



Significant outcomes
-
• Phytopharmaceuticals have a promising role as a complementary or alternative option for dementia patients who cannot tolerate or respond to standard medications.
-
• Certain phytopharmaceuticals demonstrated comparable short-term symptomatic effects to standard treatments in small trials; however, evidence is insufficient to support equivalence or superiority.
Limitations
-
• Many of the studies reviewed are limited by very small sample sizes, which is associated with a high risk of bias when interpreting large effect sizes (Cohen’s d).
-
• The short duration of interventions (often only 3 to 6 months) is insufficient to assess whether phytotherapeutics can constitute disease-modifying treatments (DMTs).
Introduction
Sociodemographic implications
The dynamic development of modern medicine has allowed for an increase in the average human lifespan. However, a natural consequence of this phenomenon is demographic ageing; people are living longer and healthier lives, thus the world’s percentage of older people has increased. Statistics for dementia and Alzheimer’s disease, affecting mostly older people (over 65 y.o.), increase hand in hand with the demographic ageing. In 2020 it was estimated that over 55 million people worldwide were suffering from dementia, and it is predicted to double every 20 years (ADI – Dementia statistics, n.d.).
The challenges of Alzheimer’s and dementia goes further than health, and are recognised as an immense socioeconomic burden. Such conditions impact not only the affected individuals but also their families and close communities. The caregivers are exposed to severe distress, as well as social isolation (‘World-Alzheimer-Report-2024.pdf’, no date; no date a). Just in the United States the total costs of Alzheimer’s and dementia patient care was estimated at 384 billion dollars. In Europe those costs vary depending on the country and reach from 163 million EUR to over 32 billion EUR (Jönsson, Reference Jönsson2022).
Despite the growing number of clinical trials evaluating natural remedies, a thorough synthesis of the results is necessary to assess their true place in therapeutic regimens for AD, VaD, and MCI.
Dementia – with emphasis on diagnostic methods
Dementia is not a single health disorder, rather a group of symptoms that can develop on many different origins. The main indicator of dementia is a significant loss of cognition that interferes with everyday tasks, and others include difficulty focusing, planning, problem solving, and behavioural changes, such as apathy, anxiety, or depression (Gale et al., Reference Gale, Acar and Daffner2018; Wilbur, Reference Wilbur2023).
The leading cause of dementia is Alzheimer’s disease (AD), a neurodegenerative disorder. The pathological accumulation of amyloid-beta (Aβ) and hyperphosphorylated tau proteins leads to weakening or loss of synapses, and progressive neurodegeneration. In addition, metabolic, vascular, and inflammatory changes, along with other coexisting pathologies, play a crucial role in the development and progression of the disease (Soria Lopez et al., Reference Soria Lopez, González and Léger2019).
Vascular dementia (VaD) is the second most common cause of dementia. It encompasses a broad spectrum of cognitive impairments resulting from cerebrovascular disease. These causes include small vessel disease, territorial infarcts, and strategic infarcts. VaD often coexists with AD, leading to mixed dementia (Chang Wong & Chang Chui, Reference Chang Wong and Chang Chui2022).
Between a normal age-related cognitive decline and dementia there is a stage of mild cognitive impairment (MCI). At this stage the patient already presents a decline in cognition but it does not significantly interfere with their daily activities. It can also be an outcome of a different underlying disease or a brain injury (Sanford, Reference Sanford2017; Jongsiriyanyong & Limpawattana, Reference Jongsiriyanyong and Limpawattana2018).
To assess the severity of dementia, neurologists and neuroscientists developed many guidelines, including screening tools. The most common is Mini-Mental Status Examination (MMSE), which is used to assess cognitive impairment. It was developed in 1975 and is used to this day. The MMSE is widely applied due to its practicality and short time to run. It consists of 11 questions, covering 5 aspects of cognitive function: orientation, registration, attention and calculation, recall, and language. The maximum score is 30 points, and 23 points or lower indicate a cognitive impairment. Additionally, when used repeatedly, the instrument can track changes in cognitive status that could potentially respond to intervention (Kurlowicz & Wallace, Reference Kurlowicz and Wallace1999).
The second major tool is the Montreal Cognitive Assessment (MoCA). It is a validated tool used since the 2000, that takes about 10 minutes to complete. It assesses 6 different areas of cognition: short-term memory, visuospatial abilities, executive functions, attention, concentration, and working memory, language, orientation to time and place. The maximum score is 30 points, with the recommendation of applying a 26 point cut-off for cognitive impairment (mocacognition.com, n.d.). Recent comparative studies of MoCA and MMSE have consistently indicated that MoCA exhibits greater diagnostic efficacy than MMSE, mainly due to a better sensitivity (Pinto et al., Reference Pinto, Machado, Bulgacov, Rodrigues-Júnior, Costa, Ximenes and Sougey2019; Siqueira et al., Reference Siqueira, Hagemann, Coelho, Santos and Bertolucci2019; Jia et al., Reference Jia, Wang, Huang, Su, Du, Jiang, Wang, Wang, Wang, Su, Xiao, Wang and Zhang2021). Nevertheless, both tests are still widely being used.
The Alzheimer’s Disease (AD) Assessment Scale-Cognitive Subscale (ADAS-Cog) is a major tool used for assessing the cognitive deficits in patients with AD. Its main application is for monitoring the efficacy of antidementia treatments. The cognitive subscale of the ADAS-Cog comprises 11 tasks, including both self-administered and observer-based assessments, designed to evaluate functions such as word recall, naming objects and fingers, following commands, constructional and ideational praxis, orientation, word recognition, language abilities, comprehension of spoken language, word-finding difficulties, and remembering test instructions (Kueper et al., Reference Kueper, Speechley and Montero-Odasson.d.).
Beside rating the cognitive decline, it is important to assess psychological consequences of dementia, which are known as Behavioural and Psychological Symptoms of Dementia (BPSD). The tools used for this rating are: Behaviour Rating Scale for Dementia (BRSD), Behavioural Pathology in Alzheimer’s Disease (BEHAVE-AD), Cohen-Mansfield Agitation Inventory (CMAI), and Neuropsychiatric Inventory (NPI). The BRSD measures a wide range of psychopathology, such as depressive symptoms, psychotic symptoms, aggression, and apathy. The BEHAVE-AD rates paranoia, hallucinations, activity disturbance, aggression, diurnal rhythm disturbances, affective disturbances, and anxiety and phobias. CMAI focuses on agitated behaviours and categorises it into physical, verbal, and aggressive types. The NPI is a very widely used tool, considered to be the ‘golden standard’ for tracking psychiatric changes in dementia patients. It is designed as a caregiver-based assessment that covers delusions, hallucinations, agitation/aggression, apathy, and sleep/night-time disturbances (Tariot et al., Reference Tariot, Mack, Patterson, Edland, Weiner, Fillenbaum, Blazina, Teri, Rubin and Mortimer1995; DOMS: Behaviour Measures & Tools, n.d.).
Approved drugs
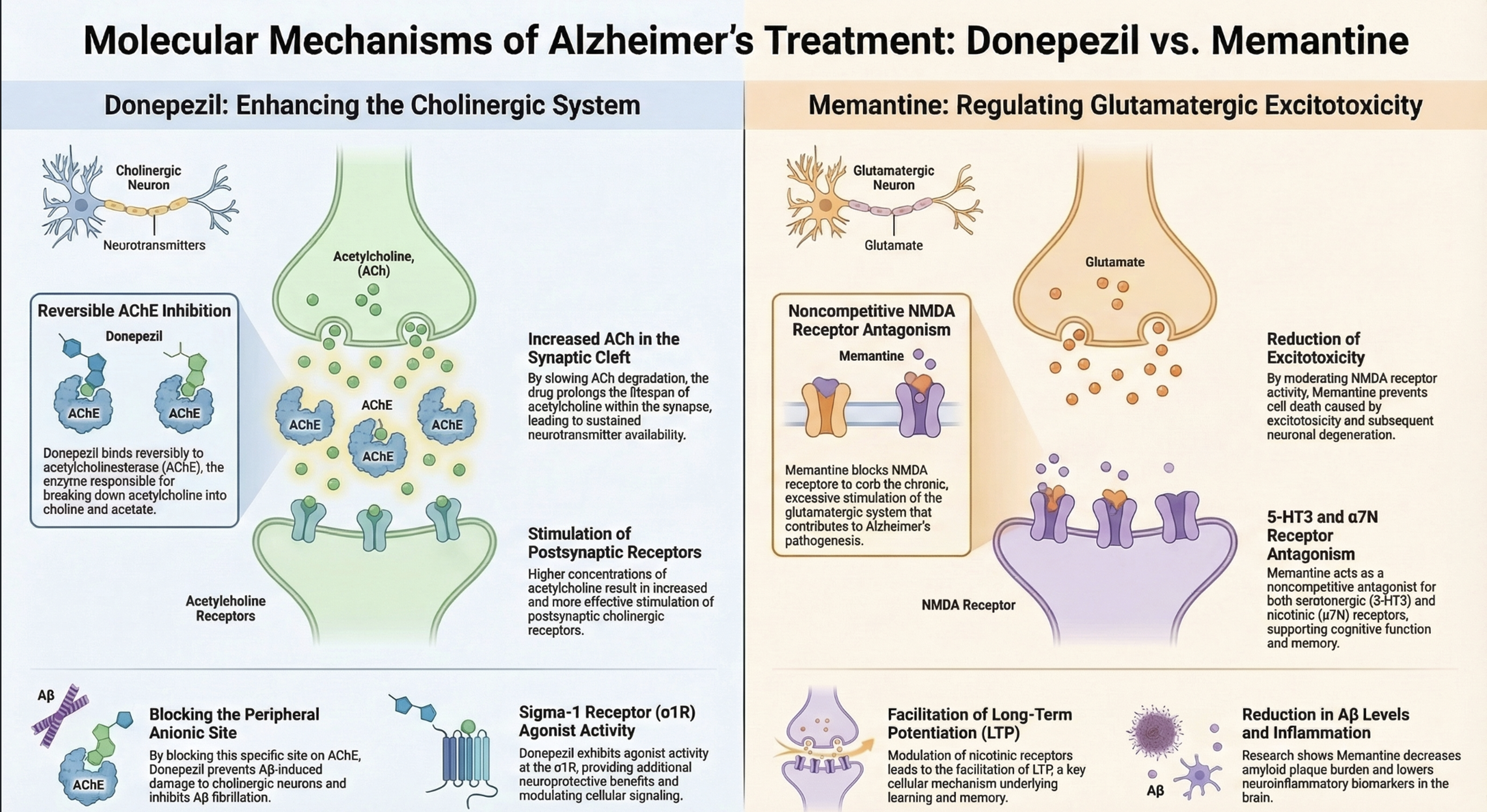
Currently in Europe there are six drugs legislated for use in the treatment of dementia. These are three cholinesterase inhibitors (donepezil, galantamine, rivastigmine), an NMDA antagonist (memantine), and two new anti-amyloid therapeutics used for an early stage, mild disorders (lecanemab, donanemab). In clinical trials, donepezil and memantine are the most commonly used positive controls (Dekker et al., Reference Dekker, Bouvy, O’Rourke, Thompson, Makady, Jonsson and Gispen-de Wied2019; Public Health - European Commission, n.d.). Donepezil is a reversible inhibitor of acetylcholinesterase (AChE), an enzyme that normally terminates nerve impulses by hydrolysing acetylcholine (ACh) to choline and acetate. By inhibiting AChE, donepezil prolongs the lifespan of acetylcholine in the synaptic cleft, resulting in increased stimulation of postsynaptic cholinergic receptors. It modifies the pathology of AD by increasing acetylcholine levels in the brain while simultaneously reducing AChE activity. Additionally, donepezil blocks the peripheral anionic site of AChE, preventing Aβ-induced damage to cholinergic neurons and inhibiting the nonclassical activity of AChE, which involves Aβ fibrillation. It also exhibits agonist activity at the sigma-1 receptor (σ1R) (Zhang & Gordon, Reference Zhang and Gordon2018; Brewster et al., Reference Brewster, Dell’Acqua, Thach and Sessler2019).
The action mechanism of memantine is primarily based on antagonism of the NMDA (N-methyl-D-aspartate) receptor, as excessive stimulation of the glutamatergic system (with chronic NMDA receptor activity) is thought to contribute to the pathogenesis of Alzheimer’s disease (AD) by inducing excitotoxicity and subsequent neuronal degeneration. Memantine acts as a noncompetitive NMDA receptor antagonist, allowing it to reduce chronic NMDA receptor activity, which leads to cell death. Furthermore, memantine also affects other ion channel receptors belonging to the serotonergic and cholinergic systems, which has a supportive effect on memory and learning. In the serotonin system, it is a noncompetitive 5-HT3 receptor antagonist, which facilitates learning and cognitive functions and may also have antiemetic effects. In the cholinergic system, it is a noncompetitive antagonist of the α7N (nicotinic) receptor, and its action leads to facilitation of LTP (long-term potentiation) and upregulation of nicotinic receptors. In animal models, memantine treatment also resulted in a reduction in Aβ levels and amyloid plaque burden in the brain, as well as a decrease in neuroinflammatory biomarkers (Kishi et al., Reference Kishi, Matsunaga, Oya, Nomura, Ikuta and Iwata2017; Balázs et al., Reference Balázs, Bereczki and Kovács2021). The mechanisms of action of donepezil and memantine are depicted in Figure 1.
Mechanism of action of donepezil and memantine.

Figure 1. Long description
The diagram compares the molecular mechanisms of Alzheimer’s treatments Donepezil and Memantine. On the left, Donepezil enhances the cholinergic system through reversible AChE inhibition, increasing acetylcholine in the synaptic cleft, stimulating postsynaptic receptors, blocking the peripheral anionic site, exhibiting sigma-1 receptor agonist activity, and reducing amyloid beta levels and inflammation. On the right, Memantine regulates glutamatergic excitotoxicity through noncompetitive NMDA receptor antagonism, reducing excitotoxicity, exhibiting 5-HT3 and alpha7 nicotinic receptor antagonism, facilitating long-term potentiation, and reducing amyloid beta levels and inflammation.
Although donepezil and memantine are the first-line drugs for dementia, they are known for many adverse effects. The most common for memantine are agitation, insomnia, confusion, depression, headache, hypertension, dizziness, fall, accidental injury, urinary incontinence, diarrhoea and influenza-like symptoms (McShane et al., Reference McShane, Westby, Roberts, Minakaran, Schneider, Farrimond, Maayan, Ware and Debarros2019). Adverse effects of donepezil include diarrhoea, nausea, vomiting, dizziness, and anorexia (Chen et al., Reference Chen, Lai and Tao2024). Additionally, in the human studies the efficacy of donepezil was comparable to herbal interventions (Mazza et al., Reference Mazza, Capuano, Bria and Mazza2006; Akhondzadeh et al., Reference Akhondzadeh, Sabet, Harirchian, Togha, Cheraghmakani, Razeghi, Hejazi, Yousefi, Alimardani, Jamshidi, Zare and Moradi2010; Sadhu et al., Reference Sadhu, Upadhyay, Agrawal, Ilango, Karmakar, Singh and Dubey2014; Zhang et al., Reference Zhang, Lin, Zhang, Cui, Gu, Guo, Wu, Li and Song2015; Lin et al., Reference Lin, Huang, Huang and Zheng2020; Wang et al., Reference Wang, Liu, Zhang, Yang, Wang, Wei, Liu, Pei and Li2020).
There are unmet clinical needs to find more effective, better tolerated or complementary therapeutic options, especially in cases of mild to moderate disease severity. This need is driven by many aspects that require improvement in dementia treatment regimens. These include the numerous side effects of currently used medications, the need to improve the tolerability and safety of drugs, and the limited effectiveness of conventional treatments.
Interestingly, in addition to the pharmacotherapy described above, research is increasingly using plant-derived therapeutics. Herbal preparations are administered in many forms, such as infusions, drops, extracts, or encapsulated powders. In studies different preparations of varying concentrations, obtained using different methods are used. Currently, there are no registered herbal medicines on the pharmaceutical market indicated for the treatment of dementia.
The primary goal of this publication is to comprehensively analyse the results of clinical trials and other human studies regarding the efficacy and safety of natural remedies and complex herbal formulas used in patients with dementia. This review aimed to systematically evaluate the effectiveness and safety of herbal interventions and to compare their clinical effects with standard pharmacological treatments and placebo, including the consistency of outcomes across different types of dementia and the areas of greatest clinical benefit.
Materials and methods
Search strategy
Databases Medline (PubMed), Web of Science, Cochrane Library, and Embase were screened for English-language publications concerning phytopharmaceutical interventions in patients suffering from different types of dementia until September 18th, 2025. We used the search terms ‘therapeutic AND plants AND alzheimer’, ‘therapeutic AND plants AND dementia’. Additionally, the search criteria were expanded to include the following terms: ‘herbal and Alzheimer’, ‘phytotherapy and Alzheimer’, ‘botanical and Alzheimer’, ‘medicinal plants and Alzheimer’, and ‘traditional medicine and Alzheimer’. It resulted in a total of 3 255 publications. Databases were screened by two independent researchers.
The exclusion criteria were non-research articles (reviews), in-vitro studies, animal studies, computational studies, study protocols, case reports, administration other than oral, studies on healthy subjects, intervention including phytotherapeutic and other treatments (standard drugs, cognitive training, physical activity), study populations with major comorbidities.
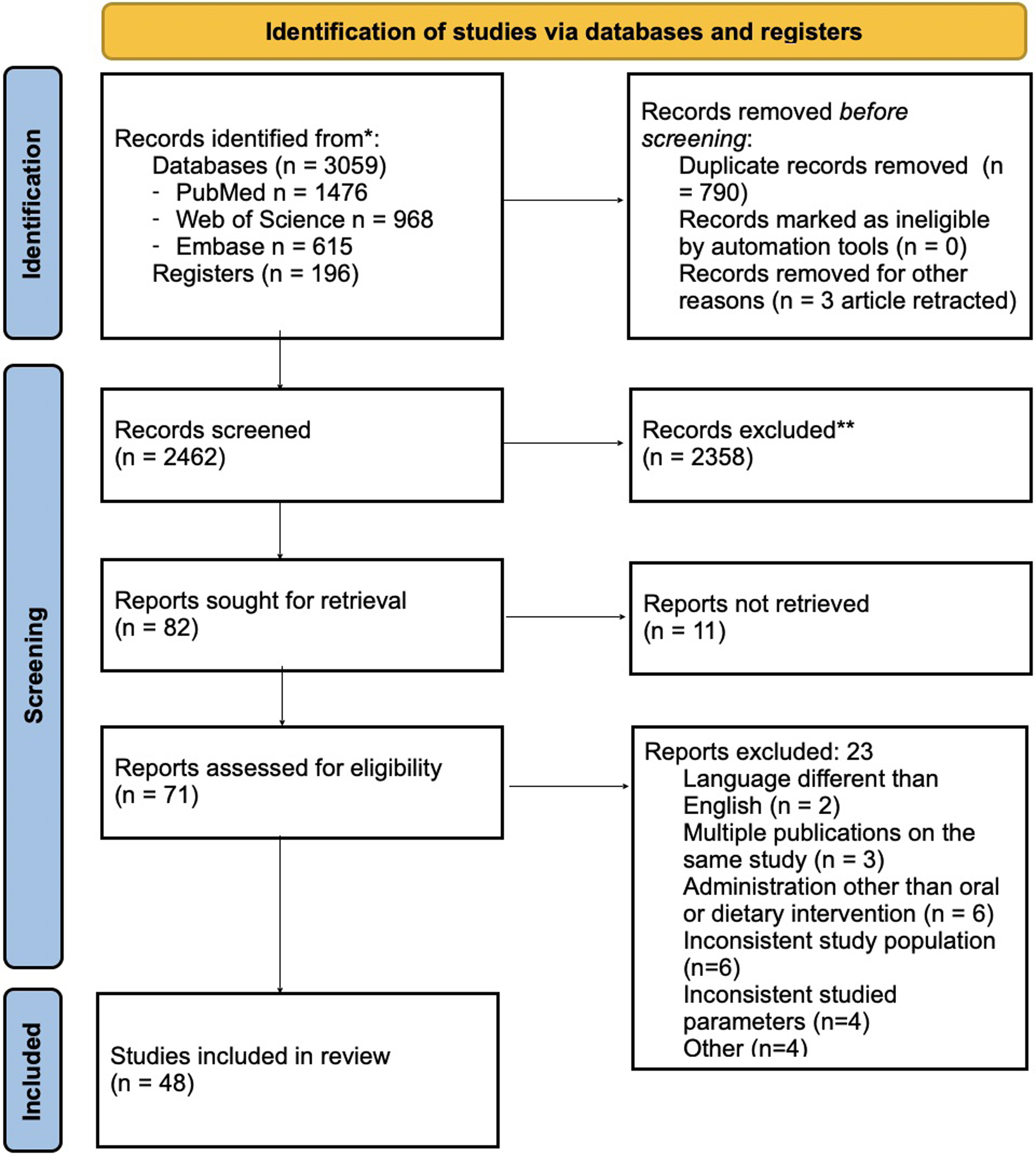
We included studies on different types of dementia – Alzheimer’s disease, vascular dementia, mild cognitive impairment, and others. We included studies on the intervention with one active substance as well as a mixture or multi-component preparations, intervention with standardised substances (for ex. Ginkgo biloba extract EGb 761) or non-standardised (for ex. TCM preparations). Randomised controlled trials (RCTs), double-blind, placebo-controlled studies, and, where necessary, other clinical trials (e.g. open-label, uncontrolled) were included. The search scheme is presented in Figure 2.
Search scheme.

Figure 2. Long description
Flowchart illustrating the stages of identifying studies via databases and registers. The process begins with records identified from databases such as PubMed, Web of Science, Embase, and registers, totaling 3059 records. Duplicate records, amounting to 790, are removed before screening. No records are marked as ineligible by automation tools, and three records are removed for other reasons. The remaining 2462 records are screened, with 2358 records excluded. Reports sought for retrieval total 82, with 11 reports not retrieved. Reports assessed for eligibility number 71, with exclusions due to language, multiple publications, administration methods, inconsistent study population, inconsistent studied parameters, and other reasons. Finally, 48 studies are included in the review.
The sought data consisted of the type of study, aim, used cognitive tests or scales, results, characteristics of the study group (dementia type, number of patients, sex and age of participants), study duration. In case of missing data on the age range we used mean (SD) given in the publication.
For the risk of bias assessment, two researchers worked independently. We analysed each of the research projects, the presence of a control group/control measurements, the use of validated tests.
Systematic review protocol
This review was conducted to assess the efficacy of phytotherapeutic interventions in the treatment of different types of dementia. The methodology is based on the PRISMA guidelines and PICO criteria (Leonardo, Reference Leonardo2018; Page et al., Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann, Mulrow, Shamseer, Tetzlaff, Akl, Brennan, Chou, Glanville, Grimshaw, Hróbjartsson, Lalu, Li, Loder, Mayo-Wilson, McDonald, McGuinness, Stewart, Thomas, Tricco, Welch, Whiting and Moher2021; Nowak & Walkowiak, Reference Nowak and Walkowiak2023).
Qualification criteria (PICO)
Publications meeting the following criteria were included in this study:
Population (P)
Studies had to include adult patients diagnosed with cognitive impairment, including:
-
1. Alzheimer’s disease (AD): Mild, moderate, or severe.
-
2. Vascular dementia (VaD) or mixed dementia.
-
3. Mild cognitive impairment (MCI), including vascular MCI and MCI associated with AD.
-
4. Other dementias (e.g. Lewy body dementia (DLB), Parkinson’s disease dementia (PDD), frontotemporal dementia (FTD)) for which intervention data are available.
Intervention (I) and comparison (C)
Studies were included that assessed:
-
1. Phytopharmaceuticals and TCM: Herbal extracts (e.g. Crocus sativus, Ginkgo biloba (EGb 761), Bacopa monnieri, Cistanche tubulosa) or complex formulas (e.g. Jiannao Yizhi Formula, Tiaobu Xinshen Recipe, Yokukansan, Choto-san, Pushen capsule).
-
2. Comparison (C): Studies had to include a control group (placebo) or an active comparator (e.g. donepezil, memantine, Ginkgo biloba*). In the absence of a control group, studies had to include paired measurements – before and after the intervention.
* Ginkgo biloba was used as a control intervention in some studies, as it is currently the best-researched phytotherapeutic, with relatively predictable and stable outcomes.
Outcomes (O)
Key outcome measures for extraction and analysis included:
-
1. Cognitive function: Changes on the ADAS-cog, MMSE, SKT, and MoCA scales.
-
2. Functioning of daily living (ADL): Changes on the ADCS-ADL, GBS-ADL, and FAQ scales.
-
3. Behavioural and psychological symptoms of dementia (BPSD): Changes on the Neuropsychiatric Inventory (NPI) and NPI-Q scales.
-
4. Safety and tolerability: Incidence of adverse events.
Statistical analysis
Comparative analysis of the studies was conducted based on p-value and effect size (Cohen’s d). Effect sizes were calculated based on the numerical values provided in the publication. In the absence of SD change values that were necessary to assess Cohen’s d a sensitivity analysis was performed to determine this value, using three r values; r = 0.2, r = 0.5, r = 0.8. The MMSE and ADAS-cog tests were selected for comparative analysis as the most universal parameter and the ones present in most of the included publications. Calculations were conducted in Numbers (Apple Inc., version 14.4) and Jamovi (version 2.7.13). The eligibility of the studies for the synthesis was assessed by tabulating the interventions and comparing them against the characteristics of the remaining studies. The data we pulled were: phytotherapeutic used as an intervention, dose administered, control type (standard drug/placebo) if applicable, dementia type, used test, number of participants in both groups, p-value of the result, mean and standard deviation of the result.
The certainty of the evidence was not formally assessed due to the heterogeneity of study designs and results. However, key factors such as methodological quality and consistency of findings were considered in the narrative synthesis.
Risk of bias
Risk of bias assessment was performed independently for each included study. Particular attention was paid to elements such as blinded study design, randomisation, and the presence and nature of the control group (placebo-controlled or nonplacebo-controlled).
Statistical synthesis and analysis (methods for calculating effect size)
For all paired comparisons (Intervention vs. Control/Placebo or baseline and endpoint in case of no control group) for which sufficient numerical data (mean, standard deviation, and count) were available, the standardised mean difference (SMD), or Cohen’s effect size (d), was calculated.
The formula for pooled standard deviation (SDpooled) was used in this calculation to obtain the standardised denominator for the mean difference:
 $d = {M_A - M_C \over SD_{{\rm pooled}}}$
$d = {M_A - M_C \over SD_{{\rm pooled}}}$
where:
 $SD_{{\rm pooled}} = \sqrt{{(n_A - 1)SD_A^2 + (n_C - 1)SD \over n_A + n_C - 2}}$
$SD_{{\rm pooled}} = \sqrt{{(n_A - 1)SD_A^2 + (n_C - 1)SD \over n_A + n_C - 2}}$
A – active group, C – control group
Cohen’s d values were interpreted according to conventional thresholds (e.g. d = 0.20 small, d = 0.50 medium, d = 0.80 large). If SD change was needed to be calculated, we used r = 0.2, r = 0.5, and r = 0.8 to show the sensitivity of obtained results. Additionally, we calculated Cochran’s Q and I 2 for partial heterogeneity analysis.
Heterogeneity analysis and descriptive synthesis
Due to the heterogeneity of the available data, the results that did not qualify for statistical calculations were subjected to descriptive and thematic synthesis.
Results
We enrolled a total of 48 studies for this systematic review (Tables 1 and 2), of which 27 were included into the statistical analysis of effect size (Table 3). The remaining studies were excluded from statistical analysis due to the use of different diagnostic tests (other than ADAS-cog or MMSE). The statistics also did not include studies with missing necessary numerical data. For plants included in more than one study, we performed heterogeneity analysis (Table 4).
Descriptive synthesis of single herb interventions

Table 1. Long description
The table presents a descriptive synthesis of single herb interventions across various studies. It includes columns for the herb name, study details such as the number of participants and duration, and the results of the interventions. The table has multiple rows, each representing a different herb and its associated study data. Notable trends include the variety of herbs studied and the different outcomes measured in each study. The data type includes numerical values and descriptive text, providing a comprehensive overview of the interventions’ effectiveness.
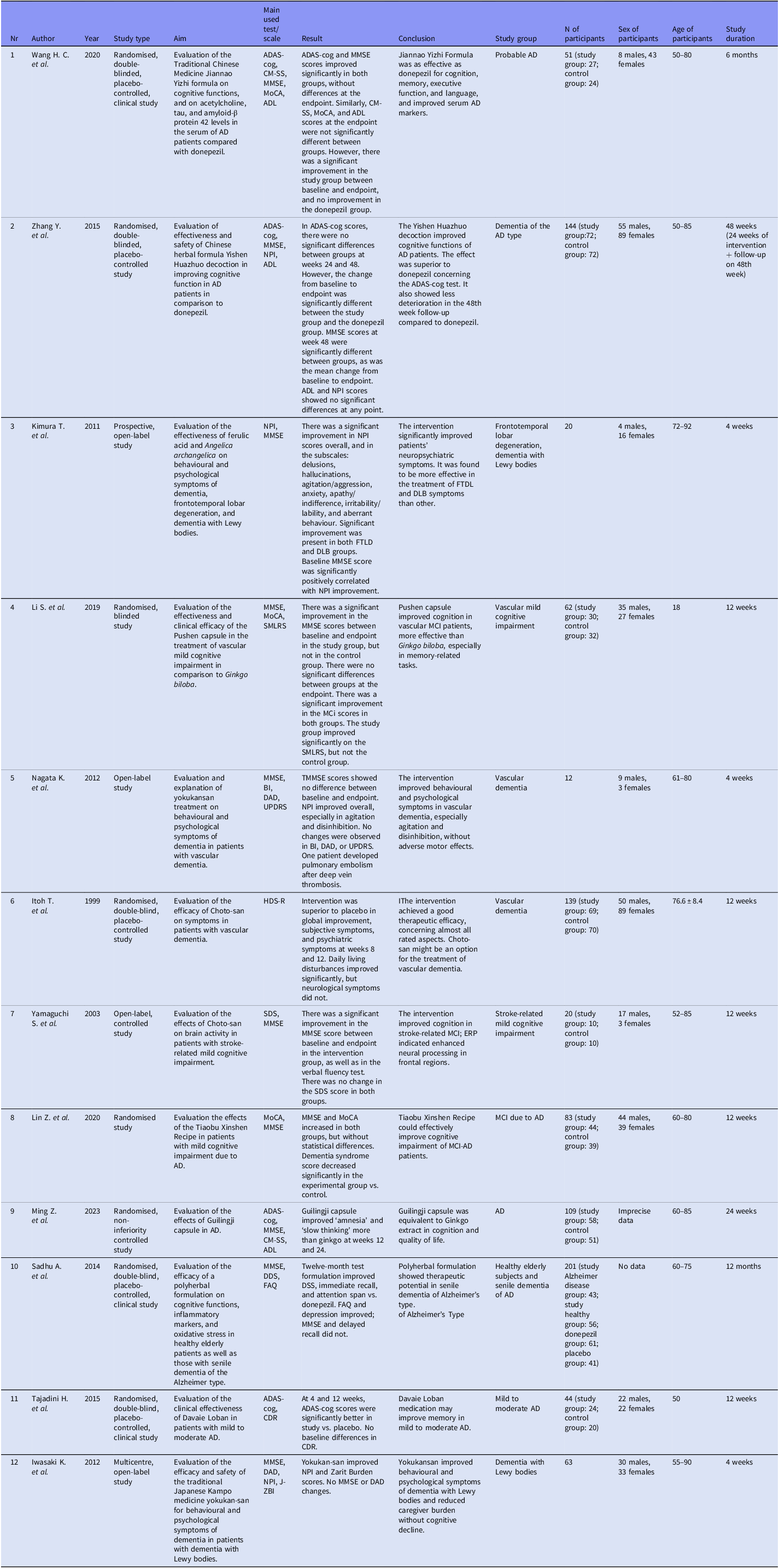
Descriptive synthesis of polyherbal interventions

Table 2. Long description
The table presents a detailed synthesis of 48 studies on polyherbal interventions for cognitive functions, with 27 studies included in the statistical analysis of effect size. The table includes columns for author, year, study type, aim, main outcome measure, result, conclusion, study group, number of participants, sex of participants, age of participants, and study duration. Each row provides specific details for each study, such as the author’s name, the year of publication, the type of study conducted, the aim of the study, the main outcome measure used, the results obtained, the conclusions drawn, the study group, the number of participants, the sex of the participants, the age of the participants, and the duration of the study.
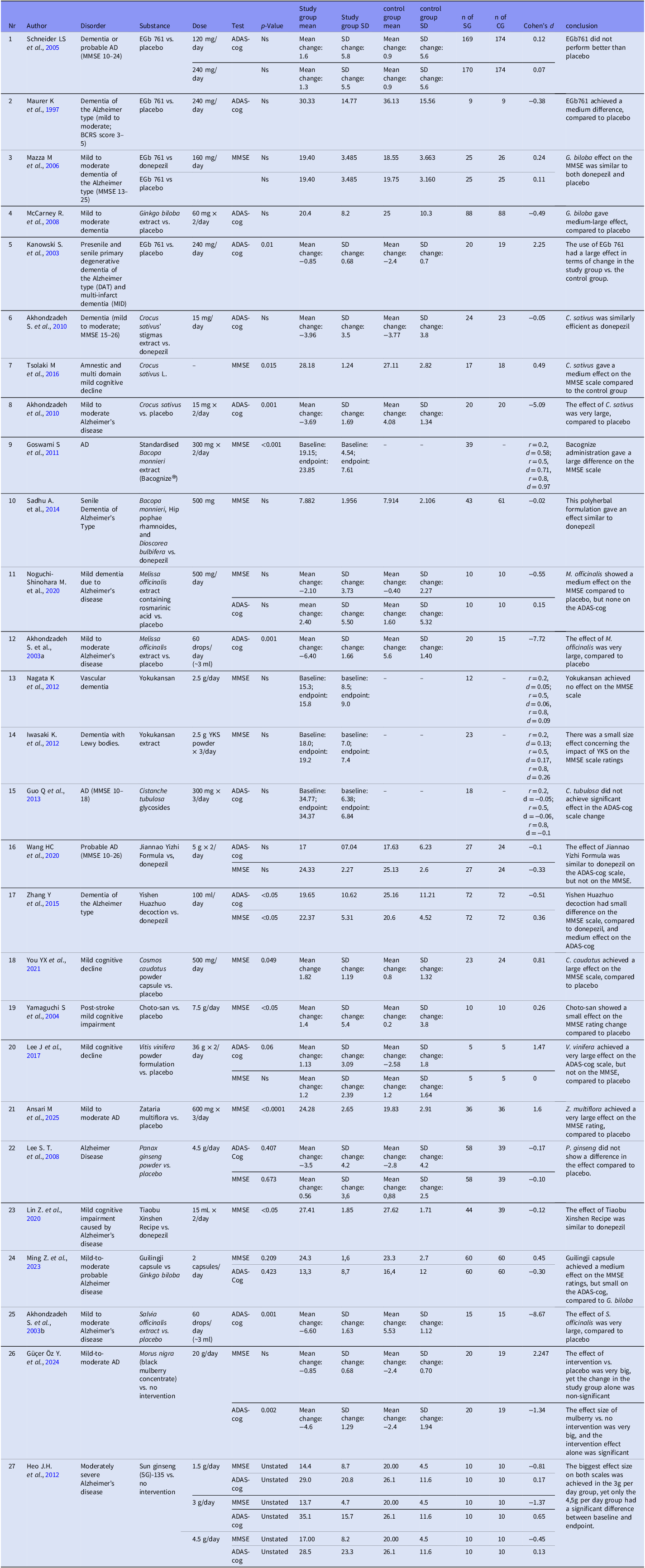
Effect size comparison

Table 3. Long description
The table presents a systematic review of 48 studies, with 27 included in the statistical analysis of effect size. The studies focus on dementia and mild cognitive impairment, using diagnostic tests such as ADAS-cog and MMSE. The table includes columns for the author, year, condition, intervention, comparator, outcome, study design, mean change, standard deviation change, and effect size. Notable trends include the use of different diagnostic tests and the exclusion of studies with missing numerical data. Heterogeneity analysis was performed for plants included in more than one study.
Partial heterogeneity analysis

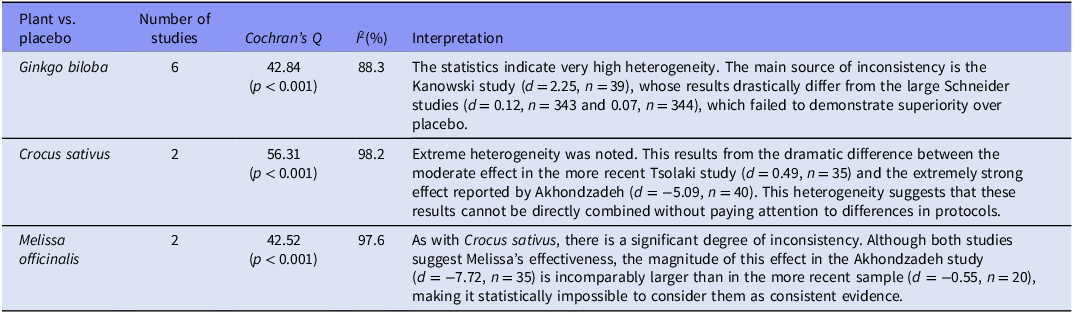
Table 4. Long description
The table presents a heterogeneity analysis of different plants versus placebo, focusing on the number of studies, Cochran’s Q, I squared percentage, and interpretation. It includes data for Ginkgo biloba, Crocus sativus, and Melissa officinalis. Each row lists the plant name, number of studies, Cochran’s Q value with p-value, I squared percentage, and an interpretation of the results. The table highlights the sources of inconsistency and the dramatic differences between studies for each plant.
The most examined herbal therapeutic used in dementia and other neuropsychiatric disorders is Ginkgo biloba, especially the EGb 761® agent. EGb 761 is a standardised dry extract derived from Ginkgo biloba leaves, containing 22.0–27.0% ginkgo flavonoids and 5.0–7.0% terpene lactones. The latter comprise 2.8–3.4% ginkgolides A, B, and C, and 2.6–3.2% bilobalide. The extract contains less than 5 ppm of ginkgolic acids (Kandiah et al., Reference Kandiah, Ong, Yuda, Ng, Mamun, Merchant, Chen, Dominguez, Marasigan, Ampil, Nguyen, Yusoff, Chan, Yong, Krairit, Suthisisang, Senanarong, Ji, Thukral and Ihl2019). The effects of GBE are pleiotropic and have been confirmed in numerous in vitro and in vivo models. GBE has the ability to modify cerebral blood flow, strengthen capillary walls, and prevent blood clot formation (Smith et al., Reference Smith, Maclennan and Darlington1996; Diamond et al., Reference Diamond, Shiflett, Feiwel, Matheis, Noskin, Richards and Schoenberger2000; Maclennan et al., Reference Maclennan, Darlington and Smith2002; Ahlemeyer & Krieglstein, Reference Ahlemeyer and Krieglstein2003). G. biloba extract protects cultured neurons from death induced by hypoxia, glutamate, cyanide, and amyloid-β. It has been shown to improve energy metabolism, stabilise mitochondrial membrane potential, and regulate pro-and antiapoptotic proteins, thereby reducing cell death following oxidative stress (Ponto & Schultz, Reference Ponto and Schultz2003; Smith & Luo, Reference Smith and Luo2004; Shi et al., Reference Shi, Zhao, Zhu, Li, Yew, Yao and Xu2009). Oxidative stress imbalance is a hallmark of AD pathogenesis. G. biloba extract acts as a free radical scavenger, mitigating reactive oxygen species (ROS) levels. Additionally, it can increase the activity of endogenous antioxidant enzymes such as superoxide dismutase (SOD) and catalase, and enhance glutathione (GSH) synthesis. The flavonoid fraction is primarily responsible for antioxidant activity (Colak et al., Reference Colak, Sahin, Alataş, Inal, Yaşar and Kiper1998; Wei et al., Reference Wei, Ni, Hou, Chen, Zhao and Xin2000; Bridi et al., Reference Bridi, Crossetti, Steffen and Henriques2001). G. biloba extract may protectprotects against Aβ-induced neurotoxicity, which has been linked to the inhibition of Aβ production by lowering free cholesterol levels, Aβ oligomerisation, and iron-chelating properties, which may inhibit Aβ fibril formation (Bastianetto et al., Reference Bastianetto, Ramassamy, Doré, Christen, Poirier and Quirion2000; Yao et al., Reference Yao, Han, Drieu and Papadopoulos2004; Ramassamy, Reference Ramassamy2006; Shi et al., Reference Shi, Zhao, Zhu, Li, Yew, Yao and Xu2009).
Most studies have focused on assessing the efficacy of standardised Ginkgo biloba extract (EGb 761) in Alzheimer’s dementia (AD), vascular dementia (VaD), or mixed forms. Multiple randomised controlled trials (RCTs) have shown significant improvements in SKT scores in the EGb 761 group, while a decrease in brain performance was observed in the placebo group (Le Bars et al., Reference Le Bars, Katz, Berman, Itil, Freedman and Schatzberg1997; Kanowski & Hoerr, Reference Kanowski and Hoerr2003; Scripnikov et al., Reference Scripnikov, Khomenko, Napryeyenko and Group2007; Herrschaft et al., Reference Herrschaft, Nacu, Likhachev, Sholomov, Hoerr and Schlaefke2012). The biggest studies (n > 400) reported improvements in the ADAS-cog and SKT scores in 32% of subjects taking EGb 761, compared to 15% in the placebo group (Ihl & Bachinskaya, Reference Ihl, Tribanek and Bachinskaya2010). In the study by Herrschaft et al., patients treated with EGb 761 improved their SKT scores by 2.2 ± 3.5 points, while the change in the placebo group was only 0.3 ± 3.7 points (p < 0.001) (Herrschaft et al. Reference Herrschaft, Nacu, Likhachev, Sholomov, Hoerr and Schlaefke2012). These differences were consistent across subgroups, demonstrating similar efficacy in AD and vascular dementia (Napryeyenko et al., Reference Napryeyenko and Borzenko2007; Napryeyenko et al., Reference Napryeyenko, Sonnik and Tartakovsky2009; Ihl et al., Reference Ihl, Tribanek, Bachinskaya and Group2012). In one study, the percentage of patients with clinically significant improvement in the ADCS-CGIC was 52% in the AD group and 64% in the VaD group (Ihl et al., Reference Ihl, Tribanek, Bachinskaya and Group2012).
Some large RCTs found no significant differences in cognitive decline on the ADAS-cog between the Ginkgo biloba groups and placebo (van Dongen et al., Reference van Dongen, van Rossum, Kessels, Sielhorst and Knipschild2000; Schneider et al., Reference Schneider, DeKosky, Farlow, Tariot, Hoerr and Kieser2005; McCarney et al., Reference McCarney, Fisher, Iliffe, van Haselen, Griffin, van der Meulen and Warner2008). A 2008 study by McCarney et al. found no significant effect of EGb 761 on the ADAS-cog score (McCarney et al., Reference McCarney, Fisher, Iliffe, van Haselen, Griffin, van der Meulen and Warner2008). Furthermore, a 2000 study by van Dongen found that Ginkgo was not effective in treating mild to moderate dementia (van Dongen et al., Reference van Dongen, van Rossum, Kessels, Sielhorst and Knipschild2000).
Treatment with Ginkgo biloba EGb 761 significantly improved neuropsychiatric symptoms and reduced caregiver distress compared to placebo (Scripnikov et al., Reference Scripnikov, Khomenko, Napryeyenko and Group2007; Napryeyenko et al., Reference Napryeyenko, Sonnik and Tartakovsky2009; Ihl & Bachinskaya, Reference Ihl, Tribanek and Bachinskaya2010). A study from 2012 showed that the Neuropsychiatric Inventory (NPI) composite score improved by 4.6 ± 7.1 in the Ginkgo biloba EGb 761 group, compared to 2.1 ± 6.5 in the placebo group (p < 0.001) (Herrschaft et al., Reference Herrschaft, Nacu, Likhachev, Sholomov, Hoerr and Schlaefke2012). Significant improvements were also observed in all secondary outcome measures, including daily living (ADL) and the Clinical Global Assessment (CGI) (Napryeyenko et al., Reference Napryeyenko, Sonnik and Tartakovsky2009; Ihl & Bachinskaya, Reference Ihl, Tribanek and Bachinskaya2010; Herrschaft et al., Reference Herrschaft, Nacu, Likhachev, Sholomov, Hoerr and Schlaefke2012).
Another interesting and well-studied plant species in dementia is Crocus sativus. Its therapeutic effects are attributed to its main bioactive components: crocin, crocetin and safranal (Hatziagapiou et al., Reference Hatziagapiou, Kakouri, Lambrou, Bethanis and Tarantilis2019). Saffron and its components are powerful antioxidants. The main carotenoids in saffron (crocin and crocetin) reduce reactive oxygen species (ROS), thus protecting nerve cells from damage (Avgerinos et al., Reference Avgerinos, Vrysis, Chaitidis, Kolotsiou, Myserlis and Kapogiannis2020; D’Onofrio et al., Reference D’Onofrio, Nabavi, Sancarlo, Greco and Pieretti2021). Some studies suggest that aqueous methanolic extracts of saffron can moderate AChE activity, which increases acetylcholine concentrations in synapses and thereby improves cholinergic transmission and cognitive function. AChE inhibition is primarily attributed to safranal, as well as crocetin and dimethylcrocetin (Avgerinos et al., Reference Avgerinos, Vrysis, Chaitidis, Kolotsiou, Myserlis and Kapogiannis2020). Saffron extracts and crocetin exhibit high affinity for the phencyclidine binding site of the NMDA receptor. This modulation may lead to an antagonistic effect similar to memantine, helping to regulate glutamate levels and prevent excessive excitation of nerve cells, which leads to their death (Berger et al., Reference Berger, Hensel and Nieber2011; Geromichalos et al., Reference Geromichalos, Lamari, Papandreou, Trafalis, Margarity, Papageorgiou and Sinakos2012). crocin and crocetin, exhibit antiaggregatory effects on the Aβ peptide. Crocetin stabilises Aβ oligomers (the most toxic form) and prevents their transformation into neurotoxic fibrils. Crocin may prevent Aβ aggregation by binding to the carotene core, stabilising the central, aggregation-prone hydrophobic cluster, thus preventing the transition from an α-helix to a neurotoxic β-sheet structure (Papandreou et al., Reference Papandreou, Kanakis, Polissiou, Efthimiopoulos, Cordopatis, Margarity and Lamari2006; Ahn et al., Reference Ahn, Hu, Hernandez and Kim2011; Ghahghaei et al., Reference Ghahghaei, Bathaie, Kheirkhah and Bahraminejad2013). Crocin also inhibits the aggregation of human tau protein (by reducing the ratio of β-sheet structure to loose/random structure), which is important in the context of neurofibrillary tangle (NFT) formation, the second pathological hallmark of AD (Zarei Jaliani et al., Reference Zarei Jaliani, Riazi, Ghaffari, Karima and Rahmani2013; Karakani et al., Reference Karakani, Riazi, Mahmood Ghaffari, Ahmadian, Mokhtari, Jalili Firuzi and Zahra Bathaie2015; Hire et al., Reference Hire, Srivastava, Davis, Kumar Konreddy and Panda2017).
Studies comparing saffron with standard treatments and placebo indicate a potential therapeutic effect. Data from short‑term trials suggest that saffron may provide cognitive benefits comparable to those observed with donepezil in patients with mild to moderate Alzheimer’s disease. In a 16‑week double‑blind, placebo‑controlled study, saffron (30 mg/day) showed similar short‑term improvements in ADAS‑cog and CDR‑SB scores to those seen with donepezil (10 mg/day), with no significant differences between groups. However, the study’s short duration and small sample size limit the strength of these findings and do not allow conclusions regarding long‑term efficacy. Saffron extract demonstrated similar efficacy to memantine in reducing cognitive decline in patients with moderate to severe AD, with no statistically significant differences in the SCIRS, FAST, or MMSE scales (Farokhnia et al., Reference Farokhnia, Shafiee Sabet, Iranpour, Gougol, Yekehtaz, Alimardani, Farsad, Kamalipour and Akhondzadeh2014a). In another study, saffron resulted in significantly better cognitive scores compared to placebo (ADAS-cog: p = 0.04; CDR: p = 0.04) after 16 weeks (Akhondzadeh et al., Reference Akhondzadeh, Sabet, Harirchian, Togha, Cheraghmakani, Razeghi, Hejazi, Yousefi, Alimardani, Jamshidi, Zare and Moradi2010). In patients with amnestic MCI, saffron supplementation resulted in significant improvements in MMSE scores (p = 0.015) (Tsolaki et al., Reference Tsolaki, Karathanasi, Lazarou, Dovas, Verykouki, Karacostas, Georgiadis, Tsolaki, Adam, Kompatsiaris and Sinakos2016). Although these findings suggest potential cognitive benefits, the available studies are short in duration and involve relatively small samples, limiting conclusions regarding long‑term efficacy.
The plant that has been a subject of extensive research is Bacopa monnieri. It exhibits potent neuroprotective and antioxidant effects, primarily attributed to bacosites. B. monnieri prevents neuroinflammation and restores redox balance (i.e. the balance of oxidation and reduction) in the brain, mitigating oxidative stress. It does this by modulating inflammatory pathways (e.g. the TNF and IL-6 pathways) and by strengthening the internal defence system, including restoring reduced glutathione (GSH) levels and increasing the activity of antioxidant enzymes (SOD, CAT, GPx) (Preethi et al., Reference Preethi, Singh, Charles and Rajan2012; Liu et al., Reference Liu, Yue, Zhang, Shan, Wang and Zhang2013; Maruthiyodan et al., Reference Maruthiyodan, Munegowda, Thomas, Gangadharan, Joshi, Mumbrekar, Goyal, Mahadevan, Erayur Mana, Thrikovil Sankaran, Marthanda Varma Sankaran and Kanive Parashiva2026). B. monnieri extracts protect neurons from amyloid-beta (Aβ)-induced neurotoxicity and even reduce Aβ levels in AD mouse models (Aguiar & Borowski, Reference Aguiar and Borowski2013). The action of B. monnieri involves activation of choline transferase (ChAT), which leads to increased synthesis of acetylcholine (ACh). Furthermore, it increases dendritic branching (arborisation) in neurons, which is associated with improved learning and neuronal plasticity (Vollala et al., Reference Vollala, Upadhya and Nayak2011; Maruthiyodan et al., Reference Maruthiyodan, Munegowda, Thomas, Gangadharan, Joshi, Mumbrekar, Goyal, Mahadevan, Erayur Mana, Thrikovil Sankaran, Marthanda Varma Sankaran and Kanive Parashiva2026).
Studies included in this review, comparing Bacopa monnieri with donepezil, found no significant difference in the rate of deterioration on the ADAS-cog over 52 weeks (Prabhakar et al., Reference Prabhakar, Vishnu, Modi, Mohanty, Sharma, Medhi, Mittal, Khandelwal, Goyal, Lal, Singla, Kansal and Avasthi2020). The herbal formula containing B. monnieri produced an effect similar to donepezil on the MMSE (Sadhu et al., Reference Sadhu, Upadhyay, Agrawal, Ilango, Karmakar, Singh and Dubey2014). In a study of patients with MCI, B. monnieri showed improvement only in the attention and language subscales (Delfan et al., Reference Delfan, Kordestani-Moghaddam, Gholami, Kazemi and Mohammadi2024). In an uncontrolled study of patients with AD, significant improvements were noted on the MMSE after six months, with the greatest changes in orientation and language abilities (Goswami et al., Reference Goswami, Saoji, Kumar, Thawani, Tiwari and Thawani2011).
Other herbs tested for therapeutic properties against dementia are Panax ginseng, Melissa officinalis, Salvia officinalis, or Cosmos caudatus, among other plants emerging in phytopharmaceutical studies. Melissa officinalis and Salvia officinalis have a beneficial effect on dementia, mainly through their ability to modulate the acetylcholine signalling pathway through an acetylcholine receptor activity. Each of those herbs display binding properties with both nicotinic and muscarinic receptors, while Melissa officinalis also compensates for neurotransmitter deficits through an inhibition of acetylcholine esterase (AChE) (Akhondzadeh et al., Reference Akhondzadeh, Noroozian, Mohammadi, Ohadinia, Jamshidi and Khani2003a, Reference Akhondzadeh, Noroozian, Mohammadi, Ohadinia, Jamshidi and Khani2003b). Ginsenosides of Panax ginseng reduce Aβ40 and Aβ42 levels, regenerate axons and synapses, and minimise the inhibitory effect of Aβ on cholinergic transmission in the hippocampus. They also act as antioxidants, increase synaptic density in the hippocampus, and enhance the proliferation and differentiation of neural progenitor cells (Lee et al., Reference Lee, Chu, Sim, Heo and Kim2008). Other herbs, such as Cosmos caudatus are characterised by a high amount of flavonoids. C. caudatus contains quercetin and quercitrin. These chemical compounds have powerful free radical scavenging properties. They potentially reduce oxidative damage to DNA and lipids and prevent lipid peroxidation (You et al., Reference You, Shahar, Rajab, Haron, Yahya, Mohamad, Din and Maskat2021b).
These herbs also had variable results in dementia patients. Melissa officinalis and Salvia officinalis reduced agitation in Alzheimer’s subjects (Akhondzadeh et al., Reference Akhondzadeh, Noroozian, Mohammadi, Ohadinia, Jamshidi and Khani2003a, Reference Akhondzadeh, Noroozian, Mohammadi, Ohadinia, Jamshidi and Khani2003b). Panax ginseng turned out to be a transient cognitive enhancer, yet there was no difference compared to placebo (Lee et al., Reference Lee, Chu, Sim, Heo and Kim2008). Cosmos caudatus achieved a large effect on MMSE scale (d = 0.81) attributed to high polyphenol concentration (You et al., Reference You, Shahar, Rajab, Haron, Yahya, Mohamad, Din and Maskat2021b). Zataria multiflora gave significant and sustained improvements in cognitive function (MMSE, d = 1.6) and dementia symptoms compared with placebo, which was transient. In this study a large effect on MMSE was observed in mild to moderate AD (Ansari et al., Reference Ansari, Sargazi-Moghadam, Tajadini, Kamali, Kamali, Dehesh, Shojaei and Sharififar2025). On the contrary, Cistanche tubulosa was not effective in the treatment of AD. No significant differences were found between baseline and endpoint in the ADAS-cog and MMSE (Guo et al., Reference Guo, Zhou, Wang, Huang, Lee, Su and Lu2013).
Traditional Chinese Medicine (TCM) preparations are becoming increasingly popular in dementia research. Blends such as Choto-san, Yokukansan, Jiannao Yizhi Formula, Yishen Huazhuo decoction, Pushen capsule, Tiaobu Xinshen Recipe, or Guilingji capsule are complex herbal mixtures developed based on the principles of energy balance and harmonisation of organ function. In the context of treating dementia, including Alzheimer’s disease, they demonstrate multifaceted biological effects.
Experimental and clinical studies have shown that these preparations may exhibit neuroprotective, anti-inflammatory, antioxidant, and modulatory effects on the cholinergic and glutamatergic systems, as well as inhibiting β-amyloid aggregation and tau protein phosphorylation. Some of them also improve cerebral blood flow and metabolism, which may translate into beneficial effects on cognitive function (Itoh et al., Reference Itoh, Shimada and Terasawa1999; Iwasaki et al., Reference Iwasaki, Kosaka, Mori, Okitsu, Furukawa, Manabe, Yoshita, Kanamori, Ito, Wada, Kitayama, Horiguchi, Yamaguchi, Takayama, Fukuhara, Ouma, Nakano, Hashimoto and Kinoshita2012; Zhang et al., Reference Zhang, Lin, Zhang, Cui, Gu, Guo, Wu, Li and Song2015; Li et al., Reference Li, Cao, Deng, Zhu and Yan2019; Lin et al., Reference Lin, Huang, Huang and Zheng2020; Wang et al., Reference Wang, Liu, Zhang, Yang, Wang, Wei, Liu, Pei and Li2020; Ming et al., Reference Ming, Yimiao, Huichan, Yu, Lina, Hui and Hao2023). Despite promising preliminary research results, clinical evidence regarding the efficacy and safety of these preparations remains limited, with most data coming from studies with small sample sizes and varying methodological quality. Therefore, TCM preparations are currently viewed as potential adjunctive therapies requiring further validation in well-designed, randomised clinical trials.
Yishen Huazhuo decoction showed greater improvements than donepezil on the ADAS‑cog and MMSE scales. The MMSE score also improved more markedly in the herbal treatment group. However, these studies did not include a placebo control group and were limited to short‑term observation periods (24 weeks), which restricts the ability to draw firm conclusions about the true magnitude of the effect and its long‑term clinical relevance. (Zhang et al., Reference Zhang, Lin, Zhang, Cui, Gu, Guo, Wu, Li and Song2015). The intervention with Choto-san was significantly superior to placebo in terms of global improvement, subjective symptoms, and impairment in daily functioning in vascular dementia (Itoh et al., Reference Itoh, Shimada and Terasawa1999). In the post-stroke MCI the effect was primarily on symptoms and functioning, with a small effect on change in the MMSE (d = 0.26) (Yamaguchi et al., Reference Yamaguchi, Matsubara and Kobayashi2004).
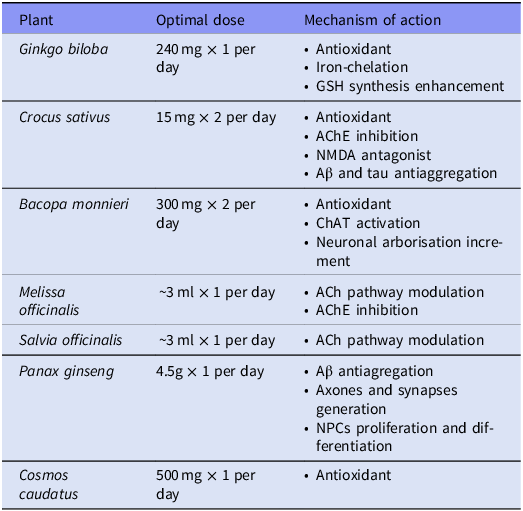
The optimal doses of selected plant extracts used in interventions according to the source studies are presented in Table 5. Additionally, we included the mechanism of action of each of them.
Optimal doses of selected plant extracts and their mechanism of action

Table 5. Long description
The table presents the optimal doses of various plant extracts used in interventions and their mechanisms of action. It includes seven rows and three columns. The columns are labeled Plant, Optimal dose, and Mechanism of action. The plants listed are Ginkgo biloba, Crocus sativus, Bacopa monnieri, Melissa officinalis, Salvia officinalis, Panax ginseng, and Cosmos caudatus. The optimal doses range from 15 milligrams twice per day to 4.5 grams once per day. The mechanisms of action include antioxidant properties, iron chelation, GSH synthesis enhancement, AChE inhibition, NMDA antagonism, Aβ and tau antiaggregation, ChAT activation, neuronal arborisation increment, ACh pathway modulation, Aβ antiaggregation, axons and synapses generation, NPCs proliferation and differentiation.
Discussion and conclusions
The main purpose of this study was to assess the effects of phytopharmaceutics on cognition and neuropsychiatric symptoms in dementia patients. Most of the studied plants, herbs and formulas had a great positive clinical impact on treating mild to moderate dementia, especially Ginkgo biloba, Crocus sativus, and Salvia officinalis, which supports the hypothesis of their therapeutic value (Akhondzadeh et al., Reference Akhondzadeh, Noroozian, Mohammadi, Ohadinia, Jamshidi and Khani2003b, Reference Akhondzadeh, Sabet, Harirchian, Togha, Cheraghmakani, Razeghi, Hejazi, Yousefi, Alimardani, Jamshidi, Zare and Moradi2010; Ihl & Bachinskaya, Reference Ihl, Tribanek and Bachinskaya2010; Ihl et al., Reference Ihl, Tribanek, Bachinskaya and Group2012; Tsolaki et al. Reference Tsolaki, Karathanasi, Lazarou, Dovas, Verykouki, Karacostas, Georgiadis, Tsolaki, Adam, Kompatsiaris and Sinakos2016).
Although Ginkgo biloba showed results of a large effect size, the outcomes were not consistent throughout all of the studies. Some authors obtained significant improvement of EGb 761 interventions in the field of SKT, ADL, and NPI (Kanowski et al., Reference Kanowski, Herrmann, Stephan, Wierich and Hörr1996; Le Bars et al., Reference Le Bars, Katz, Berman, Itil, Freedman and Schatzberg1997; Kanowski & Hoerr, Reference Kanowski and Hoerr2003; Mazza et al., Reference Mazza, Capuano, Bria and Mazza2006; Scripnikov et al., Reference Scripnikov, Khomenko, Napryeyenko and Group2007; Napryeyenko et al., Reference Napryeyenko, Sonnik and Tartakovsky2009; Ihl & Bachinskaya, Reference Ihl, Tribanek and Bachinskaya2010; Ihl et al., Reference Ihl, Tribanek, Bachinskaya and Group2012; Herrschaft et al., Reference Herrschaft, Nacu, Likhachev, Sholomov, Hoerr and Schlaefke2012; Chowdhury et al., Reference Chowdhury, Roy, Reddy, Gupta, Nigam and Hoerr2024), whereas some did not achieve any difference between Ginkgo biloba and placebo (Por & Evans, Reference Por and Evans1998; van Dongen et al., Reference van Dongen, van Rossum, Kessels, Sielhorst and Knipschild2000; Schneider et al., Reference Schneider, DeKosky, Farlow, Tariot, Hoerr and Kieser2005; McCarney et al., Reference McCarney, Fisher, Iliffe, van Haselen, Griffin, van der Meulen and Warner2008). These inconsistencies might be influenced by an abnormal deterioration rate in the placebo group, like in the case of studies by Schneider et al. (Schneider et al., Reference Schneider, DeKosky, Farlow, Tariot, Hoerr and Kieser2005). The other reason might be the differences in test sensitivity. In most cases, the effects measured by the SKT score were significantly better, whereas the same intervention did not show any differences on other scales. This happened in the study by Le Bars et al. on Ginkgo biloba efficacy, a significant improvement on the SKT scale was noted, yet the measurements on ADAS were negligible (Le Bars et al., Reference Le Bars, Katz, Berman, Itil, Freedman and Schatzberg1997). Similar outcomes were revealed by Mazza et al. where the SKT improved significantly, while MMSE did not show any changes (Mazza et al., Reference Mazza, Capuano, Bria and Mazza2006). The differences in the results suggest that the SKT scale may have been more sensitive to changes compared to the ADAS-Cog or MMSE scales in the studied populations, which creates a bias in the interpretation of the results. However, there was a consistent effectiveness of EGb761 on the neuropsychiatric symptoms. NPI scores improved in the studies of Ihl et al., Herrschaft et al. and Scripnikov et al. (Scripnikov et al., Reference Scripnikov, Khomenko, Napryeyenko and Group2007; Ihl and Bachinskaya, Reference Ihl, Tribanek and Bachinskaya2010; Herrschaft et al., Reference Herrschaft, Nacu, Likhachev, Sholomov, Hoerr and Schlaefke2012).
Crocus sativus extract has been repeatedly demonstrated to be comparable to conventional medications. Studies have shown that saffron (at a dose of 30 mg/day) was as effective as donepezil (10 mg/day) in the treatment of mild to moderate AD. In these clinical trials, no statistically significant differences were observed in ADAS-cog and CDR-SB scores between the saffron and donepezil groups (Akhondzadeh et al., Reference Akhondzadeh, Sabet, Harirchian, Togha, Cheraghmakani, Razeghi, Hejazi, Yousefi, Alimardani, Jamshidi, Zare and Moradi2010). Despite indications of potential cognitive benefits, the currently available studies are short-term and include relatively small samples, which limits the ability to draw conclusions about long-term efficacy. Furthermore, saffron demonstrated similar efficacy to memantine in reducing cognitive decline in patients with moderate to severe AD, with no statistically significant differences on the SCIRS, FAST, and MMSE scales (Farokhnia et al., Reference Farokhnia, Shafiee Sabet, Iranpour, Gougol, Yekehtaz, Alimardani, Farsad, Kamalipour and Akhondzadeh2014a).
Similar results were observed for complex TCM formulas. The Jiannao Yizhi formula proved equally effective as donepezil in terms of cognitive function, memory, executive function, and language skills. In this case, scores on the ADAS-cog and MMSE significantly improved in both groups, but the differences at the end of the study were not significant (Guo et al., Reference Guo, Zhou, Wang, Huang, Lee, Su and Lu2013). Similar efficacy in slowing cognitive decline, comparable to donepezil, was also observed in a study evaluating a complex preparation containing, among others, Bacopa monnieri extract (Sadhu et al., Reference Sadhu, Upadhyay, Agrawal, Ilango, Karmakar, Singh and Dubey2014).
The Yishen Huazhuo decoction demonstrated superiority over donepezil in improving ADAS-cog scores. The change in ADAS-cog scores between baseline and post-baseline was significantly different in favour of the herbal formula, and achieved a medium effect size (d=−0.51) (Zhang et al., Reference Zhang, Lin, Zhang, Cui, Gu, Guo, Wu, Li and Song2015). A comparative study suggested that Pushen capsule – a formula consisting mainly of Polygonum multiflorum, Pollen Typhae, Salvia miltiorrhiza, Ligusticum chuanxiong, and paeoniflorin – may have superior beneficial effects over Ginkgo biloba extract in vascular MCI. Pushen capsule improved cognitive function, especially in the field of memory (Li et al., Reference Li, Cao, Deng, Zhu and Yan2019). Wang et al. in a meta-analysis from 2021, showed a promising potential in numerous Chinese herb formulas. One of them was Bushen Jianpi Huatan Pills (formula containing Cistanche deserticola, Rhizoma Alismatis, Polygonum multiflorum thumb), which scored significantly higher compared to placebo in the MMSE scale. It also showed an optimistic effect of the Guipi Decoction (mixture consisting of 14 herbs), combined with donepezil and nimodipine (versus both drugs alone) on the MMSE. The last one, which achieved a significant effect was the Dream sweet oral liquid (17 herbs) with citicoline, compared to the citicoline alone (Wang et al., Reference Wang, Diwu, Liu, Zhou, Sayed, Wang and Gou2021).
In addition to stabilising cognitive function, a key therapeutic goal in dementia treatment is managing behavioural and psychological symptoms of dementia (BPSD), such as apathy, anxiety, agitation, and depression. These symptoms significantly lower patients’ quality of life and increase caregiver distress. Ginkgo biloba extract (EGb 761®) is well documented in this context, demonstrating significant improvements in the NPI score and reducing caregiver stress (Scripnikov et al., Reference Scripnikov, Khomenko, Napryeyenko and Group2007; Ihl et al., Reference Ihl, Tribanek, Bachinskaya and Group2012; Kandiah et al., Reference Kandiah, Ong, Yuda, Ng, Mamun, Merchant, Chen, Dominguez, Marasigan, Ampil, Nguyen, Yusoff, Chan, Yong, Krairit, Suthisisang, Senanarong, Ji, Thukral and Ihl2019). Other phytopharmaceuticals also play a significant role in mood and behaviour modulation. In clinical trials, Melissa officinalis and Salvia officinalis demonstrated a positive effect not only on improving cognitive function (ADAS-cog) but also on reducing agitation (Akhondzadeh et al., Reference Akhondzadeh, Noroozian, Mohammadi, Ohadinia, Jamshidi and Khani2003a, Reference Akhondzadeh, Noroozian, Mohammadi, Ohadinia, Jamshidi and Khani2003b). These findings are consistent with other authors’ reports. Noguchi-Shinohara et al. described Melissa’s properties in the treatment of AD, through anti-Aβ action, cholinergic pathway modulation, and both anti-inflammatory and anti-oxidative characteristics. Participants received the intervention via aromatherapy (Noguchi-Shinohara et al., Reference Noguchi-Shinohara, Ono, Hamaguchi, Nagai, Kobayashi, Komatsu, Samuraki-Yokohama, Iwasa, Yokoyama, Nakamura and Yamada2020). Kennedy et al. used encapsulated dried leaves of Melissa and achieved a great improvement in patient’s calmness and cognition (Kennedy et al., Reference Kennedy, Wake, Savelev, Tildesley, Perry, Wesnes and Scholey2003). Burns et al. also utilised aromatherapy as a form of Melissa’s delivery, and reached similar effects to donepezil concerning, agitation and NPI scores (Burns et al., Reference Burns, Perry, Holmes, Francis, Morris, Howes, Chazot, Lees and Ballard2011). Regarding sage, Lopresti described its wide-range anti-oxidant and anti-inflammatory properties, which were confirmed in numerous in vitro and animal studies (Lopresti, Reference Lopresti2017). Kennedy et al. studied Salvia’s impact on mood in AD patients and found it effective in reducing anxiety, improving calmness, alertness, and task performance (Kennedy et al., Reference Kennedy, Pace, Haskell, Okello, Milne and Scholey2006). Other combination formulations, such as Yokukansan, have shown significant improvement in behavioural and psychological symptoms (BPSD) in dementia with Lewy bodies (DLB), including delusions, hallucinations, and aggression/agitation, without compromising cognitive function (Nagata et al., Reference Nagata, Yokoyama, Yamazaki, Takano, Maeda, Takahashi and Terayama2012). In a study of Cosmos caudatus in elderly individuals with MCI, significant improvements in tension and total mood disturbance were observed (You et al., Reference You, Shahar, Rajab, Haron, Yahya, Mohamad, Din and Maskat2021b).
Although the largest evidence base concerns Ginkgo biloba and Crocus sativus, this review indicates the presence of other, less-researched substances that have demonstrated exceptionally large clinical effect sizes in smaller trials, requiring further clinical research. Zataria multiflora achieved a very large effect size (d = 1.6) on the MMSE scale in patients with mild to moderate AD compared to placebo. The benefits of Zataria on brain health were already proven in animal studies. Arab et al. used a rat model of AD and revealed that it reversed the disorders caused by lipopolysaccharide in the Morris maze and dark chamber tests. It also lowered the oxidative stress through increasing the levels of superoxide dismutase, catalase, and IL-6 (Arab et al., Reference Arab, Hosseini, Marefati, Beheshti, Anaeigoudari, Sadeghnia and Boskabady2022). Eskandari-Roozbahani et al. however, did not reveal any changes in the oxidative levels in rat’s brain tissue. Nevertheless, they reported improvement in the Morris maze test, reduction of AChE and increased levels of Brain-Derived Neurotrophic Factor (BDNF) (Eskandari-Roozbahani et al., Reference Eskandari-Roozbahani, Shomali and Taherianfard2019).
Another plant to achieve a large effect size (d = 0.81) on the MMSE scale in patients with MCI was Cosmos caudatus, which is attributed to its high concentration of polyphenols, such as quercetin and quercitrin. You et al. performed an interesting study on Task-Based Dorsolateral Prefrontal Cortex Activation through an MRI imaging. They administered 500 mg C. caudatus capsules, twice a day for 12 weeks to older adults with MCI. They revealed that this intervention significantly improved the digit span test scores, working memory test scores, and Stroop test score, which implicates a better cognitive control and information processing (You et al., Reference You, Shahar, Mohamad, Rajab, Haron, Che Din and Abdul Hamid2021a).
Many of the beneficial effects of phytopharmaceuticals go beyond the anticholinergic mechanism of action, which is the one modulated by conventional drugs. Oxidative stress is a key factor in the pathogenesis of AD. Studies clearly indicate that antioxidant properties are important. Cosmos caudatus, for example, significantly reduced serum malondialdehyde (MDA) concentrations and increased glutathione (GSH) concentrations (You et al., Reference You, Shahar, Rajab, Haron, Yahya, Mohamad, Din and Maskat2021b). Similarly, Bacopa monnieri prevented oxidative stress by restoring redox balance and increasing the activity of antioxidant enzymes such as SOD, catalase, and glutathione peroxidase (Aguiar & Borowski, Reference Aguiar and Borowski2013). Action against β-amyloid peptide (Aβ) and tau protein aggregation is another key mechanism. In the case of Crocus sativus, crocin and crocetin have been shown to protect against Aβ-induced toxicity. Crocin inhibits tau protein aggregation and the production of Aβ oligomers (Hatziagapiou et al., Reference Hatziagapiou, Kakouri, Lambrou, Bethanis and Tarantilis2019). EGb 761 has been shown to protect neurons against Aβ-induced cell death and inhibit Aβ aggregation (Singh et al., Reference Singh, Srivastav, Castellani, Plascencia-Villa and Perry2019; Lorca et al., Reference Lorca, Mulet, Arévalo-Caro, Sanchez, Perez, Perrino, Bach-Faig, Aguilar-Martínez, Vilella, Gallart-Palau and Serra2023). Some substances act as transient cognitive enhancers. In the case of Panax ginseng, the observed improvement in the ADAS-cog and MMSE scales disappeared after treatment discontinuation, suggesting that its effect is rather the result of neurotransmitter modulation (dopamine and serotonin) than modification of the disease pathology (Lee et al., Reference Lee, Chu, Sim, Heo and Kim2008).
The great advantage of phytotherapeutic interventions is their good tolerability and high safety profile. Studies have shown that Melissa officinalis was well-tolerated and did not cause safety issues (Noguchi-Shinohara et al., Reference Noguchi-Shinohara, Ono, Hamaguchi, Nagai, Kobayashi, Komatsu, Samuraki-Yokohama, Iwasa, Yokoyama, Nakamura and Yamada2020). Furthermore, phytotherapeutic agents often outperform conventional medications in terms of safety. In clinical trials, Crocus sativus demonstrated similar efficacy and a better safety profile compared to donepezil or memantine (Akhondzadeh et al., Reference Akhondzadeh, Sabet, Harirchian, Togha, Cheraghmakani, Razeghi, Hejazi, Yousefi, Alimardani, Jamshidi, Zare and Moradi2010; Farokhnia et al., Reference Farokhnia, Shafiee Sabet, Iranpour, Gougol, Yekehtaz, Alimardani, Farsad, Kamalipour and Akhondzadeh2014b). Ginkgo biloba extract (EGb 761) was also well tolerated, and its use was not associated with (serious) adverse events (van Dongen et al., Reference van Dongen, van Rossum, Kessels, Sielhorst and Knipschild2000; Mazza et al., Reference Mazza, Capuano, Bria and Mazza2006). Furthermore, substances such as Melissa and Salvia have a direct positive effect on neuropsychiatric symptoms (BPSD), including a reduction in agitation and irritability, with agitation being less frequently observed in the groups treated with these herbs than in the placebo groups (Akhondzadeh et al., Reference Akhondzadeh, Noroozian, Mohammadi, Ohadinia, Jamshidi and Khani2003a, Reference Akhondzadeh, Noroozian, Mohammadi, Ohadinia, Jamshidi and Khani2003b).
Many of the clinical trials analysed, especially those involving new or less frequently studied substances, are characterised by significant limitations in sample size. Examples include studies with very small sample sizes, such as the Cistanche tubulosa study and Ginkgo biloba study, which included only 18 patients each (Le Bars et al., Reference Le Bars, Katz, Berman, Itil, Freedman and Schatzberg1997; Guo et al., Reference Guo, Zhou, Wang, Huang, Lee, Su and Lu2013), the Melissa officinalis study (23 participants) (Noguchi-Shinohara et al., Reference Noguchi-Shinohara, Ono, Hamaguchi, Nagai, Kobayashi, Komatsu, Samuraki-Yokohama, Iwasa, Yokoyama, Nakamura and Yamada2020), Choto-san (20 participants) (Yamaguchi et al., Reference Yamaguchi, Matsubara and Kobayashi2004), Yokukansan (12 participants) (Nagata et al., Reference Nagata, Yokoyama, Yamazaki, Takano, Maeda, Takahashi and Terayama2012), ferulic acid and Angelica archangelica (20 participants) (Kimura et al., Reference Kimura, Hayashida, Murata and Takamatsu2011), or the grape powder formulation study (10 participants) (Lee et al., Reference Lee, Torosyan and Silverman2017). This small sample size means that conclusions drawn from even large effect sizes (Cohen’s d), such as those observed in small studies with Vitis vinifera (d = 1.47) (Lee et al., Reference Lee, Torosyan and Silverman2017) or Zataria multiflora (d = 1.6) (Ansari et al., Reference Ansari, Sargazi-Moghadam, Tajadini, Kamali, Kamali, Dehesh, Shojaei and Sharififar2025), are subject to a high risk of bias. Small sample sizes make it difficult to assess whether the obtained large effect sizes (Cohen’s d) are reliable and whether a given phytopharmaceutical could actually be considered a disease-modifying drug (DMT).
The lack of standardisation of plant extracts is one of the most serious challenges in phytotherapy, which is directly reflected in the sources analysed. The use of different extraction methods and preparation forms (standardised extracts, powders, decoctions, concentrates) significantly contributes to the inconsistency of reported results and hinders their direct comparison. The analysed studies use dramatically different formulations, which directly translates into variability in results. For example, one study on Melissa officinalis used an extract standardised for rosmarinic acid content, achieving a medium effect size (d = −0.55) (Noguchi-Shinohara et al., Reference Noguchi-Shinohara, Ono, Hamaguchi, Nagai, Kobayashi, Komatsu, Samuraki-Yokohama, Iwasa, Yokoyama, Nakamura and Yamada2020). However, an older study, which described the preparation only as ‘extract’, reported an extremely high effect size (d = −7.72) (Akhondzadeh et al., Reference Akhondzadeh, Noroozian, Mohammadi, Ohadinia, Jamshidi and Khani2003a). This discrepancy may be due to differences in the concentration of active ingredients obtained using different extraction methods. Studies on Panax ginseng and Cosmos caudatus used powder, while studies on Morus nigra used concentrate (Lee et al., Reference Lee, Torosyan and Silverman2017; You et al., Reference You, Shahar, Rajab, Haron, Yahya, Mohamad, Din and Maskat2021b; Güçer Öz et al., Reference Güçer Öz, Naharcı, Çelebi, Rakıcıoğlu and Göktaş2024). These formulations typically have lower compositional consistency than solvent-based extracts, which may explain why in some cases (e.g. ginseng) no difference was observed compared to placebo. The high heterogeneity index values calculated in our study (I 2 from 88.3% to 98.2%) provide mathematical evidence that the differences in results are not accidental. They result largely from the fact that different chemicals were actually tested in different studies under the same plant name (e.g. saffron or ginkgo) in terms of their phytochemical profile.
The clinical efficacy of phytopharmaceuticals must always be considered in the context of their safety, especially in the geriatric population, which often has multiple comorbidities. For instance, Ginkgo biloba’s phytocompounds (gingkolides) may inhibit platelet-activating factor (PAF). Therefore, patients taking anticoagulants (e.g. warfarin) or antiplatelet drugs (e.g. aspirin) should be monitored for an increased risk of bleeding, which is particularly important in older adults with cardiovascular disease (Bent et al., Reference Bent, Goldberg, Padula and Avins2005; Koch, Reference Koch2005). The lack of long-term studies on the toxicity and interactions of these extracts after many months of use requires caution in recommending them as stand-alone therapies in advanced stages of AD. Furthermore, many of the substances analysed, such as Crocus sativus, Melissa officinalis, Salvia officinalis, and Bacopa monnieri, affect the cholinergic pathway by inhibiting acetylcholinesterase (AChE) activity or receptor activity. Using them as a complementary option alongside standard medications, such as donepezil, may lead to additive pharmacodynamic effects. Although phytopharmaceuticals are often better tolerated than conventional medications, the lack of long-term studies on their use makes it difficult to fully assess the risk of cumulative adverse effects in complex drug regimens.
Another significant limitation is the short duration of interventions. Although some studies, such as those involving Crocus sativus, lasted up to 12 months (Farokhnia et al., Reference Farokhnia, Shafiee Sabet, Iranpour, Gougol, Yekehtaz, Alimardani, Farsad, Kamalipour and Akhondzadeh2014a; Tsolaki et al., Reference Tsolaki, Karathanasi, Lazarou, Dovas, Verykouki, Karacostas, Georgiadis, Tsolaki, Adam, Kompatsiaris and Sinakos2016), a significant number of interventional studies lasted only 3 to 6 months, and the shortest only 4 weeks (Kimura et al., Reference Kimura, Hayashida, Murata and Takamatsu2011; Iwasaki et al., Reference Iwasaki, Kosaka, Mori, Okitsu, Furukawa, Manabe, Yoshita, Kanamori, Ito, Wada, Kitayama, Horiguchi, Yamaguchi, Takayama, Fukuhara, Ouma, Nakano, Hashimoto and Kinoshita2012; Nagata et al., Reference Nagata, Yokoyama, Yamazaki, Takano, Maeda, Takahashi and Terayama2012 Albertyn et al., Reference Albertyn, Guu, Chu, Creese, Young, Velayudhan, Bhattacharyya, Jafari, Kaur, Kandangwa, Carter and Aarsland2025). Such a short time frame may be insufficient for evaluating phytotherapeutics as disease-modifying treatments (DMTs). We strongly recommend long-term follow-up periods (e.g. 12–24 months) for future research designs.
Summary
In light of the evidence, phytopharmaceuticals have a promising role as a co-therapeutic option or alternative for patients with dementia who do not tolerate or have contraindications to standard medications. However, further research is necessary to translate these initial promising results into clinical practice. Longer-term, multicenter, randomised controlled trials (RCTs) with larger patient groups using consistent and sensitive outcome measures (such as the ADAS-Cog and NPI) are recommended. This is particularly important for compounds with large effects (e.g. Zataria multiflora and Cosmos caudatus), for which preliminary conclusions are limited by very small sample sizes.
Given that dementia represents a growing public health challenge, this area offers a critical, extensive, and high-priority scope for exploring novel therapeutic avenues.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/neu.2026.10085.
Data availability statement
All data collected for this systematic review are available in the text.
Author contributions
KA Kaczmarek-Kryszak – literature search, data collection and extraction, data processing, manuscript writing
M Dobrzyńska – literature search, data collection and extraction, data processing
M Banaszak – data processing
S Drzymała-Czyż – correction and supervision
Funding statement
Authors declare no funding.
Competing interests
Authors declare no conflict of interests.
Registration
This systematic review was registered in the PROSPERO register under the number CRD420251239096.
AI declaration
Graphical abstract and Figure 1 were generated using AI, based on original descriptions.




 Open access
Open access