


Introduction
The Centers for Disease Control and Prevention (CDC) estimates that approximately 1 in 31 hospitalized patients has at least one healthcare-associated infection (HAI). 1 As hospitals seek to reduce and eliminate HAIs, a key step is understanding the causes of health disparities. Reference Serpa, Gemeinhardt and Arias2 Health disparities are health differences linked to economic, social and/or environmental disadvantages. These disparities are best captured using the framework of social determinants of health (SDOH), or “the conditions in which people are born, grow, live, work and age.” 3 Attention is shifting towards identifying and addressing disparities in HAIs. Evaluation of health disparities data and the association with HAIs may have significant implications for quality improvement metrics and hospital reimbursement. 4
Although there is increasing interest in racial and ethnic disparities in HAIs and associations with SDOH, the scope of evidence on the topic has not been widely reported. Reference Advani, Smith and Kalu5 A number of studies have looked at race, ethnicity, and/or SDOH and associations with specific HAIs, but few studies have summarized the literature sufficiently to inform national policy. Reference McGrath, Bettinger and Stimpson6–Reference Gualandi, Mu and Bamberg8 To better understand the current landscape, we performed a systematic review and meta-analysis to evaluate the disparities in HAIs by race and ethnicity with additional review for SDOH measures. The review is centered around racial and ethnic disparities, but the authors recognize the differential healthcare exposures and structural inequities which drive these disparities. Reference Chen, Khazanchi, Bearman and Marcelin9 We hypothesized that we would find significant differences in the rates of HAIs across different racial and ethnic groups.
Methods
Systematic Review Methodology: We followed the 2020 Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) checklist to ensure that all components of preferred methodology were incorporated into this review. Review protocol was registered with the PROSPERO database (Protocol# CRD42024429721) and the full search strategy with inclusion/exclusion criteria are available in the supplement (S1–S3). The primary review question was: Is there an association between race, ethnicity and social determinants of health and the incidence of HAIs? We searched Medline (OVID), Embase (Elsevier), and Scopus (Elsevier) for manuscripts published between 2008 and 2022 describing reportable HAIs among inpatients and with reference to race or ethnicity. We imported all citations to Covidence (www.covidence.org, Veritas Health Innovation) and removed duplicates. Studies were included if differences in HAIs based upon race, ethnicity or SDOH were evaluated. We used the Office of Disease Prevention and Health Promotion’s Healthy People 2030 framework for SDOH with 5 major categories: economic stability, neighborhood and built environment, education access and quality, social and community context, and health care access and quality. 3 Given the importance of social context, we only included studies based in the United States. Two blinded reviewers (listed authors) assessed all studies first in a title and abstract review. If both reviewers agreed that the study qualified, the article moved to a full text review. Studies undergoing full text review were again assessed by two blinded reviewers and required agreement to be included in the final review. At both stages, discrepancies between reviewers were resolved by a third blinded reviewer. Studies under consideration were then evaluated utilizing the Joanna Briggs Institute critical appraisal tools for an assessment of bias and internal validity before final inclusion (S4). Reference Barker, Hasanoff, Aromataris, Stone, Leonardi-Bee, Sears, Habibi, Klugar, Tufanaru, Moola, Liu and Munn10 All studies that met these inclusion criteria were summarized as part of the systematic review. Relevant statistical data were extracted from the studies into a secure REDCap database for incorporation into the accompanying meta-analysis.
Statistical analysis
Meta-analysis was employed for data synthesis when at least three manuscripts identified by the systematic review examined a common infection, common exposure, and common reference group (e.g., rate of HAI in Black vs White patients) and provided sufficient statistical information (e.g., odds ratios). Among studies that met these criteria, infections evaluated included surgical site infection (SSI), central line-associated bloodstream infection (CLABSI), and hospital-onset Clostridioides difficile (HO-CDI). No meta-analysis was performed related to methicillin-resistant Staphylococcus aureus (MRSA) infections, ventilator-associated pneumonias or other HAI outcomes due to inadequate numbers of studies. Exposure/reference categories that were considered included race, ethnicity, sex, and insurance status with reference categories based upon source literature. Unadjusted log relative risks (RR) or unadjusted log odds ratios (OR) from the individual studies were combined using random-effects meta-analysis, with heterogeneity estimated by previously established methods. Reference DerSimonian and Laird11–Reference Higgins, Thompson, Deeks and Altman13 If RR or OR were directly reported in the individual studies, standard errors were extracted from the study or derived from the 95% confidence intervals. If RR or OR were not directly reported, but sample sizes and event counts were reported, then the metrics and corresponding standard errors were calculated. The final RR or OR, 95% confidence interval, and test of heterogeneity were reported. SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA) was used for all analyses.
Results
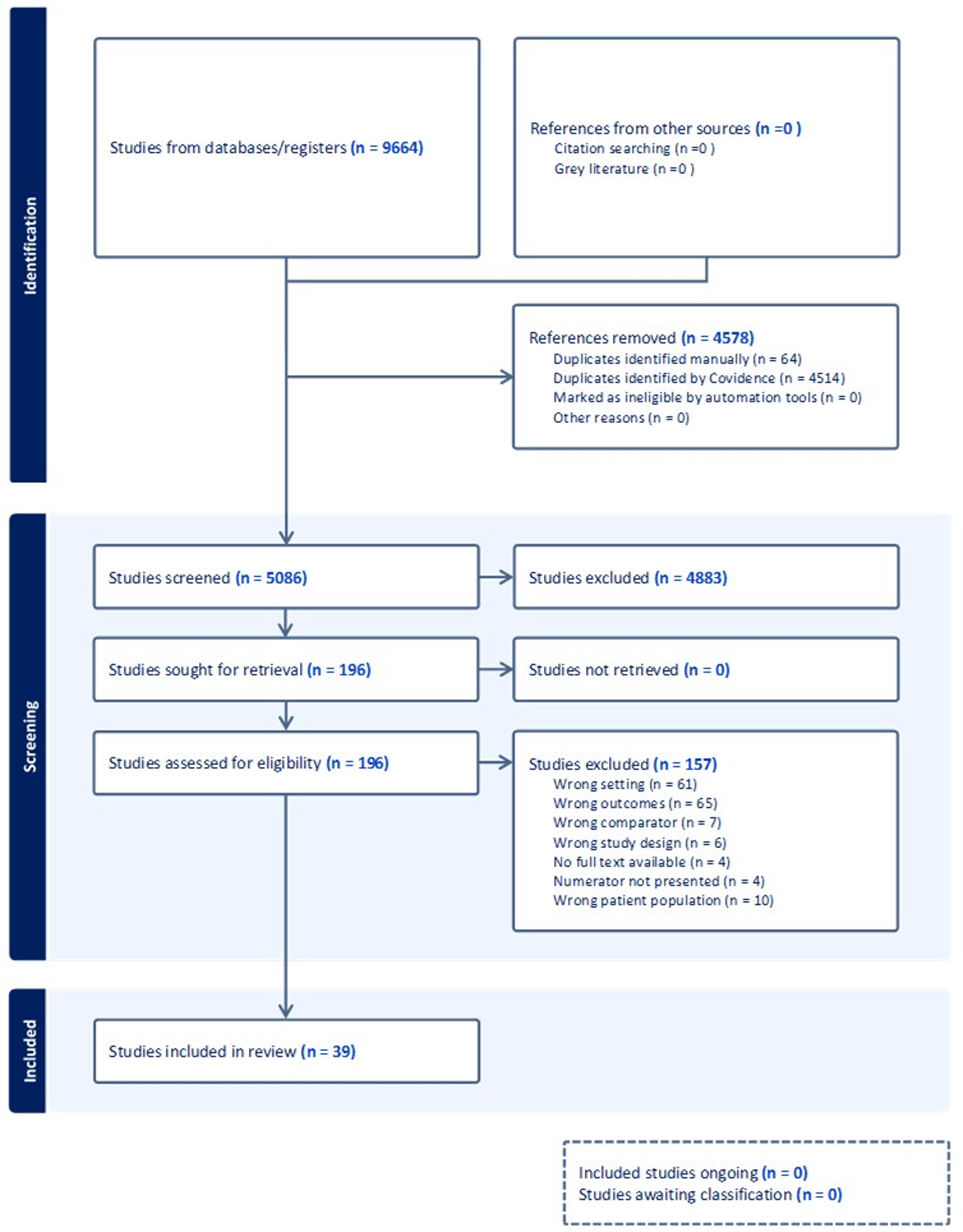
We screened 5,150 titles and abstracts; 4,883 studies were excluded due to irrelevance, leaving 203 studies for full text review. Of these, 39 studies met criteria for inclusion in our systematic review (Figure 1). Details for each included study are summarized in Table 1. Included studies primarily consisted of retrospective cohort data with the addition of two prospective cohort studies and two retrospective case-control studies. Of these 39 studies, Reference Bakullari, Metersky and Wang7,Reference Gualandi, Mu and Bamberg8,Reference Allareddy, Das and Lee14–Reference Zarzaur, Bell, Croce and Fabian50 18 prespecified an investigation into race, ethnicity or SDOH, Reference Bakullari, Metersky and Wang7,Reference Gualandi, Mu and Bamberg8,Reference Arsoniadis, Ho, Melton, Madoff, Le and Kwaan15–Reference Browne, Novicoff and D’Apuzzo17,Reference Edwards, Sarvepalli, Mazzei, Acevedo, Lu and Zhao20,Reference Qi, Peacock, Luke, Barker, Olsen and Joynt Maddox27,Reference Singh and Cleveland30–Reference Wang, Piple and Chen34,Reference Snyder and Burjonrappa38–Reference Argamany, Delgado and Reveles40,Reference Vader, Weldie, Welles, Kutzler and Goldstein44,Reference Jeon, Muennig, Furuya, Cohen, Nash and Larson46,Reference Ricciardi, Selker, Baxter, Marcello, Roberts and Virnig49,Reference Zarzaur, Bell, Croce and Fabian50 while the remaining studies broadly assessed patient characteristics and reported a result relevant to our systematic review. Twenty-three studies examined SSI, Reference Bakullari, Metersky and Wang7,Reference Allareddy, Das and Lee14–Reference Zhao, Marchaim and Palla35 6 examined CDI, Reference Bakullari, Metersky and Wang7,Reference Argamany, Delgado and Reveles40–Reference Vader, Weldie, Welles, Kutzler and Goldstein44 5 examined CLABSI, Reference Bakullari, Metersky and Wang7,Reference Fargen, Neal, Blackburn, Hoh and Rahman36–Reference Willer, Tobias, Suttle, Nafiu and Mpody39 and 8 explored other HAIs or pooled infection outcomes Reference Bakullari, Metersky and Wang7,Reference Gualandi, Mu and Bamberg8,Reference Burke, Halpern, Baron and Gutierrez45–Reference Zarzaur, Bell, Croce and Fabian50 (Table 1). Seven studies focused on pediatric patients Reference Bucher, Guth and Elward18,Reference Simon, Hall and Riva-Cambrin29,Reference Snyder and Burjonrappa38,Reference Willer, Tobias, Suttle, Nafiu and Mpody39,Reference Burke, Halpern, Baron and Gutierrez45,Reference Liu, Sakarovitch, Sigurdson, Lee and Profit47,Reference Milstone, Goldner, Ross, Shepard, Carroll and Perl48 and the remaining 32 analyzed adults. The most commonly studied exposures were race and ethnicity (n = 32), followed by age (n = 16), sex (n = 15), and insurance status (n = 11). Based on the available data, 22 studies were included in the summary meta-analyses. Reference Bakullari, Metersky and Wang7,Reference Blum, Singh, Lee, Richardson, Chen and Ibrahim16,Reference Bucher, Guth and Elward19–Reference Singh, Debbaneh and Rivero31,Reference Zhao, Marchaim and Palla35,Reference Snyder and Burjonrappa38–Reference Argamany, Delgado and Reveles40,Reference Rosenblatt, Mehta and Cohen-Mekelburg42,Reference Vader, Weldie, Welles, Kutzler and Goldstein44,Reference Ricciardi, Selker, Baxter, Marcello, Roberts and Virnig49 There was sufficient data to examine 10 HAI/exposure combinations with meta-analytic techniques. A visual summary of included study findings by HAI and exposure is available in the supplement (S5,S6).
PRISMA diagram for study inclusion.

Figure 1 Long description
The flowchart begins with the identification stage, where studies from databases and registers total 9664, and references from other sources are zero. It then shows the removal of 4578 references due to duplicates and other reasons. The screening stage involves 5086 studies, with 4883 studies excluded, leaving 196 studies sought for retrieval. All 196 studies are retrieved and assessed for eligibility, with 157 studies excluded for various reasons such as wrong setting, wrong outcomes, and wrong comparator. Finally, 39 studies are included in the review.
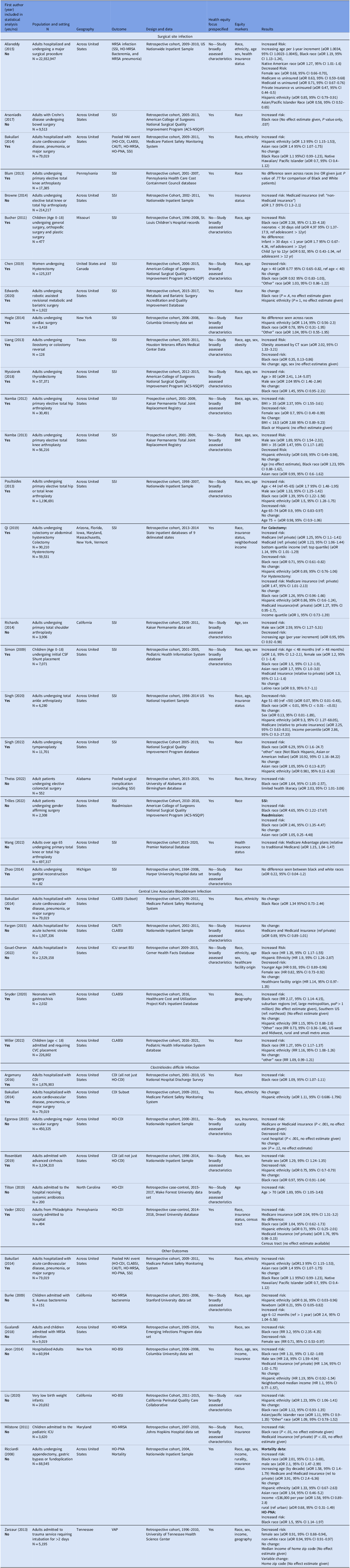
Included studies by healthcare-associated infection (HAI) including study designs and results

Table 1 Long description
A table with 39 rows and 7 columns summarizing healthcare-associated infection studies. The columns include Study ID, Design, Population, Infection Type, Exposures, Results, and Notes. The table details various study designs such as retrospective cohort, prospective cohort, and retrospective case-control. It lists different infection types like SSI, CDI, CLABSI, and other HAIs. The exposures studied include race, ethnicity, age, sex, and insurance status. The results and notes provide specific findings from each study.
Note: White race is the reference group for all racial comparisons. Private insurance is the reference group for all insurance comparisons unless otherwise specified.
Surgical site infection
SSI was the most commonly studied HAI (n = 23), representing over half of the included articles. Most studies evaluated differences in patient outcomes for a single category of procedures (e.g., orthopedic surgery); only three studies evaluated surgical patients more broadly. Reference Bakullari, Metersky and Wang7,Reference Allareddy, Das and Lee14,Reference Bucher, Guth and Elward18 The most frequently studied surgical categories were orthopedic surgeries (n = 8), bowel surgeries (n = 5), and gynecologic surgeries (n = 3). There was a high degree of heterogeneity across studies regarding patient inclusion/exclusion criteria, definitions of the SSI outcome, and strategies for dealing with incomplete racial and ethnicity data. Despite this heterogeneity in approach, we determined all included studies were methodologically sound on the basis of our risk of bias assessments. Sufficient data were available to perform meta-analysis for race, ethnicity, sex, and type of medical insurance.
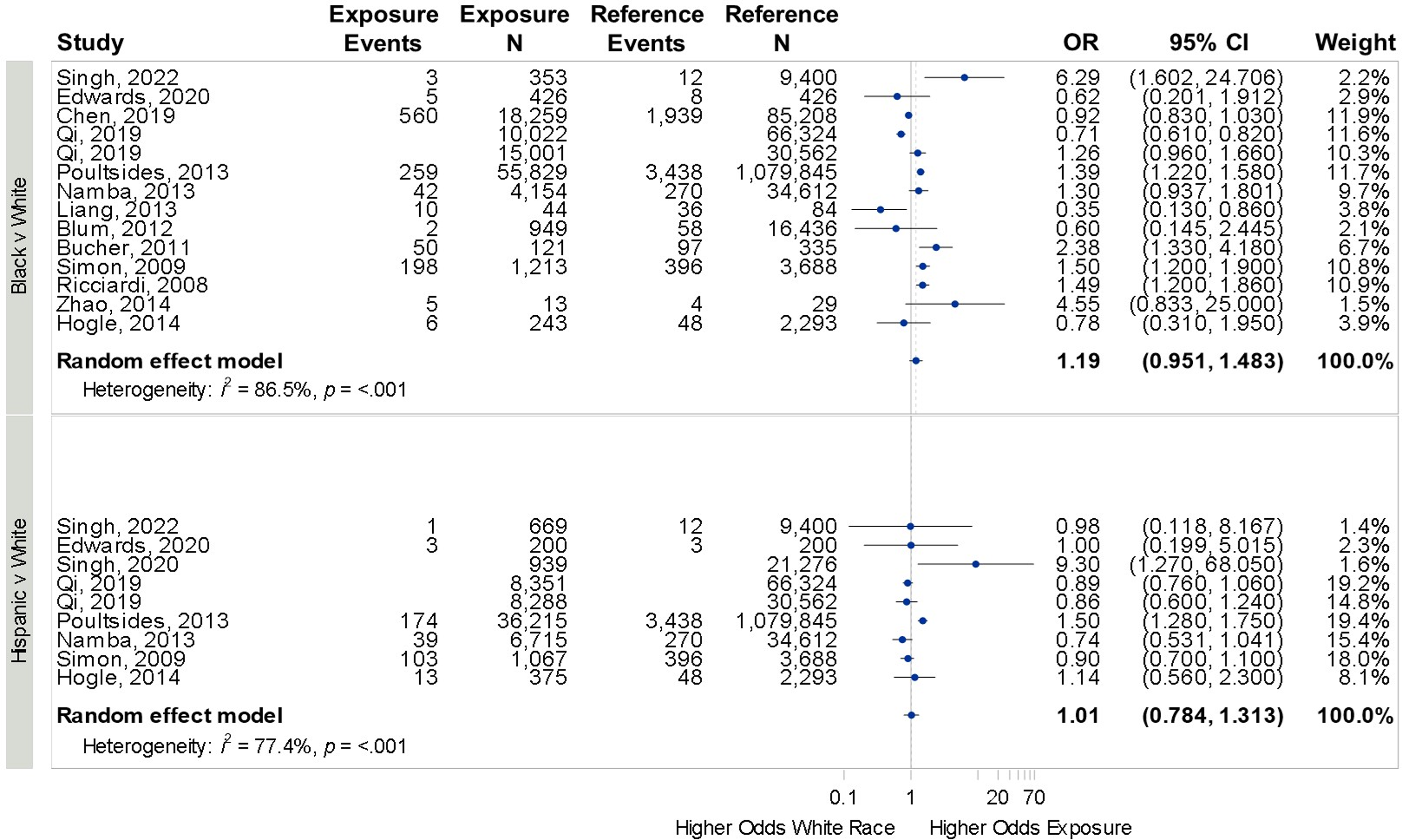
Twenty studies compared SSI rates between Black and White patients; Reference Bakullari, Metersky and Wang7,Reference Allareddy, Das and Lee14–Reference Blum, Singh, Lee, Richardson, Chen and Ibrahim16,Reference Bucher, Guth and Elward18–Reference Qi, Peacock, Luke, Barker, Olsen and Joynt Maddox27,Reference Simon, Hall and Riva-Cambrin29–Reference Trilles, Chaya and Brydges33,Reference Zhao, Marchaim and Palla35 14 were included in the statistical analysis. Eleven studies compared SSI among Hispanic and White patients, Reference Bakullari, Metersky and Wang7,Reference Allareddy, Das and Lee14,Reference Edwards, Sarvepalli, Mazzei, Acevedo, Lu and Zhao20,Reference Hogle, Cohen, Hyman, Larson and Fowler21,Reference Namba, Inacio and Paxton24–Reference Qi, Peacock, Luke, Barker, Olsen and Joynt Maddox27,Reference Simon, Hall and Riva-Cambrin29–Reference Singh, Debbaneh and Rivero31 nine of which were included in the statistical analysis. Six studies compared SSI among Black and Hispanic patients. No difference was seen in SSI across any of the racial and ethnic comparisons: Black vs White: OR 1.19 (95% CI 0.95–1.48, I 2 = 86.5%), Hispanic vs White: OR 1.01 (95% CI 0.78–1.31, I 2 = 77.4%), (Figure 2). Eight studies compared SSI rates between male and female patients, Reference Allareddy, Das and Lee14,Reference Liang, Li, Avellaneda, Moffett, Hicks and Awad22–Reference Poultsides, Ma, Della Valle, Chiu, Sculco and Memtsoudis26,Reference Richards, Inacio and Beckett28,Reference Simon, Hall and Riva-Cambrin29 seven of which were included in the statistical analysis. Female sex was associated with a lower SSI rate : OR 0.74 (95% CI 0.54–0.97, I 2 = 90.6%, S7). Five studies compared outcomes in patients with public vs private insurance, Reference Allareddy, Das and Lee14,Reference Browne, Novicoff and D’Apuzzo17,Reference Qi, Peacock, Luke, Barker, Olsen and Joynt Maddox27,Reference Singh and Cleveland30,Reference Wang, Piple and Chen34 three of which were included in the statistical analysis. Medicare insurance was associated with a higher SSI incidence: OR 1.28 (95% CI 1.16–1.41, I 2 = 100%, S8).
Forrest plot for odds of surgical site infection across race and ethnicity.
Individual study details are available in Table 1. Surgeries were diverse including total knee, hip, or shoulder arthroplasty, hysterectomy, bariatric surgery, colon surgery, genital reconstruction, and other general surgeries.

Figure 2 Long description
A horizontal dot plot compares the odds of surgical site infection across different races and ethnicities. The plot is divided into two sections: Black vs. White and Hispanic vs. White. Each section lists multiple studies with their respective data points. The x-axis represents the odds ratio (OR) ranging from 0.1 to 20, while the y-axis lists the studies involved. Each dot represents the OR for a specific study, with horizontal lines indicating the 95 percent confidence interval (CI). The weight percentage of each study is also shown. The Black vs. White section includes studies from 2008 to 2022, with a random effect model OR of 1.19 and a heterogeneity of 86.5 percent. The Hispanic vs. White section includes studies from 2009 to 2022, with a random effect model OR of 1.01 and a heterogeneity of 77.4 percent. The plot highlights variations in infection odds across different racial and ethnic groups, with some studies showing higher odds for certain groups. All values are approximated.
The low study number and significant methodological heterogeneity precluded meta-analysis of other SDOH. Specifically, studies were inconsistent in their definitions of age groups, precluding a formal meta-analysis of the risk of age on SSI, and individual studies showed mixed results for the interaction between age and SSI. One study evaluated patient income as a risk factor for SSI, demonstrating low income to be a risk factor. Reference Qi, Peacock, Luke, Barker, Olsen and Joynt Maddox27 One study found an association between low health literacy (defined by a score <12 on the Brief Health Literacy Screen) and SSI. Reference Theiss, Wood and McLeod32 Three studies suggested an increased SSI risk in patients with obesity, though insufficient information was provided in these studies to perform meta-analysis. Reference Liang, Li, Avellaneda, Moffett, Hicks and Awad22,Reference Namba, Inacio and Paxton24,Reference Namba, Inacio and Paxton25
Clostridioides difficile
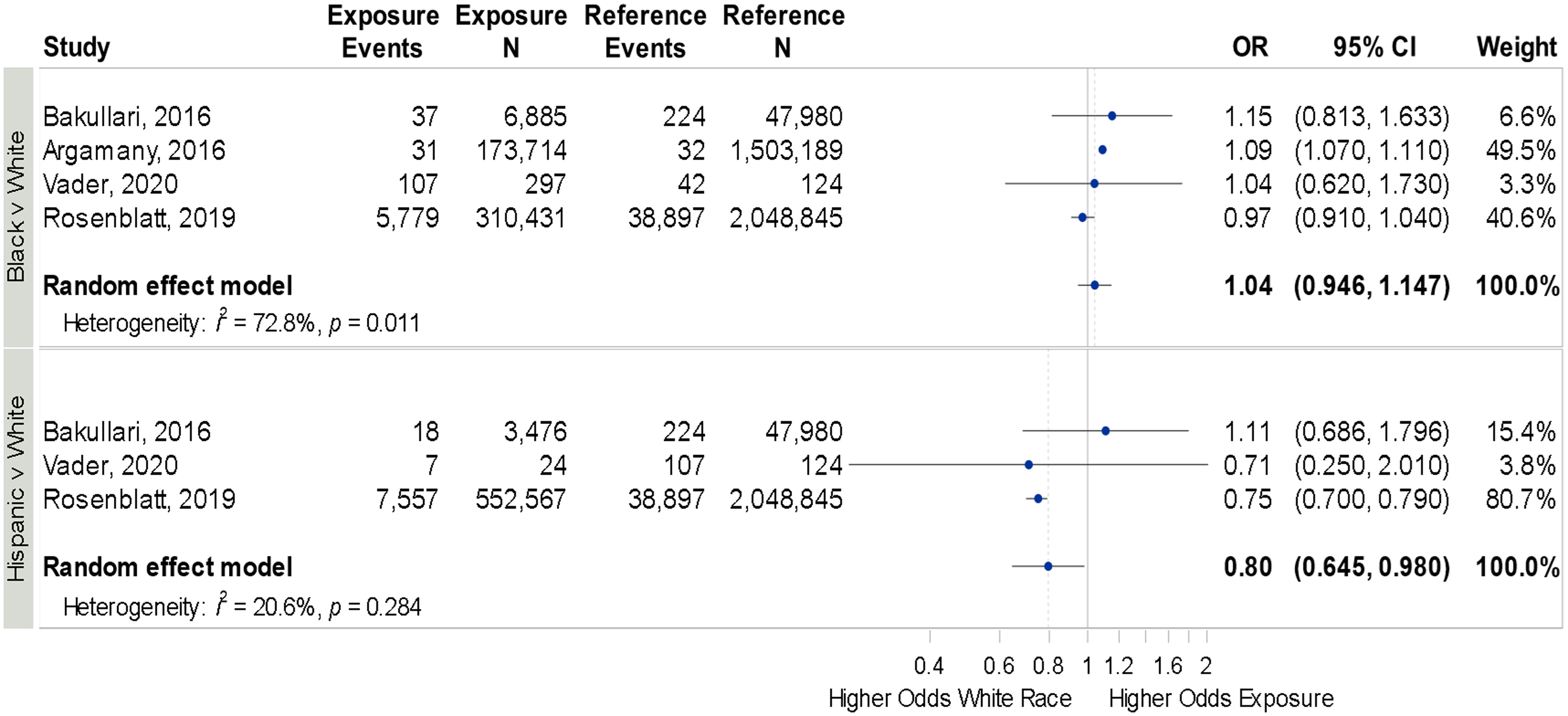
Of the 6 studies examining HO-CDI, 3 evaluated all hospitalized patients Reference Bakullari, Metersky and Wang7,Reference Argamany, Delgado and Reveles40,Reference Vader, Weldie, Welles, Kutzler and Goldstein44 while the other 3 evaluated distinct populations of inpatients (patients receiving systemic antibiotics, Reference Tilton and Johnson43 patients with advanced cirrhosis, Reference Rosenblatt, Mehta and Cohen-Mekelburg42 or patients undergoing major vascular surgery Reference Egorova, Siracuse, McKinsey and Nowygrod41 ), again resulting in significant heterogeneity across the included studies. Four studies evaluated race, ethnicity and HO-CDI, Reference Bakullari, Metersky and Wang7,Reference Argamany, Delgado and Reveles40,Reference Rosenblatt, Mehta and Cohen-Mekelburg42,Reference Vader, Weldie, Welles, Kutzler and Goldstein44 3 of which were included in the meta-analysis. No difference in HO-CDI was seen between Black and White patients (OR 1.04, 95% CI 0.93–1.14, I 2 = 72.8%), though Hispanic patients had a lower HO-CDI risk compared to White patients (OR 0.80, 95% CI 0.64–0.98, I 2 = 20.6%, Figure 3).
Forrest plot for odds of hospital-onset Clostridioides difficile infection across race and ethnicity.
Individual study details are available in Table 1.

Figure 3 Long description
The table presents a comparison of the odds of hospital-onset Clostridioides difficile infection across different races and ethnicities. It includes data from multiple studies, with columns for exposure events, exposure sample size, reference events, reference sample size, odds ratio (OR), confidence interval (CI), and weight. The studies compare Black versus White and Hispanic versus White populations. For Black versus White, the studies are Bakullari, 2016; Argaman, 2016; Vader, 2020; and Rosenblatt, 2019. For Hispanic versus White, the studies are Bakullari, 2016; Vader, 2020; and Rosenblatt, 2019. The random effect models show an overall OR of 1.04 for Black versus White and 0.80 for Hispanic versus White. The table highlights the heterogeneity and p-values for each model.
Of studies not included in the meta-analysis, 2 studies evaluated sex, only 1 of which showed female sex to be a risk factor for HO-CDI. Reference Egorova, Siracuse, McKinsey and Nowygrod41,Reference Rosenblatt, Mehta and Cohen-Mekelburg42 One study evaluated patient census tract and demonstrated no change in risk of HO-CDI based on residential address. Reference Vader, Weldie, Welles, Kutzler and Goldstein44 One study showed a significant association between HO-CDI and age > 70. Reference Tilton and Johnson43 Another single study showed a decreased HO-CDI risk when hospitalized in a rural setting. Reference Egorova, Siracuse, McKinsey and Nowygrod41 Two studies reported an increased risk of HO-CDI associated with Medicare health insurance compared to private insurance (Table 1). Reference Egorova, Siracuse, McKinsey and Nowygrod41,Reference Vader, Weldie, Welles, Kutzler and Goldstein44
Central line associated bloodstream infections and hospital onset bloodstream infections
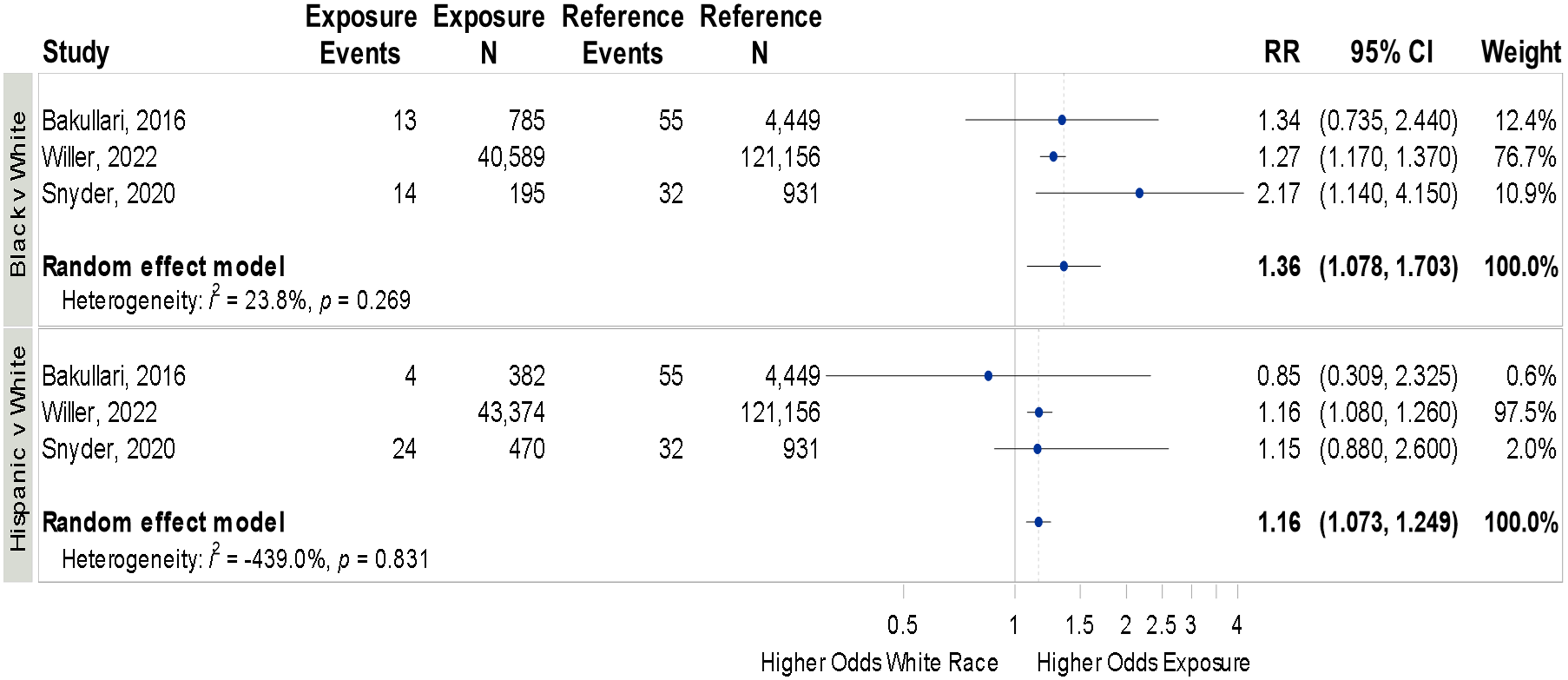
Five studies evaluated CLABSI with substantial heterogeneity in patient populations and clinical context; one exclusively included neonates, Reference Snyder and Burjonrappa38 one evaluated all pediatric patients, Reference Willer, Tobias, Suttle, Nafiu and Mpody39 and three included adults on single units or with a specific diagnosis. Reference Bakullari, Metersky and Wang7,Reference Fargen, Neal, Blackburn, Hoh and Rahman36,Reference Gouel-Cheron, Swihart and Warner37 Four studies evaluated race and CLABSIs, Reference Bakullari, Metersky and Wang7,Reference Gouel-Cheron, Swihart and Warner37–Reference Willer, Tobias, Suttle, Nafiu and Mpody39 three of which (two pediatric and one adult) were included in the meta-analysis. Both Black and Hispanic patients had higher CLABSI rates compared to White patients: Black vs White OR 1.36 (95% CI 1.07–1.70,I 2 = 23.8%), Hispanic vs White OR 1.16 (95% CI 1.07–1.24, I 2 = 100%; Figure 4).
Forrest plot for odds of central line associated bloodstream infections across race and ethnicity.
Individual study details are available in Table 1.

Figure 4 Long description
The bar graph compares the odds of central line associated bloodstream infections across different races and ethnicities. It features horizontal bars representing the relative risk (RR) with 95% confidence intervals (CI) for each study. The x-axis ranges from 0.5 to 4, indicating the higher odds for white race versus exposure. The y-axis lists the studies by authors and years: Bakulari, 2016; Willer, 2022; Snyder, 2020. The graph is divided into two sections: Black vs. White and Hispanic vs. White. Each section includes data from the three studies, with the random effect model summarized at the bottom. The bars show the RR values and their CI, with weights assigned to each study. The color scheme uses blue for the data points and lines. The graph highlights the heterogeneity and p-values for the random effect models. All values are approximated.
Of studies not included in meta-analyses, one showed female sex was associated with a lower CLABSI incidence (Table 1). Reference Gouel-Cheron, Swihart and Warner37 In one pediatric study examining HO-BSI, age less than 1 year (excluding neonates hospitalized at birth) was associated with higher HO-BSI rates; Reference Burke, Halpern, Baron and Gutierrez45 younger age (as a continuous linear variable) was associated with lower CLABSI risk in an adult study. Reference Gouel-Cheron, Swihart and Warner37 One study of HO-BSI found no association with patient income. Reference Jeon, Muennig, Furuya, Cohen, Nash and Larson46 Two studies found that public insurance was associated with a higher CLABSI or HO-BSI incidence. Reference Fargen, Neal, Blackburn, Hoh and Rahman36,Reference Jeon, Muennig, Furuya, Cohen, Nash and Larson46 One study explored patient localities and found that patients from suburban areas (ref: central metropolitan, population >1 million) and location in the southern US (ref: Northeast US) had higher CLABSI incidences. Reference Snyder and Burjonrappa38
Other HAIs and exposures
No other meta-analyses could be performed from the remaining extracted studies and data. Two studies examined risk factors for ventilator-associated pneumonia (VAP) or hospital-onset pneumonia, with one suggesting an increased risk in patients of Black race and the other suggesting a decreased risk for “non-White” race. Reference Ricciardi, Selker, Baxter, Marcello, Roberts and Virnig49,Reference Zarzaur, Bell, Croce and Fabian50 Median income of home zip code was not associated with a change in VAP rates, while female sex was associated with a lower incidence of VAP. Reference Zarzaur, Bell, Croce and Fabian50
Three studies examined various hospital-onset MRSA infections (e.g., SSI, skin infection, and BSI). Reference Gualandi, Mu and Bamberg8,Reference Allareddy, Das and Lee14,Reference Milstone, Goldner, Ross, Shepard, Carroll and Perl48 All of these identified Black race as a risk factor, but were inconsistent on the effects observed for Hispanic and Asian ethnic and racial groups. Two manuscripts suggested female sex was associated with a lower MRSA incidence. Reference Gualandi, Mu and Bamberg8,Reference Allareddy, Das and Lee14 A single study suggested public health insurance was associated with an increased risk of MRSA infections relative to private insurance. Reference Milstone, Goldner, Ross, Shepard, Carroll and Perl48
Discussion
To our knowledge, this is the first systematic review and meta-analysis to evaluate the association of race and ethnicity with reportable HAIs such as SSI, HO-CDI, and CLABSI. We found that 1) methods used to evaluate race, ethnicity, SDOH, and HAI outcomes were highly heterogeneous and 2) the presence and directionality of differences between racial and ethnic groups varied based on the underlying disease process. During the selection process, we also reviewed the papers for additional SDOH measures. Public health insurance remained a persistent risk factor compared to private health insurance across almost all types of HAI; otherwise, most SDOH evaluated in our study varied by disease process. Most significantly, however, our study highlighted the paucity of data looking at the influence of most SDOH on HAI disparities, particularly in pediatric populations.
Although studies identifying racial and ethnic disparities in HAIs are increasing, this area of research is relatively new. 51 Few studies have risen to the level of systematic reviews or meta-analyses. In a previous study, our group identified 2 other systematic reviews that evaluated the associations between race, ethnicity, and SDOH with SSIs. Reference Advani, Smith and Kalu5 Both of these studies looked exclusively at neurosurgical patients; one showed an association between SSI and “non-white” race, and the other showed increased SSI risk in obese patients. Reference Mo, Ikwuezunma and Mun52,Reference Mendoza, Pangal and Cardinal53 Our current review includes data from a larger array of surgical procedures and a more diverse set of HAIs. The more expansive scope of this review is novel in emphasizing which combinations of SDOH domains and HAIs need further investigation.
Our analysis identified significant differences across racial and ethnic groups in CLABSI and HO-CDI but not amongst SSIs. Insufficient data existed to analyze other HAIs. It is unclear if these differences represent the unique pathophysiology and risk factors of these infections or are simply related to the lower number of studies in the CLABSI and HO-CDI analyses (fourteen SSI vs four HO-CDI and three CLABSI). Our search strategy focused on race and ethnicity with only secondary review of other SDOH, limiting our ability to make this determination. It is notable that beyond race, ethnicity, and sex, demographics required for most research, the only SDOH studied consistently enough to allow for meta-analysis was insurance status.
In preparing this manuscript, the authorship group is aware of the problematic nature of racial categories in clinical research. In American society, racial categorizations are primarily aggregate indicators of the degree of structural racism (including adverse SDOH profiles) that individuals have been exposed to over the course of their lives in our society. We fully acknowledge that racial categories are a social construct and have essentially no basis in biology, and our findings based on this reality do not imply any genetic associations with the pathophysiology of the observed disease states. However, in retrospect, we have determined that the study of racial associations with HAIs provide a crude yet useful insight into the effect of structural racism and racialization on the health outcomes of individuals stratified by race in the US. Given the limitations of our retrospective review (and the race-based variable collected in prior reports) further study is needed to better identify the precise drivers of disparate HAI outcomes among persons of different racial strata in the American context. The differences we observed by race in this meta-analysis provide the critical premise to justify further study along this line of investigation. Reference Flanagin, Frey and Christiansen54–Reference Kaplan and Bennett57
Few studies that examine racial and ethnic disparities consider the SDOH for which race and ethnicity may be a marker. More research is needed to disentangle the interdependent relationships of SDOH, race, and ethnicity before we can fully understand their independent effects. Systematic reviews with a narrower scope may provide further insight to these relationships. We initially attempted to use Boolean operators in our search that would look for any analysis of race, ethnicity or SDOH. This approach resulted in millions of articles and made for an untenable approach. We subsequently limited our search to race and ethnicity. By asking more targeted questions with specific SDOH variables and stricter inclusion criteria, more robust meta-analysis may be possible.
Two additional striking features of our review were the lack of prospective data and the dependence on readily available local or national databases such as the National Surgical Quality Improvement Program (NSQIP) or the National Inpatient Sample for outcome determination. Finding ways to incentivize the routine and accurate documentation of race, ethnicity, and SDOH will be essential to better understand health disparities in HAIs.
Our study has the following limitations. First, HAI outcomes largely used ICD codes for diagnosis or data available from large data sets as opposed to formal NHSN definitions for HAIs of interest. Additionally, included manuscripts had variable approaches for categorizing racial and ethnic groups, analyses of multiracial individuals, and accounting for patients with missing race or ethnicity data. For example, some studies considered Hispanic as a race mutually exclusive to other categories, and others considered it an ethnicity to be combined with other racial groups. Furthermore, some manuscripts focused on specific age ranges or conditions limiting generalizability to larger populations. Together these factors resulted in a very high level of heterogeneity across our included studies with most I 2 values >75%. As a result, we recommend strong caution with interpretation of statistical inference from our analyses. Second, many studies identified by our systematic review did not include sufficient primary data to allow for inclusion in our statistical analysis. In addition, as this review comes from the published literature, and many of the included studies did not prespecify a health equity focus, it is possible that studies demonstrating a racial or ethnic difference are overrepresented secondary to publication bias. Third, our search may not have identified all published studies that were applicable to our study objectives. For example, an additional search by the authors using their own terms was able to identify additional potentially relevant articles not originally identified. Reference See, Wesson and Gualandi58–Reference Pollack, Lowder, Keller, Chang, Gehlert and Olsen63 Despite these limitations, we believe this review is a valuable summary of the current landscape.
Conclusion
The study findings highlight potential racial and ethnic disparities in CLABSI and HO-CDI rates, but further work is needed to standardize how race and ethnicity are defined and collected across all electronic health record systems. Other SDOH, including healthcare access and support, community context, and economic stability are likely important drivers but, similarly, more research is needed to better elucidate these relationships. To facilitate robust health equity research, HAI surveillance, and prevention efforts, we need standardized definitions, and validated questions to report race, ethnicity, and social risk factors.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/ice.2026.10461.
Data availability statement
Data used in this study are readily available in the referenced publications.
Acknowledgements
The project described was supported in part by a contract (#75D30122F00002; PI—Anderson) from CDC to Duke University. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of CDC.
Financial support
This study was supported by the CDC Safety and Healthcare Epidemiology Prevention Research Development (SHEPheRD) Program.
Competing interests
Dr. Advani reports past support from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK grant no. K12DK100024), Centers for Disease Control and Prevention grant no. 5U54CK000616-02), the Society for Healthcare Epidemiology of America, and the Duke Claude D. Pepper Older Americans Independence Center (National Institute on Aging grant no. P30AG028716), as well as past consulting fees from Locus Biosciences, Sysmex America, GSK, bioMérieux, and the Infectious Diseases Society of America. Starting July 1, 2024, Dr. Advani became an employee of GSK/ViiV Healthcare holds financial equities in GSK. Dr Kalu reports grants from Bristol Myers Squibb Foundation and National Institute of Child Health and Human Development (NICHD No: HHSN275201800003I TO7) as well as consulting fees from IPEC Experts outside the submitted work.
Role of the funder/sponsor
CDC sponsors were involved in the design of the study and providing financial support. They were not involved in final review or approval of this manuscript.



 Open access
Open access