


Attention-deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterised by maladaptive patterns, including inattention, hyperactivity and impulsivity, that may result in functional limitations. Reference Meyer, Alaie, Ramklint and Isaksson1 The disorder typically manifests in early childhood and may persist into adolescence and adulthood. Reference Asherson2 ADHD has been linked to adverse educational, social and occupational outcomes, as well as reduced quality of life. Reference Fredriksen, Dahl, Martinsen, Klungsoyr, Faraone and Peleikis3,Reference Danckaerts, Sonuga-Barke, Banaschewski, Buitelaar, Döpfner and Hollis4 In addition, ADHD in children and adolescents is associated with a substantial economic burden driven primarily by education-related costs, followed by healthcare and caregiver expenses. Reference Schein, Adler, Childress, Cloutier, Gagnon-Sanschagrin and Davidson5 Within the Global Burden of Disease (GBD) framework, ADHD is classified as a non-fatal condition and contributes exclusively to health loss through years lived with disability (YLDs), reflecting its chronic and functionally impairing nature rather than increased mortality. Reference Cortese, Song, Farhat, Yon, Lee and Kim6
ADHD is one of the most prevalent neurodevelopmental disorders among children and adolescents worldwide. Reference Salari, Ghasemi, Abdoli, Rahmani, Shiri and Hashemian7 Large epidemiological studies and systematic reviews have consistently reported that global prevalence estimates for ADHD have remained relatively stable over time. Reference Cortese, Song, Farhat, Yon, Lee and Kim6,Reference Ayano, Yohannes and Abraha8,Reference Johnson, Lim, Jacoby, Faraone, Su and Solmi9 GBD analyses similarly indicate limited temporal variation in age-standardised prevalence and YLD rates. This suggests that changes in burden might be influenced more by population growth and age structure than by shifts in underlying disease risk. Reference Altobaishat, Abouzid, Omari, Sange, Al-zoubi and Bani-salameh10 Well-documented risk factors for ADHD include male gender, genetic predisposition and a range of prenatal, perinatal and early-life environmental exposures. Reference Bitsko, Holbrook, O’Masta, Maher, Cerles and Saadeh11,Reference Schwabe, Jović, Rimfeld, Allegrini and van den Berg12 Although incidence is primarily concentrated in childhood, symptoms frequently persist, resulting in sustained prevalence and disability into adulthood, a pattern consistently reported in global meta-analyses and GBD 2010–2019 publications. Reference Cortese, Song, Farhat, Yon, Lee and Kim6,Reference Erskine, Ferrari, Polanczyk, Moffitt, Murray and Vos13
In the Middle East and North Africa (MENA) region, available evidence suggests that ADHD prevalence and disability burden are broadly comparable to global estimates. Reference Al-Wardat, Etoom, Almhdawi, Hawamdeh and Khader14,Reference Safiri, Mousavi, Nejadghaderi, Noori, Sullman and Amiri15 GBD regional analyses have reported similar age- and gender-specific patterns, with higher prevalence and YLD rates among males and a concentration of burden in paediatric and adolescent age groups. Reference Cortese, Song, Farhat, Yon, Lee and Kim6,Reference Wang, Wang, Qiu, Yu and Wang16 However, both the availability and quality of country-specific epidemiological data across the MENA region remain heterogeneous. Reference Al-Wardat, Etoom, Almhdawi, Hawamdeh and Khader14,Reference Safiri, Mousavi, Nejadghaderi, Noori, Sullman and Amiri15 Due to lack of long-term, nationally representative epidemiological studies in several MENA countries, including Jordan, available estimates rely heavily on the statistical modelling approach used by the GBD framework to synthesise data and fill these data gaps. Existing studies from the region have primarily focused on clinical samples, school-based surveys or short time periods, limiting their generalisability and ability to capture long-term trends and total population burden. Reference Al-Wardat, Etoom, Almhdawi, Hawamdeh and Khader14,Reference Safiri, Mousavi, Nejadghaderi, Noori, Sullman and Amiri15
Jordan is among the MENA group of countries, with an estimated population of 11.44 million people as of 2023. 17 The demographic profile of Jordanians is decidedly young, with a large proportion of residents under 20 years (44.7%) and a significantly smaller proportion over 65 years (3.7%). The working-age population (15–64 years) represented the majority (79.1%) of the population in 2023, 18 indicating a demographic structure dominated by a younger and more economically active age group. 18 According to World Bank Open Data, males in Jordan constituted a slightly higher proportion (51.6%) of the general population than females (48.4%) in 2024. 19 With a younger population and marginally higher male distribution, childhood conditions such as ADHD may be more prevalent, with significant repercussions on individuals, families and healthcare systems in Jordan.
Despite the growing recognition of ADHD as a public health concern in Jordan, the literature lacks a country-specific, comprehensive, population-based assessment of its burden across the life course. No previous study has systematically quantified long-term trends in incidence, prevalence and YLDs attributable to ADHD in Jordan using standardised methods that allow direct comparison with regional and global estimates. Addressing this evidence gap is essential for situating ADHD within national mental health priorities and informing health and education planning. Such data would be vital for researchers and health policy-makers to enable contextual, regional and international comparisons and decision-making. Therefore, the aim of this study was to assess the burden of ADHD in Jordan from 1990 to 2023 using data from the GBD 2023 study, with analyses stratified by age and gender.
Method
Study design and data source
This descriptive study examined the burden of ADHD in Jordan from 1990 to 2023 using estimates from the GBD 2023 Study (GBD 2023). 20 GBD is an international collaborative initiative that began more than 30 years ago. Reference Murray21 It was developed to produce standardised and comparable estimates of disease burden across countries, age groups, gender and time periods by synthesising data from population-based surveys, epidemiological studies, health system records and published literature through advanced statistical modelling approaches. Reference Murray21
Case definition
For epidemiological studies, ADHD is defined in the GBD framework based on diagnostic criteria from the Diagnostic and Statistical Manual of Mental Disorders (DSM) and the International Classification of Diseases (ICD). ADHD is accordingly classified as a non-fatal neurodevelopmental disorder in GBD, and therefore no estimates of mortality or years of life lost are produced. The total burden of ADHD is quantified exclusively through YLDs, reflecting functional impairment rather than premature death.
Measures of disease burden
This study analysed three core epidemiological measures: incidence, prevalence and YLDs. Incidence represents the number of new ADHD cases occurring within a given year, with prevalence reflecting the total number of individuals living with ADHD at a specific point in time. YLDs were calculated in the GBD framework by multiplying prevalence estimates by disability weights that represent the severity of health loss associated with ADHD. These disability weights are derived from large, population-based surveys and are applied consistently across countries to ensure comparability. All measures were extracted as absolute numbers and as rates per 100 000 population, with corresponding 95% uncertainty intervals to capture uncertainty related to data inputs and model assumptions.
Population stratification
ADHD burden estimates were stratified by age and gender. For this analysis, age was categorised into paediatric (2–9 years), adolescent (10–19 years) and adult (20–69 years) groups to reflect key developmental stages, and to align with previous GBD mental disorder analyses. Notably, no estimates (incidence, prevalence or YLDs) were reported by GBD for older adolescents aged 15–19 years. This does not represent a true absence of disease burden (a zero value), but rather reflects specific GBD modelling constraints and assumptions regarding diagnostic thresholds for this specific age cohort. Gender-specific estimates were obtained for males, females and both genders combined, allowing for assessment of gender differences across all age categories.
Data extraction and processing
ADHD-specific data for Jordan were extracted from the GBD 2023 results tool for all available years between 1990 and 2023. Extracted variables included location, year, age group, gender, measure, metric and uncertainty intervals. Data obtained from multiple extraction files were carefully reviewed for consistency, and duplicate entries for overlapping years were identified and removed before analysis to ensure accuracy and completeness of the data-set.
Statistical analysis
Analyses were descriptive in nature and focused on summarising age-specific, gender-specific and temporal patterns of ADHD burden in Jordan. Results are presented using tables reporting rates and absolute numbers with their corresponding uncertainty intervals. No inferential statistical testing was conducted, in accordance with standard practice for GBD-based burden of disease studies.
Results
Incidence, prevalence and YLDs
Paediatric (2–9 years)
Among children aged 2–9 years, ADHD incidence rates were reported for age groups 2–4 years and 5–9 years in both 1990 and 2023. In 1990, incidence rates per 100 000 population for both genders were 279.9 (95% uncertainty interval 186.6–403.7) in children aged 2–4 years and 352.0 (95% uncertainty interval 236.6–503.7) in children aged 5–9 years; corresponding rates in 2023 were 280.3 (186.9–404.3) and 352.3 (236.7–504.0), respectively. Gender-specific incidence rates were reported for both years, with higher estimates observed among males compared with females in each paediatric age group (Table 1).
Incidence, prevalence and years lived with disability (YLDs) of attention-deficit hyperactivity disorder among children aged 2–9 years in Jordan, 1990 and 2023

Table 1 Long description
The table presents data on ADHD incidence rates, prevalence rates, and years lived with disability (YLD) rates among children aged 2-4 years and 5-9 years in Jordan for the years 1990 and 2023. The table has 10 rows and 10 columns. The columns are labeled as Age group (years), Gender, Incidence rate 1990 (95% UI), Incidence rate 2023 (95% UI), Prevalence rate 1990 (95% UI), Prevalence rate 2023 (95% UI), YLD rate 1990 (95% UI), and YLD rate 2023 (95% UI). The rows are labeled with age groups and gender categories. For children aged 2-4 years, the incidence rate for both genders in 1990 was 279.9 (95% uncertainty interval 186.6-403.7) and in 2023 it was 280.3 (95% uncertainty interval 186.9-404.3). For males in the same age group, the incidence rate in 1990 was 433.3 (95% uncertainty interval 286.9-632.2) and in 2023 it was 433.3 (95% uncertainty interval 286.9-632.2). For females, the incidence rate in 1990 was 118.9 (95% uncertainty interval 78.8-179.6) and in 2023 it was 118.9 (95% uncertainty interval 78.8-179.6). For children aged 5-9 years, the incidence rate for both genders in 1990 was 352.0 (95% uncertainty interval 236.6-503.7) and in 2023 it was 352.3 (95% uncertainty interval 236.7-504.0). For males in the same age group, the incidence rate in 1990 was 543.1 (95% uncertainty interval 362.9-773.5) and in 2023 it was 543.1 (95% uncertainty interval 362.9-773.5). For females, the incidence rate in 1990 was 151.8 (95% uncertainty interval 100.9-228.6) and in 2023 it was 151.8 (95% uncertainty interval 100.9-228.6). The table also includes prevalence rates and YLD rates for the same age groups and years, showing similar trends and comparisons.
UI, uncertainty interval.
Prevalence rates among children aged 2–9 years are presented in Table 1. In 1990, prevalence per 100 000 population for both genders was 5089.6 (95% uncertainty interval 3624.6–6815.4) in children aged 2–4 years and 6350.3 (95% uncertainty interval 4545.5–8494.1) in children aged 5–9 years; in 2023, prevalence rates were 5104.9 (3635.3–6834.1) and 6363.1 (4554.4–8507.7), respectively. Gender-stratified estimates showed higher prevalence rates among males than females in both years, and across both paediatric age groups.
YLD rates among children aged 2–9 years are summarised in Table 1. In 1990, YLD rates per 100 000 population for both genders were 214.8 (95% uncertainty interval 128.4–318.0) in the 2–4-year-old group and 262.3 (95% uncertainty interval 157.3–387.4) in the 5–9-year-old group; in 2023, corresponding rates were 215.6 (128.8–319.3) and 262.8 (157.4–387.9). Gender-specific YLD rates were consistently higher among males than females across both paediatric age groups and time points.
Adolescent (10–19 years)
Among adolescents, ADHD incidence estimates were reported for the 10–14-year-old age group, but no estimates were available for individuals aged 15–19 years across both genders in 1990 and 2023. In the 10–14-year-old group, incidence rates per 100 000 population for both genders were 31.1 (95% uncertainty interval 21.0–44.4) in 1990 and 31.1 (95% uncertainty interval 20.9–44.3) in 2023. Gender-specific incidence rates were higher among males than females in both years (Table 2).
Incidence, prevalence and years lived with disability (YLDs) of attention-deficit hyperactivity disorder among adolescents aged 10–19 years in Jordan, 1990 and 2023

Table 2 Long description
The table presents data on the incidence, prevalence, and years lived with disability (YLD) rates of attention-deficit hyperactivity disorder (ADHD) among adolescents aged 10-19 years in Jordan for the years 1990 and 2023. The table has five columns: Gender, Incidence rate 1990 (95% uncertainty interval), Incidence rate 2023 (95% uncertainty interval), Prevalence rate 1990 (95% uncertainty interval), Prevalence rate 2023 (95% uncertainty interval), YLD rate 1990 (95% uncertainty interval), and YLD rate 2023 (95% uncertainty interval). The table includes data for both genders combined, males, and females. Row 1: Gender, Both; Incidence rate 1990, 31.1 (21.0-44.4); Incidence rate 2023, 31.1 (20.9-44.3); Prevalence rate 1990, 525.8 (374.5-702.5); Prevalence rate 2023, 525.0 (374.0-701.4); YLD rate 1990, 21.1 (12.6-31.4); YLD rate 2023, 21.1 (12.4-31.5). Row 2: Gender, Male; Incidence rate 1990, 47.8 (32.0-67.8); Incidence rate 2023, 47.8 (32.0-67.8); Prevalence rate 1990, 790.6 (562.8-1056.3); Prevalence rate 2023, 790.6 (562.8-1056.3); YLD rate 1990, 32.0 (19.1-47.6); YLD rate 2023, 32.0 (19.1-47.6). Row 3: Gender, Female; Incidence rate 1990, 13.5 (8.9-20.3); Incidence rate 2023, 13.5 (8.9-20.3); Prevalence rate 1990, 242.3 (169.4-328.4); Prevalence rate 2023, 242.3 (169.4-328.4); YLD rate 1990, 10.0 (5.8-15.3); YLD rate 2023, 10.0 (5.3-15.6). The data shows that incidence and prevalence rates are higher among males than females in both years.
UI, uncertainty interval.
Prevalence estimates were reported for adolescents aged 10–14 years, with no prevalence estimates for the 15–19-year-old age group in either year. In 1990, prevalence per 100 000 population for both sexes in the 10–14-year-old group was 525.8 (95% uncertainty interval 374.5–702.5) compared with 525.0 (95% uncertainty interval 374.0–701.4) in 2023. Gender-specific prevalence rates were higher among males than females at both time points (Table 2).
YLD rates among adolescents aged 10–14 years are presented in Table 2. In 1990, YLD rates per 100 000 population for both genders were 21.1 (95% uncertainty interval 12.6–31.4), and in 2023 they were 21.1 (95% uncertainty interval 12.4–31.5). Male adolescents exhibited higher YLD rates than females in both years. No YLD estimates were reported for adolescents aged 15–19 years (see Table 2).
Adult (20–69 years)
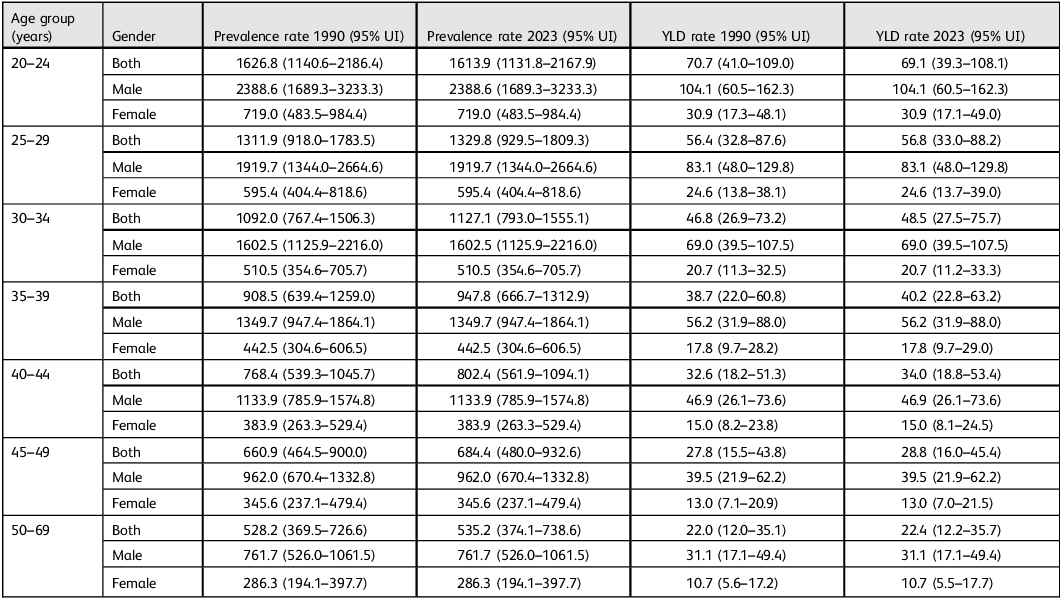
Prevalence estimates for ADHD were available across all adult age groups (20–69 years; Table 3). In 1990, prevalence rates per 100 000 population for both genders were 1626.8 (95% uncertainty interval 1140.6–2186.4) in adults aged 20–24 years and 528.2 (95% uncertainty interval 369.5–726.6) in those aged 50–69 years; in 2023, corresponding prevalence rates were 1613.9 (1131.8–2167.9) and 535.2 (374.1–738.6). Gender-specific prevalence rates were reported for all adult age groups in both years, with higher estimates among males than females.
Prevalence and years lived with disability (YLDs) of attention-deficit hyperactivity disorder among adults aged 20–69 years in Jordan, 1990 and 2023

Table 3 Long description
The table presents data on the prevalence and years lived with disability (YLD) rates of attention-deficit hyperactivity disorder (ADHD) among adults aged 20 to 69 years in Jordan for the years 1990 and 2023. The table is divided into age groups, gender categories, and includes prevalence rates and YLD rates for each group. It has 10 rows and 8 columns. The columns are labeled as Age group (years), Gender, Prevalence rate 1990 (95% uncertainty interval), Prevalence rate 2023 (95% uncertainty interval), YLD rate 1990 (95% uncertainty interval), and YLD rate 2023 (95% uncertainty interval). The age groups range from 20 to 69 years, and the gender categories include both, male, and female. The prevalence rates and YLD rates are provided with their respective 95% uncertainty intervals. Notable trends include higher prevalence rates among males compared to females across all age groups and years. The prevalence rates for both genders show slight variations between 1990 and 2023.
UI, uncertainty interval.
YLD rates among adults aged 20–69 years are shown in Table 3. In 1990, YLD rates per 100 000 population for both genders ranged from 70.7 (95% uncertainty interval 41.0–109.0) in the 20–24-year-old group to 22.0 (95% uncertainty interval 12.0–35.1) in the 50–69-year-old group; in 2023, corresponding rates ranged from 69.1 (39.3–108.1) to 22.4 (12.2–35.7). Gender-specific YLD estimates were reported for all adult age groups in both years (Table 3).
Discussion
This study provides the first comprehensive assessment of the burden of ADHD in Jordan from 1990 to 2023 using GBD 2023 estimates. The results demonstrated that ADHD burden in Jordan is evident across the lifespan, with substantial incidence and prevalence rates among paediatric, adolescent and adult populations. ADHD appeared to be a major non-fatal health loss in Jordan as measured by YLDs.
At the international level, ADHD has been repeatedly recognised as one of the most prevalent neurodevelopmental disorders. In addition, ADHD is a leading contributor to YLDs among children and adolescents. GBD studies consistently report stable age-standardised prevalence and YLD rates for ADHD over time. Reference Cortese, Song, Farhat, Yon, Lee and Kim6,Reference Erskine, Ferrari, Polanczyk, Moffitt, Murray and Vos13 This pattern may be reflecting the chronic nature of the condition rather than changes in disease occurrence. The highest incidence and prevalence observed in Jordan are concentrated in early childhood and decline across adolescence and adulthood.
ADHD incidence is largely confined to childhood in prior global studies, whereas prevalence and YLDs persist into adulthood due to symptom continuation. Reference Ilic and Ilic22,Reference Song, Zha, Yang, Zhang, Li and Rudan23 The absence of adult incidence and the presence of substantial adult prevalence and YLDs in Jordan align well with this global epidemiological profile. These findings confirm that ADHD burden is predominantly driven by long-term functional impairment rather than by new-onset disease in adulthood.
Within the MENA region, previous GBD analyses have reported ADHD prevalence and YLD rates comparable to global averages, with limited variation among countries. Reference Al-Wardat, Etoom, Almhdawi, Hawamdeh and Khader14,Reference Safiri, Mousavi, Nejadghaderi, Noori, Sullman and Amiri15 The age-specific rates observed in Jordan fall within the range reported for neighbouring MENA countries, because these countries have similar demographic and socioeconomic characteristics.
Consistent with regional evidence, males in Jordan exhibit higher incidence, prevalence and YLD rates than females across all paediatric, adolescent and adult age groups. This gender influence has been widely reported in MENA and global studies and is a characteristic feature of ADHD epidemiology within the GBD framework. Reference Cortese, Song, Farhat, Yon, Lee and Kim6,Reference Erskine, Ferrari, Polanczyk, Moffitt, Murray and Vos13 Male gender has been associated with a higher likelihood of ADHD diagnosis. This gender-related difference has arisen from a combination of biological mechanisms and variations in symptom presentation and diagnostic approaches. Males are more likely to present with hyperactive and impulsive symptoms, whereas females often exhibit inattentive symptoms that can be overlooked. Reference Skogli, Teicher, Andersen, Hovik and Øie24 Therefore, the higher prevalence of ADHD among males may present diagnostic bias rather than genuine aetiological disparity, with gender differences diminishing in adulthood. Reference Mestres, Richarte, Crespín, Torrent, Biel and Ramos25
GBD regional estimates suggest that ADHD contributes a meaningful share of total mental and neurodevelopmental YLDs in MENA, particularly among children. The paediatric and adolescent burden observed in Jordan is comparable in magnitude to that reported across the region, supporting the view that ADHD represents a sustained and region-wide source of non-fatal health loss.
The concentration of ADHD burden in children aged 2–9 years and adolescents aged 10–14 years in Jordan is consistent with global diagnostic and modelling patterns used in the GBD study. Reference Cortese, Song, Farhat, Yon, Lee and Kim6 During these early developmental stages, ADHD can jeopardise learning and participation, with potential long-term implications for academic and social functioning. Reference Faraone, Asherson, Banaschewski, Biederman, Buitelaar and Ramos-Quiroga26 Similar age distributions have been reported in high- and middle-income countries alike, suggesting that the observed pattern in Jordan reflects established epidemiological characteristics rather than country-specific anomalies. The absence of estimates among older adolescents aged 15–19 years in Jordan mirrors patterns reported in other GBD-based studies, and reflects modelling assumptions related to symptom persistence and diagnostic thresholds rather than a true absence of ADHD-related impairment.
Adult prevalence and YLD rates in Jordan demonstrate that ADHD-related disability persists well beyond childhood. This finding aligns with a growing global recognition of ADHD as a lifelong condition with sustained functional impact. Comparable adult prevalence and YLD estimates have been reported across MENA and globally, particularly in settings with young population structures such as Jordan; systematic reviews of ADHD prevalence in adults reported a rate between 2.58 and 6.76%. Reference Ayano, Yohannes and Abraha8,Reference Song, Zha, Yang, Zhang, Li and Rudan23 In comparison, the findings of the current study in Jordan indicate lower prevalence estimates among adults, with rates ranging from approximately 0.5 to 1.6% (uncertainty interval 535.2–1626.8 per 100 000) in 2023. The gradual decline in prevalence and YLD rates with increasing adult age observed in Jordan mirrors global trends and reflects the natural history of symptom attenuation over time, rather than complete resolution. Reference Faraone, Asherson, Banaschewski, Biederman, Buitelaar and Ramos-Quiroga26,Reference Lin, Zhai, An, Wu, Qiu and Li27
In the Jordanian context, these findings are particularly relevant given the country’s young population structure. Furthermore, there has been a growing recognition of mental and neurodevelopmental disorders as public health priorities in the country. Untreated ADHD could exclusively contribute to disability rather than mortality, emphasising its impact on educational attainment, productivity and quality of life rather than survival. Reference Danckaerts, Sonuga-Barke, Banaschewski, Buitelaar, Döpfner and Hollis4,Reference Arnold, Hodgkins, Kahle, Madhoo and Kewley28,Reference Jangmo, Kuja-Halkola, Pérez-Vigil, Almqvist, Bulik and D’Onofrio29 Jordan faces similar international challenges including early identification, continuity of care across the life course and addressing long-term functional impairment rather than acute outcomes. Reference Altobaishat, Abouzid, Omari, Sange, Al-zoubi and Bani-salameh10
Although ADHD is primarily characterised by its contribution to disability, particularly YLDs and long-term functional impairment, this highlights the key role of rehabilitation in its management. Rehabilitation approaches, including behavioural therapy, cognitive training and school-based interventions, aim to improve functional outcomes across academic, social and daily life domains. Reference Cheng, Tang, Jin, Li, Hou and Wang30,Reference Peyvandi, Bondi, Cirella, Bressi and Delvecchio31 Multidisciplinary strategies can enhance adaptive skills and participation, particularly when implemented early. Reference Lv, Cheng, Wang, Wang, Hu and Lv32 Therefore, integration of rehabilitation services into health and education systems in Jordan may help reduce the substantial non-fatal burden associated with ADHD. Strengthening the integration of these services within health and education systems in Jordan is essential. Ensuring continuity of care may therefore play a key role in reducing the substantial non-fatal burden associated with ADHD.
Limitations
Several limitations should be considered when interpreting the findings of this study. First, this analysis is based on estimates from the GBD 2023 study, which was founded on statistical modelling to synthesise data from multiple sources of varying quality and availability. Although GBD applies standardised methods to enhance comparability across countries and over time, the accuracy of national estimates for Jordan is partly dependent on the availability of underlying epidemiological data from the region. The incidence, prevalence and YLD rates reported for 1990 and 2023 across all age groups are nearly identical. This is a recognised artefact of the GBD’s model-driven smoothing, which assumes stable underlying disease risk over time for conditions such as ADHD when empirical temporal data are limited. Therefore, these stable rates should be interpreted cautiously as a reflection of modelling assumptions, rather than definitive proof of unchanging incidence or prevalence in the population. Second, incidence estimates for ADHD were not available for adults aged 20–69 years in the GBD framework and, as a result, this study could not assess adult-onset incidence or changes in incident ADHD cases beyond adolescence. The absence of adult incidence data reflects GBD modelling assumptions that ADHD onset occurs primarily in childhood and therefore limits the ability to examine potential late- or adult-diagnosed cases within the population. Third, estimates for older adolescents aged 15–19 years were not reported for incidence, prevalence or YLDs, which restricts the assessment of ADHD burden across the full adolescent age spectrum. This limitation is consistent with previous GBD mental disorder analyses, Reference Cortese, Song, Farhat, Yon, Lee and Kim6 and reflects modelling constraints rather than a true absence of disease burden. Finally, the use of aggregate, population-level data precluded analyses by clinical severity, comorbidity, socioeconomic status or access to care. Consequently, the results describe overall burden patterns but do not capture within-country heterogeneity or individual-level determinants of ADHD-related disability in Jordan. Despite these limitations, the use of GBD data provides a robust and standardised framework for evaluating long-term trends and enables meaningful comparison of ADHD burden in Jordan with regional and global estimates.
Conclusion
This study provides the first comprehensive, population-based assessment of the burden of ADHD in Jordan from 1990 to 2023 using GBD 2023 estimates. ADHD in Jordan is characterised exclusively by non-fatal health loss, with burden expressed through prevalence and YLDs across paediatric, adolescent and adult populations. The burden is most pronounced in early childhood and early adolescence, whereas prevalence and disability persist into adulthood without evidence of incident adult-onset disease. These age- and gender-specific patterns align closely with regional and global GBD estimates, indicating that Jordan’s ADHD burden follows established international epidemiological profiles. Overall, ADHD represents a sustained source of disability across the life course in Jordan, with implications for health systems, education and long-term functional outcomes.
Data availability
The data that support the findings of this study are publicly available from the Global Burden of Disease (GBD) Results Tool provided by the Institute for Health Metrics and Evaluation (https://ghdx.healthdata.org/gbd-results-tool). No new primary data were created in this study.
Acknowledgements
We thank the Institute for Health Metrics and Evaluation staff and its collaborators, who prepared these publicly available data. The authors are grateful to the Deanship of Research and Graduate Studies, Jordan University of Science and Technology.
Author contributions
All authors meet the International Committee of Medical Journal Editors criteria for authorship. M.A.-W. and Y.K. conceptualised the study. M.A.-W., A.J., N.I. and H.A. contributed to the study design and data extraction. M.A.-W. and Y.K. performed the data analysis and interpretation. K.A.A., A.O.O. and O.A. contributed to the interpretation of findings and critically revised the manuscript. M.A.-W. drafted the manuscript, and all authors critically reviewed, revised and approved the final version.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.
Ethical standards
This study is based on secondary analysis of publicly available, de-identified data from the GBD study conducted by the Institute for Health Metrics and Evaluation. Because no individual-level identifiable human participant data were used, ethical approval was therefore not required, in accordance with institutional and national research guidelines. The authors assert that all procedures contributing to this work comply with the ethical standards of relevant national and institutional committees on human experimentation, and with the Helsinki Declaration of 1975 as revised in 2013.
Transparency declaration
The lead author (M.A.-W.) affirms that this manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
Consent statement
Patient consent for publication was not required. This study used publicly available, fully anonymised and de-identified secondary data from the GBD study. No individual-level identifiable human participant data were accessed or included.
Analytic code availability
The analytic code used to generate the results of this study is available from the corresponding author (M.A.-W.) upon reasonable request.



 Open access
Open access
eLetters
No eLetters have been published for this article.