



Impact statement
This systematic review offers a comprehensive synthesis of youth mental health interventions targeting individuals aged 15 to 24 across a broad range of global contexts. The heterogeneity observed in intervention types, delivery modes, study settings and outcome measures reflects the diverse mental health needs of youth, as well as the varying service capacities and cultural understandings of mental health across regions. Rather than being a constraint, this variability underscores the need for flexible, context-sensitive approaches that can address both local and cross-cultural priorities.
This review highlights the co-existence of disorder-specific and transdiagnostic intervention strategies, with some studies focusing on clinical symptoms such as anxiety and depression, while others targeted broader constructs like emotional regulation and self-efficacy. This diversity points to the value of integrating diagnostic and transdiagnostic approaches to address the full spectrum of youth mental health concerns. Additionally, the wide range of measurement tools used, while introducing heterogeneity, reflects differing priorities in research focus, cultural relevance and levels of care, spanning prevention to treatment. These findings reinforce the importance of using standardised, culturally validated instruments to ensure both precision in assessment and comparability across studies.
Importantly, this review identifies gaps in the transparent reporting of cultural adaptations and implementation processes, which limits the field’s ability to distinguish between meaningful contextual tailoring and methodological inconsistencies. Addressing this gap is essential for improving the transferability and scalability of interventions across diverse settings. By mapping out current practices and limitations, this review provides a critical foundation for advancing equitable and culturally relevant youth mental health interventions. It emphasises the need for inclusive research designs, longitudinal evaluations and clearer reporting practices to support the development of responsive mental health strategies that can effectively meet the evolving needs of young people worldwide.
Background
According to the World Health Organization (WHO, 2019), the term ‘youth’ refers to individuals aged 15 to 24 years. This age bracket, encompassing adolescence and young adulthood, signifies critical periods in human growth and maturation, marked by significant changes in physical, cognitive, emotional and social aspects (Backes and Bonnie, Reference Backes and Bonnie2019). These transitions involve achieving milestones such as completing formal education, entering the workforce, exploring personal identity, forming intimate relationships and assuming greater responsibilities within society (Newcomb, Reference Newcomb1996; Gale & Fahey, Reference Gale and Fahey2005). While these developmental milestones offer opportunities for growth and self-discovery, they also pose unique challenges and stressors that can impact mental health and well-being.
The vulnerability of this age group to mental health disorders is underscored by several factors, as highlighted in a recent report by the United Nations Children’s Fund (UNICEF, 2021). Adolescence involves profound neurological transitions affecting social perception, cognition and executive functions. These changes, coupled with the onset of puberty, can acutely affect mental health. Early onset of puberty, in particular, is associated with increased risks of anxiety, depression, eating disorders and antisocial behaviours. As young people transition into new social roles, they face greater exposure to social determinants that can impact mental health, including poverty, conflict, gender norms and labour market pressures.
Global statistics reveal a concerning prevalence of mental health disorders in this age group. UNICEF’s The Changing Childhood Project (2021) provides compelling evidence of the mental health challenges faced by today’s youth. Based on a survey of 20,000 people across 21 countries of various income groups (UNICEF, 2021), 36% of young people aged 15 to 24) report often feeling anxious, worried or nervous, and 19% say they often feel depressed or have little interest in doing things. These findings are further corroborated by other studies. Statistics from the National Alliance on Mental Illness (Cohen, Reference Cohen2022) indicate that nearly 20% of high school students report serious thoughts of suicide, with 9% having attempted to take their own lives. Moreover, various mental health challenges are prevalent during this developmental stage, including suicidal ideation and anxiety (Biswas et al., Reference Biswas, Scott, Munir, Renzaho, Rawal, Baxter and Mamun2020), self-harm behaviours (Madge et al., Reference Madge, Hewitt, Hawton, Wilde, Corcoran, Fekete, Van Heeringen, De Leo and Ystgaard2008), substance use disorders (Pearson et al., Reference Pearson, Janz and Ali2013) and eating disorders (Hoang et al., Reference Hoang, Goldacre and James2014). The complexity of youth mental health is further compounded by the concern of untreated mental health conditions during the critical developmental stage. Such untreated conditions can exert profound and enduring effects, echoing throughout individuals’ lives, impacting families and imposing societal burdens. The resultant treatment gap not only perpetuates individual suffering but also imposes a collective burden on families and society at large (Bhardwaj & Bhardwaj, Reference Bhardwaj and Bhardwaj2015).
The literature highlights the pressing need for effective mental health interventions tailored to address the diverse needs of young individuals in this age group. Given this context, it is both timely and important to conduct a systematic review of worldwide mental health interventions for youths to explore the current landscape. To ensure consistency, this review adopted the age range by WHO (2019), which defines youth as individuals aged 15 to 24 years. The main aim was to identify interventions that evaluate a range of mental health issues, including those meeting diagnostic criteria for clinical disorders according to the Diagnostic and Statistical Manual of Mental Disorders (DSM; American Psychiatric Association, 2013), as well as those using a transdiagnostic approach that considers subthreshold symptoms and overall well-being (Teng et al., Reference Teng, Venning, Winefield and Crabb2015, as cited in Kist et al., Reference Kist, Vrijsen, Mulders, Van Eijndhoven, Tendolkar and Collard2023). By synthesising data from a broad range of studies conducted worldwide for this specific age group, this review sought to advance our understanding of effective strategies for promoting mental well-being and addressing mental health challenges among youths on a global scale. This comprehensive approach aimed not only to contribute to the existing body of knowledge but also to inform the development of more targeted and effective interventions for this crucial demographic.
Methods
Search strategy
A systematic search was conducted across multiple electronic scientific databases on November 1, 2023, including PubMed, Scopus, Academic Search Complete, APA PsycInfo, CINAHL Complete, APA PsycArticles, ProQuest Dissertations & Theses Global and Cochrane. The search strategy employed a Boolean phrase applied to the title, abstract and keywords of articles, encompassing terms related to adolescents, teenagers, young people, young adults and youth, in conjunction with mental health concepts such as mental health, mental disorder, mental well-being, psychological well-being and mental wellness, as well as intervention-related terms such as program, prevention and promotion. The objective of this search was to identify English-language articles on mental health interventions targeting individuals aged 15 to 24 years, without time and geographical restrictions.
Data extraction and analysis
The data extraction and analysis adhered to the latest Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guideline (Page et al., Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann, Mulrow, Shamseer, Tetzlaff, Akl, Brennan, Chou, Glanville, Grimshaw, Hróbjartsson, Lalu, Li, Loder, Mayo-Wilson, McDonald and McGuinness2021). Employing the Population, Intervention, Comparator, Outcome, and Study design (PICOS) framework, the following inclusion criteria were applied: Participants (P): The study population comprised youth aged between 15 and 24 years. Intervention (I): Any form of mental health intervention where mental health issues were considered. Comparator (C): Not applicable as inclusion criteria encompassed a range of study designs. Outcome Measures (O): Any clinical outcome measures were considered. Study Design (S): Included randomised controlled trials (RCTs), waitlist-controlled trials and single-arm quasi-experimental studies deemed applicable.
Only outcomes directly related to the evaluation of mental health issues were included in this review. In studies where no ‘primary outcome’ was explicitly stated, any clinical outcome measures related to the evaluation of mental health issues were considered primary outcomes by default, unless otherwise specified. For instance, measures such as emotion regulation, symptoms of depression, distress tolerance and impulsivity (Russell et al., Reference Russell, Hutchison and Fusco2019), as well as anger and violence tendency (Akbaş & Yiğitoğlu, Reference Akbaş and Yiğitoğlu2022), were included as primary outcomes in relevant studies.
This review applied two main exclusion criteria. First, studies involving participants with comorbid physical conditions or disorders that could potentially confound mental health issues were excluded. These conditions encompassed chronic medical illnesses such as diabetes, epilepsy and cancer; neurological disorders like traumatic brain injury; severe physical disabilities; intellectual disabilities; and severe sensory impairments such as blindness or deafness. This exclusion criterion, adapted from Lee and Yap (Reference Lee and Yap2024) was implemented to preserve the internal validity of the findings by minimising confounding factors and reducing heterogeneity to the greatest extent possible. This approach aimed to improve the generalisability of the results to the broader population, while acknowledging the limitations posed by these exclusions, and recognising the need for separate research to address the distinct challenges and complexities faced by individuals under these excluded categories. Second, articles with fewer than three participants were excluded to mitigate potential selection bias and avoid over-pathologising the results (Yap et al., Reference Yap, Azmin, Che Hamzah, Ahmad, van de Warrenburg and Mohamed Ibrahim2022; Wong et al., Reference Wong, Ng, Lee, Yeow, Lim and Yap2024).
Two independent reviewers (M.H.L. and K.H.Y.) performed the initial screening of titles and abstracts to identify potentially relevant studies. Full-text articles were obtained for further evaluation if they met the initial inclusion criteria or if there was uncertainty regarding their eligibility. Any discrepancies or disagreements between the reviewers were resolved through discussion. Key data were extracted and tabulated (refer to the Supplementary Table), including study characteristics such as first author, year, intervention approach, country, target population, study design, setting, sample size, clinical characteristics, primary outcome, type of intervention, clinical outcomes and main findings.
To categorise the target populations, a four-tiered classification system was developed. The General Youth group comprised young people not experiencing significant psychosocial or structural challenges. The Vulnerable Youth group included individuals exposed to adverse circumstances that potentially compromised their well-being. The Youth at Risk category encompassed individuals exhibiting behaviours or psychosocial challenges that increase the likelihood of developing mental health issues. Lastly, the Youth with Diagnosis group consisted of individuals with formally diagnosed mental health or behavioural conditions requiring clinical management. This tiered approach aligns with emerging models advocating for multidisciplinary care frameworks in youth mental health (Colizzi et al., Reference Colizzi, Lasalvia and Ruggeri2020), which emphasises early intervention and the need for flexible, context-sensitive support systems.
Similarly, settings were categorised as educational, community, healthcare or general population based on the primary context in which the intervention was delivered, with classification confirmed through team discussion to maintain consistency. Primary outcome categories were also classified into mental health symptoms, mental well-being or both, following definitions established prior to data extraction and refined iteratively. These definitions were developed and refined through iterative team discussions during the data extraction phase. Where classification was unclear, final categorisation was reached by consensus among the research team. This approach enabled a structured synthesis while acknowledging the complexity and fluidity of youth mental health experiences, facilitating a nuanced understanding of intervention focus across studies. These systematic categorisations aimed to capture a broad spectrum of youth mental health contexts and outcomes, enhancing the generalisability and applicability of the findings.
Methodological quality
The risk of bias was assessed using Covidence’s quality assessment tool, with evaluations categorised as high, low or unclear across five domains: (1) bias due to sequence generation, (2) bias due to allocation concealment, (3) bias arising from blinding of participants and personnel, (4) bias in the blinding of outcome assessment and (5) bias due to incomplete outcome data. Furthermore, the levels of evidence were determined following the guidelines outlined by the National Health and Medical Research Council (NHMRC, 2009). These range from Level I (systematic reviews of Level II studies) to Level IV (case series with post-test or pre-test/post-test outcomes). This current review focused on original studies, excluding reviews and case series. Consequently, only studies classified as Level II (RCTs), Level III-1 (pseudo-RCTs), Level III-2 (comparative studies with concurrent control) and Level III-3 (comparative studies without concurrent controls) were included in the analysis.
Results
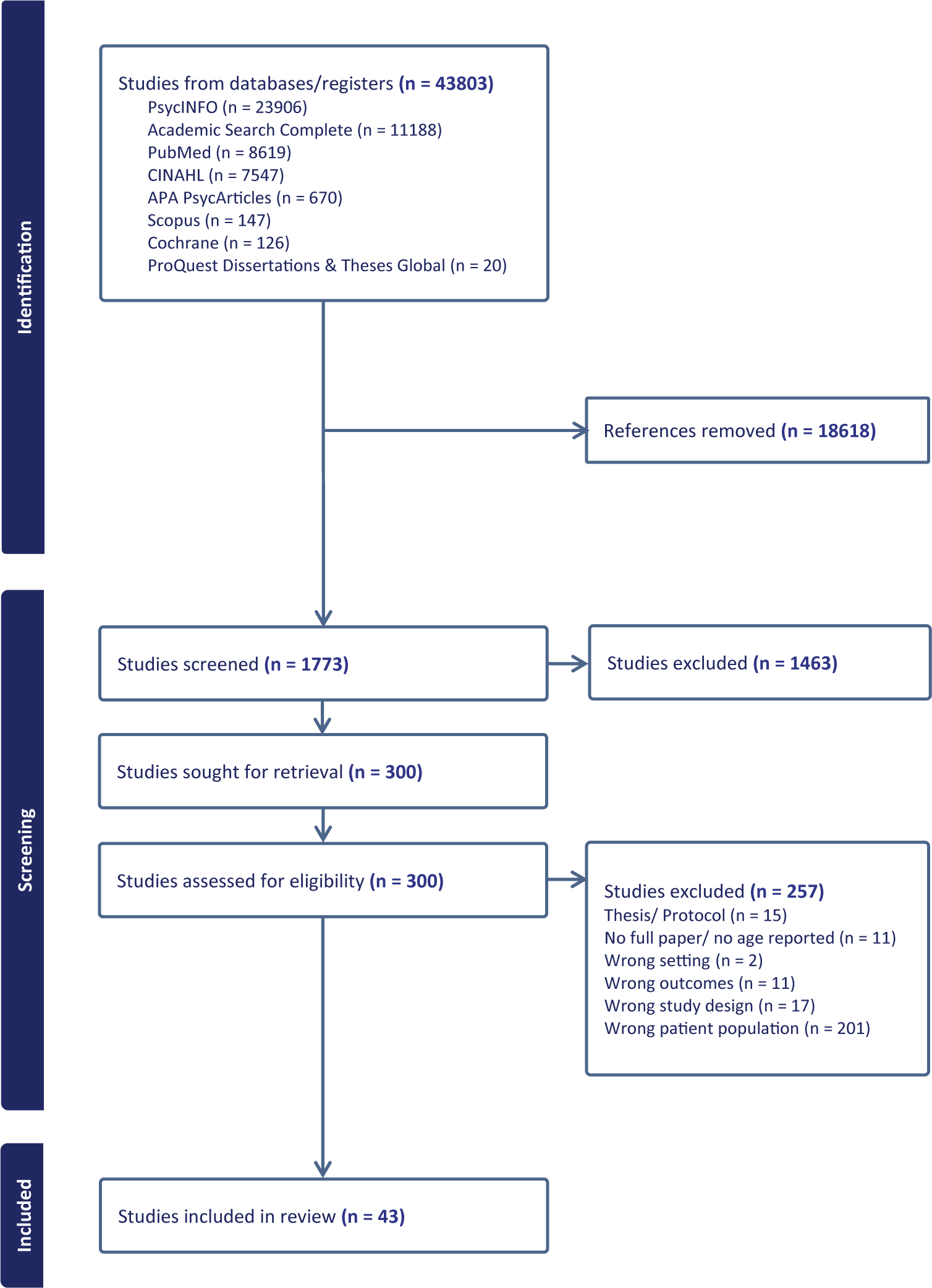
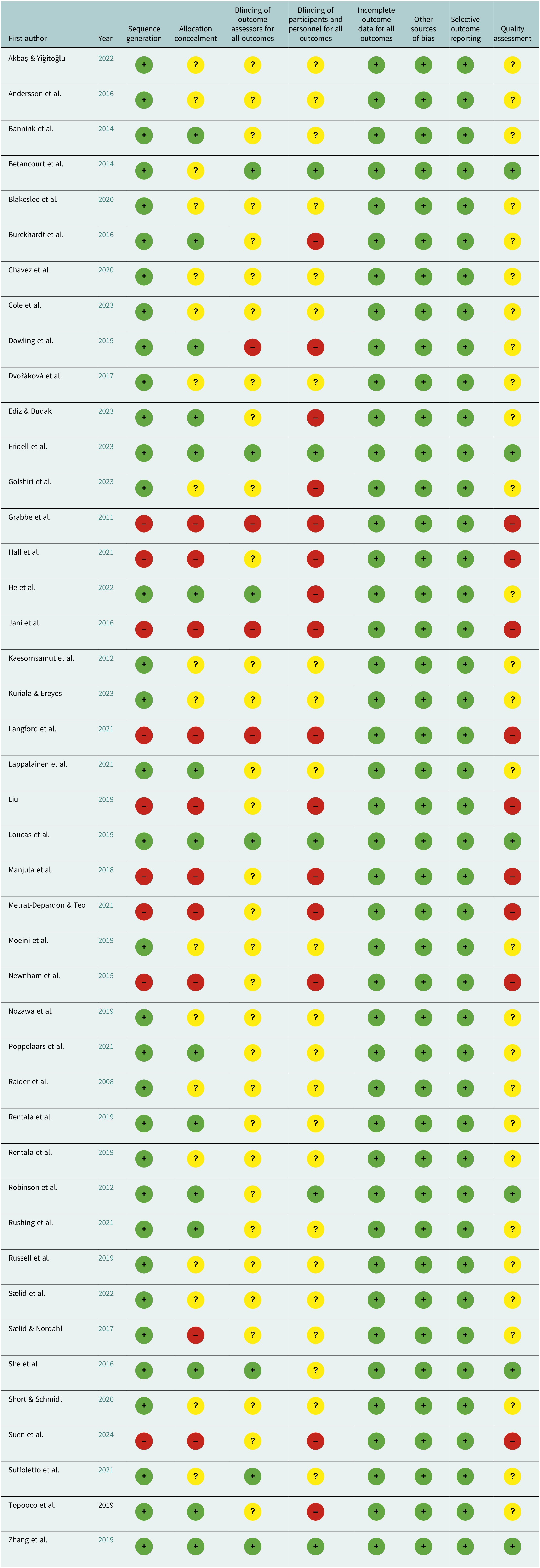
Of 43,803 references initially identified, 43 studies were included in the final analysis. All studies adhered strictly to an intention-to-treat analysis protocol. The current review’s PRISMA flowchart is shown in Figure 1. An overview of the risk of bias and quality assessment was presented in Table 1. Of the 43 studies, 6 were rated as low risk of bias and high quality. Twenty-eight studies were rated as having unclear, indeterminable, not applicable or unreported risk of bias, while nine studies were assessed as high risk of bias and low quality. The level of evidence for the included studies, based on the NHMRC hierarchy, was summarised in the Supplementary Table. Thirty-three studies were classified as Level II evidence, one study as Level III-1, two studies as Level III-2 and seven studies as Level III-3.
PRISMA flowchart.

Risk of bias assessment

Note: The risk of bias of the included studies was assessed using Covidence’s quality assessment tool. Green circle: low risk; yellow circle: unclear, cannot determine, not applicable, or not reported; red circle: high risk.
Study characteristics
A total of 29,581 participants were included across the 43 studies reviewed, with individual study sample sizes ranging from 18 to 20,665 participants, spanning from 2008 to 2023. Study designs varied, with the majority (29 out of 43) adopting an RCT methodology, and an additional four studies used a cluster RCT design. Three studies employed a quasi-experimental design with control groups, and seven without control groups.
Countries and modes of interventions
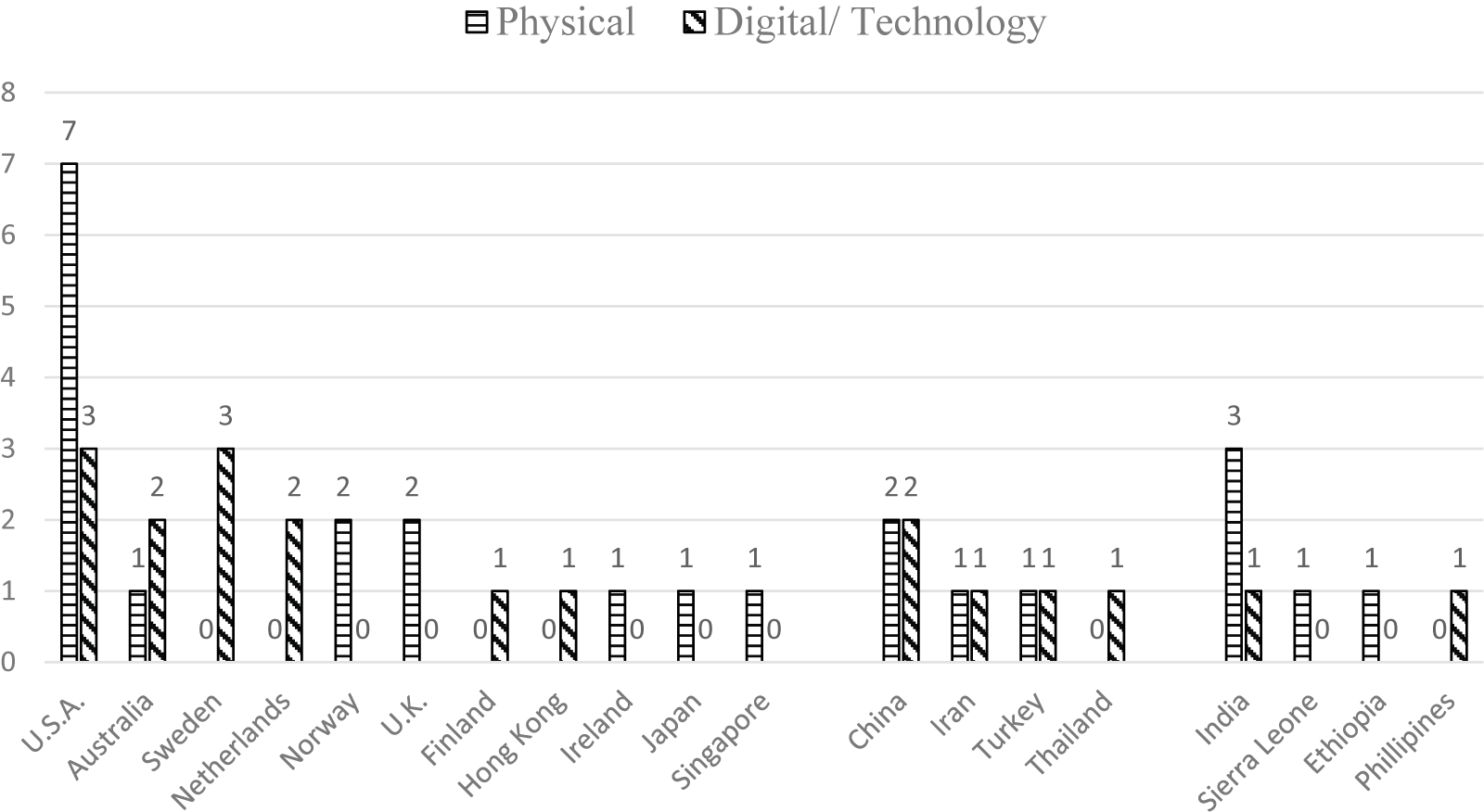
The countries of the published studies were categorised into three broad groups based on The World Bank’s classification of economies by gross national income per capita: high-income, upper-middle-income, and low- and lower-middle-income countries. The majority of the studies (27 out of 43) were conducted in high-income countries, which included the United States, Australia, Sweden, the Netherlands, Norway, the United Kingdom, Finland, Hong Kong, Ireland, Japan and Singapore. The remaining studies were distributed almost equally between upper-middle-income countries (nine studies) and low- and lower-middle-income countries (seven studies). The upper-middle-income countries included China, Iran, Turkey and Thailand, while low- and lower-middle-income countries included India, Sierra Leone, Ethiopia and the Philippines.
To further understand the nature of these interventions, the studies were categorised based on the mode of intervention, referring to the logistical format through which interventions were delivered; either physical or digital/technology-based. This categorisation aimed to explore how mental health interventions were conducted across different countries and to identify potential patterns in the delivery methods. The distribution of studies based on countries and mode of intervention is illustrated in Figure 2.
Distribution based on countries and modes of intervention.

Intervention settings
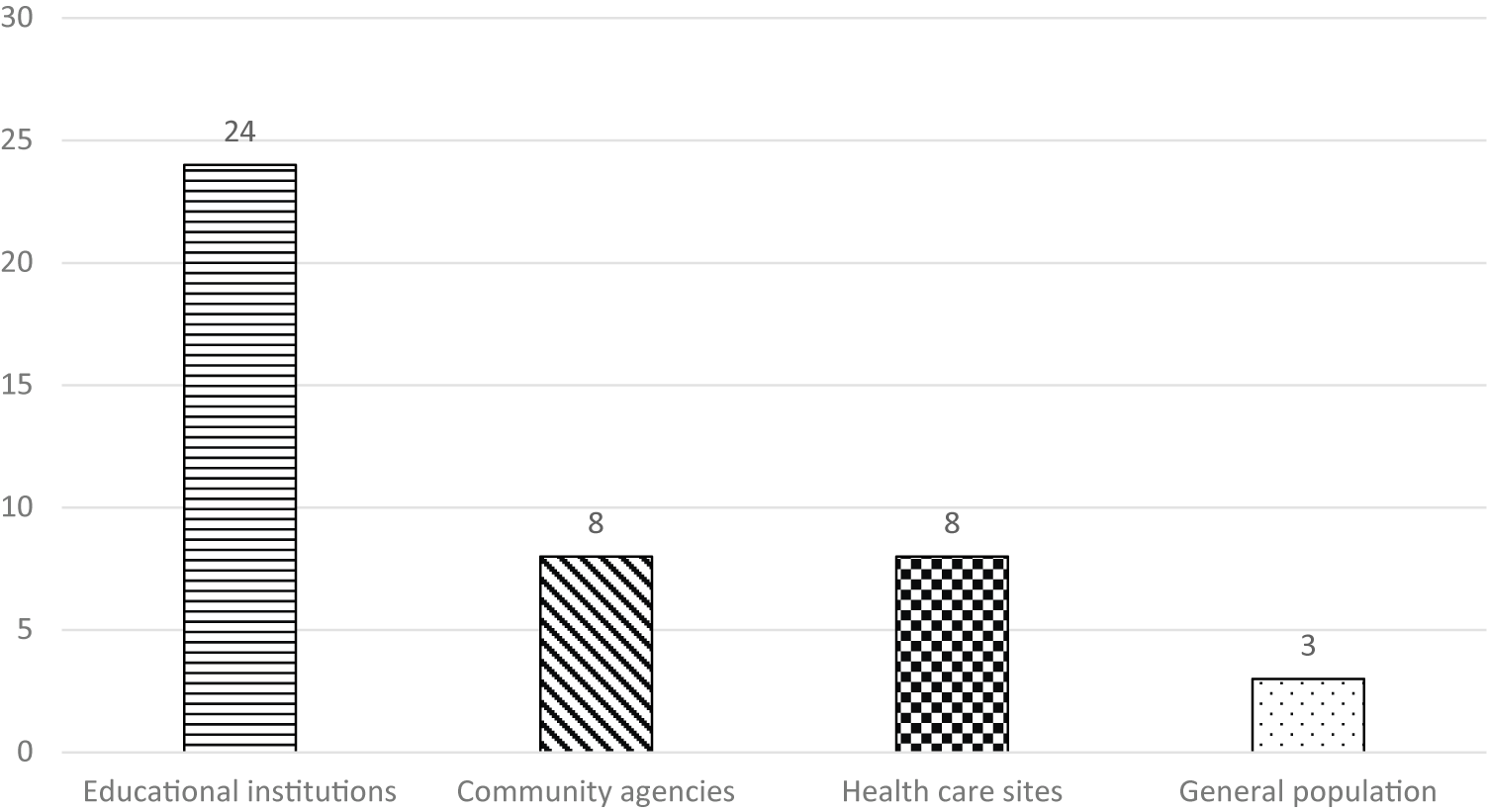
The settings in which interventions were implemented, as illustrated in Figure 3, were categorised into four key domains: educational institutions, community agencies, healthcare sites and general population platforms. The majority of interventions were delivered in educational institutions, including secondary schools, high schools, colleges, universities and vocational training centres. This was followed by interventions delivered through community agencies and healthcare sites, which frequently served as referral-based platforms for youth identified as needing further support. The least common setting was general population platforms, such as social media and digital websites. This trend suggested a predominant reliance on school-based settings for mental health interventions, with community and healthcare settings supporting more targeted efforts, and digital platforms playing a more supplementary role.
Distribution based on settings.

Modalities of interventions
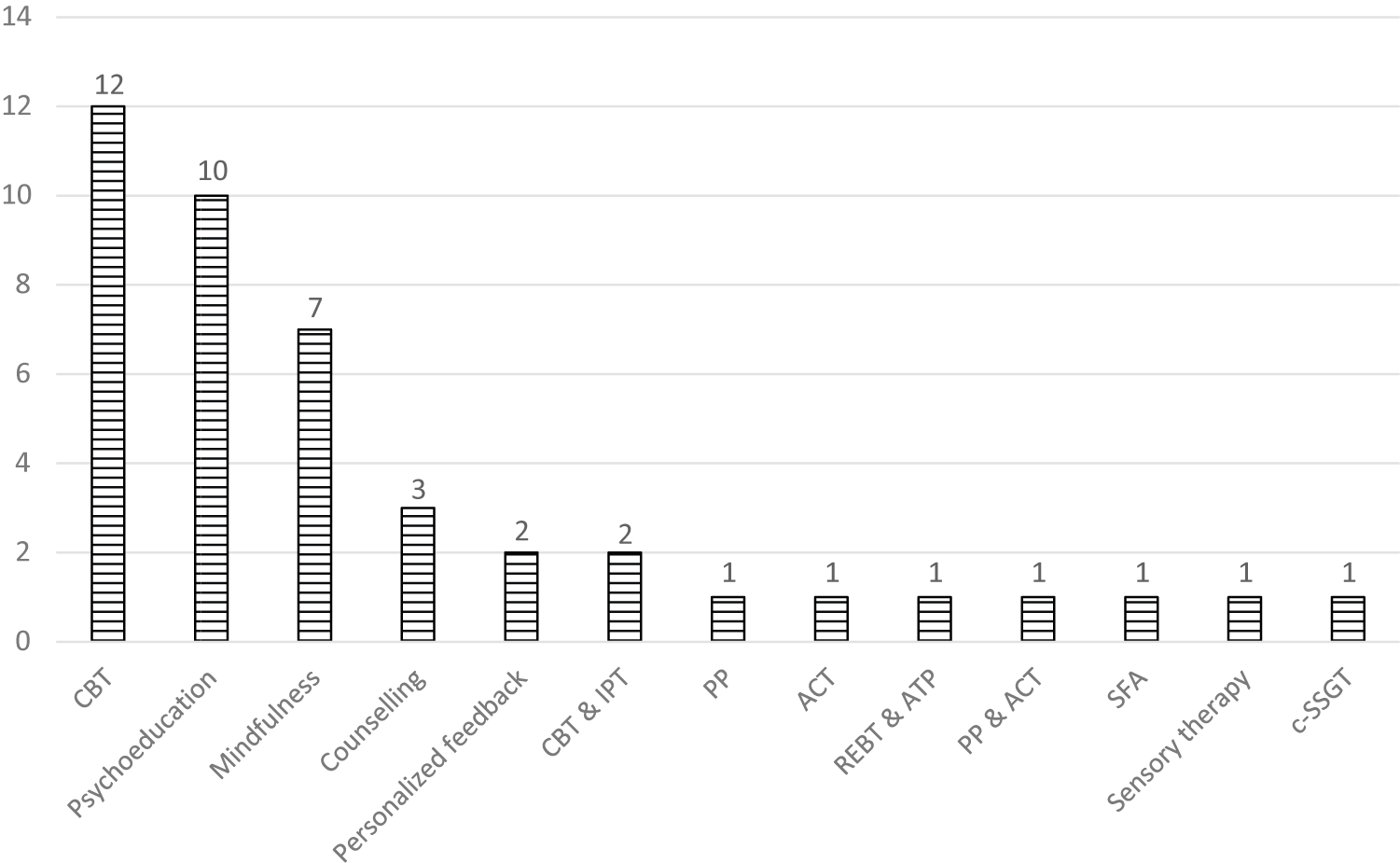
The included studies were further categorised based on their intervention modalities, referring to the therapeutic approaches employed. Cognitive behavioural therapy (CBT) was the most frequently examined modality, featured in 12 studies. Psychoeducation followed closely, appearing in ten studies, while mindfulness-based interventions were reported in seven studies. Counselling was used in three studies. Personalised feedback and the integration of cognitive behavioural therapy (CBT) with interpersonal therapy were observed in two studies. Less commonly used modalities included positive psychology (PP), acceptance and commitment therapy (ACT) and combined interventions such as rational emotive behaviour therapy with affect and problem-solving therapy, as well as PP with ACT. Additionally, the solution-focused approach, sensory therapy and group-based social skills training were each represented by a single study. An overview of this distribution was presented in Figure 4.
Distribution based on modalities on interventions.

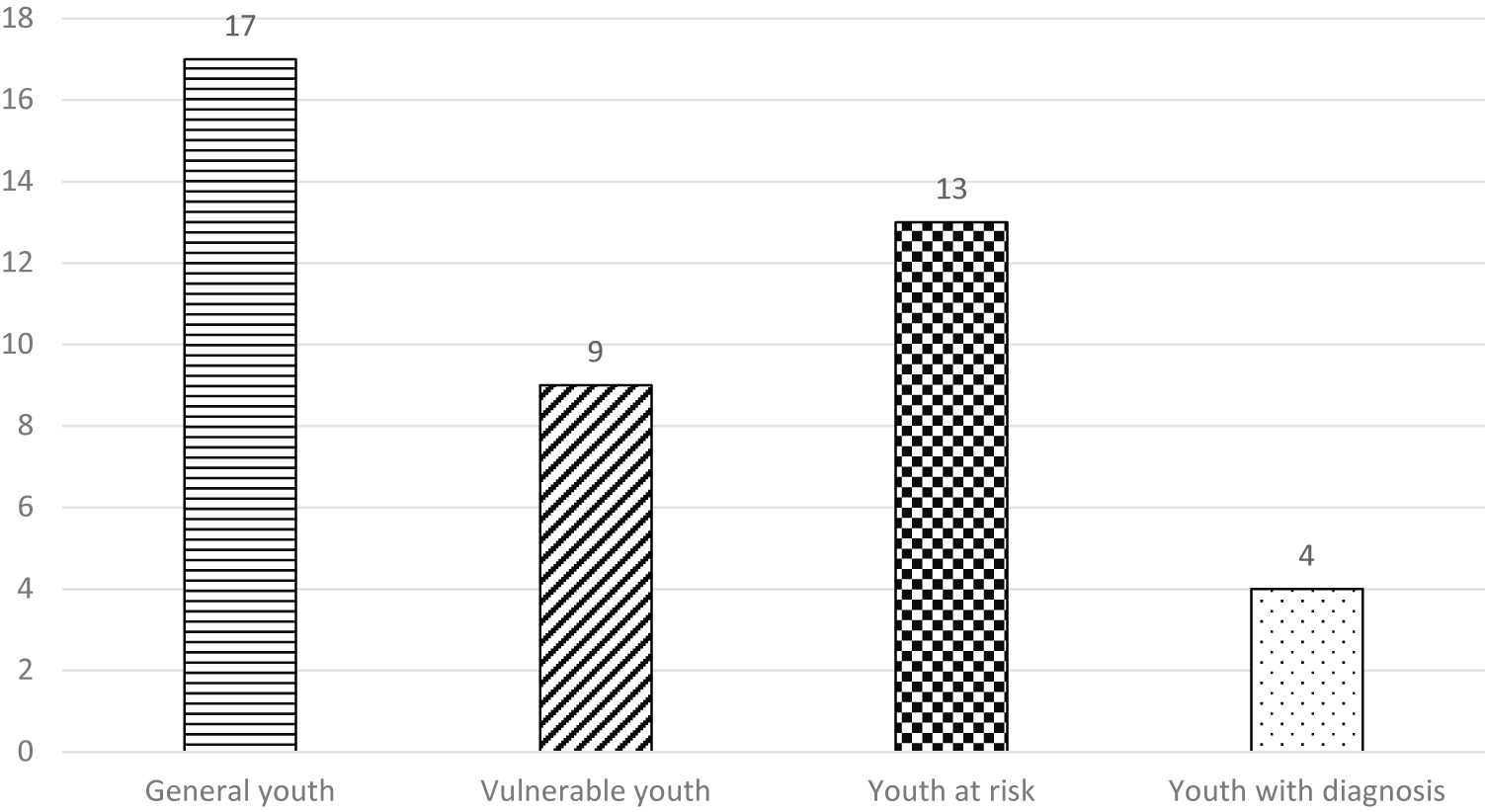
Intervention target groups
The distribution of intervention target groups, as illustrated in Figure 5, was categorised into four primary youth populations to reflect the spectrum of mental health needs. First, the General Youth group (17 studies) comprised those not currently experiencing significant psychosocial challenges. Second, the Vulnerable Youth group (nine studies) included individuals exposed to war, placed in foster care, experiencing homelessness, early pregnancy or migration, as well as those subjected to stigma, prejudice or discrimination. Third, the Youth at Risk category (13 studies) encompassed individuals with issues including anger and violent tendencies, substance use, social communication and interaction difficulties, anxiety, trauma, suicidal ideation or behaviours and other subthreshold presentations such as symptoms of internet gaming disorder and depression. Lastly, the Youth with Diagnosis group (four studies) consisted of those formally diagnosed with substance use disorders, schizophrenia and other psychiatric diagnoses requiring clinical management.
Distribution based on target populations.

Primary outcomes of interventions
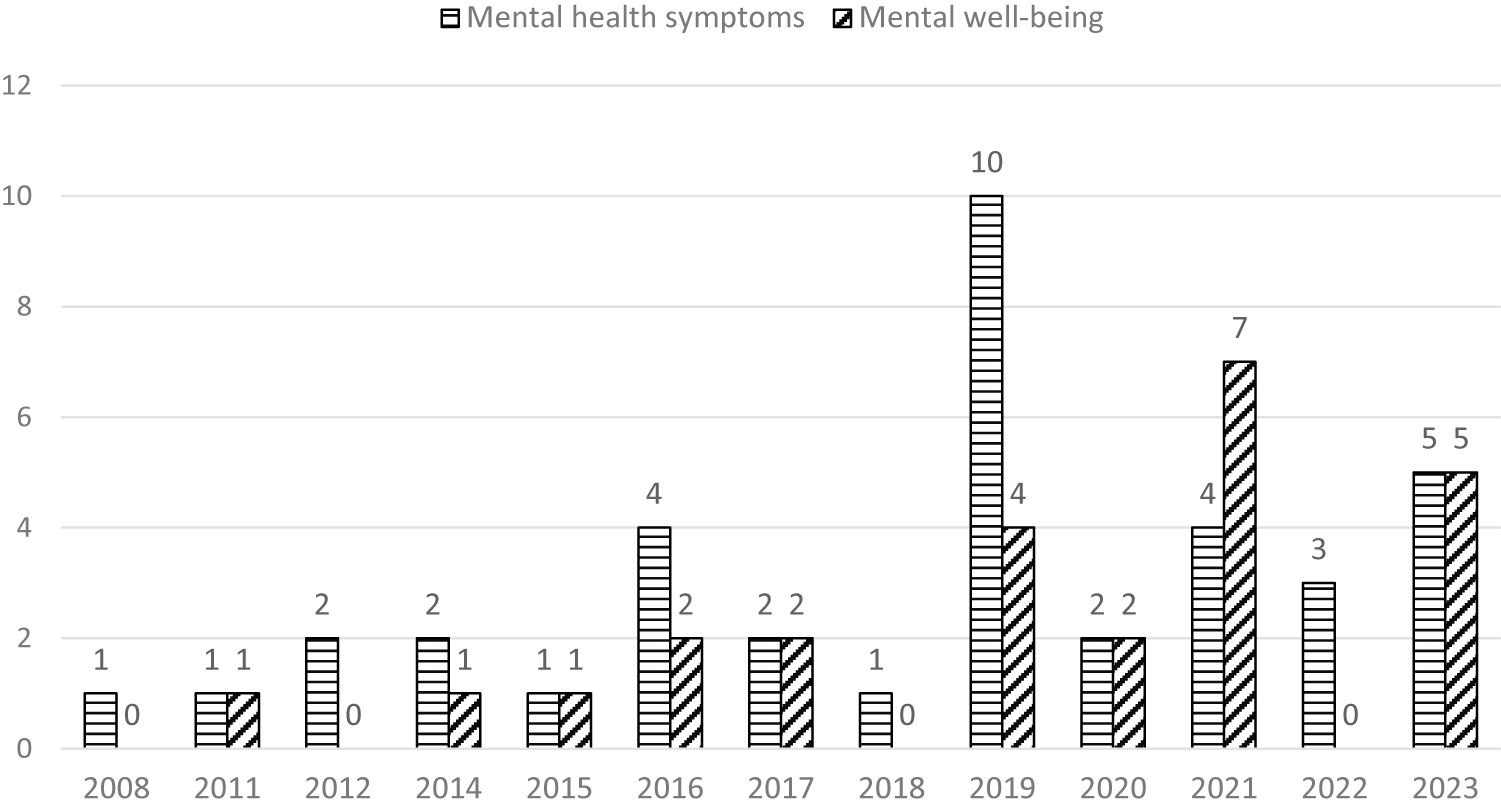
Across the 43 included studies, a wide range of primary outcomes were reported. For clarity and conceptual coherence, these outcomes were grouped into two overarching categories: mental health symptoms and mental well-being. The first category, mental health symptoms, was the most frequently reported, featured in 38 of the 43 interventions. This category encompassed clinical markers of psychological distress, including depression, anxiety, posttraumatic stress, suicidal ideation and behaviour, deliberate self-harm, substance use, obsessive–compulsive symptoms and physiological stress responses. These outcomes primarily reflected the presence, severity or reduction of diagnosable mental health conditions. The second category, mental well-being, conceptualised through the transdiagnostic lens, was reported in 25 of the 43 interventions. Outcomes under this category included emotional regulation, daily or adaptive functioning, perceived social support, psychological flexibility, self-efficacy, self-congruence, sleep quality, self-compassion, personal recovery and help-seeking attitudes or behaviours. These attributes focused on psychological qualities that support resilience, functioning and adaptation across a range of mental health challenges, encompassing broader factors than disorder-specific outcomes.
A temporal review of publication years revealed that interest in youth mental health interventions has grown steadily over the past decade. From 2008 to 2018, the number of studies published annually ranged from one to four. However, in 2019 alone, ten studies were published reporting on symptoms and four on well-being – more than double the average of preceding years. This heightened trend persisted into 2021 (four on symptoms and seven on well-being) and 2023 (five on symptoms and five on well-being), reflecting sustained interest in youth-focused mental health outcomes in the current decade. An overview of this categorisation was presented in Figure 6.
Distribution based on primary outcomes from 2008 to 2023.

Discussion
Heterogeneity among modes of interventions
The findings revealed distinct heterogeneity in the modes of intervention delivery, namely physical and digital/technology-based approaches. Digital/ technology-based interventions were noted to be prominent in high-income countries, with 12 interventions reported, compared to five in upper-middle-income countries and two in low- and lower-middle-income countries. This disparity underscored the reliance of such interventions on robust technological infrastructure, such as widespread internet connectivity (WHO, 2022), high smartphone penetration rates (International Telecommunication Union, 2023) and the availability of advanced technological resources (Chakrabarti, Reference Chakrabarti2024), which are more prevalent in high-income settings.
Digital/ technology-based interventions resonate with youth due to their interactive and engaging nature (Ferretti et al., Reference Ferretti, Hubbs and Vayena2023). In contrast, the minimal presence of digital interventions in low- and lower-middle-income countries highlighted significant barriers, including limited access to digital technology, high costs associated with devices and data and infrastructural challenges (WHO, 2020). More physical interventions, by contrast, were used in low- and lower-middle-income countries. These findings emphasised the continued importance of physical approaches in regions where technological barriers restrict the feasibility of digital solutions. As such, physical interventions may offer greater adaptability and cultural appropriateness to local contexts, considering their non-reliance on technological infrastructure.
The disparities in intervention types highlighted the importance to understand that digital health should not be regarded as a panacea, which calls for balanced and context-sensitive approaches to mental health improvement. Each modality holds distinct value and should complement, not replace, the other. While digital interventions can offer scalability, accessibility and cost-effectiveness particularly in reaching remote or underserved populations (Schueller et al., Reference Schueller, Hunter, Figueroa and Aguilera2019), physical interventions offer personal interaction, immediate feedback, and may be more suitable for complex cases or in contexts where digital literacy is low. This diversity also suggested the potential for integrating digital tools with physical approaches to optimise intervention effectiveness, particularly in transitional settings (WHO, 2020). For instance, while physical interventions may serve as the primary mode in low-income countries, the gradual incorporation of digital elements could extend reach and scalability as technological infrastructure evolves. This hybrid approach could leverage the strengths of both physical and digital interventions, potentially overcoming the limitations of each when used in isolation (Nahum-Shani et al., Reference Nahum-Shani, Dziak, Walton and Dempsey2022), accommodating diverse needs and settings, as well as ensuring equitable access to mental health care.
Heterogeneity among intervention modalities and settings
This review also revealed a notable trend in the intervention modalities for youth aged 15 to 24, with CBT, psychoeducation and mindfulness-based interventions emerging as the most prominently used approaches compared to other modalities. This could potentially suggest that CBT’s structured nature and emphasis on skill-building (Nelson & Tusaie, Reference Nelson and Tusaie2011), psychoeducation’s emphasis on provision of both disease-specific information (e.g., recognition and management of disorders) and general information (e.g., promotion of optimal well-being) (Bjørnsen et al., Reference Bjørnsen, Eilertsen, Ringdal, Espnes and Moksnes2017), and mindfulness’ key feature of paying attention to the events occurring within one’s mind and body (Napoli et al., Reference Napoli, Krech and Holley2005) align well with the developmental needs of youths, who are in a critical period of cognitive and emotional growth. These approaches have consistently demonstrated strong empirical effectiveness across a wide range of mental health issues common in this age group, such as anxiety, depression and stress-related disorders, attention deficit and hyperactivity disorder, conduct disorder and behavioural addictions (Semple et al., Reference Semple, Lee and Miller2006; Hofmann et al., Reference Hofmann, Asnaani, Vonk, Sawyer and Fang2012; Banaschewski et al., Reference Banaschewski, Becker, Döpfner, Holtmann, Rösler and Romanos2017; Jones et al., Reference Jones, Thapar, Stone, Thapar, Jones, Smith and Simpson2017; Cardamone-Breen et al., Reference Cardamone-Breen, Jorm, Lawrence, Rapee, Mackinnon and Yap2018; González-Bueso et al., Reference González-Bueso, Santamaría, Fernández, Merino, Montero, Jiménez-Murcia, Del Pino-Gutiérrez and Ribas2018).
While these approaches address the cognitive-behavioural aspects of mental health and the broader understanding of mental well-being, most included studies did not report culturally adapted interventions, raising questions about the need for more diverse interventions tailored to specific cultural contexts, individual preferences and varying mental health needs of this age group. The need for culturally adapted interventions stems from the recognition that many mental health interventions, including CBT, are often developed within Western cultural frameworks (Naeem et al., Reference Naeem, Sajid, Naz and Phiri2023), which may not fully align with the values, beliefs and lived experiences of individuals from non-Western or minority cultural backgrounds. Research has shown that cultural factors significantly influence the acceptability, engagement and effectiveness of interventions. For instance, studies have demonstrated that some principles underlying CBT can conflict with cultural beliefs and practices, resulting in lower recruitment, retention and engagement among ethnic minority participants (Naeem et al., Reference Naeem, Phiri, Rathod and Ayub2019; Rathod et al., Reference Rathod, Phiri and Naeem2019).
Although this review did not explicitly analyse the outcomes of culturally adapted versus non-adapted interventions, existing literature provides compelling evidence for the importance of cultural tailoring. For example, culturally adapted CBT has been shown to improve access, engagement and outcomes for diverse populations (Naeem et al., Reference Naeem, Phiri, Rathod and Ayub2019; Naeem et al., Reference Naeem, Sajid, Naz and Phiri2023). Frameworks for cultural adaptation emphasise the need to address barriers such as language, cultural stigma and differing conceptualisations of mental health. These findings highlight the importance of tailoring interventions to ensure their relevance and effectiveness across diverse settings.
This underscores the importance of flexibility and individualisation in mental health care. Rather than adhering to a one-size-fits-all approach, interventions should be adapted to meet the unique needs, preferences and circumstances of each individual (Stanhope et al., Reference Stanhope, Ingoglia, Schmelter and Marcus2013; Miller et al., Reference Miller, Stanhope, Restrepo-Toro and Tondora2017; Moreno & Chhatwal, Reference Moreno and Chhatwal2020). This recognition of diversity within the treatment approaches signifies a shift towards holistic and inclusive models of care, prioritising symptom reduction alongside overall well-being and resilience (Cloninger et al., Reference Cloninger2010). This would potentially expand the width of exploration and innovation in mental health research and practice, ultimately enhancing outcomes for youths facing mental health challenges.
In terms of delivery platforms, educational settings emerged as the most common, offering accessibility, built-in populations and opportunities for stigma reduction (Fazel et al., Reference Fazel, Hoagwood, Stephan and Ford2014; O’Reilly et al., Reference O’Reilly, Dogra, Whiteman, Hughes, Eruyar and Reilly2018). Schools facilitate consistent engagement and leverage existing infrastructure (Weist et al., Reference Weist, Mellin, Chambers, Lever, Haber and Blaber2012), making them ideal venues for universal and preventive efforts. However, over-reliance on school-based settings risks excluding out-of-school youth such as migrants, homeless individuals or young parents, who often face heightened vulnerability (UNICEF & UNESCO Institute for Statistics, 2016). Community and healthcare settings, though less frequently used, played important roles in delivering targeted or clinical interventions, often functioning as referral points from schools. Meanwhile, general population platforms particularly digital and social media remain underused despite growing evidence that youth value the anonymity, flexibility and immediacy offered by such channels (Rickwood et al., Reference Rickwood, Deane and Wilson2007; Pretorius et al., Reference Pretorius, Chambers and Coyle2019). Their limited uptake may be attributed to their relative novelty, as well as the ongoing need to validate their safety, efficacy and ethical deployment.
Collectively, these findings underscore the importance of diversifying both intervention modalities and delivery settings. Expanding beyond traditional school-based platforms to include community, clinical and digital approaches particularly those grounded in youth-aligned and culturally sensitive frameworks can help bridge current implementation gaps. A more balanced and inclusive implementation strategy is needed to reach underserved and high-risk youth, particularly those outside formal education systems, thereby promoting equity and effectiveness in youth mental health support (Naslund et al., Reference Naslund, Aschbrenner, Araya, Marsch, Unützer, Patel and Bartels2017).
Heterogeneity of mental health concepts
The systematic review had also revealed that interest in youth mental health interventions has grown steadily over the past decade, with a particularly notable increase in 2019. This signified the global awareness and urgency to explore both mental health symptoms and well-being outcomes among youth aged 15 to 24, which also aligned with the emergence of key statistics and research emphasising its significance (e.g., WHO, 2019; UNICEF, 2021). More importantly, this review uncovered significant diversity within the mental health concept, notably distinguishing between mental health symptoms viewed through the lens of disorder and mental well-being from a transdiagnostic perspective. Specifically, 38 studies focused on specific mental health symptoms such as anxiety, depression and suicidal tendencies, while 25 studies targeted mental well-being, encompassing aspects like emotional regulation, self-efficacy, self-esteem and daily functioning. Aligning with the current categorisation of youth into General Youth, Vulnerable Youth, Youth at Risk and Youth with Diagnoses, this suggests a growing urgency of mental health continuum from normative stressors to clinically significant conditions (Kessler et al., Reference Kessler, Chiu, Demler and Walters2005; Patel et al., Reference Patel, Flisher, Hetrick and McGorry2007), as well as the understanding of the multifaceted nature of mental health and the necessity for comprehensive approaches to support individuals’ overall mental status.
Throughout history, distress and suffering have been recognised as inherent aspects of the human condition (Kendler, Reference Kendler2009). The interpretation and characterisation of mental distress have evolved significantly, particularly in Western contexts, where mental health struggles have traditionally been categorised within formal taxonomic systems like the DSM and the International Classification of Diseases (Kendler, Reference Kendler2009). These systems serve as foundational frameworks in psychiatry, clinical psychology and abnormal psychology, guiding training across various helping professions and shaping global approaches to assessing, managing and treating mental health issues (Cosgrove et al., Reference Cosgrove, Krimsky, Vijayaraghavan and Schneider2006; Marecek and Hare-Mustin, Reference Marecek, Hare-Mustin, Fox, Prilleltensky and Austin2009). However, there is a growing recognition of the limitations of these taxonomies, including issues of heterogeneity within diagnoses and incomplete symptom capture (Dalgleish et al., Reference Dalgleish, Black, Johnston and Bevan2020), leading to the emergence of transdiagnostic approach.
Transdiagnostic approach diversifies the perspectives on understanding mental health challenges and fosters new conceptualisations of the underlying theories and processes of mental distress. At its core is the recognition that risk, protective and maintenance factors and processes implicated in mental health problems, whether biological, socio-environmental or psychological, do not exhibit specificity for particular diagnostic disorders but instead operate across traditional diagnostic boundaries (Buckholtz & Meyer-Lindenberg, Reference Buckholtz and Meyer-Lindenberg2012). This approach has been shown to have an impact on assessment (Mansell, Reference Mansell2019), treatment and recovery (Murray et al., Reference Murray, Metz and Callaway2019). This notion is also supported by a body of research (e.g., Haslam et al., Reference Haslam, Holland and Kuppens2011; Waszczuk et al., Reference Waszczuk, Zimmerman, Ruggero, Li, MacNamara, Weinberg, Hajcak, Watson and Kotov2017) where mental health problems are most effectively understood along continua rather than as discrete entities. However, like the disorder perspective, the transdiagnostic approach also has limitations, where one significant drawback is its lack of a clear phenomenological framework, which can be ambiguous and lacking specificity (Fusar-Poli et al., Reference Fusar-Poli, Solmi, Brondino, Davies, Chae, Politi, Borgwardt, Lawrie, Parnas and McGuire2019). This ambiguity could complicate the measurement of psychometric items in non-clinical samples that may exhibit clinical symptoms or established mental disorders.
Considering the advantages and limitations of both approaches, it is vital to consider the proposition that mental health is not simply a uniform state of being, such as depression, anxiety or delusion (Parnas, Reference Parnas2015), nor is it solely the result of an array of subjective appraisals of problems (Ghaemi, Reference Ghaemi2006; Parnas, Reference Parnas2014). Instead, it is the integration of both diagnostic and transdiagnostic concepts where mental health is to be perceived as a multifaceted construct encompassing diverse dimensions. It is consistent with the concept where humans navigate a continuum, encountering a spectrum of symptoms ranging from mild distress to severe psychiatric disorders, each characterised by distinct origins, presentations and impacts on daily functioning (Keyes, Reference Keyes2002). As such, there is value in recognising both an individual’s position on this continuum as posited in the transdiagnostic approach and the point at which certain difficulties persist beyond a potentially individualistic threshold, thereby constituting disorders based on the diagnostic approach. This notion is consistent with the hierarchical framework as exemplified by the Hierarchical Taxonomy of Psychopathology (HiToP; Kotov et al., Reference Kotov, Krueger, Watson, Achenbach, Althoff, Bagby, Brown, Carpenter, Caspi, Clark, Eaton, Forbes, Forbush, Goldberg, Hasin, Hyman, Ivanova, Lynam, Markon and Miller2017), where it organises mental health problems into a hierarchy, with a general factor of psychopathology at the apex, broad spectra like internalising and disinhibited/externalising problems beneath, and progressively lower levels detailing co-occurring disorders, symptom components and individual signs. This perspective holds weight in assessment, diagnosis, treatment and management of mental health issues, providing a more comprehensive framework for addressing the complexities of mental well-being (Dalgleish et al., Reference Dalgleish, Black, Johnston and Bevan2020).
Heterogeneity among measurement tools
The diverse conceptualisations of mental health across studies naturally led to a variety of measurement tools, each designed to capture specific facets of its complex and multifaceted nature. For instance, depressive symptoms were assessed using standardised tools such as the 9-item Patient Health Questionnaire (PHQ-9), Center for Epidemiological Studies-Depression Scale, Mood and Feelings Questionnaire and Beck Depression Inventory-II (BDI-II). These instruments, including the BDI (Beck et al., Reference Beck, Steer and Brown1996) and the PHQ (Kroenke et al., Reference Kroenke, Spitzer and Williams1999), provided standardised scoring systems and cut-offs, facilitating comparisons across studies and populations. Similarly, the Generalized Anxiety Disorder Scale (Spitzer et al., Reference Spitzer, Kroenke, Williams and Löwe2006) and the State–Trait Anxiety Inventory offered standardised assessments of anxiety symptoms, enabling researchers to quantify and track changes over time. The current difference in measurement outcome, prevalence rate and sensitivity of scores could give rise to further heterogeneity in interpretation, which highlights the importance of standardised instruments.
Standardised instruments play a crucial role in mental health research by providing a common language for assessment and enabling objective and quantitative evaluation of psychopathological phenomena (Möller, Reference Möller2009). They are essential for assessing treatment outcomes and evaluating psychiatric service systems from both objective and subjective perspectives (Kilian et al., Reference Kilian, Bernert, Matschinger, Mory, Roick and Angermeyer2001). In addition to standardised tools, researchers often used specialised measures tailored to capture specific aspects of mental health. For example, the Rosenberg Self-Esteem Scale (Rosenberg, Reference Rosenberg1965) focuses on self-esteem, while the Social Skills Group Assessment Questionnaire (Goldstein and Pollock, Reference Goldstein and Pollock1988) assesses social functioning and interpersonal skills. Measures like the Children’s Depression Inventory (Kovacs, Reference Kovacs1978) and the Reynolds Adolescent Depression Scale (Reynolds, Reference Reynolds2010) cater to developmental differences in symptom expression among children and adolescents.
Furthermore, culturally adapted instruments in Farsi and Krio (e.g., Betancourt et al., Reference Betancourt, McBain, Newnham, Akinsulure-Smith, Brennan, Weisz and Hansen2014; Newnham et al., Reference Newnham, McBain, Hann, Akinsulure-Smith, Weisz, Lilienthal, Hansen and Betancourt2015; Jani et al., Reference Jani, Vu, Kay, Habtamu and Kalibala2016; Moeini et al., Reference Moeini, Bashirian, Soltanian, Ghaleiha and Taheri2019) ensured that assessments are sensitive and relevant to diverse populations (Van Voorhees et al., Reference Van Voorhees, Fogel, Reinecke, Gladstone, Stuart, Gollan, Bradford, Domanico, Fagan, Ross, Larson, Watson, Paunesku, Melkonian, Kuwabara, Holper, Shank, Saner, Butler and Chandler2009; Moeini et al., Reference Moeini, Bashirian, Soltanian, Ghaleiha and Taheri2019). While there were only four studies within this current review exploring this concept of cultural adaptation while conducting psychological measurements, these context-specific assessments further highlight the rising need for validity and reliability of mental health measures, in order to capture unique experiences across diverse groups (Kaiser et al., Reference Kaiser, Ticao, Anoje, Minto, Boglosa and Kohrt2019). This has the potential to facilitate a nuanced understanding of specific domains of mental health, allowing researchers to explore intricate relationships and processes. Recognising the importance of sensitivity to cultural differences and the subjective nature of mental and behavioural disorders (Brugha & Meltzer, Reference Brugha and Meltzer2017) could open up a new avenue to the path of a comprehensive approach that aligns with the broader concept of mental health, encompassing emotional, psychological and social well-being (Doré & Caron, Reference Doré and Caron2017).
Limitations and future directions
While this systematic review provides valuable insights into the current landscape of youth mental health interventions, four key limitations must be acknowledged. First, the inclusion and exclusion criteria, such as the 15 to 24 age range and the exclusion of comorbid conditions, might have inadvertently omitted relevant studies, thereby narrowing the scope and limiting applicability to more complex youth populations. Second, the use of a four-tier classification system (General Youth, Vulnerable Youth, Youth at Risk and Youth with Diagnosis) enabled structured synthesis but might oversimplify the fluid and overlapping nature of youth mental health experiences. Although each study was categorised into only one group for analytic clarity, conceptual overlap among categories is likely. Third, considerable heterogeneity was observed across the included studies, particularly in intervention types, settings and outcome measures. While such variation reflects the diversity of youth mental health needs and service contexts, it might also limit the comparability of findings and the strength of conclusions that could be drawn. Finally, the narrative synthesis approach allowed for the integration of diverse study designs and contextual factors, offering a comprehensive overview of intervention trends and implementation contexts; however, this method did not support causal inference or direct comparisons of intervention effectiveness.
Given these limitations, the findings of this review should be interpreted within the context of its methodological scope, offering a foundation for future targeted research. Future research should adopt a more inclusive and context-sensitive approach to study selection and synthesis, including greater attention to comorbidities and age overlaps. Longitudinal and comparative studies are needed to assess the suitability and relative effectiveness of different intervention strategies over time and across youth subgroups. Efforts should also focus on examining the heterogeneity identified in this review, particularly in intervention types, settings and outcome measures, and assessing their relevance to specific implementation contexts. Transparent reporting of cultural adaptations and implementation processes is essential to distinguish meaningful contextual tailoring from methodological variation. Lastly, expanding research in underrepresented regions and populations, and exploring multi-category or dimensional classification systems to better capture the complexity of youth mental health, will be critical for advancing equity, relevance and impact in future intervention research.
Conclusion
This systematic review underscored the complex and varied landscape of mental health interventions targeting youth aged 15 to 24 globally. The findings highlighted the critical need for a balanced approach that integrates both digital and traditional methods, particularly in response to infrastructural and technological disparities across different income settings. The significant heterogeneity in conceptualisations of intervention modalities, mental health concepts and measurement tools underscored the diverse approaches required to effectively address the mental well-being of young individuals. These findings emphasised the importance of adopting comprehensive, culturally sensitive and personalised strategies to support this demographic. By advancing our understanding of mental health concepts, embracing both disorder-specific and transdiagnostic perspectives, and standardising our approach to assessment, mental health care for youths has the potential to be more inclusive, responsive and ultimately more effective in promoting long-term well-being. Moving forward, it is essential to continue developing and testing these interventions to ensure that they are contextually relevant and capable of meeting the evolving challenges faced by youths worldwide.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2025.10042.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/gmh.2025.10042.
Author contribution
Data collection: M.H.L.; Data screening and analysis: M.H.L., K.H.Y.; Draft manuscript preparation: M.H.L.; Interpretation of results: M.H.L.; Study conception and design: M.H.L., M.-H.R.H. All authors reviewed the results and approved the final version of the manuscript.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors declare no competing interests.



 Open access
Open access
Comments
No accompanying comment.