


Introduction
Self-harm and suicide (definitions in Table 1) have been recognized by the World Health Organization (WHO) as major public health concerns and consistently remained in the top four causes of death among individuals aged 15–29 year (WHO, 2021, 2023). These behaviors impose substantial economic burdens, with estimated average annual costs of $570 billion (2022 USD) in the US (Peterson, Haileyesus, & Stone, Reference Peterson, Haileyesus and Stone2024) and $5.87 billion (2022 USD) in Australia (Kinchin & Doran, Reference Kinchin and Doran2017), largely due to diminished quality-of-life, productivity losses, and healthcare expenditure. While comparable estimates are lacking for low- and middle-income countries (LMICs), the impact is likely substantial, with over 73% of global suicides occurring in LMICs in 2021 (WHO, 2023).
Definitions of key terms

Table 1. Long description
The table has two columns. The left column lists terms: Self-harm, Suicide, Suicidal ideation, Universal intervention, Selective intervention, Indicated intervention, Multi-level intervention. The right column provides definitions. Self-harm is defined as a non-fatal act where an individual causes harm to themselves, with motives that may or may not include intent to die; suicide attempt is a type of self-harm with intent to die but survival. Suicide is a fatal act carried out to deliberately end one’s own life. Suicidal ideation refers to thoughts of suicide, ranging from a sense of meaninglessness to intense preoccupation with ending life. Universal intervention targets the entire population without assessing risk. Selective intervention focuses on individuals with risk factors such as stressful life events, family history, mental illness, or impulsivity, even if they have not engaged in self-harm or suicide. Indicated intervention targets those who have already engaged in self-harming or suicidal behaviors, such as people with previous self-harm episodes. Multi-level intervention combines universal, selective, and indicated interventions delivered together. Each definition cites Pirkis et al., 2022 or 2023, or Hegerl, Heinz, O’Connor, and Reich, 2021.
A range of interventions (definitions in Table 1) have been shown to reduce self-harm and suicide, including universal interventions (e.g. restricting access to lethal means), selective interventions (e.g. medications like clozapine for people with mental illness), indicated interventions (e.g. psychological therapies for people with previous suicidal behaviors), and multi-level interventions (e.g. a combination of universal, selective, and indicated interventions) (Hegerl et al., Reference Hegerl, Heinz, O’Connor and Reich2021; Laflamme et al., Reference Laflamme, Vaez, Lundin and Sengoelge2022; Pirkis et al., Reference Pirkis, Dandona, Silverman, Khan and Hawton2024; Zalsman et al., Reference Zalsman, Hawton, Wasserman, Heeringen, Arensman, Sarchiapone, Carli, Höschl, Barzilay, Balazs, Purebl, Kahn, Sáiz, Lipsicas, Bobes, Cozman, Hegerl and Zohar2016). However, evidence on the cost-effectiveness or value-for-money of these interventions still remains unclear, underscoring the need for reviewing economic evaluations to guide resource allocation (Kernick, Reference Kernick2003).
Earlier systematic reviews of economic evidence of self-harm and suicide preventive interventions tended to situate within interventions for mental illness and mental health promotion (Feldman et al., Reference Feldman, Gebreslassie, Sampaio, Nystrand and Ssegonja2021; Ha et al., Reference Ha, Huong, Anh and Anh2022; Le et al., Reference Le, Esturas, Mihalopoulos, Chiotelis, Bucholc, Chatterton and Engel2021; Mihalopoulos & Chatterton, Reference Mihalopoulos and Chatterton2015; Mihalopoulos et al., Reference Mihalopoulos, Vos, Pirkis and Carter2011; Zechmeister et al., Reference Zechmeister, Kilian and McDaid2008). These reviews largely focused on interventions in high-income countries (HICs) and primarily covered educational and training interventions (Feldman et al., Reference Feldman, Gebreslassie, Sampaio, Nystrand and Ssegonja2021; Mihalopoulos, Vos, Pirkis, & Carter, Reference Mihalopoulos, Vos, Pirkis and Carter2011; Zechmeister et al., Reference Zechmeister, Kilian and McDaid2008). To address these limitations, Madsen and colleagues (Reference Bustamante Madsen, Eddleston, Schultz Hansen and Konradsen2018) conducted the first systematic review devoted exclusively to economic evaluations of self-harm and suicide interventions across both HICs and LMICs, identifying 25 studies. However, this review was conducted a decade ago, had limited coverage of studies published between 2003 and 2016, and likely underestimated return-on-investment (ROI) studies as ROI-related search terms were not included.
Since the review by Madsen and colleagues (Reference Bustamante Madsen, Eddleston, Schultz Hansen and Konradsen2018), many economic evaluations of self-harm and suicide preventive interventions, including ROI studies, have been published, highlighting the need for an updated and more comprehensive synthesis. Expanding the coverage beyond the 2003–2016 period would enhance understanding of the interventions’ development history and assess whether interventions produce consistent economic outcomes across time and contexts (Drummond et al., Reference Drummond, Barbieri, Cook, Glick, Lis, Malik, Reed, Rutten, Sculpher and Severens2009). With these motivations, this systematic review aims to provide a comprehensive and up-to-date overview of the available economic evidence on self-harm and suicide interventions without any restrictions (e.g. target population, prevention strategy) to identify those with strong cost-effectiveness potential.
Methods
This systematic review conformed to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann, Mulrow, Shamseer, Tetzlaff, Akl, Brennan, Chou, Glanville, Grimshaw, Hróbjartsson, Lalu, Li, Loder, Mayo-Wilson, McDonald and Moher2021). The review protocol was registered in the PROSPERO database (#CRD42023460339).
Identification and selection of studies
Eligible economic evaluations were identified through searches of multiple electronic databases, namely MEDLINE, Embase, PsycINFO, CINAHL, and EconLit, from inception to January 15, 2026. Reference list checks and grey literature searches on ProQuest and Google Scholar were also conducted. The search string was developed by adapting the search terms published in previous reviews (Madsen et al., Reference Bustamante Madsen, Eddleston, Schultz Hansen and Konradsen2018; Feldman et al., Reference Feldman, Gebreslassie, Sampaio, Nystrand and Ssegonja2021; Le et al., Reference Le, Esturas, Mihalopoulos, Chiotelis, Bucholc, Chatterton and Engel2021). Details on search strategies are provided in Supplementary Material 1.
Covidence was used to ensure that each record was independently screened by at least two reviewers at each stage of the review process. Four reviewers (AT, DL, DW, and PL) screened titles and abstracts, and two (DL, PL) reviewed the full text for appropriateness based on pre-defined inclusion and exclusion criteria (see below). High proportionate agreement was observed for both abstract (93.71%) and full-text (86.01%) reviews. A senior health economist (LL) arbitrated discrepancies among the four reviewers.
Inclusion and exclusion criteria
The review included full economic evaluations assessing the cost-effectiveness of any preventive intervention for self-harm, suicide, and suicidal ideation, with no restrictions on prevention strategy, intervention type, target population, comparator, follow-up time, publication time, location, or setting. Eligible study designs included cost–benefit analysis (CBA), cost-minimization analysis (CMA), cost-utility analysis (CUA), cost-effectiveness analysis (CEA), or a ROI analysis that examined both the costs and benefits of at least two alternative courses of action (e.g. policies, interventions). The review excluded partial economic analyses (i.e. studies examined costs or benefits of both courses of action), studies focused on suicide gene therapy or accidental overdose, comments, editorials, opinion pieces, letters, conference abstracts, and studies written in languages other than English.
Data extraction
Characteristics of the included studies were extracted and summarized in a table format adapted from prior systematic reviews (Le et al., Reference Le, Esturas, Mihalopoulos, Chiotelis, Bucholc, Chatterton and Engel2021; Mihalopoulos & Chatterton, Reference Mihalopoulos and Chatterton2015). To ensure comparability, all costs were converted into 2022 US dollars using the purchasing power parity approach sourced from the International Monetary Fund – World Economic Outlook database (Shemilt, James, & Marcello, Reference Shemilt, James and Marcello2010). If the year of pricing was not specified, it was assumed to be 2 years prior to the year of publication. If the analysis perspective was not reported or unclear, it was inferred based on the cost and outcome measures. If the study did not calculate an incremental cost-effectiveness ratio (ICER), net monetary benefit (NMB), benefit-to-cost ratio (BCR), or ROI ratio, the extracted data on costs and outcomes were used to compute these ratios.
Data synthesis
Interventions were first grouped into four strategies – universal, selective, indicated, and multi-level, and further classified by specific types like means restriction, medication, or psychological therapies (definitions in Supplementary Material 2). Given the substantial heterogeneity in intervention characteristics and economic evaluation methods, a meta-analysis was not conducted. Instead, a structured narrative synthesis was undertaken to evaluate and compare economic evidence across diverse interventions and contexts. Additionally, a dominance ranking framework derived from the Joanna Briggs Institute’s systematic review guidelines was employed to further categorize interventions through three color codes: red for ‘unfavored’ (higher costs and lower effectiveness), green for ‘favored’ (better outcomes at lower costs), and yellow for ‘unclear’ cost-effectiveness (e.g. more [less] effective and more [less] costly than the control) (Gomersall et al., Reference Gomersall, Jadotte, Xue, Lockwood, Riddle and Preda2015). For studies comparing multiple interventions against a control, each intervention’s cost-effectiveness was assessed separately. If conflicting cost-effectiveness outcomes appeared across different perspectives and/or outcome measures within a study, the intervention’s cost-effectiveness in that study was classified as unclear. If conflicting findings on cost-effectiveness were found among studies evaluating the same intervention type, the intervention type was concluded to have inconsistent results overall.
Although there is no consensus on cost-effectiveness thresholds for commonly used outcome measures such as costs per QALY gained or DALY averted (Pichon-Riviere et al., Reference Pichon-Riviere, Drummond, Palacios, Garcia-Marti and Augustovski2023; Sun et al., Reference Sun, Peng, Li and Huang2023), the threshold of 50,000 USD per QALY gained or DALY averted has been widely adopted (Neumann, Cohen, & Weinstein, Reference Neumann, Cohen and Weinstein2014), aligning with the recommendations by decision makers in Australia (Productivity Commission, 2024) and in the UK (NICE, 2013). Accordingly, this review applied the above threshold to ensure consistency in cost-effectiveness judgments while also reporting the specific thresholds within the included studies in the data extraction tables. For studies employing less frequently used cost-effectiveness measures (i.e. cost per suicide case averted), judgments were based on the thresholds specified within each study.
Methodology quality assessment
Drummond’s 10-item checklist was used to evaluate the methodological quality of the included studies (Drummond et al., Reference Drummond, Sculpher, Claxton, Stoddart and Torrance2015). Following prior publications (Madsen et al., Reference Bustamante Madsen, Eddleston, Schultz Hansen and Konradsen2018; Le et al., Reference Le, Le, Le, Yap and Mihalopoulos2025), each item was scored based on whether it met (1 point), partially met (0.5 point), or did not meet (0 point) the criteria. A total score was used to classify study quality as high (8–10), average (5–7), or poor (0–4) (Le et al., Reference Le, Le, Le, Yap and Mihalopoulos2025 Reference Bandara, Pirkis, Clapperton, Shin, Too, Reifels, Onie, Page, Andriessen, Krysinska, Flego, Schlichthorst, Spittal, Mihalopoulos and Le5; Mihalopoulos et al., Reference Mihalopoulos, Vos, Pirkis and Carter2011). Two reviewers (PL and DL) assessed the quality of each study independently (proportionate agreement of 81.32%). Disagreements were resolved by discussion or arbitration by a third reviewer (LL).
Results
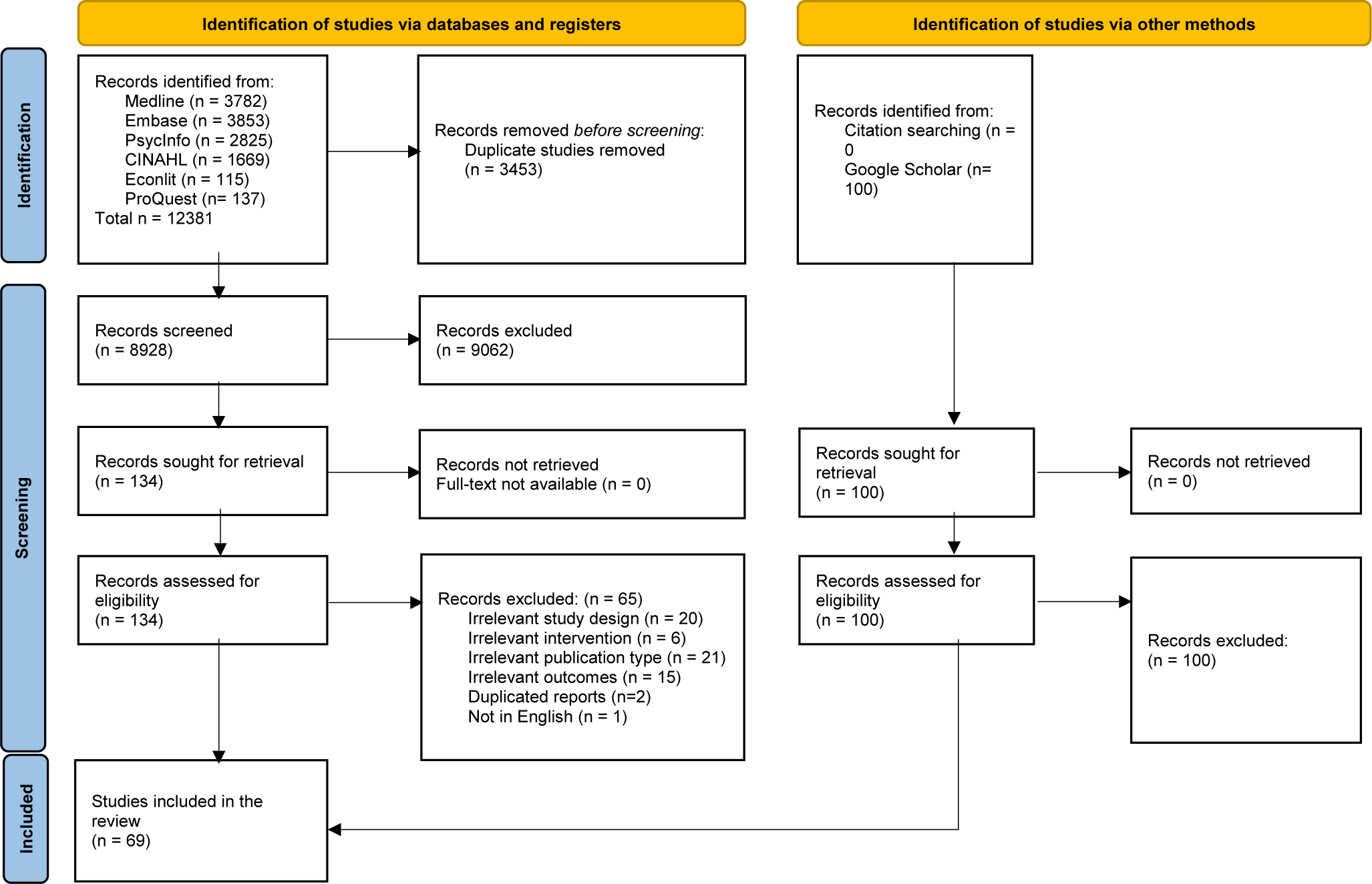
The systematic searches identified a total of 12,381 records. After removing duplicates and screening titles, abstracts, and full-texts, 69 studies were eligible, including 30 studies identified in previous reviews (Madsen et al., Reference Bustamante Madsen, Eddleston, Schultz Hansen and Konradsen2018; Feldman et al., Reference Feldman, Gebreslassie, Sampaio, Nystrand and Ssegonja2021; Ha et al., Reference Ha, Huong, Anh and Anh2022; Le et al., Reference Le, Esturas, Mihalopoulos, Chiotelis, Bucholc, Chatterton and Engel2021). No additional studies were identified through reference searches of included articles. Further details are presented in the PRISMA flow diagram (Figure 1).
PRISMA flow diagram.

Figure 1. Long description
Starting at the top left, the first track is labeled Identification of studies via databases and registers. Records identified from Medline 3782, Embase 3853, PsycInfo 2825, C I N A H L 1669, EconLit 115, ProQuest 137, total 12381. An arrow points right to Records removed before screening, Duplicate studies removed 3453. Downward, Records screened 8928, arrow to the right to Records excluded 9062. Downward, Records sought for retrieval 134, arrow right to Records not retrieved, Full-text not available 0. Downward, Records assessed for eligibility 134, arrow right to Records excluded 65, with breakdown: Irrelevant study design 20, Irrelevant intervention 6, Irrelevant publication type 21, Irrelevant outcomes 15, Duplicated reports 2, Not in English 1. Downward, Studies included in the review 69. The second track, right side, is labeled Identification of studies via other methods. Records identified from Citation searching 0, Google Scholar 100. Downward, Records sought for retrieval 100, arrow right to Records not retrieved 0. Downward, Records assessed for eligibility 100, arrow right to Records excluded 100. No studies from this track are included. All arrows indicate the flow of records through each phase, with exclusion points detailed at each step.
Characteristics of included studies
This review included 69 studies evaluating the cost-effectiveness of three types of universal, five types of selective, five types of indicated, and nine multi-level interventions for self-harm, suicide, and suicidal ideation prevention (Table 2). Most studies (n = 59) evaluated one type of intervention, with means restriction, support services, and psychotherapy were the most frequently evaluated universal, selective, and indicated interventions, respectively. Nearly all studies (n = 64) compared the interventions with no intervention or treatment-as-usual (TAU). Most studies were conducted in HICs, with only three from LMICs. The evaluation methods included CUA (n = 38), CEA (n = 37), ROI (n = 15), and CBA (n = 8). Over half of the studies (n = 39) were model-based with longer time horizons (typically 5 years to a lifetime), while the remaining were mostly trial-based with shorter time horizons (typically under 1 year). Only 19 studies targeted children and adolescents, and none focused on older adults.
Characteristics of included studies

Table 2. Long description
This is a multi-column table with 15 columns and over 60 rows, organized by intervention type: Universal, Selective, Indicated, and Multi-level interventions. The first row contains headers: Lead author (year) country, Description of interventions, Description of comparators, Types of suicide targeted, Target population (age, percent male), Evaluation method, Study design, Perspective, Time horizon, Year of pricing and discount rates, Cost of intervention, Cost savings, Health outcomes/benefits, Results ICERS (in 2022 USD value) threshold, and Quality. Each subsequent row details a study, beginning with the lead author and year, followed by country, intervention description (e.g., means restriction, awareness training, support services, psychotherapy, medication, screening, policy), comparator (e.g., no intervention, treatment as usual), suicide type (e.g., suicide, self-harm, suicidal ideation), target population (with age and gender breakdowns), evaluation method (e.g., CEA, CUA, ROI, CBA), study design (e.g., model, RCT, cohort), perspective (e.g., societal, healthcare), time horizon (ranging from months to lifetime), year and currency for costs, intervention cost details, cost savings (direct and indirect), health outcomes (e.g., QALY, DALY, suicide cases averted), ICER or ROI results with thresholds, and study quality (H, A, L). Universal interventions include means restriction (barriers, gatekeeper training, banning pesticides), awareness training, and media guidelines. Selective interventions cover support services (helplines, peer support, institutional care), psychotherapy (CBT, DBT, family therapy), medication (clozapine, SSRIs, pharmacogenetic testing), and health policies. Indicated interventions focus on psychotherapy (DBT, CBT, family therapy, web-based self-help), support services (crisis plans, follow-up calls), and screening. Multi-level interventions include school-based, community, and workplace programs. Each study row provides specific data, such as sample size, cost components, outcome measures, and economic results (e.g., ROI values, ICERs per QALY or life-year gained, dominance statements). The table footnote defines quality ratings: H for high, A for average, L for low.
Note: H, high quality; A, average quality; L, low quality.
Summary findings
Universal interventions
Universal means restriction: The cost-effectiveness of universal means restriction was inconsistent across four high-quality (Bandara et al., Reference Bandara, Pirkis, Clapperton, Shin, Too, Reifels, Onie, Page, Andriessen, Krysinska, Flego, Schlichthorst, Spittal, Mihalopoulos and Le2022; Damerow et al., Reference Damerow, Weerasinghe, Madsen, Hansen, Pearson, Eddleston and Konradsen2020; Law & Yip, Reference Law and Yip2011; Lee et al., Reference Lee, Chisholm, Eddleston, Gunnell, Fleischmann, Konradsen, Bertram, Mihalopoulos, Brown, Santomauro, Schess and van Ommeren2021) and one low-quality (Whitmer & Woods, Reference Whitmer and Woods2013) studies. Barriers at bridges were cost-effective over 5–20 years from a partial societal perspective in Australia (Bandara et al., Reference Bandara, Pirkis, Clapperton, Shin, Too, Reifels, Onie, Page, Andriessen, Krysinska, Flego, Schlichthorst, Spittal, Mihalopoulos and Le2022) and the US (Whitmer & Woods, Reference Whitmer and Woods2013) but not at cliff sites in Australia (Bandara et al., Reference Bandara, Pirkis, Clapperton, Shin, Too, Reifels, Onie, Page, Andriessen, Krysinska, Flego, Schlichthorst, Spittal, Mihalopoulos and Le2022) and railway platforms in Hong Kong (Law & Yip, Reference Law and Yip2011). Hazardous pesticide access restriction was cost-effective from a healthcare perspective across 14 countries over a lifetime (Lee et al., Reference Lee, Chisholm, Eddleston, Gunnell, Fleischmann, Konradsen, Bertram, Mihalopoulos, Brown, Santomauro, Schess and van Ommeren2021). In Sri Lanka, a threshold analysis indicated that preventing as few as 0.23 suicides per 100,000 population over 3 years would render pesticide restriction cost-effective (Damerow et al., Reference Damerow, Weerasinghe, Madsen, Hansen, Pearson, Eddleston and Konradsen2020).
Universal awareness training: The cost-effectiveness of universal awareness training varied across three high-quality studies (Jackson-Morris et al., Reference Jackson-Morris, Meyer, Morgan, Stelmach, Jamison and Currie2024; Kinchin et al., Reference Kinchin, Russell, Petrie, Mifsud, Manning and Doran2020; Sari et al., Reference Sari, de Castro, Newman and Mills2008). The intervention was cost-effective for self-harm prevention in Australia and in the US from a societal perspective (Kinchin et al., Reference Kinchin, Russell, Petrie, Mifsud, Manning and Doran2020; Sari et al., Reference Sari, de Castro, Newman and Mills2008). However, in the UK, Jackson-Morris et al. (Reference Jackson-Morris, Meyer, Morgan, Stelmach, Jamison and Currie2024) reported uncertain cost-effectiveness for self-harm prevention from a partial societal perspective.
Universal media guidelines: In Australia, a high-quality study found media guidelines for reporting suicide were cost-effective in preventing self-harm and suicide in the general population over 5 years, compared to no intervention, from a societal perspective (Flego et al., Reference Flego, Reifels, Mihalopoulos, Bandara, Page, Fox, Skehan, Hill, Krysinska, Andriessen, Schlichthorst, Pirkis and Le2022).
Selective interventions
Selective support services: Support services were cost-effective in preventing self-harm, suicide, and suicidal ideation among individuals displaying risk factors (e.g. individuals facing life challenges) according to five high-quality studies (Comans, Visser, & Scuffham, Reference Comans, Visser and Scuffham2013; Pil et al., Reference Pil, Pauwels, Muijzers, Portzky and Annemans2013; Ross et al., Reference Ross, Zuromski, Reis, Nock, Kessler and Smoller2021; Sari et al., Reference Sari, de Castro, Newman and Mills2008; Wilson-Barthes et al., Reference Wilson-Barthes, Chrysanthopoulou, Atwoli, Ayuku, Braitstein and Galárraga2021). In the US, active follow-up and peer support groups were cost-effective over a lifetime from healthcare and societal perspectives, respectively (Ross et al., Reference Ross, Zuromski, Reis, Nock, Kessler and Smoller2021; Sari et al., Reference Sari, de Castro, Newman and Mills2008). Telephone and chat helplines also demonstrated cost savings from a societal perspective in Australia (Comans, Visser, & Scuffham, Reference Comans, Visser and Scuffham2013) and Belgium (Pil et al., Reference Pil, Pauwels, Muijzers, Portzky and Annemans2013). In Kenya, institutional care for orphaned children was more cost-effective than family-based care (Wilson-Barthes et al., Reference Wilson-Barthes, Chrysanthopoulou, Atwoli, Ayuku, Braitstein and Galárraga2021).
Selective psychotherapy: The cost-effectiveness of selective psychotherapy for preventing self-harm, suicide, and suicidal ideation in populations displaying risk factors (e.g. mental illness) was demonstrated in four studies of mixed quality in the US (Gray et al., Reference Gray, Dawson, Grey and McMahon2011; Ross et al., Reference Ross, Zuromski, Reis, Nock, Kessler and Smoller2021; Tebbett-Mock et al., Reference Tebbett-Mock, Saito, McGee, Woloszyn and Venuti2020; Zaloshnja et al., Reference Zaloshnja, Miller, Galbraith, Lawrence, DeBruyn, Bill, Hicks, Keiffer and Perkins2003). The intervention was cost-saving for adolescents at risk of mental illness over a 1-year period and a lifetime from healthcare and societal perspectives (Gray et al., Reference Gray, Dawson, Grey and McMahon2011; Tebbett-Mock et al., Reference Tebbett-Mock, Saito, McGee, Woloszyn and Venuti2020; Zaloshnja et al., Reference Zaloshnja, Miller, Galbraith, Lawrence, DeBruyn, Bill, Hicks, Keiffer and Perkins2003). However, among primary care patients, the intervention’s cost-effectiveness depended on whether suicide prediction scales had a minimum sensitivity of 75% and specificity of 97% (Ross et al., Reference Ross, Zuromski, Reis, Nock, Kessler and Smoller2021).
Selective medication: The cost-effectiveness of medication for populations displaying risk factors (e.g. mental illness, pregnant women with anemia) showed inconsistent results across five average-to-high quality studies (Dazelle et al., Reference Dazelle, Ebner, Potarazu, Kazma and Ahmadzia2026; Duggan et al., Reference Duggan, Warner, Knapp and Kerwin2003; Freemantle et al., Reference Freemantle, House, Song, Mason and Sheldon1994; Goren et al., Reference Goren, Rose, Smith and Ney2016; Groessl et al., Reference Groessl, Tally, Hillery, Maciel and Garces2018). In the US, clozapine and antidepressants were cost-saving over 1–3 years from healthcare (Goren et al. Reference Goren, Rose, Smith and Ney2016) and societal (Groessl et al., Reference Groessl, Tally, Hillery, Maciel and Garces2018) perspectives, respectively. Similarly, iron supplementation therapy was also cost-effective among pregnant women with anemia over a lifetime from healthcare and societal perspectives (Dazelle et al., Reference Dazelle, Ebner, Potarazu, Kazma and Ahmadzia2026). However, in the UK, antidepressants (e.g. selective serotonin reuptake inhibitors) had uncertain cost-effectiveness, being more costly and more effective than older tricyclics, with ICERs of $54,600–$486,000 per life-year gained over a lifetime from a healthcare perspective (Freemantle et al., Reference Freemantle, House, Song, Mason and Sheldon1994). A threshold analysis over 10 years also showed a cost per life-year saved of $12,000 if clozapine were cost-neutral, and a cost saving if it reduced annual support costs by 10% from a healthcare perspective (Duggan et al., Reference Duggan, Warner, Knapp and Kerwin2003).
Selective health policies: A high-quality study in the US demonstrated that a health policy granting prescriptive authority for psychotropic medications to qualified psychologists was cost-effective in preventing self-harm and suicide among people with mental illness from a societal perspective over 20 years (Hughes et al., Reference Hughes, Phillips, McGrath and Thomas2023).
Selective combined intervention: Based on one high-quality study in the UK, the selective combined intervention (including medication, psychotherapy, counselling, and vocational therapies) was cost-saving compared to TAU for individuals with mental disorders over 10 years from a societal perspective (Park, McCrone, & Knapp, Reference Park, McCrone and Knapp2016).
Indicated interventions
Indicated psychotherapy: Psychotherapy for individuals with previous self-harm episodes was largely cost-effective in preventing self-harm, suicide, and suicidal ideation across 25 studies, mostly high quality (n = 24) and conducted in HICs (n = 24).
Employing a 1-year time horizon, psychotherapy was found cost-effective for preventing self-harm, suicide, and suicidal ideation in adolescents and adults with previous self-harm across six studies, mostly of high-quality, undertaken in the US (Acolin, Reference Acolin2022; Denchev et al., Reference Denchev, Pearson, Allen, Claassen, Currier, Zatzick and Schoenbaum2018; McCutchan et al., Reference McCutchan, Yates, Jobes, Kerbrat and Comtois2022), Pakistan (Alvi et al., Reference Alvi, Shiri, Iqbal, Husain, Chaudhry, Shakoor, Ansari, Kiran, Chaudhry and Husain2022), Norway (Haga et al., Reference Haga, Aas, Grøholt, Tørmoen and Mehlum2018), and Spain (Martínez-Alés et al., Reference Martínez-Alés, Cruz Rodríguez, Lázaro, Domingo-Relloso, Barrigón, Angora, Rodríguez-Vega, Jiménez-Sola, Sánchez-Castro, Román-Mazuecos, Villoria, Ortega, Navío, Stanley, Rosenheck, Baca-García and Bravo-Ortiz2021). Specifically, this intervention was either cost-saving (McCutchan et al., Reference McCutchan, Yates, Jobes, Kerbrat and Comtois2022) or had acceptable ICERs (Alvi et al., Reference Alvi, Shiri, Iqbal, Husain, Chaudhry, Shakoor, Ansari, Kiran, Chaudhry and Husain2022; Denchev et al., Reference Denchev, Pearson, Allen, Claassen, Currier, Zatzick and Schoenbaum2018; Haga et al., Reference Haga, Aas, Grøholt, Tørmoen and Mehlum2018; Martínez-Alés et al., Reference Martínez-Alés, Cruz Rodríguez, Lázaro, Domingo-Relloso, Barrigón, Angora, Rodríguez-Vega, Jiménez-Sola, Sánchez-Castro, Román-Mazuecos, Villoria, Ortega, Navío, Stanley, Rosenheck, Baca-García and Bravo-Ortiz2021) compared to TAU from healthcare (Alvi et al., Reference Alvi, Shiri, Iqbal, Husain, Chaudhry, Shakoor, Ansari, Kiran, Chaudhry and Husain2022; Denchev et al., Reference Denchev, Pearson, Allen, Claassen, Currier, Zatzick and Schoenbaum2018; Haga et al., Reference Haga, Aas, Grøholt, Tørmoen and Mehlum2018; McCutchan et al., Reference McCutchan, Yates, Jobes, Kerbrat and Comtois2022) and societal (Martínez-Alés et al., Reference Martínez-Alés, Cruz Rodríguez, Lázaro, Domingo-Relloso, Barrigón, Angora, Rodríguez-Vega, Jiménez-Sola, Sánchez-Castro, Román-Mazuecos, Villoria, Ortega, Navío, Stanley, Rosenheck, Baca-García and Bravo-Ortiz2021) perspectives in these locations. In the US, dialectical behavior therapy was more cost-effective than cognitive behavior therapy from a healthcare perspective (Acolin, Reference Acolin2022).
However, mixed or unfavorable evidence was found in other locations and populations. Across seven high-quality studies in the UK, psychotherapy showed inconsistent cost-effectiveness for adults with previous self-harm (Byford et al., Reference Byford, Knapp, Greenshields, Ukoumunne, Jones, Thompson, Tyrer, Schmidt, Davidson and Group2003; Haddock et al., Reference Haddock, Pratt, Gooding, Peters, Emsley, Evans, Kelly, Huggett, Munro, Harris, Davies and Awenat2019; Priebe et al., Reference Priebe, Bhatti, Barnicot, Bremner, Gaglia, Katsakou, Molosankwe, McCrone and Zinkler2012; Tyrer et al., Reference Tyrer, Tom, Byford, Schmidt, Jones, Davidson, Knapp, MacLeod and Catalan2004) and was not cost-effective for adolescents with previous self-harm over 1 year or less (Byford et al., Reference Byford, Harrington, Torgerson, Kerfoot, Dyer, Harrington, Woodham, Gill and McNiven1999; Green et al., Reference Green, Wood, Kerfoot, Trainor, Roberts, Rothwell, Woodham, Ayodeji, Barrett, Byford and Harrington2011; Tubeuf, Saloniki, & Cottrell, Reference Tubeuf, Saloniki and Cottrell2019) from healthcare (Haddock et al., Reference Haddock, Pratt, Gooding, Peters, Emsley, Evans, Kelly, Huggett, Munro, Harris, Davies and Awenat2019; Tubeuf, Saloniki, & Cottrell, Reference Tubeuf, Saloniki and Cottrell2019) and societal perspectives (Byford et al., Reference Byford, Harrington, Torgerson, Kerfoot, Dyer, Harrington, Woodham, Gill and McNiven1999, Reference Byford, Knapp, Greenshields, Ukoumunne, Jones, Thompson, Tyrer, Schmidt, Davidson and Group2003; Green et al., Reference Green, Wood, Kerfoot, Trainor, Roberts, Rothwell, Woodham, Ayodeji, Barrett, Byford and Harrington2011; Priebe et al., Reference Priebe, Bhatti, Barnicot, Bremner, Gaglia, Katsakou, Molosankwe, McCrone and Zinkler2012; Tyrer et al., Reference Tyrer, Tom, Byford, Schmidt, Jones, Davidson, Knapp, MacLeod and Catalan2004). Similarly, three high-quality studies in the Netherlands reported inconsistent cost-effectiveness over a 1-year horizon or less from both healthcare and societal perspectives (Huntjens et al., Reference Huntjens, Smit, van den Bosch, Kerkhof, Sizoo and van der Gaag2025; Spijker et al., Reference Spijker, Majo, Smit, Straten and Kerkhof2012; van Bentum et al., Reference van Bentum, Wijnen, Bachrach, Creemers, van Dijk, Dingemanse, van Haaren, Stikkelbroek, Van, Vrijsen, de Winter and Sijbrandij2026). While psychotherapy demonstrated good value-for-money among adults with previous self-harm (Huntjens et al., Reference Huntjens, Smit, van den Bosch, Kerkhof, Sizoo and van der Gaag2025) or suicidal ideation (Spijker et al., Reference Spijker, Majo, Smit, Straten and Kerkhof2012), it was not cost-effective among psychiatric outpatient adults experiencing suicidal intrusions (van Bentum et al., Reference van Bentum, Wijnen, Bachrach, Creemers, van Dijk, Dingemanse, van Haaren, Stikkelbroek, Van, Vrijsen, de Winter and Sijbrandij2026). Over a shorter time horizon (1–3 months), a high-quality Swedish study found psychotherapy for adolescents with previous self-harm was not cost-effective (Bjureberg et al., Reference Bjureberg, Ojala, Rasmusson, Malmgren, Hellner, Sampaio and Flygare2025).
Over 2 years to a lifetime, the cost-effectiveness of psychotherapy for preventing self-harm and suicide among individuals with previous self-harm remained inconsistent across eight high-quality studies. In the US (Bernecker et al., Reference Bernecker, Zuromski, Curry, Kim, Gutierrez, Joiner, Kessler, Nock, Rudd and Bryan2020), Canada (Vasiliadis et al., Reference Vasiliadis, Dezetter, Latimer, Drapeau and Lesage2017), Australia (Krysinska et al., Reference Krysinska, Andriessen, Bandara, Reifels, Flego, Page, Schlichthorst, Pirkis, Mihalopoulos and Khanh-Dao Le2024), and Switzerland (Park et al., Reference Park, Gysin-Maillart, Müller, Exadaktylos and Michel2018), psychotherapy was cost-saving compared to TAU or no intervention from healthcare (Park et al., Reference Park, Gysin-Maillart, Müller, Exadaktylos and Michel2018), payer (Bernecker et al., Reference Bernecker, Zuromski, Curry, Kim, Gutierrez, Joiner, Kessler, Nock, Rudd and Bryan2020), partial societal (Krysinska et al., Reference Krysinska, Andriessen, Bandara, Reifels, Flego, Page, Schlichthorst, Pirkis, Mihalopoulos and Khanh-Dao Le2024), and societal (Vasiliadis et al., Reference Vasiliadis, Dezetter, Latimer, Drapeau and Lesage2017) perspectives. However, in the UK, the cost-effectiveness of psychotherapy compared with TAU was inconsistent across three studies (Bojke et al., Reference Bojke, Cottrell, Wright-Hughes, Farrin and Tubeuf2024; Cottrell et al., Reference Cottrell, Wright-Hughes, Collinson, Boston, Eisler, Fortune, Graham, Green, House, Kerfoot, Owens, Saloniki, Simic, Tubeuf and Farrin2018; Mavranezouli et al., Reference Mavranezouli, Pelone, Connolly, Mughal, Witt, Hawton, Lascelles, Wildgoose, Childs, Pilling and Kapur2024). Specifically, over a 5-year horizon, one study found psychotherapy cost-effective among adolescents (Cottrell et al., Reference Cottrell, Wright-Hughes, Collinson, Boston, Eisler, Fortune, Graham, Green, House, Kerfoot, Owens, Saloniki, Simic, Tubeuf and Farrin2018), another demonstrated the intervention was dominated (Bojke et al., Reference Bojke, Cottrell, Wright-Hughes, Farrin and Tubeuf2024), and a third found it cost-effective among adults but not among children (Mavranezouli et al., Reference Mavranezouli, Pelone, Connolly, Mughal, Witt, Hawton, Lascelles, Wildgoose, Childs, Pilling and Kapur2024), all from a healthcare perspective.
Indicated support services: Support services were mostly cost-effective compared to TAU or no intervention in preventing self-harm, suicide, and suicidal ideation among individuals with previous self-harm, based on 10 studies of average (Denchev et al., Reference Denchev, Pearson, Allen, Claassen, Currier, Zatzick and Schoenbaum2018) to high (Borschmann et al., Reference Borschmann, Barrett, Hellier, Byford, Henderson, Rose, Slade, Sutherby, Szmukler, Thornicroft, Hogg and Moran2013; Gallien et al., Reference Gallien, Broussouloux, Demesmaeker, Fouillet, Mertens, Chin, Cassourret, Caserio-Schonemann, du Roscoät, Le Strat and Collaborators2025; Le et al., Reference Le, Flego, Krysinska, Andriessen, Bandara, Page, Schlichthorst, Pirkis, Mihalopoulos, Carter and Reifels2023; Lindkvist et al., Reference Lindkvist, Steen Carlsson, Daukantaitė, Flyckt and Westling2024; Martínez-Alés et al., Reference Martínez-Alés, Cruz Rodríguez, Lázaro, Domingo-Relloso, Barrigón, Angora, Rodríguez-Vega, Jiménez-Sola, Sánchez-Castro, Román-Mazuecos, Villoria, Ortega, Navío, Stanley, Rosenheck, Baca-García and Bravo-Ortiz2021; O’Connor et al., Reference O’Connor, Ferguson, Scott, Smyth, McDaid, Park, Beautrais and Armitage2017; Richardson, Mark, & McKeon, Reference Richardson, Mark and McKeon2014; Ryan, Reference Ryan2015; Stelmach et al., Reference Stelmach, Kocher, Kataria, Jackson-Morris, Saxena and Nugent2022) quality. Under 1-year time horizon, support services (e.g. postcard/telephone outreach) were cost-effective from payer, healthcare, and societal perspectives in the US (Denchev et al., Reference Denchev, Pearson, Allen, Claassen, Currier, Zatzick and Schoenbaum2018; Richardson, Mark, & McKeon, Reference Richardson, Mark and McKeon2014), the UK (Borschmann et al., Reference Borschmann, Barrett, Hellier, Byford, Henderson, Rose, Slade, Sutherby, Szmukler, Thornicroft, Hogg and Moran2013; O’Connor et al., Reference O’Connor, Ferguson, Scott, Smyth, McDaid, Park, Beautrais and Armitage2017), France (Gallien et al., Reference Gallien, Broussouloux, Demesmaeker, Fouillet, Mertens, Chin, Cassourret, Caserio-Schonemann, du Roscoät, Le Strat and Collaborators2025), and Spain (Martínez-Alés et al., Reference Martínez-Alés, Cruz Rodríguez, Lázaro, Domingo-Relloso, Barrigón, Angora, Rodríguez-Vega, Jiménez-Sola, Sánchez-Castro, Román-Mazuecos, Villoria, Ortega, Navío, Stanley, Rosenheck, Baca-García and Bravo-Ortiz2021). However, findings from Sweden and the US showed unclear cost-effectiveness of support services, including brief hospital admission by self-referral (Lindkvist et al., Reference Lindkvist, Steen Carlsson, Daukantaitė, Flyckt and Westling2024) and crisis helpline (Ryan, Reference Ryan2015) over 1 and 5 year(s), respectively. Over 10–80 years, support services (e.g. aftercare, follow-up contact) were dominant in Australia (Le et al., Reference Le, Flego, Krysinska, Andriessen, Bandara, Page, Schlichthorst, Pirkis, Mihalopoulos, Carter and Reifels2023) and across 36 HICs and LMICs (Stelmach et al., Reference Stelmach, Kocher, Kataria, Jackson-Morris, Saxena and Nugent2022) from societal and partial societal perspectives.
Indicated suicide risk screening: Three high-quality studies from the US and the UK found suicide risk screening cost-effective for self-harm and suicide prevention among adults with previous self-harm or suicidal ideation in emergency departments from healthcare and societal perspectives over 1–2 year time horizon (Botchway et al., Reference Botchway, Tsiachristas, Pollard and Fazel2022; Dunlap et al., Reference Dunlap, Orme, Zarkin, Arias, Miller, Camargo, Sullivan, Allen, Goldstein, Manton, Clark and Boudreaux2019; McDaid et al., Reference McDaid, Park, Tsiachristas, Brand, Casey, Clements, Geulayov, Kapur, Ness, Waters and Hawton2022).
Indicated training for professionals: A high-quality study found training for mental health professionals not cost-effective in preventing suicidal ideation among adults with prior suicidal ideation, but potentially cost-effective for those with depression and suicidal ideation compared to TAU over 3 months from a societal perspective in the Netherlands (de Beurs et al., Reference de Beurs, Bosmans, de Groot, de Keijser, van Duijn, de Winter and Kerkhof2015).
Indicated combined interventions: The cost-effectiveness of indicated combined interventions for self-harm and suicide prevention among individuals with previous self-harm compared to TAU or no intervention remained inconsistent across one low-quality (Appleby et al., Reference Appleby, Morriss, Gask, Roland, Perry, Lewis, Battersby, Colbert, Green, Amos, Davies and Faragher2000) and three high-quality studies (Dunlap et al., Reference Dunlap, Orme, Zarkin, Arias, Miller, Camargo, Sullivan, Allen, Goldstein, Manton, Clark and Boudreaux2019; Jackson-Morris et al., Reference Jackson-Morris, Meyer, Morgan, Stelmach, Jamison and Currie2024; Latimer, Gariépy, & Greenfield, Reference Latimer, Gariépy and Greenfield2014) in HICs. In Canada, the combined intervention (assessment, referrals, and treatments) was less costly and less effective over 6 months from healthcare and societal perspectives (Latimer, Gariépy, & Greenfield, Reference Latimer, Gariépy and Greenfield2014). Conversely, in the US, the intervention (screening, safety/treatment plan, hotlines) was cost-effective for adults over 12 months from a program provider perspective (Dunlap et al., Reference Dunlap, Orme, Zarkin, Arias, Miller, Camargo, Sullivan, Allen, Goldstein, Manton, Clark and Boudreaux2019). Nevertheless, in the UK, the cost-effectiveness of combined interventions (training professionals, follow-up contact, problem-solving for patients) remained uncertain from healthcare and partial societal perspectives over the lifetime (Appleby et al., Reference Appleby, Morriss, Gask, Roland, Perry, Lewis, Battersby, Colbert, Green, Amos, Davies and Faragher2000; Jackson-Morris et al., Reference Jackson-Morris, Meyer, Morgan, Stelmach, Jamison and Currie2024).
Multi-level interventions
Multi-level interventions were mostly cost-effective in preventing self-harm and suicide over long time horizons (10 years to a lifetime) compared to no intervention, based on one average quality (Doran et al., Reference Doran, Ling, Gullestrup, Swannell and Milner2016) and seven high-quality studies (Ahern et al., Reference Ahern, Burke, McElroy, Corcoran, McMahon, Keeley, Carli, Wasserman, Hoven, Sarchiapone, Apter, Balazs, Banzer, Bobes, Brunner, Cosman, Haring, Kaess, Kahn and Wasserman2018; Crosland et al., Reference Crosland, Ho, Hosseini, Vacher, Skinner, Natsky, Rosenberg, Hasudungan, Huntley, Song, Lee, Marshall, Occhipinti and Hickie2024; Garraza et al., Reference Garraza, Peart Boyce, Walrath, Goldston and McKeon2018; Kinchin & Doran, Reference Kinchin and Doran2017; Lebenbaum et al., Reference Lebenbaum, Cheng, de Oliveira, Kurdyak, Zaheer, Hancock-Howard and Coyte2020; Stelmach et al., Reference Stelmach, Kocher, Kataria, Jackson-Morris, Saxena and Nugent2022; Vasiliadis et al., Reference Vasiliadis, Lesage, Latimer and Seguin2015).
In the US, a multi-level intervention (gatekeeper training, hotlines, education, screening) was cost-saving for youths (ages 16–23) with a ROI of 4.5 from a healthcare perspective (Garraza et al., Reference Garraza, Peart Boyce, Walrath, Goldston and McKeon2018). However, similar interventions in Australia were not cost-effective for children and young people (aged below 25) with psychological distress from healthcare and societal perspectives (Crosland et al., Reference Crosland, Ho, Hosseini, Vacher, Skinner, Natsky, Rosenberg, Hasudungan, Huntley, Song, Lee, Marshall, Occhipinti and Hickie2024). Nevertheless, a multi-level intervention (awareness trainings, suicide intervention skills) for construction workers in Australia demonstrated positive ROIs of 1.5–4.6 across 5-year and lifetime horizons from a societal perspective (Doran et al., Reference Doran, Ling, Gullestrup, Swannell and Milner2016; Kinchin & Doran, Reference Kinchin and Doran2017). In Canada, two studies also found multi-level interventions (awareness campaigns, training, psychosocial interventions) to be cost-effective (Lebenbaum et al., Reference Lebenbaum, Cheng, de Oliveira, Kurdyak, Zaheer, Hancock-Howard and Coyte2020) or cost-saving (Vasiliadis et al., Reference Vasiliadis, Lesage, Latimer and Seguin2015) compared to no intervention over a lifetime from both healthcare and societal perspectives.
Globally, a study across 36 HICs and LMICs found a multi-level intervention (awareness campaigns, training, and screening) cost-effective among adolescents from a societal perspective over a lifetime (Stelmach et al., Reference Stelmach, Kocher, Kataria, Jackson-Morris, Saxena and Nugent2022). However, when components were examined separately in 10 European countries, their cost-effectiveness was uncertain from the education, health, and social care system perspective over 12 months (Ahern et al., Reference Ahern, Burke, McElroy, Corcoran, McMahon, Keeley, Carli, Wasserman, Hoven, Sarchiapone, Apter, Balazs, Banzer, Bobes, Brunner, Cosman, Haring, Kaess, Kahn and Wasserman2018).
Synthesis of findings
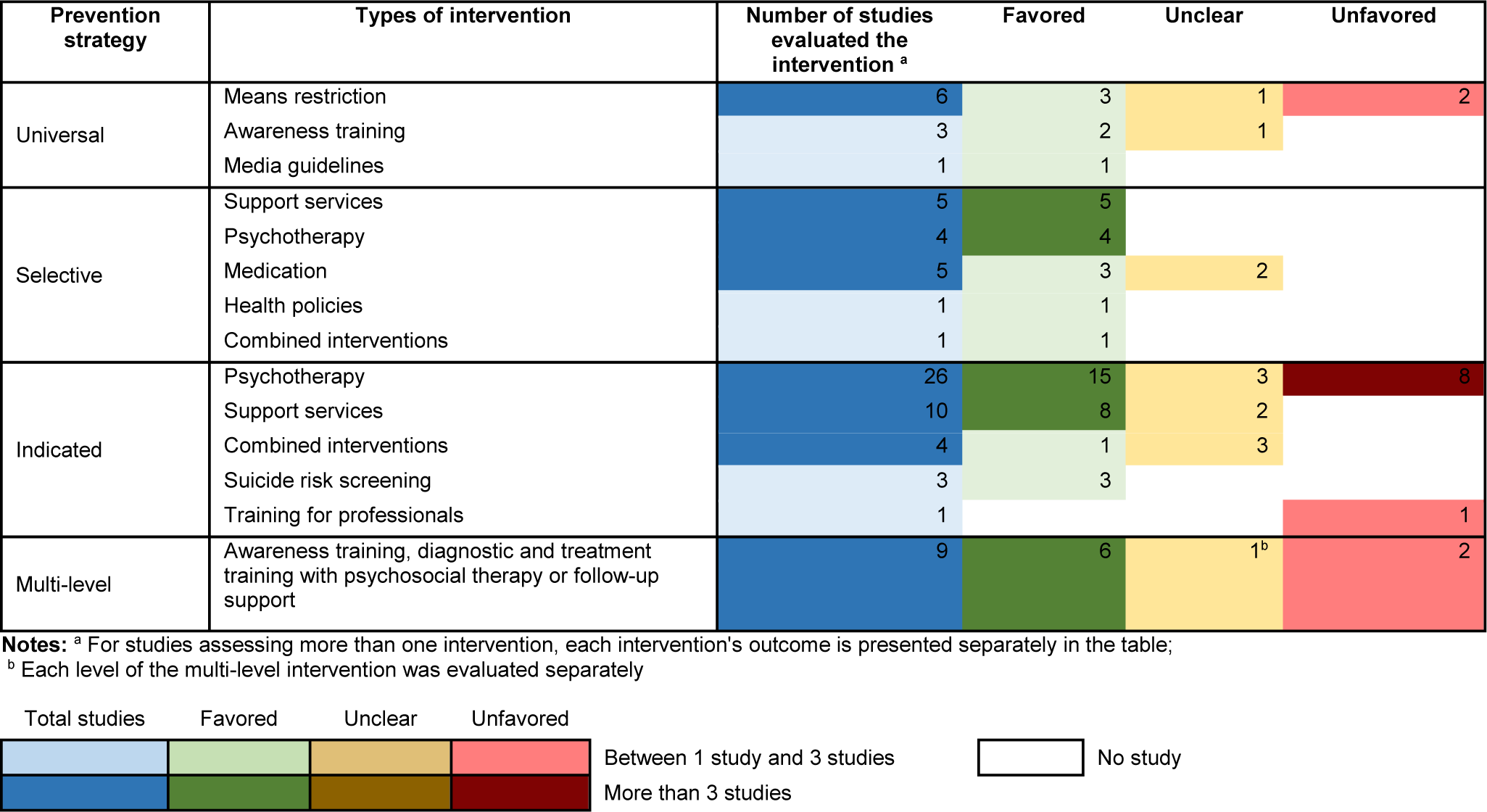
As shown in Table 2, the included studies showed high heterogeneity in the intervention characteristics and economic evaluation methods, leading to the use of a dominance ranking framework with three classifications – ‘favored’, ‘unfavored’, and ‘unclear’ (Figure 2). The majority (67%) of studies reported ‘favored’ outcomes. While a few interventions (e.g. universal means restriction, indicated psychotherapy) demonstrated either ‘unclear’ or ‘unfavored’ results, several selective (e.g. psychotherapy, support services) and indicated (e.g. suicide risk screening) interventions consistently generated ‘favored’ cost-effectiveness. Notably, cost-effectiveness varied across countries and health system contexts, with several interventions appearing more consistently cost-effective in the US than in countries with universal healthcare systems (e.g. Australia, the UK), likely reflecting higher baseline healthcare costs and greater potential for cost offsets.
Cost-effectiveness results and implications for decision makers.

Figure 2. Long description
The table has four main rows for prevention strategy: Universal, Selective, Indicated, and Multi-level. Each row lists types of intervention in the second column. The third column shows the number of studies evaluating each intervention, with blue for 1 to 3 studies and dark blue for more than 3. The next three columns show study outcomes: Favored (green), Unclear (yellow), and Unfavored (red). Universal strategies include means restriction (6 studies: 3 favored, 1 unclear, 2 unfavored), awareness training (3 studies: 2 favored, 1 unclear), and media guidelines (1 study: 1 favored). Selective strategies include support services (5 studies: 5 favored), psychotherapy (4 studies: 4 favored), medication (5 studies: 3 favored, 2 unclear), health policies (1 study: 1 favored), and combined interventions (1 study: 1 favored). Indicated strategies include psychotherapy (26 studies: 15 favored, 3 unclear, 8 unfavored), support services (10 studies: 8 favored, 2 unclear), combined interventions (4 studies: 1 favored, 3 unfavored), suicide risk screening (3 studies: 3 favored), and training for professionals (1 study: 1 unfavored). Multi-level strategies (awareness training, diagnostic and treatment training with psychosocial therapy or follow-up support) have 9 studies: 6 favored, 1 unclear, 2 unfavored. The legend at the bottom explains color codes and study count ranges. Notes clarify that multi-level interventions are evaluated separately and that each intervention’s outcome is presented individually.
Although psychotherapy was the most frequently evaluated indicated intervention (n = 26), its cost-effectiveness remained inconsistent across the studies. Most studies (n = 15) reported ‘favored’ cost-effectiveness for psychotherapy in many countries (e.g. Australia, the US, Canada), though the results remained ‘unclear’ for adults and ‘unfavored’ for adolescents in the UK. In cases of ‘unclear’ cost-effectiveness, the primary reason was the absence of defined cost-effectiveness thresholds for outcome-specific measures (i.e. cost per suicide case averted).
Observations from interventions evaluated by multiple studies across three 10-year periods (1995–2025) revealed notable cost-effectiveness trends. Selective support services (Comans, Visser, & Scuffham, Reference Comans, Visser and Scuffham2013; Pil et al., Reference Pil, Pauwels, Muijzers, Portzky and Annemans2013; Ross et al., Reference Ross, Zuromski, Reis, Nock, Kessler and Smoller2021; Sari et al., Reference Sari, de Castro, Newman and Mills2008) and selective psychotherapy (Gray et al., Reference Gray, Dawson, Grey and McMahon2011; Ross et al., Reference Ross, Zuromski, Reis, Nock, Kessler and Smoller2021; Zaloshnja et al., Reference Zaloshnja, Miller, Galbraith, Lawrence, DeBruyn, Bill, Hicks, Keiffer and Perkins2003) consistently demonstrated ‘favored’ cost-effectiveness across all periods. The cost-effectiveness of selective medication improved over time, shifting from ‘unclear’ in earlier periods (Duggan et al., Reference Duggan, Warner, Knapp and Kerwin2003; Freemantle et al., Reference Freemantle, House, Song, Mason and Sheldon1994) to ‘favored’ in the most recent period (Goren et al., Reference Goren, Rose, Smith and Ney2016; Groessl et al., Reference Groessl, Tally, Hillery, Maciel and Garces2018). Nevertheless, indicated psychotherapy exhibited inconsistent cost-effectiveness outcomes across multiple studies at different periods (Haddock et al., Reference Haddock, Pratt, Gooding, Peters, Emsley, Evans, Kelly, Huggett, Munro, Harris, Davies and Awenat2019; Spijker et al., Reference Spijker, Majo, Smit, Straten and Kerkhof2012; Tubeuf, Saloniki, & Cottrell, Reference Tubeuf, Saloniki and Cottrell2019; Tyrer et al., Reference Tyrer, Tom, Byford, Schmidt, Jones, Davidson, Knapp, MacLeod and Catalan2004).
Quality assessment
As shown in Table 3, most studies were of high quality (n = 61, 88%), with the majority of these (n = 47, 77%) published between 2015 and 2025, demonstrating an increase in publication quality and quantity over time. However, a few limitations persisted across several studies. Uncertainty and sensitivity analyses were often neglected or poorly conducted in many studies (e.g. Gray et al., Reference Gray, Dawson, Grey and McMahon2011; Tebbett-Mock et al., Reference Tebbett-Mock, Saito, McGee, Woloszyn and Venuti2020). Some studies inadequately addressed the generalizability of their findings and barriers to implementation (e.g. Tubeuf, Saloniki, & Cottrell, Reference Tubeuf, Saloniki and Cottrell2019; Whitmer & Woods, Reference Whitmer and Woods2013). Additionally, the range of costs analyzed did not fully align with the stated perspective in certain studies (e.g. Appleby et al., Reference Appleby, Morriss, Gask, Roland, Perry, Lewis, Battersby, Colbert, Green, Amos, Davies and Faragher2000; Latimer, Gariépy, & Greenfield, Reference Latimer, Gariépy and Greenfield2014).
Results of quality assessment using Drummond’s 10-item checklist

Table 3. Long description
The table contains 69 rows, each representing a study, and 14 columns. The columns are: number, lead author with year, ten checklist items (each scored 0, 0.5, or 1), total score, and quality rating. The checklist items are: 1. Was a well-defined question posed in answerable form 2. Was a comprehensive description of the competing alternatives given 3. Was the effectiveness of the program or services established 4. Were all the important and relevant costs and consequences for each alternative identified 5. Were costs and consequences measured accurately in appropriate physical units 6. Were the costs and consequences valued credibly 7. Were costs and consequences adjusted for differential timing 8. Was an incremental analysis of costs and consequences of alternatives performed 9. Was allowance made for uncertainty in the estimates of costs and consequences 10. Did the presentation and discussion of study results include all issues of concern to users. For each study, the checklist items are scored, summed for a total (maximum 10), and assigned a quality rating: High quality, Average quality, or Low quality. Most studies score between 7 and 10 and are rated High quality. A few studies, such as Whitmer and Gray, have lower totals (3 and 5) and are rated Low quality. The table allows comparison of methodological quality across studies.
Discussion
This review provides the most comprehensive analysis of existing economic evidence on self-harm and suicide prevention, covering a wide range of interventions and identifying significant growth in quality and quantity of publications, particularly in the past decade. Despite high heterogeneity, around 67% of the studies found suicide prevention to be cost-effective or cost-saving. Most cost-effectiveness evidence supported universal (e.g. awareness training), selective (e.g. support services), indicated (e.g. suicide risk screening, support services, psychotherapy for adults in Australia, the US, Canada), and multi-level interventions. However, our review also shows limited cost-effectiveness evidence of self-harm and suicide prevention in children, adolescents, and especially older adults, despite the high prevalence of such phenomena in these age groups (WHO, 2023). Similarly, there is significantly limited evidence from LMICs, which accounted for more than two-thirds of total suicides worldwide in 2021 (WHO, 2023).
Policy implications and directions for future research
More economic evaluations are urgently needed, particularly in the underrepresented populations and regions mentioned above, to accelerate the implementation of cost-effective interventions. Critically, scaling up cost-effective interventions requires careful consideration of important local factors (Lee et al., Reference Lee, Chisholm, Eddleston, Gunnell, Fleischmann, Konradsen, Bertram, Mihalopoulos, Brown, Santomauro, Schess and van Ommeren2021) because what works (or is cost-effective) in one context might not work (or be cost-effective) in another. For instance, system inefficiencies and higher baseline healthcare costs in the US may increase the potential for cost offsets from prevention, which may partly explain why preventive interventions often appear more cost-effective in US-based studies than in countries with universal healthcare. Furthermore, large-scale implementation requires a multidisciplinary approach impacting multiple sectors (WHO, 2021), which can lead to fragmentation of responsibility and funding across stakeholders.
Methodological issues of current evidence
While most studies were high-quality, heterogeneity in outcome measures and comparators still exists, making direct comparisons and firm conclusions difficult across studies. Although suicide impacts broader society, many studies did not adopt a societal perspective, underestimating costs related to lost productivity, social services, and burden on families and communities (Werdin & Wyss, Reference Werdin and Wyss2024). Additionally, inadequate discussion of broader implementation issues (e.g. generalizability and implementation barriers) and unclear cost-effectiveness thresholds, especially for clinical outcomes, might create hesitation and sub-optimal outcomes while implementing the interventions in the real-world.
Strengths and limitations
To our knowledge, this is the first comprehensive and up-to-date review of the cost-effectiveness of self-harm and suicide interventions that employed broad inclusion criteria, including ROI studies. These ROI studies, accounting for 10% of the studies included, showed strong returns for self-harm and suicide interventions. However, the present review may have missed unpublished studies, studies published in grey literature (due to our limited search of grey literature), and studies written in non-English languages, which may underestimate the cost-effectiveness evidence from LMICs. In addition, the available evidence may be influenced by publication and commissioning practices. Nevertheless, the inclusion of studies reporting unfavorable or inconclusive cost-effectiveness findings suggests that negative economic results are not systematically excluded from the peer-reviewed literature.
Conclusions
This review found strong and promising evidence for the cost-effectiveness of self-harm and suicide interventions, including several universal (e.g. awareness training), selective (e.g. psychotherapy, support services), indicated (e.g. suicide risk screening, support services, and psychotherapy for adults in countries including Australia, the US, Canada), and multi-level interventions. However, research on children, adolescents, and especially older adults remains limited, and evidence from LMICs, where most suicides occur, is also scarce. More economic evaluations for underrepresented populations and regions, as well as translational research on real-world implementation of suicide prevention, are urgently needed.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/S0033291726104814.
Funding statement
This study was conducted as part of the LIFEWAYS project with funding support from the Australian Government Department of Health, Disability and Ageing under the National Suicide Prevention Leadership and Support Program.
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.






 Open access
Open access