


Blood-based biomarkers have emerged as promising tools within the diagnostic pathway for Alzheimer’s disease. Confirmation of amyloid pathology usually requires cerebrospinal fluid analysis or positron emission tomography imaging, both of which are informative but costly and difficult to scale in routine care. The May 2025 clearance by the Food and Drug Administration of the Lumipulse G pTau217/β-Amyloid 1-42 plasma ratio test marked the first authorisation of such an assay for clinical use, with potential implications for clinical assessment and treatment planning. 1
The February 2026 recall was not a failure but an early warning. Manufacturing variability, temperature excursions, freeze–thaw cycles and lot-to-lot differences raised concerns about the consistency of results across production and laboratory workflows before widespread adoption. 2 These issues highlight a critical distinction between assay performance under initial validation conditions and its reliability in routine clinical use. Results seen during initial validation may not be reproduced in practice, where variation in sample handling and laboratory processes can influence assay performance. Real-world practice introduces additional sources of heterogeneity, including differences in patient populations, institutional workflows and the practice context in which testing is performed and interpreted. This variability may matter most when results are borderline, as small differences may change classification and affect diagnostic interpretation. Reference Ashton, Keshavan, Brum, Andreasson, Arslan and Droescher3,Reference Grande, Valletta, Rizzuto, Xia, Qiu and Orsini4 The key lesson is clear: good technical performance alone cannot ensure that results remain consistent and reliable in routine use.
Timing is another relevant issue. In many validation cohorts, blood sampling and clinical confirmation are separated by a substantial interval. In routine care, however, testing is often requested when patients first reach specialist assessment, while the broader clinical picture is still being established. Performance estimates based on later confirmation therefore do not always reflect the setting in which the assay is actually used. This difference in timing can affect how well performance estimates translate to practice. It is especially relevant in services in which blood-based biomarkers inform initial clinical interpretation before the context is fully resolved, as the meaning of a result can differ according to when in the pathway the test is used. This point is important because performance in validation cohorts is often assessed under temporal and clinical conditions that differ from those in which uncertainty first arises in routine care. The same result can therefore carry different practical implications when considered at first presentation, when uncertainty remains high, than when interpreted later against a more fully characterised clinical and biological context.
For practising psychiatrists, the clinical value of a blood-based biomarker depends on how well it fits the overall clinical assessment. For example, a result suggestive of amyloid pathology can still require confirmatory evaluation through additional clinical or biological measures when the overall presentation remains unclear. It is also helpful to know which assay was used and to interpret the result in light of its intended use and local reporting context. This is particularly important in settings in which cognitive symptoms overlap with affective, behavioural or other neuropsychiatric presentations that complicate early interpretation. In such cases, biomarker results can support clinical judgement, but they are unlikely to be sufficient in isolation. Their usefulness depends not only on assay characteristics, but also on how the result is situated with respect to the patient’s symptoms and history, and the clinical context.
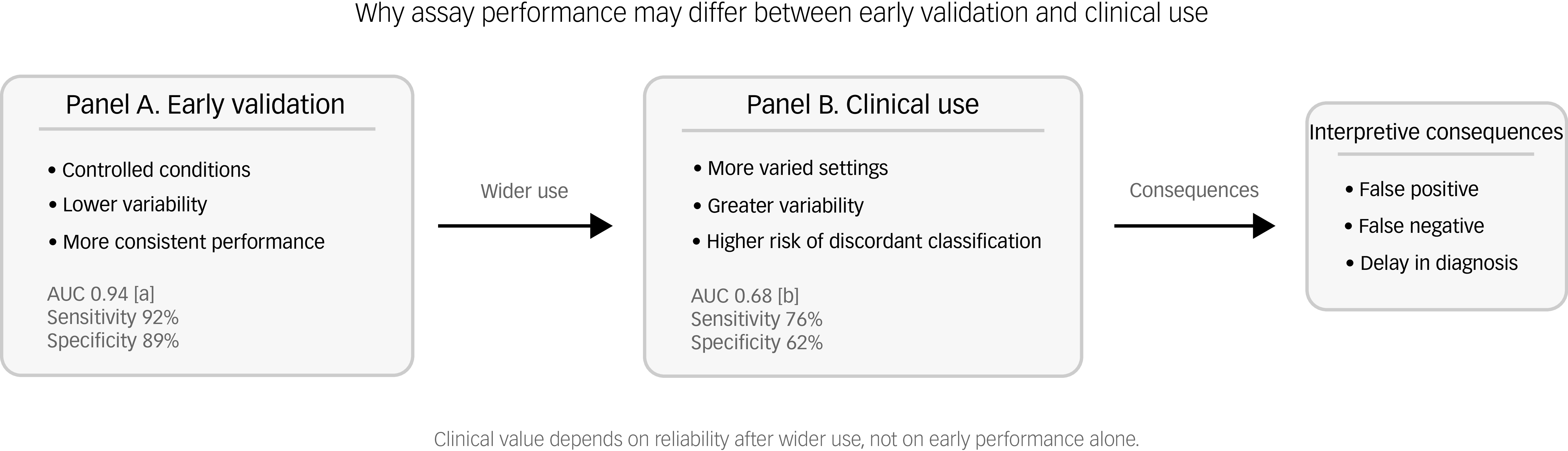
Although this episode occurred in the context of Alzheimer’s disease, it also highlights a broader issue in the clinical use of blood-based biomarkers. Performance observed during validation is not always sustained once testing moves into routine care across more variable settings (Fig. 1). Robust implementation depends on responsibilities beyond direct patient care. Manufacturers need timely corrective action when assay-related concerns arise, whereas laboratories need consistent procedures and attention to comparability across sites, as differences between services may contribute to discordant classifications. Reference Ashton, Keshavan, Brum, Andreasson, Arslan and Droescher3,Reference Magnelli, Pagano and Sabbatini6 The interval between clinical clearance in May 2025 and recall in February 2026 is therefore informative, suggesting that some problems become visible only after testing moves into broader clinical use, when results may already influence assessment, further testing and follow-up decisions. This highlights why post-release scrutiny remains necessary even after a biomarker crosses an important regulatory threshold.
Conceptual illustration of biomarker performance in early validation and in clinical use, showing how assay performance may differ once testing moves beyond early validation and into broader clinical use, in a more controlled validation context (left) and across more heterogeneous settings (middle). Performance values for early validation and clinical use were adapted from refs. Reference Fu and Ho8,Reference West9 , respectively. AUC, area under the curve.

Blood-based biomarkers remain an important development in Alzheimer’s disease assessment. As Alzheimer pathology is increasingly recognised beyond highly selected specialist populations, such biomarkers are likely to become more relevant to routine pathways. Reference Aarsland, Sunde, Tovar-Rios, Leuzy, Fladby and Zetterberg7 For psychiatrists, the practical challenge is how such results should contribute to assessment while remaining only one part of the overall diagnostic process. In practice, their value will depend on whether they clarify clinical uncertainty without displacing the broader clinical evaluation.
The February 2026 episode did not undermine the promise of blood-based biomarkers, but it did clarify the conditions required for their clinical value to hold in practice. Initial performance alone is not enough if results do not remain reliable once testing moves into routine clinical use. Their value will depend on whether they remain robust beyond initial validation settings. As well as being a regulatory event, this was a reminder that initial findings are not enough unless reliability is sustained in practice.
Acknowledgements
During the preparation of this manuscript, Trinka AI on macOS (Sequoia 15, Crimson Interactive Pvt. Ltd., Singapore; https://www.trinka.ai) and DeepL Write Trinka AI on macOS (Sequoia 15, DeepL SE, Cologne, Germany; https://www.deepl.com/write) were used to improve the clarity, grammar and readability of the English text. The authors reviewed and edited the manuscript after using these tools and assume full responsibility for the final content.
Author contributions
All authors contributed to conceptualisation and writing of the original draft, and read and approved the final version of the manuscript.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.

eLetters
No eLetters have been published for this article.