


Introduction
How information about the donor and donor relatives in reproductive donation is managed has been debated ever since insemination with donor sperm became part of medical practice.Reference Richards and Freeman 1 Over 30 years ago, Francois Shenfield described information giving as the “main controversy in assisted reproduction with donor gametes.” Reference Shenfield2 In 2023, the Human Fertilisation and Embryology Authority (HFEA), the UK’s regulator, noted, “The future of donor conception information … raises some of the most sensitive, challenging, and complex questions for the HFEA as the regulator.”Reference Fertilisation and Authority 3 Information giving in reproductive donation involves legal, sociological, and ethical questions underpinned by complex assumptions about what reproductive donation is and what it represents. These speak to how we view and construct the family; what family forms are supported socially and legally; what information is meaningful to people; what information, if any, they should have a right to receive; and what corresponding duties, if any, these place on others.Reference Daniels and Haimes 4
In this paper I develop a novel typology of models of reproductive donation, dividing this practice into two main models, the biomedical and the psychosocial model. The biomedical model will be subdivided into the bioscientific and the clinical models, and the psychosocial model into the family, person, and network models — to give a more granular understanding of reproductive donation. The models reflect what happens in practice and policy and are a representation of a set of beliefs and approaches to reproductive donation that coalesce around key themes, with overlapping points of similarity and departure. I will not debate the merits of the models, advance one model’s superiority, or revisit debates over gamete donor anonymity.Reference Frith 5 The aim here is to develop a typology that clarifies the underpinning conceptual commitments of different approaches (models) to reproductive donation. While the models have implications for all aspects of reproductive donation, here I will focus specifically on the implications for information giving.
This typology of models of reproductive donation can elucidate our understanding of reproductive donation and how it has been governed. Drawing on Dean Spade’s influential work on how law contributes to certain societal arrangements, I will show how the regulation of reproductive donation both shapes and reinforces specific concepts (models) of reproductive donation. Spade conceptualizes law as a set of tactics,Reference Spade 6 arguing that the law is always a mess of contradictions, and cautions against taking what the law says about itself at face value, suggesting, “Instead, we might look for the broader patterns, beyond what law says it is doing, to see how it contributes to certain arrangements that concern us.” 7 In reproductive donation, the law reinforces certain conceptualizations of reproductive donation and deprivileges others.Reference Foucault 8
I will trace the evolution of the regulation of reproductive donation, using the UK as a case study alongside examples from other jurisdictions. This will show how these different models have shaped UK and international regulations and oversight of information giving. Then the models will be used to explicate recent changes in the landscape of reproductive donation, the increasing use of commercial online direct-to-consumer genetic (DNA) testing (DTCGT), growth in social media platforms that enable people to be traced more easily, and changing societal attitudes — showing how these challenge current regulation and oversight. These models have a threefold purpose: as a conceptual framework, a useful heuristic, for understanding reproductive donation; as a basis for critiquing regulation and oversight in this area; and as a basis for formulating coherent approaches to the oversight and regulation of reproductive donation.
By developing this novel typology, this paper makes an important contribution to the debate over information provision in reproductive donation. The models provide a conceptual framework for analyzing the key elements of reproductive donation and, by distinguishing between different conceptualizations, establishes a clearer language for academic and professional debate. This framework can serve as a foundation for subsequent theoretical advancement in the field. Understanding how reproductive donation is conceptualized is critical, as it significantly influences how it is organized and regulated. This typology makes visible the conceptual underpinnings of regulation and oversight, showing which elements of the different models are at play and which are subsumed or overlooked. This provides a basis for analyzing and critiquing current regulation and oversight and can serve as a starting point for determining what arrangements should be upheld or revised. However, specific regulatory reform recommendations are outside this paper’s scope.
Considering these models of reproductive donation is particularly timely and pressing, because technological advances offer new and previously unanticipated opportunities to search for information about the donor, donor relatives, and wider family networks in unregulated and/or unmanaged spaces. Social media and DTCGT, for example, have enabled those seeking donor relations to find — and in some cases contact — these donor relations without going through either state registers or official “mediators” such as fertility clinics.Reference Gilman 9 New developing technologies, such as facial kinship verification software,Reference Łukasiewicz, Frith and Redhead 10 could also be used to search for donors and donor relatives in the future and, like DTCGT, have the potential to further disrupt and circumvent regulatory systems. This poses challenges for regulatory authoritiesReference Phillips 11 and, prompted by these developments, there are discussions both in the UK and internationally about how regulators should respond and what, if any, regulatory reform is needed. 12
Terminology, Scope, and Clarifications
Terminology in assisted technology and reproductive donation incorporates normative assumptions and is often contentious.Reference Shaw 13 I will adopt commonly used terms while recognizing potential disputes or disagreement. “Recipient” is used to refer to someone receiving gametes/embryos to have children, whether couples or individuals. “Donor-conceived person” describes someone conceived from donor gametes. I shall use donor-conceived offspring when I am talking about young donor-conceived people (i.e., under 16). “Donor-siblings” is used to denote genetic half-siblings conceived from the same donor. Some do not like this term as they do not think that those conceived from the same donor should be seen as siblings, but I will use it here as it is commonly used in the literature. What constitutes a “donor relation” is not straightforward; I will use this term to describe those related through donor conception. These relations are not always genetic — for example, the donor’s partner could be a donor relation.
Two categories of information, non-identifying and identifying information, need to be distinguished. Non-identifying information is information about the donor that does not identify them, such as details of the donor’s physical appearance, interests, and education. Identifying information, as the name suggests, is information that could identify the donor — such as their name, last known address, or other contact details. It is this type of identifying information that is usually held by registers and clinics.
In terms of jurisdictional scope, I will use the UK’s legal and regulatory framework as a case study, 14 and also draw on other countries’ regulatory and practice-based approaches. The models of reproductive donation I develop underpin other jurisdictions’ approaches across the global north, so their relevance extends beyond the UK.Reference Schurr 15 There has been a rise in donation outside of clinics, which has been termed “informal donation.” As I am concerned with the regulation and oversight of reproductive donation in clinics, informal donation is not considered in any detail.Reference Taylor 16
Models of Reproductive Donation
In this section I will outline this novel typology of models of reproductive donation, dividing reproductive donation into two main models, the biomedical and the psychosocial. To develop the models, I have drawn on historical accounts of reproductive donation, theoretical discussions from the academic literature, medical journals, legal and regulatory sources (such as statutes, case law, and codes of practice), professional guidelines, and empirical investigations into peoples’ experiences of reproductive donation.
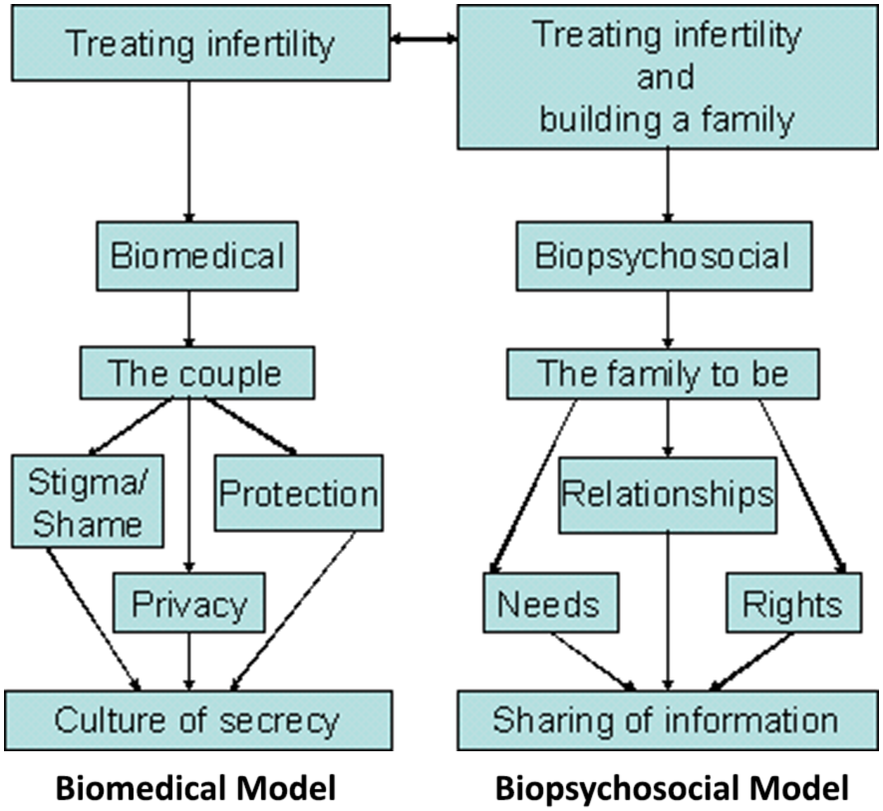
In using the term “models,” I have adapted the distinction between biomedical and psychosocial models in medical sociology, where such categories are used to delineate different practices and approaches to medicine, disease, and health. These biomedical and psychosocial models of medicine have provided a useful way to categorize and analyze modern medicine in terms of understanding medicine as a social institution: how it is influenced by broader structures and cultural beliefs.Reference Clarke 17 Models are ideal types and do not exist in pure form in practice; they are idealizations as they flatten, to a degree, the complexity of reality.Reference Frigg, Hartmann, Zalta and Nodelman 18 Medicine has never operated solely according to the biomedical model, for example. However, the models are not divorced from reality. They are based on what happens in practice; they are descriptive and based on theoretical understandings of what the practice is and should be. The models have a temporal component, reflecting the evolution of reproductive donation over time. Further, there may be more than one element, or a combination of models of reproductive donation at play, in practice and regulation at any one point in time. Different places — the clinic, regulatory structures, and social spaces (including social media and other networks) — may embody different elements of the models, privileging or downplaying certain aspects of reproductive donation depending on circumstance and context. Ken Daniels, who has written extensively on reproductive donation, applied the biomedical and the psychosocial (biopsychological in his terminology) models to reproductive donation (see Figure 1).Reference Daniels 19
Contrasting Models.

Figure 1. Long description
A double-headed horizontal arrow connects the top boxes of two parallel flowcharts.
The left flowchart represents the Biomedical Model. It begins at the top with a box labeled Treating infertility. A downward arrow leads to a box labeled Biomedical. A downward arrow leads to a box labeled The couple. From this box, three arrows diverge to three separate boxes labeled Stigma forward slash Shame, Privacy, and Protection. These three boxes then have arrows converging into the final bottom box labeled Culture of secrecy.
The right flowchart represents the Biopsychosocial Model. It begins at the top with a box labeled Treating infertility and building a family. A downward arrow leads to a box labeled Biopsychosocial. A downward arrow leads to a box labeled The family to be. From this box, three arrows diverge to three separate boxes labeled Needs, Relationships, and Rights. These three boxes then have arrows converging into the final bottom box labeled Sharing of information.
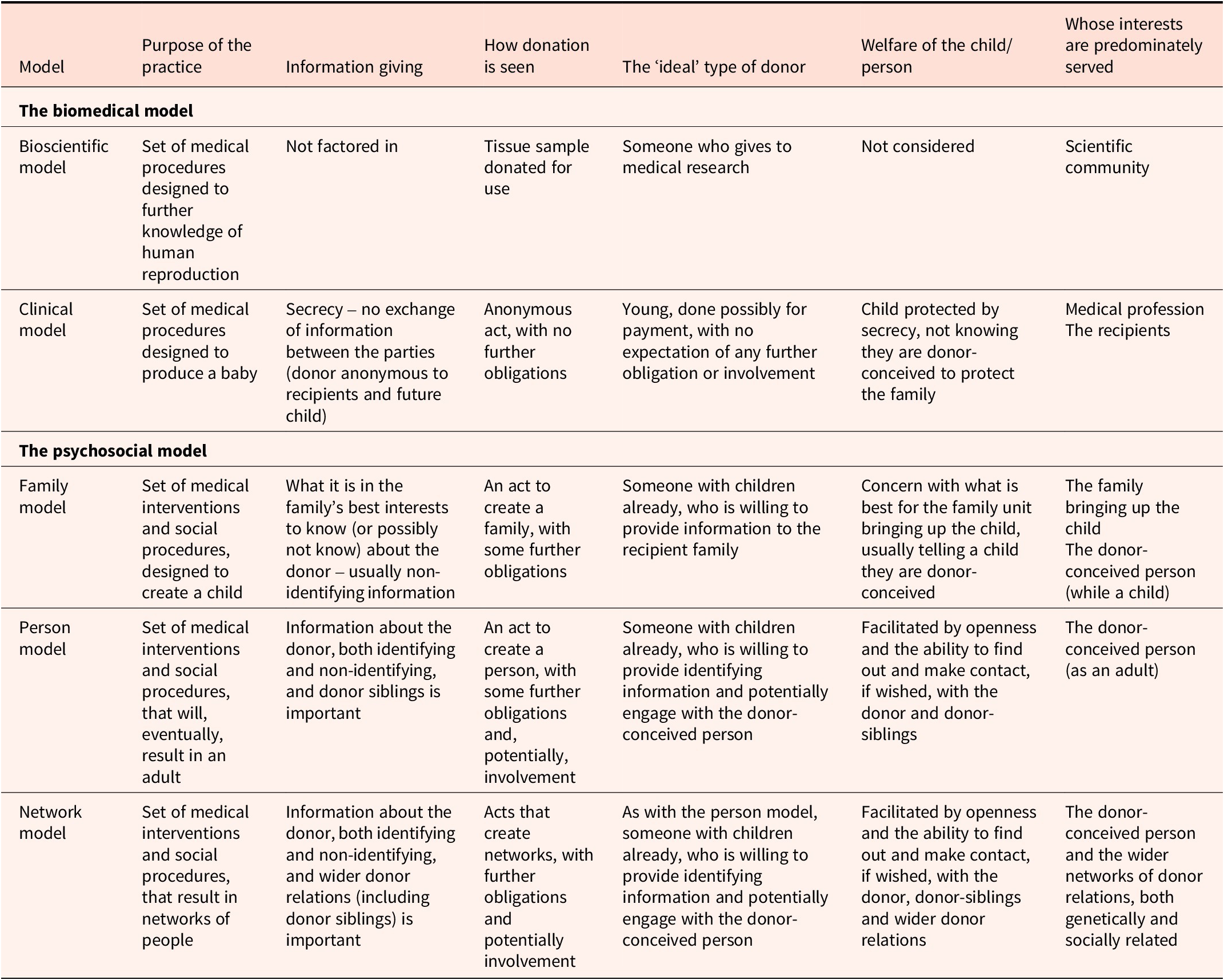
Taking Daniels’ work as a starting point, my typology of models of reproductive donation is as follows (see table 1):
-
• Biomedical models
-
○ Bioscientific model — medical procedures designed to produce knowledge about human reproduction.
-
○ Clinical model — medical procedures designed to produce a baby.
-
-
• Psychosocial models
-
○ Family model — a set of medical interventions and social procedures, designed to create a child. 20
-
○ Person model — a set of medical interventions and social procedures that will, eventually, result in an adult.
-
○ Network model — a set of medical interventions and social processes that will result in networks of people.
-
Overview of the models of reproductive donation

Table 1. Long description
The table is organized into seven columns including Model, Purpose of the practice, Information giving, How donation is seen, The ideal type of donor, Welfare of the child or person, and Whose interests are predominately served.
The first section is The biomedical model.
* Bioscientific model. Purpose is medical procedures to further knowledge of human reproduction. Information is not factored in. Donation is seen as a tissue sample donated for use. Ideal donor gives to medical research. Welfare is not considered. Interests served are the scientific community.
* Clinical model. Purpose is medical procedures to produce a baby. Information is secret with no exchange of information between the parties. Donation is an anonymous act with no further obligations. Ideal donor is young, possibly paid, with no further involvement. Welfare is protected by secrecy. Interests served are the medical profession and recipients.
The second section is The psychosocial model.
* Family model. Purpose is medical and social procedures designed to create a child. Information is based on the family’s best interests, usually non-identifying. Donation is an act to create a family with some obligations. Ideal donor has children and provides information. Welfare focuses on the family unit. Interests served are the family and the child.
* Person model. Purpose is medical and social procedures resulting in an adult. Information includes identifying and non-identifying data and donor siblings. Donation is an act to create a person with potential involvement. Ideal donor has children and provides identifying information. Welfare is facilitated by openness and contact. Interests served are the adult donor-conceived person.
* Network model. Purpose is medical and social procedures resulting in networks of people. Information includes identifying data and wider donor relations including donor siblings. Donation creates networks with obligations. Ideal donor is the same as the person model. Welfare is facilitated by openness with wider relations. Interests served are the donor-conceived person and wider networks.
When saying that some models aim to produce a baby, or adult, this refers to their primary goal and focus. The clinical model, for example, did expect that a child and adult would eventually result, but its main objective was achieving a live birth.
By elucidating the type of practice we understand reproductive donation to be, the models shed light on key features of reproductive donation: what is the main intended outcome of the practice; who has access to information, about whom, when, and what type of information; who is seen as the ideal donor;Reference Ameling 21 how the welfare of the future child (or adult) should be considered; and whose interests are taken into account, privileged, or ignored. Welfare in this context is used to mean that a child’s basic need for a stable, supportive, environment can be met.Reference McCandless and Sheldon 22 When outlining the models I will consider how they approach each of these elements.
Biomedical Models of Reproductive Donation
For the biomedical models, much of the material is found in articles and accounts written before 2000, after which the psychosocial approaches to reproductive donation became more prominent in the literature. These biomedical models arose in an ad hoc, ungoverned space, at a time where sex and reproduction were taboo subjects, and techniques such as artificial insemination, whether using donor or the husband’s sperm, challenged notions of the sanctity of marriage and were often seen as forms of adultery and/or inappropriate sexual conduct. For example, the views expressed in Earl of Feversham’s Report (1960), a committee of inquiry set up by the UK government to investigate the legal aspects of Artificial Insemination by Donor (AID), raised concerns about adultery, masturbation, and the effects on the family and society. 23
The Bioscientific Model
The bioscientific model focuses on advancing our knowledge of human reproduction. At its root, this model represents a concern with pushing the boundaries of science. In the bioscientific model, the provision of information about the donor to any future donor-conceived person was not considered. This is simply beyond the scope of its concern.Reference Braude and Johnson 24 The focus on biomedical research enables this type of “social” consideration to be bracketed off. Scientific regulation and oversight are conducted in a different regulatory space from child health, child welfare, and family law. The regulatory structures governing medical research prioritize the “here and now” of consent to participate, any foreseeable harm to participants, and the use of human tissue.Reference Burget 25 Arguably, the interests at the heart of this model might be couched not only in terms of pushing the frontiers of knowledge, but also — in its modern iteration — incorporating the imperatives of the scientific-industrial complex to produce commercially exploitable outputs and economic growth. 26
The bioscientific model has not been superseded now that IVF, egg freezing, and other once-cutting-edge technologies are now part of routine fertility treatment. There are always new techniques coming through, developments such as in vitro gametogenesis and exogenesis.Reference Cohen and Adashi 27 Therefore, elements of reproductive donation may, when they are at the experimental stage, be understood as operating within the bioscientific model.
The Clinical Model
The clinical model becomes relevant when the developments produced by the bioscientific model are sufficiently advanced to become part of clinical practice, moving out of the laboratory and into the clinic. The clinical model sees reproductive donation as a medical procedure and its main goal is producing a live birth.Reference Swanson 28 Haimes argues that seeing the “donor insemination offspring” as a successful outcome of a medical procedure, “acts to draw a line under the involvement of clinicians.”Reference Haimes, Daniels and Haimes 29 It is not within the clinical remit what happens subsequently. For example, in the early days of artificial insemination, and later IVF, developments were rolled out with no systems for monitoring the future health of any children born from these techniques. In the discussion that took place in the Panel on Human Artificial Insemination, set up by the British Medical Association in 1971, it was argued that follow-up should not be done due to secrecy concerns. The committee did, however, recommend putting in place procedures for long-term monitoring of children born from artificial insemination, but this did not become common practice. 30
The clinical model operated reproductive donation under conditions of anonymity of the donor and secrecy of the practice in the second half of the twentieth century.Reference Pfeffer and Stanworth 31 The stigma attached to male infertility, concerns over legal parenthood and the moral concerns with the procedure itself,Reference Dempsey, Nordqvist and Kelly 32 underpinned the imperative to keep the practice secret and ensure that the donor and recipients never had any need to meet. This enabled clinicians to run a practice that, until the late 1980s, was seen as immoral and, “a bit grubby,” 33 without undue external censure. In the clinical model the notion of the baby as successful outcome and secrecy come together. The goal was to produce a baby, and secrecy allowed the method of conception to be hidden, with no consideration of what information the donor-conceived person might need later.Reference Price, Clarke and Parsons 34 Once techniques such as IVF became routine in clinical practice, concern for the welfare of any child produced became more relevant, and secrecy was a key element in this. It was thought that the nuclear family should be protected from intrusion by the donor, and the welfare of the child was best ensured by them being unaware of the circumstances of their conception. 35
Secrecy and anonymity are also relevant to how the donor was seen in the clinical model. The ideal donor is happy to be anonymous and remain so to the recipients and the donor-conceived person. This donor should be young(ish), receive payment, and give, “with the intention to help others but without wishing to become involved in the receiving family.”Reference Pennings 36 The medical student donor of yesteryear who donated for beer money and never gave it a second thought was, perhaps, the ideal donor! The donor’s interests were considered in the clinical model only insofar as it was thought important to maintain secrecy to ensure a supply of willing donors, and to protect them from paternity claims. This was the case in England until a provision in the 1987 Family Law Reform Act allowed the husband of the woman who had used sperm donation to be entered on the birth certificate as the father of the child.Reference McHale and Fox 37 The donor should, as far as possible, be “matched” to the appearance of the recipient father. 38 In this way the practice of reproductive donation was intended to be concealed, and by matching donors and recipients, the “natural” family was mimicked as closely as possibleReference Haimes 39 — enabling the donor-conceived child to “pass” as the “naturally” conceived child of the marriage.
In sum, the donor-conceived person is largely absent in the biomedical models. The main interests served are those of advancing medical science, enabling clinical practice, and those of the recipients. The bioscientific model focuses on advancing knowledge, while the clinical model focuses on producing pregnancies and live births. Although the biomedical models did consider the donor-conceived person’s interests, they believed secrecy best served these, hiding the donor’s identity and treating the conception method as unimportant once the child was born.Reference Redhead 40
Psychosocial Models of Reproductive Donation
The psychosocial models are a set of approaches that see the practice of reproductive donation as contributing to forming a family and creating a person who will have a future biography, of which the circumstances of their conception can be a part. These models have grown up, in part, as a “response” to the biomedical models and against the backdrop of shifting societal attitudes to infertility, fertility treatment, and different family forms. These models are attentive to the wider implications of reproductive donation — the psychological and the social aspects of the practice. These models recognize that those who are born as a result are likely to grow into adults who may go on to be parents themselves, seeing reproductive donation as part of the life course rather than a scientific success or a one-off clinical event. Haimes sees the contrast between the biomedical models and what she calls “the broader perspective” (akin to psychosocial models) in the following way: In the clinical model the child conceived was seen as a successful outcome of a medical procedure, whereas in the broader perspective the child is seen in terms of their future relationships with their parents and in terms of their image in wider society. 41
The increasing influence of the psychosocial models from approximately the middle 1980s is illustrated by the growing importance placed on the role of counseling in fertility treatment. Specialist counselors in fertility clinics began to emerge around this time. Counseling gave people the opportunity to think through the wider implications of donating or using reproductive donation, and it became differentiated from the process of getting consent for the fertility procedure itself, which was the responsibility of the medical staff.Reference Blyth 42 This interest in the psychosocial aspects of reproductive donation is reflected in the founding of organizations such as the British Infertility Counselling Association (BICA) in 1988 and special interest groups (SIG) in the two main professional associations for fertility professionals and reproductive scientists. The Mental Health Professional Group of the American Society of Reproductive Medicine (ASRM) was started in 1985, and the European Society of Human Reproduction’s (ESHRE) Psychology and Counselling SIG in 1993. 43
The psychosocial model has been articulated in the literature by authors such as Ken Daniels and Petra Thorn.Reference Daniels and Thorn 44 Here, I further refine this model, subdividing it into the family, person, and network models. There is overlap between the different subdivisions of the psychosocial model. These subdivisions are not mutually exclusive: the family model focuses on childhood and the welfare of the family; and the person model builds on and incorporates this focus, adding a consideration of the adult donor-conceived person’s interests and welfare. The network model builds on and incorporates both the family and person models’ focuses and extends this to consider the networks that might be created by donor conception. Despite this overlap between these subdivisions of the psychosocial models, it is illustrative to make these divisions, as it demonstrates how the psychosocial models focus on different stages of the life course, reflecting how key elements in debates over reproductive donation have changed over time in scope and emphasis.
The Family Model — A Set of Medical Interventions and Social Procedures Designed to Create a Child
Daniels and Thorn encapsulate the family model when they say, “Donor Insemination [is] a means of family creation as well as a means of treating infertility…. It creates a family — a complex social unit — with a past, present and future.”Reference Daniels and Thorn 45 In this model the main outcome of reproductive donation is the creation of a child within a family. 46 A central feature of the family model is determining how best to ensure the welfare of the family unit created through reproductive donation, with particular attention to the child’s welfare.Reference Daniels and Thorn 47
In terms of information provision to donor-conceived offspring, the main concern is to establish what it is in the family’s best interests to know (or possibly not know) about the donor. The debate in this model is how best to ensure the donor-conceived offspring’s welfare within the context of the family. Hence, the family model itself does not necessarily indicate what, if any, information donor-conceived offspring should be given. It could be that the parents’ preference is to maintain secrecy about donor conception as the best way of ensuring their child’s welfare. If this were to be the case, then it would be perfectly consistent in the family model to advocate secrecy and donor anonymity.Reference Pennings 48 However, most authors who promote a family model of reproductive donation are in favor of openness about donor conception origins.Reference Daniels, Thorn, Blyth, Langridge and Harris 49
Hence, those working within the family model of donation were generally very clear that children should be told that they were donor conceived. It is claimed that openness and honesty are to be preferred, and that basing family life on deception and secrecy can cause stress and anxiety within the family.Reference Snowden and Snowden 50 Further, there is a concern over what sort of information donor offspring should have about the donor.Reference Snowden and Mitchell 51 In this mode the focus is on non-identifying information about the donor: donor offspring might be curious about the donor’s physical characteristics and family aptitudes, and have queries and uncertainties about the donor’s medical history. Sants coined the term “genealogical bewilderment” in 1964 to refer to children who had no or only uncertain knowledge of their natural parents, and argued that such uncertainty could have a detrimental effect on the child’s mental health.Reference Sants 52 Although Sants was considering the issue in relation to adoptive children, McWhinnie argued that such “bewilderment” can apply equally to donor offspring.Reference McWhinnie 53 Other donor relatives such as donor siblings or wider family members (e.g., the donor’s parents or children) were seldom mentioned in the 1980s and 1990s.
In the family model there is a concern with ensuring that the donor offspring grows up into a well-functioning adult, and openness about donor conception and information about the donor is viewed as aiding this. However, in contrast to the person model outlined below, the family model is concerned with how to approach donor conception during childhood. There are discussions in the literature over how to tell children they are donor-conceived, what the child might understand at different ages, and developing resources such as age-appropriate books to aid children’s understanding. 54
In the family model there is greater focus on the donor and a consideration of what, if any, responsibilities should follow donation. The ideal donor should be amenable, at the very least, to providing non-identifying information. DanielsReference Daniels, Daniels and Haimes 55 argues that information sharing between gamete donor and donor offspring is the key area where this responsibility should be carried out. Daniels is not arguing that gamete donors should have any legal parental responsibility, but rather, non-identifying information should be available to donor offspring so that they can have a sense of where they come from and knowledge about their origins.Reference Daniels 56 Thus, disinterested donors who are motivated solely by financial incentives become less desirable, and donors who might already have children, and want to help others, become the “ideal” donor.Reference Daniels, Lewis and Curson 57
In sum, the family model sees the interests of the family created by reproductive donation as paramount. In foregrounding the interests of the family, the donor-conceived offspring’s interests are not seen in isolation, and a more relational concept of child welfare is advanced.Reference Nedelsky 58 That is, relationships are viewed as being central to our flourishing. It is through measures that promote the quality of the family relationships that a child’s welfare is best achieved, extending the basic definition of welfare mentioned earlier. The family model, while being primarily concerned with the family who bring the child up, does attend to how childhood will equip the donor-conceived offspring to be a healthy adult. But the focus is on how to handle donor conception when the child is young, whereas the person model, outlined next, takes how donor conception is managed in adult life as its main focus.
The Person Model — A Set of Medical Interventions and Social Procedures that Result in the Creation of an Adult
The person model builds on, and has many similarities with, the family model. Both models are concerned with the welfare of the donor-conceived offspring, but importance is given to the donor-conceived adult’s interests and welfare throughout the life course as an adult, as well as their interests when they are a child. Hence, the person model moves beyond the family model, which seeks to promote a good childhood and one that forms a basis for a good adulthood, to considering the donor-conceived adult’s interests and welfare. The person model recognizes that reproductive donation creates adults, not just children, and that being conceived by donation can be an issue (for some people) of varying degrees of importance throughout the life course.
Like the family model, the person model champions openness about the circumstances of conception and sees information provision to the donor-conceived person about the donor, both non-identifying and identifying, as important. As the concern is for the welfare of the donor-conceived person, the focus here is on giving them the option to access this information if they wish, usually when they reach an age of majority. In the person model, information provision also extends beyond the donor to include other family relationships, with discussions of donor siblings becoming more prominent from the 2000s. For some donor-conceived people, information about donor siblings can be as important, or of more importance than, information about their donor.Reference Scheib 59 There is also increasing attention given to not only finding information about the donor and donor siblings but also exploring the possibility of making contact with them. Organizations were set up around the early 2000s to facilitate this. The Donor Sibling Registry (DSR), for example, was set up in 2000 in the US to enable donor-conceived people to connect with their donor siblings and the donor. It has grown into a global organization, with more than 100,686 members from over 135 countries. 60 The DSR provides a database online where links can be made between people conceived by the same donor (by information, donor number, date of birth, and clinic or sperm bank) and their donors. The DSR says that it has facilitated over 27,912 connections between donor siblings and/or donors. In the UK, mainly for those conceived before the Human Fertilisation and Embryology (HFE) Act came into force (in 1991), the UK Donor Link was established in 2004 (it has now become the Donor Conceived Register).Reference Crawshaw 61 This is a DNA database where donors and donor-conceived people can sign up and submit their DNA, with the aim of being linked to donor relatives. In the Netherlands, the Fiom KID-DNA database was set up in 2010, and runs a bespoke DNA database to help donor-conceived people and donors find donors and donor siblings.Reference Indekeu, Prinsen and Maas 62
As in the family model, in the person model, the donor has some responsibility towards people born from their donation. Exactly what this responsibility is, however, is contested. What people want when they search for their donor varies; some just want information about the donor and others want contact, with the possibility of forming some kind of relationship. Frith et al. studied the experiences of those who used a DNA-based register to search for donor relatives and found that these experiences of searching for and finding donor relatives were largely positive, however, there was not “one story” of these experiences.Reference Frith 63
In terms of welfare of the donor-conceived person, the person model, like the family model, is concerned with the longer-term benefits of patterns of information giving and knowledge of donor relations that are established in childhood, both for the optimal functioning of the family within which the donor-conceived child is raised and for the adult that the donor-conceived child will become. As with each of the psychosocial models, there is debate over how best to ensure the longer-term welfare of the donor-conceived person, but in this model, there is a recognition that this may change across the life course. Thus, what an adolescent may want could be very different from someone who is contemplating having their own family, or someone who has children of their own.Reference Freeman and Freeman 64 The person model is concerned with how donor conception is managed in adulthood, how people might access information, and how they can be supported throughout the life course with any issues their donor-conceived status might raise. In the person model, it is about extending choice — choices that were not available under the clinical model — and there are no requirements for donor-conceived people to access this information if they do not want to. It must also be noted that some donor-conceived people have no interest in finding out information of any kind about their donor or donor relations.
In sum, in the person model, it is the adult donor-conceived person whose interests are seen as most important. Their interests are understood to be dynamic and evolving, so that attention is paid to how they might be best realized throughout the life course, rather than just in the early years of childhood in the context of immediate family relations.
The Network Model — A Set of Medical Interventions and Social Procedures that Result in a Network of People
The third subdivision of the psychosocial model in my typology is the network model. This extends the person model by moving beyond a focus on the donor and donor siblings to incorporate the wider family and relational networks that reproductive donation can create. The network model constructs the outcome of reproductive donation as creating a person within a network, broadening consideration of donor relatives from the donor and donor siblings to a wider range of potential connections. This network can extend to the donor’s “own” children, the donor’s partner, and what we think of as extended family: grandparents, aunts and uncles, cousins, etc. This model considers the temporal and spatial effects of reproductive donation that operate through time and geography, for instance to include ancestors and geographical connections such as heritage and ethnicity.
With the creation of wider networks comes the potential for the discovery of information that is potentially boundless. In light of the variety of human relationships potentially encapsulated in the network model, information giving in this model may be more akin to “information discovery,” and sometimes inadvertent discovery. The ability to “see” these networks has largely come about because of technological developments: increased use of the internet, particularly DTCGT and social media platforms. This increasing visibility is an unintended consequence of this technology. The information found by these mechanisms may be more diverse than that conventionally seen as important information in reproductive donation. It can go beyond the short précis of the donor’s characteristics and interests that clinics collect,Reference Crawshaw and Dally 65 and the type of identifying information that the HFEA 66 can release to those born from gametes donated after 2005, such as the name or last known address of the donor. This information could potentially extend to finding the donor’s social media presence, and this could be used to build up a rich picture of them, especially if they are active on social media. It can also lead to finding donor siblings or extended family and information about ancestry, heritage, ethnicity, and family geographical origins.
The network model shares many similarities with the other psychosocial models in its concern for the welfare of the donor-conceived person throughout the life course. What reproductive donation means in terms of family responsibility, kinship ties, and the formation of social relationships is less settled. These new networks are negotiated by those involved with few templates or guidance — they are pioneers.Reference Hertz and Nelson 67 As a result, there is less clarity (or uniformity) than in the other models as to what might promote or enable the long-term welfare of the donor-conceived person, and studies on the implications of the creation of these wider networks are ongoing.Reference Gilman 68 In the network model, as in the person model, the donor-conceived person is still central, whereas the interests of recipients and the donor are decentralized. Although their interests remain important, a wider range of actors enter the stage, both genetic and social, and these relations and relationships also become objects of concern in the literature, practice, and regulation.
Having outlined these models of reproductive donation, it is evident that the trend since the late twentieth century has been towards the psychosocial models. There has been: a greater focus on the welfare of the donor-conceived child and future adult; more openness about the circumstances of donor conception; and a growth in the number of countries that have regulations that encourage or proscribe the use of identity release (non-anonymous) donors. This has not been a straightforward transition or a temporal “progression” — where progression is seen as moving from outmoded ways of seeing reproductive donation to “better” ways. The bioscientific model is still with us, and these models circle back and are interwoven in current practice. Hence, the psychosocial approaches have not replaced biomedical models: they continue to coexist and interact with each other. They inform and construct the way that reproductive donation is talked about in a range of fora, from academic articles (both theoretical and practitioner literature), policy documents, to online discussion groups and in the popular media, in a myriad ways.
I will now consider how these models can be used to both further understand the oversight and regulatory frameworks used in reproductive donation and critique these frameworks.
Applying the Models of Reproductive Donation
This typology of models of reproductive donation can be used to interrogate regulation and oversight by shedding light on their often-implicit assumptions, and examining how they sustain, in Spade’s terminology, “certain arrangements” of reproductive donation. 69 While the biomedical and psychosocial models are conceptually distinct, in regulatory practice, as will be shown below, often elements of each of these models will be embedded in one regulatory framework. In this section I first consider the regulatory approach to reproductive donation in the UK, examining how the evolving regulatory landscape supports, reinforces, or marginalizes particular models of donation. Then the models will be used to explicate recent trends and changes in the landscape of reproductive donation and show how these changes challenges current regulation and oversight in many jurisdictions.
The Evolution of Regulation in the UK
The passage of the HFE Act 1990 (the 1990 Act/the Act) both reinforced and troubled the clinical model of reproductive donation. The Warnock Committee, whose report formed the basis for the Act, emphasized the secrecy of donor conception, with provisions safeguarding recipients’ confidentiality over their use of fertility services over and above general medical confidentiality requirements. 70 The donor continued to be anonymous, both to any future offspring and to the recipients, and was still treated as a potential threat to the family bringing up the donor-conceived child.
However, the 1990 Act did not entirely adopt the clinical model of reproductive donation. Rather, it introduced elements of the family model and set in motion others that would be used to move towards the person model. The Warnock Committee recommended that, on becoming adults, donor-conceived people should be provided with some non-identifying information about the donor, 71 and the Act enshrined this (limited) right to information in statute from the age of 18. They were able to access non-identifying information about their donor that clinics collected, and the goodwill messages and pen portraits that donors were given the opportunity to write. 72 In addition, to address the risk of consanguinity, donor-conceived people could, from the age of 16, approach the HFEA to see whether they were donor-conceived if they were planning to marry and were concerned that they may be biologically related to their partner. The Act also required clinics to provide “a suitable opportunity to receive proper counselling” both to those undergoing treatment and to donors. 73
The 1990 Act also established the HFEA, 74 whose purview included oversight of the use of gametes and embryos in fertility treatment and research, responding to new developments, and issuing a code of practice for clinics. 75 Further, the Act made provision 76 for establishing a register of all those born from reproductive donation. This was one of the first central registries for recording details of reproductive donation and, arguably, one of the most important achievements of the Act.Reference De Geyter 77 The HFEA register contains information about embryo and gamete donors, recipients of donated embryos and gametes, and, if notified, births of donor-conceived children. The Warnock Report recognized that the donor-conceived person might have an interest in the donor, and in establishing a register and putting the collection of information on a legal footing, enabled the possibility of people having access to it in the future.Reference Frith 78 This statutory recognition of the impact of donor conception on the lives of donor-conceived people was an important move away from the clinical model, arguably incorporating elements of both the family and person models. It was based on the family model in that there was a greater concern for the welfare of the child produced by reproductive donation. At the time, this was considered to be maximized by insulating the family from intrusion by the donor, neither acknowledging the donor’s existence nor enabling contact. Elements of the person model were incorporated by thinking about the donor-conceived person as an adult and making provision for them, through the register, to have non-identifying information about their donor when they reached majority.
Attitudes to information giving changed after the passage of the 1990 Act: from believing that a child’s welfare was best promoted by keeping the practice secret, it was subsequently seen as advantageous to the child to be told about their donor conception origins. Parents were increasingly encouraged to tell their child they were donor-conceived, as discussed earlier in the consideration of the family model. This is evidenced by the changes in the advice given to recipient parents concerning openness with children about the circumstances of their conception in HFEA guidance. Comparing the first HFEA Code of Practice, issued in 1991, to the 2007 version, for example, there is a significant change in both the advice and the language. The HFEA initially adopted a neutral stance regarding parental disclosure: it required centers to take account of, “a child’s potential need to know about their origins and whether or not the prospective parents are prepared for the questions which may arise while the child is growing up.” 79 By contrast, in 2007 the Code’s advice is, “There is evidence that finding out suddenly, later in life, about donor origins can be emotionally damaging to children and to family relations….The centre should encourage and prepare patients to be open with their children from an early age about the circumstances of their conception.” 80
This move towards openness in the form of telling children they are donor-conceived is reflected in guidance in other countries. For example, from advocating donor anonymity in the early 1990s, the ASRM in its 2018 guidance on donated gametes, “strongly encouraged … [parental] … disclosure to donor-conceived persons of the use of donor gametes or embryos in their conception.” 81 When the 1990 Act was amended in 2008, this specific guidance was given statutory reinforcement, emphasizing: “the importance of informing any resulting child at an early age that the child results from the gametes of a person who is not a parent of the child.” 82 The current HFEA Code of Practice states: “The centre must give patients seeking treatment with donor gametes and embryos information about the importance of telling any resultant children, at an early age, of their donor-conceived origins.” 83
Revising the 1990 Act
Over time, donor anonymity was challenged, both in the UK and internationally, and there was pressure on the HFEA and the Department of Health to reconsider the legal protection of donor anonymity. In 2002, in the case of Rose v Secretary of State for Health and Human Fertilisation and Embryology Authority (Rose), it was acknowledged that Article 8 of the European Convention for the Protection of Human Rights and Fundamental Freedoms 1950 (Article 8) was engaged with regard to identifying and non-identifying information about a biological parent. 84 In Odièvre v France, the European Court of Human Rights stated that, “people have a right to know their origins, […] derived from a wide interpretation of the scope of the notion of private life” enshrined in Article 8. 85 However, some argued that Article 8 could be engaged with respect to recipients’ and donors’ privacy, 86 and therefore it was unclear whose rights would take priority if there was a conflict. Nevertheless, in 2004, the Disclosure of Donor Information Regulations was made in the UK, 87 which provided that, at 18, those conceived by donations made after 2005 would be able to access identifying information recorded on the HFEA register about their donor. This, arguably, was a recognition of the importance of the donor to donor-conceived people and heralded the incorporation into legislation of further elements of the person model, where the interests of the (adult) person born as a result of reproductive donation were given more consideration.
In addition to these changes to donor anonymity, there were calls in the mid-2000s for further reforms 88 and the Human Fertilisation and Embryology Act 2008 amended the 1990 Act 89 to provide for greater access to information for donor-conceived people. 90 The main changes were: the reduction of the age at which donor-conceived people could request non-identifying information (from 18 to 16); 91 donor-conceived people (at age 16) were able to ask for information on the number and sex of any people conceived from the same donor; 92 and (from 18) to ask for identifying information about them, as long as all parties consent to the disclosure. 93 In addition, donors were permitted to request the number and sex of any offspring produced from their donation and recipients could apply for non-identifying information about the donor and any donor-conceived children born from the same donor. 94 These revisions to the 1990 Act indicated the increasing importance given to the longer-term consequences of reproductive donation and hence elements of the person model became more visible in legislation. However, there were (and remain) caveats and limitations to this.Reference Jones, Wallbank, Choudhry and Herring 95 For example, the 1990 Act (as amended) still seeks to protect the family unit by preventing access to information before 16 and 18, preventing contact between the donor and the donor-conceived person during childhood and not providing access to information on the donor’s legal children — and unless bringing a known donor, keeping recipients and donors anonymous to each other.
Other jurisdictions, notably Victoria in Australia, have followed a similar path of grounding their legislative approach to reproductive donation largely in the clinical model and then moving towards the family and person models. However, Victoria has arguably gone much further than the UK and has incorporated elements of the network model. Victoria set up the Victorian Assisted Reproduction Treatment Authority (VARTA, the Victorian equivalent of the HFEA) in 1988. This established the first centralized register of information for those who had donated reproductive material and, like the UK, subsequent iterations of the law granted donor-conceived people greater access to information about their donor. Anonymity was abolished in 1995, and this came into force for donations made after 1998, and in 2016 an amendment to the 2008 Act was passed that allowed all donor-conceived people, irrespective of when the donation had been made, to access identifying information about their donor even if the donor had donated under conditions of anonymity (i.e., pre-1998). As well as the Central Register, in which information is statutorily controlled, VARTA also has a voluntary register. 96 This voluntary register enables donor relatives and descendants to log their information and details so that they can make matches with donor-conceived people who may be related to them (under certain conditions and mutual consent). This retrospective abolition of donor anonymity, and the provisions for descendants and wider relatives to access a voluntary register, arguably move the approach taken in Victoria firmly into the network model of reproductive donation.
In the US, regulation is at state level and many US states have been reluctant to mandate policies on information giving, allowing clinics to offer different types of donation programs and donors to choose how they wish to donate. As Cohen et al. note, “the US has, until recently, been an outlier providing no legal right for a donor-conceived child to access information about the gamete donor.”Reference Cohen, Adashi and Mohapatra 97 Arguably, the dominant model of reproductive donation in the US is a clinical one, where donation is anonymous, and records and information about the donor are not available to donor-conceived people. There are, however, identity release programs where donors can choose to donate under conditions of non-anonymity, and it is estimated that about one third of donation programs in the US offer this.Reference Scheib, Ruby and Benward 98 The US regulatory landscape has begun to change since the 2010s, with California, Washington, and Utah passing laws that mandate the collection of donor information, both identifying and non-identifying, and this is available to donor-conceived people when they are 18. However, these regulations allow the donor to formally opt out of allowing provision of their identity to donor-conceived people, and in that case only non-identifying information can be released. 99 Colorado is the first state to pass a law, in 2022, that mandates both the collection of identifying information about the donor and that it be provided to the donor-conceived person on request at 18. 100 This state-enforced provision of identifying information is a significant departure from previous regulation in the US, and embodies a person model of reproductive donation. Whether Colorado’s law heralds a change in the US towards enforcing identity release donation remains to be seen, but it is probably unlikely given the presumption towards allowing participants and professionals to choose how they wish to access and organize reproductive donation. 101 However, the establishing of the mandatory collection of information about the donor in Washington, Utah, and California, even if that cannot be given to the donor-conceived person if the donor opts out, is a significant development and signifies a move away from the clinical model of reproductive donation in these jurisdictions.
The psychosocial models have gained ascendancy in the academic and practitioner literature, and this move away from the clinical model of reproductive donation has, to some extent, been reflected in regulation and professional guidance internationally. However, this has not been a seamless progression, and the HFE 1990 Act (as amended) in the UK, for example, is made up of a patchwork of models,Reference Brazier 102 with elements of the clinical,Reference Pattinson 103 family, and person models all being visible.
The Emergence of the Network Model
In the previous section, it was shown how the typology of models of reproductive donation can further understanding of regulatory and oversight approaches to information giving. In this section I will use the models to explicate recent trends and changes in the landscape of reproductive donation and draw out the challenges for regulation and oversight. The area of reproductive donation rarely stands still, and since the 2010s, the network model — a subset of the psychosocial model, which gives importance to the wider relationships created by reproductive donation across the life course — is gaining prominence in contemporary practice. As with all the shifts and developments in donor conception, it is hard to pinpoint exactly when this started, but articles discussing these trends began to appear from the 2010s onwards.Reference Borry 104 There was more focus in the literature on the adults created by reproductive donation and the wider family networks in which they sit, arguably a reconsideration of what kinship means.Reference Hertz 105 As Nordqvist and Gilman argue, there has been a significant “opening up” of family life in recent decades, with greater social acceptance of non-traditional families and new family forms increasingly recognized in law (same-sex relationships for example). As they note, “New family forms introduce new forms of connectedness that go beyond the bounds of the ‘traditional family.’”Reference Nordqvist and Gilman 106 In the area of donor conception, one way this is experienced is the greater importance given to the wider kinship relationships created by reproductive donation. The network model is fueled by the ability to search for donor relatives, and even discover that one is donor-conceived, via DTCGT. The growth in DTCGT technology coincided with this increased focus on the importance of wider kinship networks, and this ability to find wider donor relations via this technology encouraged, but did not create, this interest in wider networks.
There are also other ways in which reproductive donation is being used that broaden the conception of family and enable people to construct their own networks of relationships — for example, informal sperm donation outside of the clinic.Reference Taylor 107 This, too, is facilitated by social media and networking sites, such as Pride Angel where people who want to donate and those seeking donors can make connections. 108 As Gilman and Nordqvist have noted,Reference Gilman and Nordqvist 109 the ability for recipients to decide what kind of relationship they have with their donor, and for donor-conceived children to access identifying information about the donor before age 18, is not supported by UK regulation or most identity release donation programs in the US, 110 unless recipients bring a known donor.
Recognizing that questions over information giving in reproductive donation are being influenced by developments outside the control of regulators and clinics, how best to respond to these trends represents a pressing challenge. This challenge has been recognized by organizations such as ESHRE, who issued guidelines on information giving in reproductive donation in 2022. This guidance highlighted the implications of DTCGT for donor conception and recommends that all parties are fully informed about the possible implications of DTCGT for them and their families — namely, that no one’s identity can be guaranteed to remain unknown.Reference Kirkman-Brown 111 For jurisdictions that proscribe anonymity, donors may not be able to remain anonymous, as people are able to circumvent regulatory prohibitions on information sharing. The challenge of DTCGT was also noted by the HFEA. Their Legislative Reform Advisory Group, established in March 2022 to support the HFEA’s review of the 1990 Act, 112 produced a paper that noted the challenges for regulators as follows:
The [1990] Act’s framework of anonymity as default with managed information release via the HFEA risks being overtaken by technological change. It gives assurances to donors, donor-conceived people and their parents that their status in relation to donor conception, their identity and other information will stay confidential until the legal framework permits it to be disclosed, while in reality, the independent exchange of relevant information can freely and legally take place outside of the Act’s control. 113
Consequently, the HFEA launched a consultation in 2023 to consider how they, as a regulator, should respond to these developments. 114 As Cohen et al. note, similar factors have raised questions about regulatory reform in the US. 115 Hence, elements that I have determined to be part of the network model are on regulators’ radar and they need to consider how to respond, if at all, to these developments.
The typology of models of reproductive donation I have outlined can help regulators determine how to respond to these developments. The models can provide clarification of what is at stake and thereby provide a basis for coherent and justifiable approaches to information giving in reproductive donation. The models can help frame discussion over the “best,” most ethically defensible way of organizing reproductive donation. If an argument is made that the clinical model is the most defensible model, then policies that maintain donor anonymity (as far as possible) could be instituted or maintained. However, if a network model is seen as the most ethically defensible model, then policies that move towards the removal of donor anonymity — enabling donor-conceived people to have identifying information about their donor, and have this information earlier — and see the importance of wider donor relations can be instituted. As I stated, the purpose of this paper is not to advance an argument for which model is ethically preferable — this is a debate for another time. But being clear on what is at stake allows the debate to begin over what ethical reproductive donation looks like and subsequently how such a model could be enshrined in regulation.
Conclusion
This paper has developed a novel typology of models of reproductive donation, dividing conceptualizations of reproductive donation into two main models: the biomedical models, the bioscientific and the clinical models; and the psychosocial models, the family, person, and network models. These models reflect what has happened in practice and policy and provide a conceptual framework, a useful heuristic, for understanding reproductive donation and critiquing regulatory and oversight approaches. Further, by distinguishing between different conceptualizations, the models establish a clearer language for academic and professional debate. By clarifying underlying assumptions and making visible dimensions of reproductive donation, this can serve as a foundation for subsequent theoretical advancement in the field.
Debates over information giving in reproductive donation are unlikely to ever be settled as technology and society evolve, continuously challenging regulators and no doubt generating new models of donation. Further, there are different views on the ethics of donor conception and whose interests should be prioritized, and hence disagreement about the appropriate form and type of information giving. Most regulation and oversight has developed in an ad hoc, responsive way, with no overriding vision of what model of reproductive donation should be championed. This paper’s primary contribution lies in making explicit the often-implicit conceptual foundations underlying regulatory and oversight practice. By clarifying how reproductive donation is conceptualized, policy makers can move beyond ad hoc responses toward principled decision-making about what is an optimal model and how that can be translated into regulation. Determining the “best” model of reproductive donation remains a matter for ongoing debate. However, having a clear conceptual foundation is essential both for academic discussion and developing coherent, forward-looking regulation and oversight that can anticipate rather than merely react to technological and social developments.
Acknowledgements
I would like to thank the editor and the two anonymous reviewers for their helpful comments on this paper, and Caroline Redhead, Sarah Devaney, and Alex Mullock, who read earlier drafts.
Disclosure
This article was funded by UKRI ESRC grant number ES/VOO2430/1.

 Open access
Open access