


Introduction
The role of pharmaceutical companies in promoting overuse of opioids has been well-documented,Reference Van Zee1 but little has been written about the effect of covert marketing on medical discourse. Marketing messages, including key phrases, have been seeded into journal articles, continuing medical education (CME), prescribing guidelines, educational activities, and professional society recommendations.
Terms generated or redefined by the pharmaceutical industry created a framework for promoting opioids. This paper will focus on the terms opiophobia, pseudoaddiction, breakthrough pain and pain is the 5th vital sign. The reframing of incipient opioid use disorder as tolerance and dependence will also be discussed. Our analysis draws in significant part from documents disclosed in litigation against opioid manufacturers. These cases have not only held the companies accountable for their actions but have provided an important source of information on the covert marketing strategies used to promote opioids.
An Epidemic of Pain and Opiophobia
Opioid manufacturers persuaded clinicians that chronic pain was a widespread, disabling, and undertreated epidemic and that opioids were a safe and effective treatment. A key concept was opiophobia, which was presented as the wrongheadedness of physicians reluctant to prescribe opioids for common chronic pain syndromes. Opioids are appropriate for end-of-life care, cancer-related pain, and some acute pain, but manufacturers convinced physicians, against the evidence, that opioids were also appropriate for chronic pain syndromes. Physicians who were reluctant to treat arthritis or back pain with opioids were portrayed as out-of-date providers who deprived patients of the best care.
The term opiophobia was introduced in a chapter from the proceedings of a 1981 conference sponsored in part by drug companies,Reference Morgan and Kagan2 and expanded upon in the article “American Opiophobia: Customary Underutilization of Opioid Analgesics.”Reference Morgan3 Opiophobia was described as “an irrational and undocumented fear that appropriate use will lead patients to become addicts”Reference Morgan4 and result in unnecessary pain for patients undertreated with opioids. The term gained traction in the 1990s. In the medical literature, opiophobia was linked to poor clinical performance among doctors and nurses,Reference Lander5 undertreatment of cancer pain,Reference Zenz and Willweber-Strumf6 inadequate medical education,Reference Schnoll and Finch7 an oversight in the field of bioethics,Reference Rich8 and psychologic characteristics of medical students that “were associated with reluctance to prescribe opioids.”Reference Weinstein9
In 2002, a report by “an international panel of pain specialists” titled “Opiophobia as a Barrier to the Treatment of Pain”Reference Bennett and Carr10 stated that “irrational fear of the drugs often impedes their appropriate use.” The report asserted that “opioids are often the most effective treatment for patients with moderate to severe chronic pain.” The term opiophobia even appeared in World Health Organization guidelines on children’s pain released in 2012.Reference Clark and Rogers11 After a US Congressional report exposed the opioid industry’s influence on the guidelines in 2019, the WHO retracted them.Reference Dyer12
Medical discourse also emphasized the debilitating effects of chronic pain.Reference Webster13 The concepts that pain was undertreated, that opioids were underused, and that risks of opioids were exaggerated rehabilitated the reputation of opioids, causing opioid prescribing for nonchronic cancer pain to skyrocket in the 1990s and 2000s.Reference Atluri14
Ophiophobic clinicians, however, apply principles of judicious prescribing, relying on evidence-based best practices. Substantial evidence supports the harms of long-term opioid use.Reference Kotlińska-Lemieszek and Żylicz15 A recent systematic review of 96 randomized controlled trials with 26,169 participants found that opioids barely bested placebos for noncancer pain. In comparative trials, the analgesic effects of opioids were similar to the effects of nonsteroidal anti-inflammatory drugs, tricyclic antidepressants, and anticonvulsants.Reference Busse16
Wrangling the Reluctant: Pain as the 5th Vital Sign
Marketing strategies include the use of drug representatives,Reference Fugh-Berman and Ahari17 articles in medical journals,Reference Fugh-Berman and Melnick18 and educational activities19 featuring paid influencers called key opinion leaders (KOLs) to persuade peers about the benefits of opioids. KOLs have been viewed as objective and reliable sources of information. The term key opinion leaders, according to the pharmaceutical industry, is “a convenient shorthand for those people — usually eminent, usually physicians — who we co-opt into our development and marketing strategies.”Reference Watermeadow20 Because physicians rely on experts to provide clinical recommendations in articles, guidelines, and educational activities, activating KOLs is a key strategy for shaping perceptions of a product’s benefits and harms, as well as perceptions about competing products.
Regulatory and legislative bodies were affected by webs of influence woven by pharmaceutical companies that included licensing boards, universities, nongovernmental organizations, professional societies, and patient advocacy groups.
The term pain as the 5th vital sign was introduced by the industry-funded American Pain Society (APS) in 1996Reference Campbell21 and later copyrighted.22 The term ranked pain as equal in importance to respiration, pulse, temperature, and blood pressure. This is a catchy but flawed framing; pain is a symptom that a patient feels, not a sign that is visible or measurable.
The Veterans Health Administration launched a national pain management strategyReference Stephenson23 based on the concept in 1999 and distributed a Pain as the 5th Vital Sign toolkit24 for its implementation. An APS-backed campaign subsequentlyReference Dahl25 persuaded the Joint Commission (formerly JCAHO: Joint Commission on Accreditation of Healthcare Organizations) — an organization that accredits hospitals and other healthcare facilities — to implement pain screening standards, including industry-influenced educational programs on opioids, in 2001.Reference Berry and Dahl26 Shortly thereafter, questions regarding pain treatment were part of the initial Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) Survey, an influential patient perspective survey, scores of which were used to determine federal reimbursement rates.Reference Rummans27
Purdue Pharma’s 2001 internal OxyContin marketing report makes it clear that pain as the 5th vital sign was a marketing initiative: “Corporate initiatives and partnering efforts were very successful with the Veterans Administration, American Pain Society, and JCAHO in an effort to make Pain: The 5th Vital Sign. This ‘call to action’ was an important promotional initiative for Purdue Pharma. In addition to building sales for OxyContin Tablets, it also positioned Purdue as the leader in pain management education.”28
The concept of pain as a vital sign that needed treatment influenced regulatory bodies, which also came under pressure to prioritize pain management with opioids. In 1998, the US-based Federation of State Medical Boards (FSMB) issued model guidelines drafted by a committee that included the APS and many other industry-supported groups.Reference Joranson and Gilson29 The FSMB’s guidelines supported opioids as first-line treatment for chronic pain, even when a person had a history of substance abuse.30 In response, state medical boards, which had previously opposed expanded use of opioids, began to reduce restrictions on opioid prescribing for noncancer pain in the late 1990s.Reference Manchikanti31 Because most medical care is regulated at the state level through medical boards, there were virtually no other options to rein in the dramatically increasing doses of opioids being prescribed.
The FSMB updated the guidelines in 2004, defining undertreatment of pain as inappropriate medical care.32 This perverse incentive meant that rather than fearing disciplinary action for overprescribing opioids, physicians were warned of sanctions for underprescribing opioids. FSMB guidelines were then used by opioid manufacturers to threaten physicians with potential disciplinary actions. Cephalon, which manufactured a fentanyl lollipop, trained their speakers to convey the point that doctors could be punished if they failed to use opioids to treat pain.33 The FSMB itself accepted more than $1.5 million from Purdue, Endo, Cephalon and Mallinckrodt (an opioid distributor) between 2001 and 2011.34 Documents revealed in litigation show that Purdue Pharma sponsored and drafted the FSMB’s Responsible Opioid Prescribing, a handbook that was ultimately distributed to over 700,000 practicing physicians.Reference Miller35 The guide claimed that opioids improved function and suggested that signs of addiction actually reflected undertreated pain, which was best addressed by increasing the dose of opioids. With funding from Endo Pharmaceuticals, the guide became the basis for an online continuing medical education course.Reference Fauber36
The medical community’s acceptance of pain as the so-called 5th vital sign vastly increased opioid prescribing for chronic noncancer pain. With the FSMB and state medical boards on board, prescribing restrictions for opioids were loosened. Between 1997 and 2007, retail sales of oxycodone increased by 866% and hydrocodone increased by 280%. The total number of immediate-release opioids dispensed by outpatient pharmacies in the United States increased from 164.8 million to 234 million between 2002 and 2009; dispensing of extended-release opioids increased from 9.3 million to 22.9 million.Reference Manchikanti37
The successful promotion of opioids caused the United States to become the world leader in opioid consumption, followed by a steady rise in prescription opioid-related deaths from 1999 to 2016.Reference Kolodny38
Redefining Breakthrough Pain
Cancer patients on round-the-clock opioids may experience end-of-dose or breakthrough pain when opioid effects are wearing off, a problem usually dealt with by decreasing dosing intervals. The concept that breakthrough pain was a distinct type of pain that needed separate treatment was created and fostered by manufacturers of rapid- and short-acting fentanyl preparations. Fentanyl medications that are effective for only 45 minutes are useful for endoscopies, wound debridement, and other brief invasive procedures, but this is a very limited market.
Breakthrough pain was first defined in the medical literature by Russell Portenoy in 1989.Reference Portenoy and Hagen39 Just months before, a case report on the successful treatment of breakthrough cancer pain with transmucosal immediate release fentanyl (TIRF) appeared in the journal Anesthesiology. Reference Ashburn40 One of the authors was chairman of the board of the company that would market the first approved drug for breakthrough pain. A year later, Portenoy reported that breakthrough pain was a frequent “clinical problem, and supplemental opioid doses are … now commonly recommended” and alluded to patients who find “the onset of action of an oral dose is too slow.”Reference Portenoy and Hagen41 A new pain category was thus created to make a niche for TIRFs. In 1998, the FDA approved Actiq as the first in class for breakthrough pain in cancer patients.
In 2006, a buccal lozenge (Fentora) manufactured by Cephalon was approved. The company looked to expand the drug indication to noncancer breakthrough pain. With funding from Cephalon, Portenoy published a survey suggesting “that breakthrough pain in opioid-treated populations with noncancer pain might be similar to cancer-related breakthrough pain.”Reference Portenoy42
There is no evidence that short-acting fentanyl is useful in noncancer pain,Reference Manchikanti43 but Cephalon sponsored CME activities that claimed there was no difference in breakthrough pain experienced by patients with or without cancer. In 2007, a Cephalon-funded continuing medical education activity sponsored by Boston University School of Medicine declared that short-acting opioids were first-line treatments for breakthrough pain, and while other analgesics or nonpharmacological interventions may be helpful, transmucosal fentanyl was better for “treating unpredictable incident BTP and idiopathic BPT [sic].”Reference McCarberg44 Cephalon promoted Fentora off-label for non-opioid-tolerant patients with migraines, sickle cell pain crises, and injuries: the company’s mantra was “pain is pain.” In 2008, Cephalon was fined $425 million for marketing Fentora and two other drugs for unapproved uses.45
Teva, which acquired Cephalon, also promoted off-label uses through CME events, sponsored journal supplements, and KOL programs that positioned Fentora as a safe, effective, and appropriate treatment for non-cancer breakthrough pain.46
Other companies soon jumped on the breakthrough pain bandwagon. In 2012, Subsys, a sublingual fentanyl spray produced by Insys Therapeutics, was approved for cancer patients with breakthrough pain. Insys took opioid marketing to new depths of illegality.Reference Hughes47 John Kapoor, who founded Insys Therapeutics and later served two years in prison for his actions, held daily meetings to discuss new schemes for bribing physicians to increase Subsys prescriptions. Physicians were offered money, purportedly for lecture fees, but were evaluated based on how much Subsys they were prescribing and dropped if they didn’t meet the requirements. The Insys Reimbursement Center misled insurers, implying that they were calling from a prescriber’s office regarding a patient with cancer-related breakthrough pain when they were actually facilitating prior authorization approval for Subsys prescriptions for patients with noncancer pain, an off-label use.48
Teva funded a 2016 Delphi study to generate a consensus on breakthrough pain management. All authors were Teva employees or received support from Teva. Their article concludes that fentanyl is the optimal drug to treat breakthrough cancer pain and that patients could titrate their own doses at home.Reference Boceta49
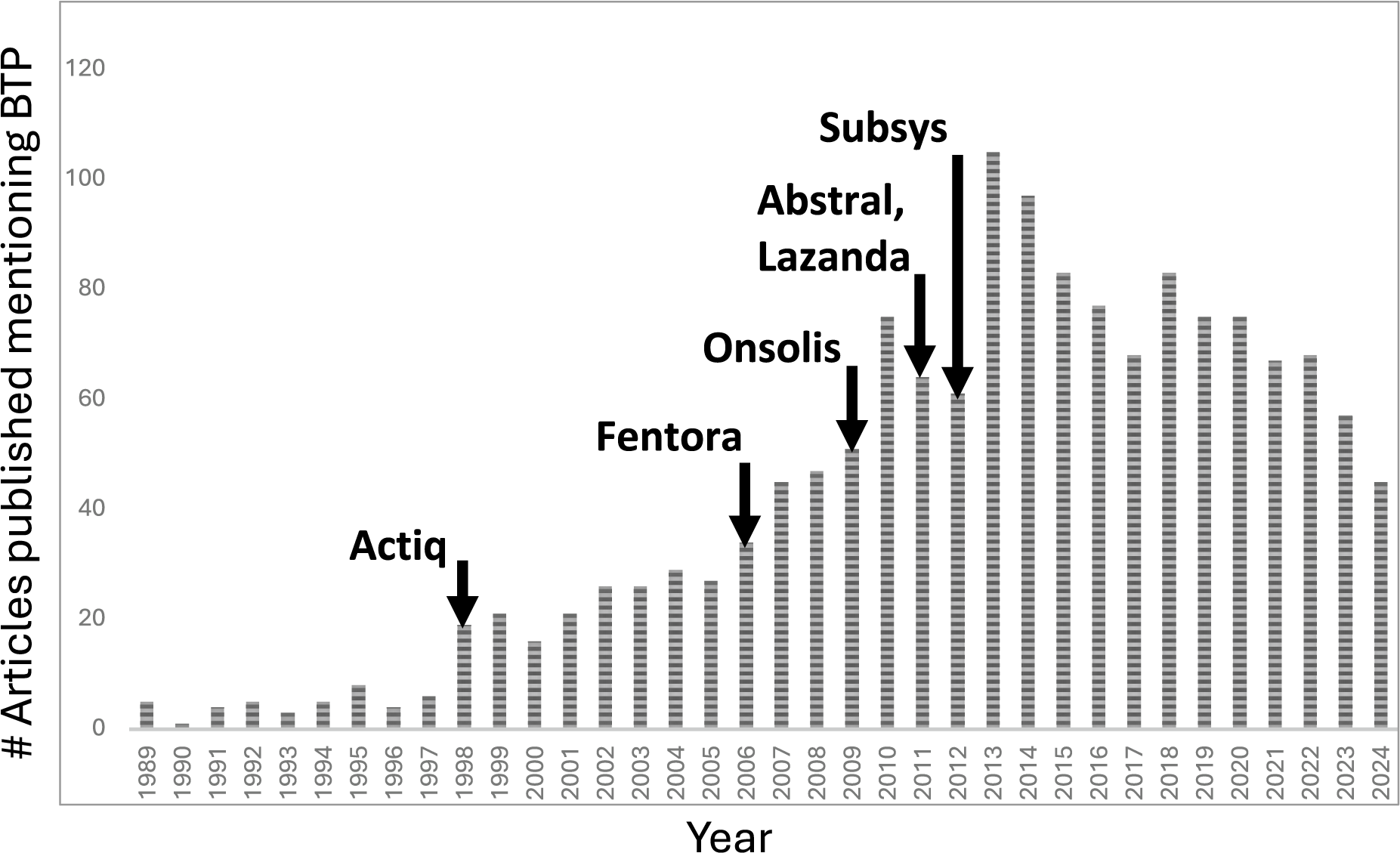
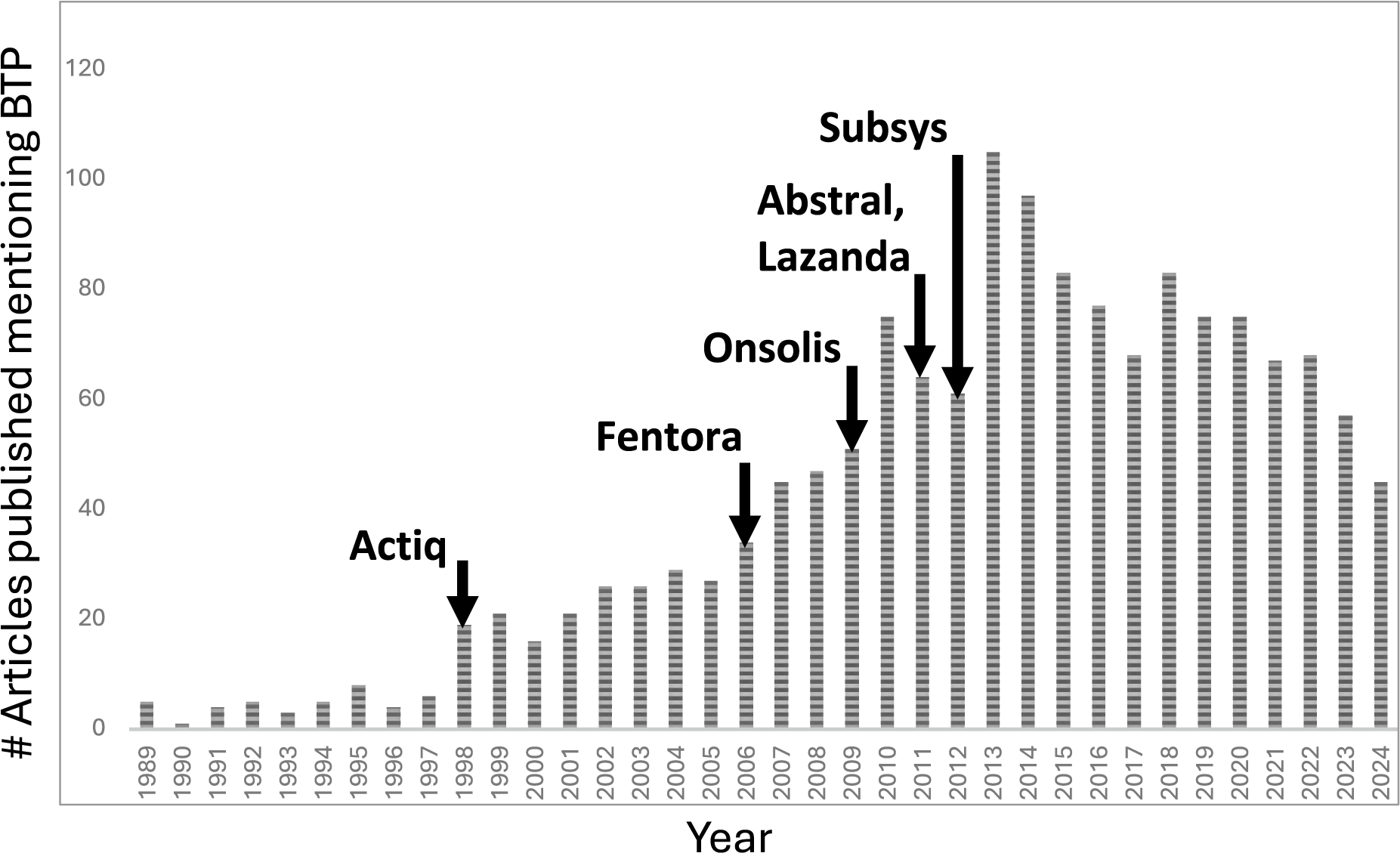
Breakthrough pain has become an accepted diagnosis. In PubMed, the term breakthrough pain increased from 5 publication mentions in 1989 to 105 mentions in 2013; by 2023, the term continued to appear frequently, with 57 mentions that year (see Figure 1). As of September 2024, transmucosal immediate release fentanyl products have been taken off the market.Reference Tin50
Breakthrough pain in medical literature. Arrows signify the date fentanyl-based drugs received FDA approval for breakthrough pain.
Pseudoaddiction: Renaming Addiction
After opioid manufacturers successfully cajoled physicians into overprescribing opioids for chronic pain, many patients who took opioids exactly as prescribed became addicted.Reference Han51 The opioid industry’s reaction was to confuse physicians into thinking that what they were seeing was not true addiction. David Haddox, who went on to become a Purdue Pharma executive, created the term pseudoaddiction to allay clinicians’ fears.Reference Weissman and Haddox52
A 2007 Purdue Pharma presentation on Medication Therapy Management, exposed in litigation against Purdue, assured doctors that symptoms of pseudoaddiction emerged because “opioids are frequently prescribed in doses that are inadequate.”Reference Compl53 As David Haddox put it, “unlike true opioid psychologic dependence where the underlying cause is unknown, pseudoaddiction is an iatrogenic syndrome caused by the undermedication of pain.”Reference Weissman and Haddox54
Purdue Pharma promoted the concept of pseudoaddiction via a 2008 pamphlet named Clinical Issues in Opioid Prescribing, which stated, “Patients with unrelieved pain may become focused on obtaining medications, may ‘clock watch,’ and may otherwise seem inappropriately ‘drug-seeking.’ Even such behaviors as illicit drug use and deception can occur in the patient’s efforts to obtain relief. Pseudoaddiction can be distinguished from true addiction in that the behaviors resolve when the pain is effectively treated.”55
The diagnosis of pseudoaddiction allayed clinicians’ discomfort with continuing to prescribe opioids to patients with clear signs of addiction. In 2011, Purdue Pharma also released Providing Relief, Preventing Abuse, a pamphlet supporting the idea of pseudoaddiction, which had purportedly “emerged in the literature.” The pamphlet associated opioid abuse with “track marks and perforated nasal septa,” thus reassuring physicians that patients who weren’t snorting or injecting opioids couldn’t be addicted.Reference Compl56
The FSMB’s Responsible Opioid Prescribing also discussed pseudoaddiction, claiming that signs of addiction reflect undertreated pain.Reference Compl57
No medical evidence supported the idea that patients who exhibited addictive behavior were only acting out because they were in pain, but the concept reassured prescribers that increasing opioid doses in patients with signs of addiction, including illicit drug use, was acceptable because the patient was suffering not from addiction, but from pseudoaddiction. The treatment was increasing opioid doses.
Key opinion leaders helped promote the concept of pseudoaddiction. For example, Lynn Webster received funding from opioid manufacturers and authored multiple CME activities, sponsored by Endo, Cephalon, and Purdue Pharma, that promoted the concept of pseudoaddiction. In 2007, Webster coauthored the book Avoiding Opioid Abuse While Managing Pain, which directed physicians to respond to patients with aberrant behavior by first increasing opioid doses.Reference Webster and Dove58 Later, Webster recanted his support for the concept of pseudoaddiction,Reference Fauber59 but the concept had already taken hold.
In fact, pseudoaddiction equals addiction. In 2015, a non-pharma-funded review of pseudoaddiction identified 224 articles that mentioned pseudoaddiction, but found no empirical validation of the concept. The authors expressed concern that the term remained widely accepted.Reference Greene and Chambers60
Tolerance, Dependence, and Addiction
Pharmaceutical companies sought to normalize warning signs of opioid use disorder by describing dependence and tolerance as normal, adaptive states. In fact, both dependence and tolerance are diagnostic criteria for substance use disorder.61 The DSM-V, in contrast to the DSM-IV, appends the curious note that tolerance and withdrawal should not be counted as criteria for diagnosis “for those taking opioids solely under appropriate medical supervision.”
Statements such as “physical dependence is a neuropharmacological phenomenon as a result of neuroadaptation and neuroplasticity, in contrast to addiction that is both neuropharmacological and behavioural”Reference Mehta and Langford62 were used to persuade physicians that patients showing prodromal signs of opioid use disorder were behaving normally. Misleading statements were made comparing opioids to insulin, antihypertensives, or asthma medication: for example, “a patient could become physically dependent on corticosteroids to treat asthma, but one would not call this patient addicted to steroids.”Reference Heit63
Tolerance refers to physiological adaptation that results in the need for increasing doses of opioids due to decreased effectiveness of a given dose. About 28% of chronic opioid users will require increased doses that are not related to progression of the underlying disease.Reference Lembke64 Escalating doses is dangerous, because while tolerance develops to therapeutic effects, tolerance does not develop to serious adverse effects: respiratory depression and other overdose risks are dose-related.Reference Lembke65
Opioid manufacturers said exactly the opposite. Purdue’s guide Providing Relief, Preventing Abuse explained, “Tolerance to the respiratory depressant effects of opioids is what allows a patient with pain to regularly take a dose of medicine that would be fatal for someone who wasn’t taking the same medicine on a regular basis.”66 Purdue trivialized tolerance while failing to acknowledge the risks associated with increasing dosages of opioids. In a Purdue-sponsored study, the authors asserted that the tolerance developed by patients needing higher and higher doses of opioids “was not a clinically significant problem when managing patients with opioids long-term.”Reference Caldwell67 In fact, Purdue encouraged increasing doses of opioids. The concept of “titrating up” was promoted under the rationale that a patient who needed a higher dosage of opioids to manage pain was either experiencing disease progression or had increased physical activity so much that opioids must be increased to keep up: “The opioid medications have increased the patient’s functional activity and therefore the opioids have to be titrated to the new functional activity.”Reference Heit68
Increasing opioid doses was normalized and even compared to hypertension and diabetes medications. “The concept is the same as titrating blood pressure medicines or insulin to achieve the desired effect.”Reference Heit69
The concept that there was no maximum dose of opioids was an important part of Purdue’s marketing strategy. No dose of opioids was too high. Purdue Pharma influenced WHO guidelines that stated that “there is no maximum dose for opioids—even in the case of children.”Reference Clark and Rogers70
Opioid Promotion Continues Today
Pharmaceutical companies continue efforts to persuade physicians to prescribe opioids inappropriately. In 2023, one author (AK) attended a medical school lecture that described pseudoaddiction as a real concept. The term opiophobia continues to appear in recent medical literatureReference Ayoub71 and popular media.Reference Achenbach and Bernstein72 And marketing messages that distort the benefits and harms of opioids have been identified in recent industry-funded CME.Reference Goodwin73
Discussion
Language is important. By using KOLs, medical publications, CME activities, medical societies, and public health organizations to manipulate medical concepts and medical language, the pharmaceutical industry created conditions favorable to marketing targeted drugs without being identified specifically as marketing. Opioid pharmacotherapy provides an instructive case study in industry control of medical knowledge. Opioid manufacturers unethically changed what prescribers thought they knew about opioids, and changed how chronic pain was treated.
Chronic pain was cast as an undertreated epidemic, and opioids emphasized as a safe and effective treatment for chronic pain. By inventing new terms and redefining others, opioid manufacturers changed what physicians thought they knew. Physicians were persuaded that addiction to opioids was rare and that tolerance and dependence could be used as diagnostic criteria for opioid use disorder only in those taking non-prescribed opioids; for those on prescribed opioids, tolerance and dependence were normalized. The terms dependence and tolerance permitted physicians to overlook early warning signs of addiction, and when the condition became all too obvious, addiction was framed as pseudoaddiction, justifying increased doses of opioids in patients with obvious opioid use disorder. Breakthrough pain was defined as a discrete condition, treatable only by fast-acting opioids. Pain was established as the 5th vital sign, creating a foundation for overprescription of potent opioids on a massive scale.
Conclusion
Pharmaceutical companies affect medical language to enhance sales of targeted drugs. We recommend a broad research initiative into the extent of influence that pharmaceutical companies have had on medical knowledge regarding other drugs and other diseases, national efforts to mitigate this harm, and preventive measures for protecting the integrity of education of physicians and other health care professionals. For both legal and ethical reasons, it is imperative to bar pharmaceutical companies, and the health care professionals they pay, from the education of physicians, other health care professionals, and health professional students.
Disclosures
Aidan Kaspari and Judy Butler have no disclosures. Adriane Fugh-Berman is a paid expert witness at the request of plaintiffs in litigation regarding pharmaceutical marketing practices.

 Open access
Open access