices that are more patient-specific and higher-performing than those generated by conventional approaches, marking a new era in intelligent orthosis development.
3.2. Design for additive manufacturing
AM enables designers to produce complex geometries that are impractical or uneconomical to fabricate using conventional methods (Reference Chen and SheaChen & Shea, 2015). Generative design can produce intricate, efficient forms, including structures like those found in nature, thereby optimising material use and mechanical performance (Reference LobosLobos, 2018). Hence, DfAM approaches are evolving to meet the needs of custom orthosis production (Reference Farrugia, Cassar, Vella, Abela, Wodehouse and TamburrinoFarrugia et al., 2023).
Reference GorskiGorski (2025) demonstrates how the advanced CAD tools can be integrated with biomedical data to tailor devices to individual anatomies. Reference GorskiGorski (2025) outlines a comprehensive framework that combines 3D scanning, parametric CAD modelling, and AM to create anatomically shaped medical devices, including orthopaedic orthoses, that are tailored to each patient. This approach connects engineering and medicine by using medical imaging data (e.g., hand scans) to guide CAD design, ensuring a 3D-printed orthosis closely matches the patient’s anatomy. Case studies by Reference GorskiGorski (2025) on orthopaedic devices demonstrate that CAD methodologies developed in collaboration with clinicians can streamline the design process while enhancing fit and functionality.
Similarly, Reference García-Domínguez, Claver-Gil and SebastiánGarcía-Domínguez et al. (2020) propose a parametric design methodology in which orthotic parts are formulated as optimisation problems for the computer to solve, rather than manually drawn shapes. In this method, generative algorithms automatically explore design alternatives and optimise the structure (e.g., internal lattice infill and shell geometry) for minimal weight and adequate strength. AM’s geometric freedom enables the AI-generated, optimised design to be physically realised, resulting in complex, performance-driven orthoses that conventional methods could not produce.
Together, the biomedical framework described by Reference GorskiGorski (2025) and the algorithmic approach of Reference García-Domínguez, Claver-Gil and SebastiánGarcía-Domínguez et al. (2020) highlight the complementary roles of clinician input and computational automation in the design of orthoses. Reference GorskiGorski (2025) emphasises the importance of capturing patient-specific requirements and clinician input; Reference García-Domínguez, Claver-Gil and SebastiánGarcía-Domínguez et al. (2020) show how automation can produce highly efficient designs beyond the traditional sense. In practice, leveraging generative design and topology optimisation has enabled designers to create lightweight yet durable orthotic structures tailored to patients’ specific needs. For example, Reference Jhunjhunwala and NarayanJhunjhunwala and Narayan (2025) achieved significant weight reduction in an orthotic device by optimising its internal lattice structure through generative methods. Further, custom-fit 3D-printed orthoses improve patient comfort and outcomes, emphasising the benefits of combining human-centred and AI-driven design approaches (Reference GorskiGorski, 2025).
In summary, modern orthosis design is increasingly exploiting AM through advanced DfAM strategies that integrate patient data, CAD, and generative optimisation (Reference Farrugia, Cassar, Vella, Abela, Wodehouse and TamburrinoFarrugia et al., 2023). These design innovations ensure that AM orthoses can be precisely fitted and performance-optimised, demonstrating how Generative AI tools are enhancing the efficiency of orthoses for patients.
3.3. Materials
Materials play a critical role in the success of additively manufactured orthoses. Reference Moroni and MajewskaMoroni and Majewska’s (2025) current research addresses both the opportunities and challenges. They highlight that AM enables the use of innovative materials and structures that can improve orthosis function. For example, new biocompatible polymers and composites can be 3D-printed into orthoses that promote better integration with the body and even aid rehabilitation. Another advancement is the design of metamaterial structures within orthoses: auxetic lattices (materials with a negative Poisson’s ratio) have been highlighted for their ability to conform and flex under load. Reference Moroni and MajewskaMoroni and Majewska (2025) shows that an orthosis incorporating auxetic lattice segments can dynamically adapt to a patient’s movements while maintaining stability and support. Alongside these benefits, however, Reference Paxton, Zhao and SauretPaxton et al. (2024) acknowledge significant material-related challenges in bringing AM orthoses into wider use.
A systematic review by Reference Fianko, Dzogbewu, Agbamava and de BeerFianko et al. (2025) found that limited availability of materials and insufficient quality assurance are key obstacles to scaling up 3D printing for medical devices. Similarly, another study by Reference Harale, Jadhav, Jadhav, Mohite and UndeHarale et al. (2025) states that, despite the promise of AM, conventional fabrication methods remain dominant for orthotic production, in part due to high material costs and regulatory hurdles in approving new materials for clinical use. Thus, hospitals and clinics may be slow to adopt 3D-printed orthoses if the materials are expensive or not yet certified for safety. There is a need to establish standards and long-term data on printed orthosis materials; without such data, professionals are likely to remain cautious in adopting these technologies. To address these issues, research is focusing on rigorous testing protocols and on developing materials specifically for medical AM that meet regulatory requirements (Reference Mishra and SinghMishra & Singh, 2025). Another emerging consideration is sustainability in material choices. For instance, Reference Harale, Jadhav, Jadhav, Mohite and UndeHarale et al. (2025) noted that the use of recycled thermoplastics in 3D printing has been explored for the creation of orthopaedic casts, aiming to reduce waste while maintaining functionality. Such efforts provide eco-friendly healthcare solutions, suggesting that future orthoses might use recycled or bio-based materials without sacrificing performance.
From a materials perspective, innovations such as auxetic lattices and new biocompatible polymers are advancing orthosis design through AM, enabling more comfortable, functional, and even smart devices. At the same time, material-related barriers, cost, regulatory approval, and quality consistency must be overcome for these advancements to fully translate into routine clinical use (Reference Moroni and MajewskaMoroni & Majewska, 2025). Overall, progress in materials science is fundamental to the development of Generative AI-driven orthoses, as the choice of printable material and its properties ultimately determine the orthosis’s safety, comfort, and effectiveness for the patient (Reference Mishra and SinghMishra & Singh, 2025).
3.4. Mass customisation
AM is acknowledged for transforming mass customisation into production, allowing the efficient fabrication of patient-specific orthotic devices (Reference Klenam, McBagonluri, Asumadu, Osafo, Bodunrin, Agyepong, Osei, Mornah and SoboyejoKlenam et al., 2025). Traditional methods made it difficult and costly to customise every orthosis, but AM technology changes that by allowing designers to create personalised designs on a large scale. A systematic review by Reference Fianko, Dzogbewu, Agbamava and de BeerFianko et al. (2025) on mass customisation strategies confirms that AM enables personalised production with good efficiency, drawing on evidence from many studies that unique, patient-specific parts can be produced with competitive lead times relative to conventional approaches for selected device classes and workflow configurations, particularly when scan-to-design steps are streamlined and printing capacity is appropriately scaled. The review highlights strategies for achieving mass customisation with AM, combining 3D printing with traditional methods, involving customers in the design process, and utilising flexible, distributed production systems. Overall, it argues that manufacturing processes must be redesigned to leverage AM’s adaptability, such as using generative design to create patient-specific orthoses. Reference García-Domínguez, Claver-Gil and SebastiánGarcía-Domínguez et al. (2020) demonstrate in their illustrative case study the use of parametric design software, such as Grasshopper scripts, which can take a set of patient measurements and provide, as output, a ready-to-print orthosis model on demand. Such approaches demonstrate how automation enables the efficient production of multiple unique designs rather than producing a single design repeatedly. Reference Mikołajewska, Mikołajewski, Mikolajczyk and PaczkowskiMikołajewska et al. (2025) found that when custom-fitted orthoses are fabricated via 3D printing, patients experience better comfort, higher satisfaction, and improved rehabilitation outcomes compared to off-the-shelf devices. Likewise, Reference Jhunjhunwala and NarayanJhunjhunwala and Narayan’s (2025) design methodologies emphasise that personalised devices can address diverse patient needs; different orthotic pat (ankle braces, knee supports, etc.) each require design parameters that generative design can accommodate on an individual patient basis. However, Reference Paxton, Zhao and SauretPaxton et al. (2024) point out that achieving mass customisation in practice is not without challenges. Technological facilitators like multi-material 3D printing and end-to-end digital workflow integration are still in their initial phase; not all clinics have the capacity to print multi-materials to fine-tune an orthosis’s flexibility or to integrate Generative AI design tools. There are also practical obstacles, i.e. limited material availability and quality-control concerns, that make it challenging to ensure that every custom-printed orthosis meets medical standards (Reference Fianko, Dzogbewu, Agbamava and de BeerFianko et al., 2025).
Additionally, managing large data files, such as 3D scan data, design files, and patient data for potentially thousands of unique devices, raises significant challenges in data management and privacy. Regardless of these hurdles, personalised care is preferable. Researchers are developing implementation frameworks that address strategic, technical, and operational aspects of scaling up custom AM production. In the context of orthoses, this means creating systems in which a patient can be scanned, their orthosis digitally designed (possibly with the assistance of AI), and fabricated in a streamlined, consistently reliable process for everyone (Reference GorskiGorski, 2025). In conclusion, AM-driven mass customisation has the potential to significantly improve orthotic care by providing adapted support for every patient. The convergence of Generative AI design tools and flexible 3D printing processes enables a high degree of personalisation; each orthosis can be uniquely optimised for its user, without the unaffordable costs and fabrication lead times (Reference García-Domínguez, Claver-Gil and SebastiánGarcía-Domínguez et al., 2020). As the remaining challenges (material qualifications, quality assurance, and workflow integration) are addressed, we can expect generative AM approaches to deliver fully patient-specific orthoses at scale, fulfilling the promise of mass customisation in healthcare (Reference Klenam, McBagonluri, Asumadu, Osafo, Bodunrin, Agyepong, Osei, Mornah and SoboyejoKlenam et al., 2025).
4. Discussion
The literature review indicates that integrating Generative AI with AM expands orthotic design by enabling automated exploration of complex geometries and multi-objective optimisation across comfort, support, and weight. The work highlights a shift from experience-driven manual processes toward computationally supported, patient-specific workflows that incorporate DfAM constraints and balance clinical and manufacturing requirements. This interpretation is consistent with Reference Harale, Jadhav, Jadhav, Mohite and UndeHarale et al. (2025) and Reference Pancholi, Gupta, Bartoszuk, Vashishtha, Ross, Korkmaz, Krolczyk and PetruPancholi et al. (2025), who highlight that AI-enabled optimisation enlarges the design space beyond conventional techniques. Comparable claims are made by Reference Jhunjhunwala and NarayanJhunjhunwala and Narayan (2025) and Reference Morano-Okuno, Esqueda, Chong-Quero, Sandoval-Benitez, Murano-Labastida and Jaramillo-GodinezMorano-Okuno et al. (2024), who demonstrate that generative and topology-optimised structures can achieve strength-to-weight ratios that surpass those of traditional designs. Furthermore, studies on digital workflows, such as 3D scanning and parametric CAD, show that patient-specific geometry can be more accurately captured, supporting improved anatomical fidelity during fabrication. These findings align with broader results indicating that 3D-printed, custom-fitted orthoses improve comfort, satisfaction, and rehabilitation outcomes compared to standard devices (Reference Klenam, McBagonluri, Asumadu, Osafo, Bodunrin, Agyepong, Osei, Mornah and SoboyejoKlenam et al., 2025; Reference Mikołajewska, Mikołajewski, Mikolajczyk and PaczkowskiMikołajewska et al., 2025). Figure 2 presents a conceptual workflow framework for integrating Generative AI and DfAM to produce orthoses based on the findings of the review and explicitly grounded in the results synthesised in Section 3, thereby strengthening its evidence base.
Conceptual workflow of generative AI-enabled DfAM for orthotic device development

In contrast to traditional fabrication, which often results in generic, one-size-fits-all supports, Generative AI combined with AM can generate intricate lattice structures to improve comfort and function that human designers may not intuitively conceive. This capability extends beyond conventional manual workflows and allows bespoke devices to be tailored to individual biomechanics. However, these advantages remain contingent on successfully incorporating printability, support strategies, and post-processing limitations into the generative workflow. This result is consistent with observations that AM variability, limited multi-material options, and regulatory uncertainty constrain the manufacturability of patient-specific devices (Reference Paxton, Zhao and SauretPaxton et al., 2024).
Despite notable technical progress, the review identifies a persistent gap between computational demonstrations and clinically validated generative AM workflows. Although several studies report promising prototypes and simulations (Reference Jhunjhunwala and NarayanJhunjhunwala & Narayan, 2025; Reference Morano-Okuno, Esqueda, Chong-Quero, Sandoval-Benitez, Murano-Labastida and Jaramillo-GodinezMorano-Okuno et al., 2024), few evaluate generatively designed orthoses under real-world functional loading or assess their compliance with medical qualification requirements. This gap is consistent with Reference Harale, Jadhav, Jadhav, Mohite and UndeHarale et al. (2025) and Reference Mishra and SinghMishra and Singh (2025), who note an absence of fully established end-to-end workflows for AI-generated orthoses. Material availability, biocompatibility certification, and quality assurance procedures also remain major obstacles to clinical translation (Reference Paxton, Zhao and SauretPaxton et al., 2024). As observed across the literature, uncertainties related to privacy, data management, and scan-to-design reproducibility further slow the progression from prototype to practice.
Current approaches additionally show limited integration of patient-specific biomechanics, such as gait dynamics and pressure distribution, into generative design pipelines. While anatomical data are often incorporated through parametric or scan-based modelling (Reference García-Domínguez, Claver-Gil and SebastiánGarcía-Domínguez et al., 2020), dynamic biomechanical information is rarely used to inform optimisation objectives. Hence, many designs do not fully reflect real-world loading conditions or functional movement requirements. This gap suggests a need for more sophisticated models that connect anatomical variability, biomechanical demands, and AM constraints within a coherent generative framework.
The review also highlights a lack of translational infrastructure necessary for routine clinical adoption. Although some authors propose digital twins, sensor-integrated systems, and feedback-driven processes (Reference Mishra and SinghMishra & Singh, 2025), the field lacks large, standardised anatomical datasets, validated AM process controls, interpretable AI models, and clear regulatory pathways. This observation parallels concerns raised in the material science and medical device literature, where uncertified polymers, unreliable post-processing methods, and ambiguous qualification standards limit scalable deployment (Reference Paxton, Zhao and SauretPaxton et al., 2024). Collectively, these findings indicate that the barriers to adoption lie not in algorithm development but in the absence of integrated, validated, and clinically trustworthy design-to-fabrication pipelines.
Overall, the review demonstrates substantial technical potential for Generative AI–enabled design for AM (DfAM) to deliver lightweight, biomechanically responsive, and anatomically precise orthoses. However, realising these benefits requires overcoming gaps in biomechanical data integration, material certification, manufacturing reliability, workflow standardisation, regulatory clarity, and clinical validation. By addressing these methodological and practical gaps, the theoretical benefits of Generative AI can be implemented successfully in patient care.
5. Conclusions and future work
The review highlights the transformative potential of integrating Generative AI, AM, and advanced DfAM strategies, combining patient-specific data, parametric CAD, and AI-based optimisation, to produce lightweight, precisely fitted, performance-optimised orthoses tailored to individual users, while enabling scalable mass customisation. New biocompatible materials and metamaterials promise further gains in comfort and dynamic performance. Figure 2 illustrates this integrated Generative AI–DfAM workflow for orthosis design. Integrating AM with AI-enabled generative design has the potential to accelerate innovation in the healthcare industry by enabling the creation of orthotic devices that are both highly functional and tailored to individual anatomy.
However, current research is largely exploratory or simulation-based, with limited incorporation of biomechanics or gait dynamics and no validated end-to-end generative design-to-print workflows. Anatomical datasets are small and heterogeneous, while certified, biocompatible multi-material options and standardised post-processing methods remain scarce. AM process variability, support structure constraints, and insufficient in-situ quality control also complicate reliable fabrication. Regulatory pathways, explainability requirements, digital data management, and clinician workflow integration remain underdeveloped. Together with privacy and data management challenges in handling patient scans, these limitations slow the translation of research into practice. Future progress will depend on coordinated advances in biomechanics-integrated generative design methods, dataset development, human digital twins and feedback-driven manufacturing, material and process qualification, rigorous clinical trials, and stronger interdisciplinary collaboration among engineers, clinicians, materials scientists, and regulatory experts, although these are not covered in depth in this paper. Researchers should also investigate new printable polymers and metamaterials, as well as post-processing techniques, to ensure that orthoses are safe, durable, and comfortable for patients.
Ultimately, achieving the full potential of AI-driven orthotic design will require close collaboration across disciplines and clinical validation at every stage. Only through such efforts can the Generative AI methods outlined here be translated into reliable, patient-specific orthotic solutions.
Acknowledgement
Thanks to Prof. Marco Luigi Giuseppe Grasso at Politecnico di Milano for his support.



 Open access
Open access