

Introduction
In Iran, women encounter numerous challenges in the workplace, including pay inequity, (1) gender discrimination, and fewer promotion opportunities. (Reference Burn2; Reference Coffman, Exley and Niederle3)Among these, a particularly serious issue, which puts their safety in danger, is sexual harassment. Those subjected to sexual harassment often suffer from depression, anxiety, and other mental health issues, which pose significant risks to their overall health and interpersonal relationships. (Reference Luong and Green4) Additionally, sexual harassment can lead to job dissatisfaction, undermining the efficiency of health care services, and may compel victims to resign, thus jeopardizing their financial stability and career advancement. (Reference Burn2; Reference Kapila5)
Moreover, a critical concern in some regions, such as Iran, is the absence of legal measures criminalizing gender-based harassment in the workplace, leaving many without a legal recourse to challenge their harassers. This lack of legal protection, coupled with insufficient research and data on the subject, especially in the medical field, renders sexual harassment a hidden yet pervasive issue that continues to afflict countless women in their professional environments. (Reference Kapila5–Reference Sadeghi Fasaei and Larijani7) While such misconduct can occur in any workplace, health care services and hospitals are important because sexual harassment not only affects the targeted individuals but also potentially compromises patient care. Given that women constitute a substantial portion of hospital staff and more than 56% of health workers in Iran, sexual harassment can significantly affect overall hospital performance.
Gender in Iran
Iran, officially the Islamic Republic of Iran, located in Western Asia, is a nation with Persian as its official language and divided into thirty-one provinces. (Reference Zeighami, Mangolian Shahrbabaki and Dehghan8) Even though Iranian women have made significant progress in recent years, they still face many challenges in various fields. Although the rate of female literacy in Iran is 90 percent, the number of educated women has increased significantly through the years and they constitute 56% of the students of Iran’s public universities, (9) they continue to face significant obstacles in the job market. The 2023 Global Gender Gap Index highlights Iran’s challenges in gender equality: its score for economic participation and opportunity and the labour force participation rate are low (see figure 22.1). Iranian women are less likely to have roles as legislators, senior officials, and managers. (1; Reference Zeighami, Mangolian Shahrbabaki and Dehghan8–10)
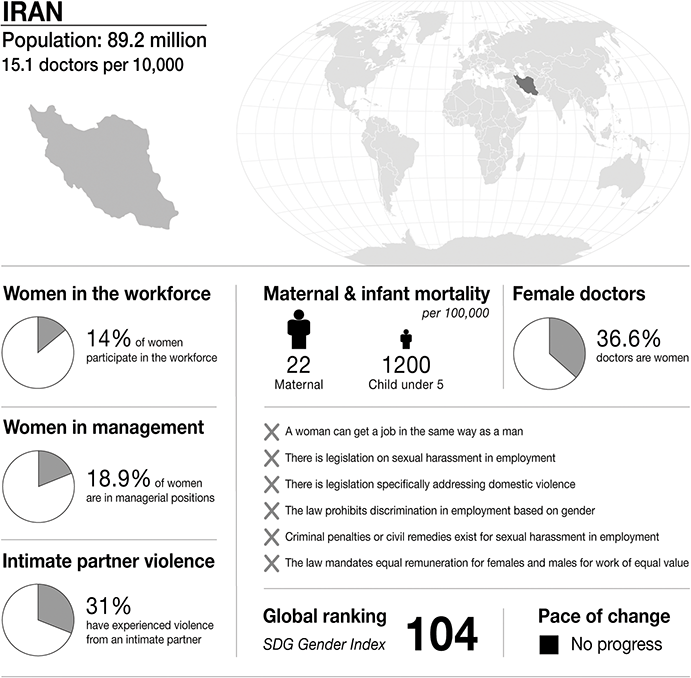
Infographic Iran. Infographics were provided by CartoGIS Services, The Australian National University. Population: from World Bank https://databank.worldbank.org/source/population-estimates-and-projections. Sustainable Development Progress, global ranking and statistics on women in the workplace, women in management and intimate partner violence: from United Nations SDGs Data Portal https://unstats.un.org/sdgs/dataportal. Female doctor percentage: from Global health workforce statistics www.who.int/data/gho/data/themes/topics/health-workforce. Legislation and law statements: from the World Bank gender data portal 2023 https://genderdata.worldbank.org/en/indicators. Maternal mortality statistics: from the Global Health Observatory 2020 https://mmr2020.srhr.org. Infant mortality statistics: from United Nations International Children’s Fund (UNICEF) https://data.unicef.org/topic/child-survival/under-five-mortality.

Figure 22.1 Long description
The infographic provides information about Iran, with a population of 89.2 million and 15.1 doctors per 10,000 people. It highlights several gender-related statistics. 14 per cent of women participate in the workforce. 18.9 per cent of women are in managerial positions. 31 per cent of women have experienced intimate partner violence. Maternal mortality is 22 per 100,000. Infant mortality under 5 is 1200 per 100,000. 36.6 per cent of doctors are women.
The infographic lists the presence or absence of law and policy on gender equality. In Iran:
– a woman cannot get a job in the same way as a man.
– there is no legislation on sexual harassment in employment.
– there is no legislation specifically addressing domestic violence.
– the law does not prohibit discrimination in employment based on gender.
– there are no criminal penalties or civil remedies for sexual harassment in employment.
– there is no law that mandates equal remuneration for females and males for work of equal value.
S D G Gender Index global ranking is 104, and is stable.
The High Council for Human Rights in Iran indicates that women make up 25.2% of public managers across all executive levels, with a total of 19,597 female managers reported in 2020. (9–10) Additionally, Iran’s score for women’s political empowerment is low. (Reference Zeighami, Mangolian Shahrbabaki and Dehghan8) These statistics underscore the profound gender inequalities faced by Iranian women. Despite making up half of the population and outpacing men in literacy and educational achievements, women continue to struggle for equal participation in the labour market and face systemic barriers in political and economic leadership. The disparity remains stark, as discriminatory policies at all levels impede their societal advancement.
Recent Change
The compulsory hijab law in Iran, implemented in the wake of the 1979 Islamic Revolution, mandates women to wear the hijab in public. This regulation has become a focal point of contention and emblematic of broader gender-based restrictions within Iranian society. In recent years, resistance against this mandatory decree has markedly intensified. The tragic death of Mahsa Amini in September 2022, reportedly occurring during enforcement actions by the moral police regarding her hijab, catalysed extensive protests under the banner of ‘Women, Life, Freedom’. This incident provoked widespread outrage within Iran, where existing public discontent towards the government was already pronounced, further galvanizing a sustained and widespread protest movement. Amini’s death resonated profoundly across the nation, precipitating an unprecedented surge of demonstrations against the government. These protests swiftly gained traction, primarily spearheaded by young women advocating for fundamental rights. Significant participation was observed from both men and women, challenging not only the hijab mandate but also broader issues concerning freedoms and rights in Iran. Despite heightened government enforcement of hijab laws and increased penalties for non-compliance, numerous Iranian women persist in their resistance. This ongoing struggle underscores a pivotal facet of the broader campaign for women’s rights and freedoms in Iran. The situation serves as a poignant reminder of the enduring struggle for personal liberties and gender parity amidst stringent societal and legal constraints.
Gender in Medicine
While women have historically comprised the majority of the workforce in health care sectors, primarily as nurses, caregivers, and midwives, their roles have significantly diversified in recent years. According to the Medical Council of Iran, there are approximately 161,000 physicians in the country, with women representing about 71,000 of these. Human rights reports from Iran indicate that 52% of physicians are men and 48% are women.
Furthermore, women dominate certain specialties, comprising 98% of obstetricians and gynecologists, 40% of specialist doctors, and 30% of subspecialist doctors. In the academic sphere, women make up 34% of faculty members in medical sciences. Within the Ministry of Treatment and Medical Education, there are 13,531 women, with 12,883 serving as basic managers and experts, 647 as middle managers, and only one as a senior manager. (9) Despite the increasing number of female physicians and faculty members in medical sciences, leadership roles and higher positions in education remain predominantly male-dominated, reflecting a significant gap in achieving gender equality. (Reference Zeighami, Mangolian Shahrbabaki and Dehghan8; Reference Mosadeghrad11)
Medical Education
In Iran, the integration of health service delivery and health professional education is overseen by the Ministry of Health and Medical Education. This body coordinates with over sixty affiliated universities of medical sciences that provide health care services and are responsible for the education and training of 77% of the health workforce. (Reference Zeighami, Mangolian Shahrbabaki and Dehghan8; Reference Zeighami, Zakeri, Mangolian Shahrbabaki and Dehghan12) The undergraduate medical training in Iran spans seven years, culminating in an MD degree. This programme includes two years of Basic Science Training followed by an examination required to progress to the next phase, three and a half years of clinical training (incorporating theoretical education and hospital placements), followed by ‘Pre-Internship Examination’, which is a requirement to proceed to internship, and an eighteen-month internship period during which students must also complete a research dissertation. Medical students receive hands-on training in specialized hospital wards, under the supervision of board-certified faculty specialists. Upon successfully completing medical school and the dissertation, graduates must register with the Iranian Medical Council and obtain a Licence to Practise. This process also involves fulfilling a government service requirement, which includes military service for male doctors and service in remote areas for female doctors, lasting up to two years for general practitioners and between four to twelve years for specialists.
Sexual Harassment Law in Iran
Iran faces significant challenges regarding legal frameworks that address sexual harassment. The absence of specific laws criminalizing gender-based harassment in the workplace and inadequate enforcement mechanisms often prevent victims from filing legal complaints against their harassers. This lack of criminalization and insufficient enforcement measures, combined with ineffective and non-deterrent punishments, undermine the obligations of employers and the government to prevent sexual harassment and provide necessary training to inform victims of their rights. This education is crucial for preventing workplace harassment. (Reference Rizvani13)
Although Iranian law includes provisions criminalizing certain sexual offences and harassment, these provisions are limited to public disturbances, excluding private settings or work environments. Additionally, Article 637 of the Islamic Penal Code specifically addresses physical sexual intercourse and the implications of physical sexual harassment. According to this article, any sexual act between a man and a woman outside of marriage is considered a crime, and the perpetrators are punished. If a sexual act (sexual harassment) is committed through force or coercion, only the harasser is sentenced to punishment. However, the law requires the accused to confess before a judge, or the victim must present male witnesses to substantiate the claim, complicating the prosecution of such cases, since sexual harassment typically occurs in private places without witnesses. A critical issue is that sexual harassment, particularly in the workplace, lacks a clear definition. Existing laws are inadequate and do not directly address sexual harassment in the workplace. (Reference Rizvani13; Reference Mesri, Farajiha, Azadfallah and Azari14) Notably, existing laws do not cover verbal, non-verbal, or quid pro quo harassment in non-public settings such as workplaces. (Reference Rizvani13; Reference Bagheri15) Therefore, accurately defining and criminalizing sexual harassment in the law is crucial, and organizations should be legally obligated to train, prevent, and protect victims against sexual harassment.
Medical Regulations in Iran
In Iran, doctors who intend to practise must be legally registered with the Iranian Medical Council (IRIMC) and receive a membership/licence number. This licence is valid nationwide, recognizing the individual as a qualified doctor of medicine throughout the country. After successful registration, doctors receive a Membership Card. The IRIMC rigourously verifies each doctor’s identity and qualifications upon registration and maintains up-to-date records of all changes to ensure the accuracy of the medical register. IRIMC members must periodically update their profiles, including photos and contact details, and renew their membership cards every five years.
Additionally, all licensed medical staff must demonstrate their continued competence and ability to provide high-quality care through a relicensing process that also occurs every five years. To be relicensed, doctors must provide evidence of their participation in Continuing Professional Development (CPD) courses approved by the IRIMC or other accredited medical organizations, earning at least 25 CPD credits annually. The IRIMC also supervises doctors’ practices to ensure adherence to medical regulatory requirements and takes disciplinary action if these standards are not met. Actions can range from issuing warnings to suspending or placing conditions on their registration, or even removing a doctor from the register. Furthermore, the IRIMC issues Certificates of Good Standing (CGS) or Certificates of Professional Conduct to active registered members upon request. These certificates are required when doctors seek licensing in other jurisdictions and are issued after assessing the doctor’s disciplinary records, ensuring they are provided in a signed and sealed envelope to maintain confidentiality and integrity. (16)
Case Studies
When we focus on sexual harassment it is important to understand the problem from victims’ points of view and their experiences. In these cases, we encounter two different strategies to cope with sexual harassment. We examine two different cases to show how and why sexual harassment happens in health care environments and how the victims cope.
Case 1
Prelude
Case 1 is about a cosmetic dermatologist who experienced sexual harassment during her internship in a public hospital. Experiencing sexual harassment caused her to eventually leave the hospital and prefer working in a private office where such dynamics were less pronounced.
Assault
The survivor, who experienced sexual harassment while she was a medical intern in a public hospital, recounted her harrowing ordeal. Despite facing sexual assault from multiple individuals, her main harasser was an anesthesiologist in the operating room. She attributed the prevalence of such behaviour to the power dynamics and hierarchical relationships inherent in hospital settings. The victim believes that younger women and medical students are particularly vulnerable to sexual harassment because they have less power and authority within the hospital. Additionally, their relative lack of influence and status makes them prime targets for harassment, exacerbating the challenges they face in these professional environments.
She elaborated on the harassment and sexual assaults in hospital settings: Patients or their relatives ask for your phone number, request dates, or stare at you, but that’s not a big deal. However, when male physicians or colleagues harass you, it’s more intense and lasts longer. It’s not easy to cope with them.
One common form of harassment she encountered involved a group of male colleagues, including an anesthesiology specialist, who made inappropriate jokes about a patient’s private parts. She described the situation:
I had to stay there and listen to their jokes about patients’ private parts, which was disgusting and terrifying. I usually tried to busy myself with files and folders and pretended I wasn’t listening.
She felt unable to object to their behaviour because it would only worsen her situation. ‘I decided not to say anything and just pretended I wasn’t listening to their conversation, instead focusing on the patients’ medical reports’, she explained.
She had a worse experience. The primary perpetrator was the anesthesiologist, who was in his forties and married. He frequently asked her personal questions about her private life. She recounted,
He asked if I was in a relationship, about my family, and what I was going to do tonight. I normally didn’t answer his questions, gave him the cold shoulder, and showed I didn’t want to answer, but that didn’t deter him.
Eventually, he began physically harassing her. Whenever they were alone, he found excuses to come close and touch her. ‘He touched my back and backside or stood too close to me, and his hand touched my body whenever he wanted to explain something. He sometimes told me how beautiful I was’, she stated. She tried to avoid him, giving him the cold shoulder and not answering his questions directly to convey her discomfort, but he remained undeterred.
Feeling trapped, she knew that reporting such incidents often led to victim-blaming and gossip, which would further isolate her. She explained,
I felt terrible because I couldn’t do anything against him. He was famous and powerful, and I couldn’t even prove sexual harassment or physically and verbally confront him because I was a student and afraid of the negative consequences.
Moreover, she believed even if she reported his behaviour, it would not lead to any positive outcomes due to the power imbalance in the hospital.
The hospital environment is characterized by a marked hierarchy, which often influences the handling of sexual harassment incidents. Authority figures typically determine the consequences for harassers based on their position within the hospital. Doctors face no punishment due to their higher status, while nurses or other staff members might be more likely to be disciplined.
She noted that this disparity in handling harassment cases contributes to significant underreporting among women. Many do not report incidents due to the lack of meaningful consequences for perpetrators and the fear of being blamed by colleagues. Moreover, ‘students and interns have no power in hospitals, and other staff don’t care about them and often place blame on them’.
Desperate, she eventually confided in her classmates and a few female colleagues whom she trusted to avoid blame or gossip. ‘After I told my colleagues and classmates, they didn’t leave me alone with him and protected me’, she said gratefully. After some time, she finished her internship and left the hospital.
I was so lucky to have supportive colleagues and friends. In some hospitals, you can’t trust your colleagues because they blame you and spread rumours. When these protective measures fail or can’t be enforced, the situation becomes perilous, leaving victims isolated and unable to seek help or share their experiences.
She lamented the toxic hospital culture, stating,
The problem is that male doctors basically consider themselves the owners of the staff. Many times, a doctor may touch you, and you don’t like it, but because he has more power, you shouldn’t say anything to him; they become rude.
Her experiences underscore the need for systemic change within medical institutions to protect interns and staff from sexual harassment and foster an environment where such abuses of power are no longer tolerated. The reluctance to report harassment is often compounded by the perception that no punitive action will be taken against the harasser, coupled with the fear of exacerbating the situation or facing victim-blaming.
Limbo
At first, the victim believed the anesthesiologist’s touches were accidental, but as the behaviour persisted, she became certain it was intentional and felt increasingly distressed. ‘I just wanted to leave and never come back’, she admitted. Overwhelmed by her situation and the lack of support from hospital management, she doubted that they would act against a well-positioned doctor. She feared that the blame would inevitably fall on her, as it often does on women in similar situations. She described grappling with self-doubt and blame:
I felt terrible and asked myself, ‘Did I do something to make him think I was interested? Why didn’t I scream at him? Why am I so weak?’
These questions reflect the internal turmoil and guilt that victims of sexual harassment frequently endure, further worsening their emotional distress. The victim identified the absence of a formal reporting system as a significant barrier to addressing sexual harassment.
There is no reporting system, and victims have to report directly to managers, who are usually men. It’s not easy to talk about sexual harassment in front of them, especially since most have closer relationships with male doctors.
She believes that the lack of a clear, supportive pathway for addressing such harassment left her vulnerable to further incidents, extending the period during which she was harassed. This scenario highlights a critical gap in many organizational cultures and structures, where inadequate support and unclear reporting mechanisms significantly worsen the impact of such experiences on victims.
Exposure
The survivor in this case managed to disclose the incidents of harassment to a few close colleagues without immediate negative repercussions. She carefully chose whom to confide in, limiting her exposure and potential fallout by sharing her experiences only with those she trusted within her department. Despite this controlled disclosure, the ongoing harassment significantly impacted her wellbeing and professional satisfaction. She experienced a profound sense of job dissatisfaction, feeling that the discriminatory environment was intolerable. Ultimately, these feelings drove her to contemplate leaving the hospital entirely, seeking a workplace where she could feel safe and respected. This decision highlights the emotional and professional toll that sexual harassment can take, even when the immediate circle’s response is not overtly negative.
Aftermath
After enduring sexual harassment in the hospital, the survivor made a significant career shift, leaving the hospital setting to establish herself in the beauty industry and work as a cosmetic dermatologist. Now working from her private office, she feels empowered and in control of her professional environment. Despite this positive change, the residual effects of her past experiences continue to influence her attitudes and behaviours. She expressed a strong aversion to hospital environments and remains cautious in her interactions with male colleagues and coworkers. This cautious approach underscores the lasting impact that such traumatic experiences can have, affecting trust and comfort in professional settings long after the incidents have ceased.
Case 2
Prelude
In Case 2, the victim, after experiencing sexual harassment from a specialist, shared her ordeal with colleagues and classmates, only to discover that they too had suffered similar mistreatment. Together, they reported the incidents to the head nurse. Unfortunately, despite their collective efforts and testimonies, the harasser faced no consequences. This lack of action from the hospital administration led to widespread feelings of depression and job dissatisfaction among the victims. Feeling disillusioned by the ineffectiveness of the reporting system and the apparent impunity enjoyed by the harasser, the victim resolved to never formally report such incidents again. The survivor is a specialist in a private hospital now.
Assault
The victim was a medical student when she experienced sexual harassment from one of the physicians in a public hospital. She describes that the hospital was rife with sexual harassment, ranging from verbal comments and jokes about women’s bodies to inappropriate physical contact. She recounts how sexual jokes, comments about physical appearances, and lewd messages were common, coming from various individuals including male nurses, students, patients, and caregivers. Despite her efforts to confront these behaviours, she often found that her protests either were ignored or exacerbated the situation, leading her to either remove herself from the environment or try to ignore the comments.
Whenever male nurses or students tell jokes, commenting which is about women and harass me, I warn them not to start again, but sometimes I know that no matter how much I protest, they do their own thing or make it worse. As a result, I either go out or do not listen to them.
Her most troubling experiences involved an internist specialist during her internship. This perpetrator not only made sexual jokes but also demeaned women who objected by calling them old-fashioned. His behaviour escalated from verbal harassment to physical actions, particularly during times when fewer staff were present, such as night shifts. He would make comments about women’s bodies and inappropriately touch female staff under the guise of compliments or observations about their weight. The victim vividly recalled the first time this internist commented on her body, suggesting her uniform was fitted to accentuate her figure, which left her feeling shamed and angry. When she objected, he ridiculed her response, intensifying her frustration.
On one occasion, when they were alone, he used the pretense of explaining something to inappropriately touch her back and other parts of her body, prompting her to quickly leave the situation. The survivor explained ‘he wanted to explain something to me about a patient’s medical report and he started to touch my back and other parts of my body. I was shocked and terrified and made an excuse to leave. I felt disgusted and I just wanted to cry.’ The victim explained ‘I got anxious and did not want go to work because of him.’
At first, when he verbally harassed her, she could not understand if it was sexual harassment or not because based on some of her colleagues’ reactions it was ‘normal’ behaviour for men and the victim doubted her feelings, thinking perhaps she was overreacting to what was considered ‘normal’ behaviour. However, the physical harassment was a turning point that made her realize the severity of the situation. She felt depressed and unsure of what to do. After a while, when he continued his harassment, she reached out to other interns and nurses, discovering that many had similar or more severe forms of physical harassment experiences.
Limbo
In a state of limbo, the victim initially struggled with her negative feelings towards the harasser, unable to pinpoint why she felt this way. She recounts that upon reflection, she realized he often made derogatory jokes about women and inappropriate comments about patients and colleagues, which many seemed to dismiss as normal or ‘manly’ behaviour. This normalization within the workplace made her feel confused about her discomfort. When the harasser first physically touched her and made explicit comments about her body, she knew she needed to take action. She expressed regret over her inability to react more assertively in the moment, questioning why she didn’t confront him directly or even retaliate physically. ‘My biggest regret is why I did not do anything, screaming at him or even physical attack, but I did not do anything and just left him to continue his harassment’, she lamented. This paralysis was partly due to not knowing how to handle the situation or where to report his behaviour.
Exposure
Together, the survivor and her close colleagues approached the head nurse, who was sympathetic and advised them to formally report the behaviour so she could escalate it to hospital management. She explained, ‘Because the head of department was a man and his friend, we decided to talk with the head nurse, she told all of us should report his behaviour and she will talk with the managers of the hospital.’
Despite their reports, the outcome was deeply disappointing: the perpetrator was merely transferred to another department without any formal punishment, leaving the victims shocked and concerned that he might continue his behaviour elsewhere. This outcome highlights the challenges victims face in environments where the hierarchy protects the perpetrator rather than supports the victims, illustrating the need for more robust mechanisms to handle such complaints effectively and protect employees from repeated abuse.
Aftermath
In the aftermath of the management’s decision not to discipline the harasser, the victim felt deeply betrayed and became depressed. The lack of consequences for the harasser, despite numerous reports from multiple victims, left her disillusioned with the formal complaint processes. As a result, she resolved to never formally report sexual harassment again, opting instead for a more direct approach: confronting any future harasser verbally and physically. She rationalized this decision by stating, ‘When there is no punishment for harassers and you cannot even sue them in court or other places, the better solution is to defend yourself and make the situation worse for the harasser.’ Determined to empower herself and prevent further incidents, the victim pursued further education and became a specialist, now working in a private hospital. This career advancement was partly driven by her desire to create a professional environment where she could establish clear boundaries. She explained,
I changed my behaviour towards male colleagues and I am so serious in my workplace to show people I do not tolerate unprofessional behaviour and they should know their boundary.
By adopting a more assertive and serious demeanor at work, she aimed to deter inappropriate behaviour and establish herself as someone who could not be easily harassed. This shift in her professional approach reflects a broader strategy of self-empowerment and boundary-setting, illustrating how individuals might adapt to protect themselves in environments where institutional support and justice are lacking.
Discussion
Sexual harassment and assault in the workplace lead to a myriad of negative effects on women’s lives, including mental health impacts, job dissatisfaction, and diminished work performance. Women experience sexual harassment and assault across various workplace environments, but certain settings, such as health care environments and hospitals, exacerbate these issues significantly. In these settings, the repercussions extend beyond the individual victims, decreasing overall hospital efficiency and potentially endangering patients’ lives. Moreover, the societal implications are profound, fostering a culture of fear and insecurity that can deter women and young people from entering the workforce, thereby perpetuating male dominance.
In Iran, the issue of sexual harassment in health care settings requires examination from multiple perspectives. A critical factor is the lack of legal measures criminalizing sexual harassment in the workplace. Despite the significant challenges Iranian women face in changing their societal and familial roles, the prevailing legislative and social frameworks continue to marginalize women’s presence in the workforce. This deficiency in the legal system not only fails to protect victims but also tacitly encourages such behaviours by signalling a lack of consequences for perpetrators. Studies, such as those by Zeighami et al., (Reference Zeighami, Zakeri, Mangolian Shahrbabaki and Dehghan12) highlight that victims often refrain from reporting harassment due to this lack of supportive legislation and policy-making. Another significant issue is the hierarchical and male-dominated nature of workplace structures, particularly in the medical field. Studies by Colenbrander et al. (Reference Colenbrander, Causer and Haire17) demonstrate how the imbalance of power between superiors (typically male doctors) and subordinates can facilitate environments conducive to sexual harassment. In Iran, where the managerial hierarchy within hospitals is predominantly male, such structures enable male doctors to exploit their positions without fear of reprisal. (Reference Mosadeghrad11; Reference Mohajaran, Derakhshan Fard and Sayah18)
Moreover, the typical targets of sexual harassment include individuals who are inherently more vulnerable within the workplace, such as divorced or separated women, young women, women in non-traditional roles, women with disabilities, lesbian women, women from ethnic minorities, as well as gay men and young men from the LGBTQI+ community. (Reference McDonald19; Reference Siuta and Bergman20) These groups often face added instability and fear within their work environments. Their job insecurities couple with a pervasive culture of victim-blaming, and self-blaming prevents many women from reporting sexual harassment. This silence not only prolongs the duration of harassment but also complicates efforts to gather accurate statistics and develop effective solutions. It also hinders the legislative advocacy needed to create safer and more equitable workplace environments. (21)
Addressing sexual harassment effectively requires a multifaceted approach that includes legal reforms, cultural shifts within workplaces, and strengthened policies and support systems that empower victims to come forward and seek justice without fear of reprisal or stigma. Indeed, addressing sexual harassment in Iranian workplaces necessitates a series of foundational changes, beginning with the criminalization of sexual harassment. This step is crucial for establishing a legal framework that not only penalizes perpetrators but also signals a zero-tolerance policy towards such behaviour.
Here are the key strategies to prevent and handle sexual harassment effectively in Iran:
Legal Reform: Enact laws that explicitly criminalize all forms of sexual harassment in the workplace. This includes defining what constitutes sexual harassment clearly and comprehensively, covering a range of behaviours from verbal comments to physical actions.
Organizational Accountability: Require organizations to implement strict policies against sexual harassment. This involves creating and enforcing rules that deter such behaviour and hold perpetrators accountable. Organizations should also be made legally responsible for preventing workplace harassment and for taking swift and appropriate action when incidents occur.
Simplified Reporting Mechanisms: Establish confidential and accessible reporting channels within organizations. Victims should have multiple options for reporting harassment, including online platforms, dedicated hotlines, and the ability to report directly to a designated, trained officer rather than just direct supervisors who may be biased.
Victim Protection: Develop protective measures for victims post-reporting. This includes ensuring that they do not face retaliation from the harasser or other colleagues, potentially offering temporary reassignments for either the victim or the harasser during the investigation, and providing support services such as counseling.
Education and Training: Implement mandatory training sessions for all employees, including management, on recognizing, preventing, and responding to sexual harassment. Training should empower employees to recognize inappropriate behaviour and understand the correct steps to take if they or a colleague are harassed. This should also cover bystander intervention techniques to encourage supportive peer actions.
Cultural Change Initiatives: Encourage a shift in workplace culture through ongoing awareness programmes and cultural sensitivity training. These initiatives should aim to change the norms and behaviours that enable sexual harassment, promoting a more inclusive and respectful work environment. By adopting these strategies, not only can the immediate issue of sexual harassment be addressed, but the broader workplace culture in Iran can begin to shift towards a more equitable and safer environment for all employees, regardless of gender.
Conclusion
Addressing the pervasive issue of sexual harassment within Iran’s health care settings requires a multifaceted approach that acknowledges both systemic challenges and cultural dynamics. The absence of explicit legal protections and the hierarchical structure within medical institutions contribute significantly to the prevalence of harassment, impacting not only victims’ wellbeing but also overall workplace morale and efficiency. To foster meaningful change, it is imperative to enact stringent legal measures that criminalize all forms of sexual harassment and establish clear protocols for reporting and accountability. Organizations must be held accountable for implementing and enforcing anti-harassment policies that prioritize victim support and discourage retaliation. Moreover, comprehensive education and training programmes are essential to empower all employees, from management to frontline staff, in recognizing, preventing, and effectively responding to harassment incidents. Cultural change initiatives are equally crucial to challenge ingrained norms and promote a workplace culture rooted in respect, inclusivity, and gender equality. By addressing these systemic issues head-on and fostering a supportive environment where victims feel safe to come forward, Iran can begin to cultivate healthier and more equitable health care workplaces, ensuring the wellbeing and dignity of all employees.

 Open access
Open access