


Imagine a person who does not want to become pregnant living in a US state where abortion is banned after six weeks. They may never have intended to use long-acting reversible contraception (LARC), but the fear of an unintended pregnancy without access to abortion suddenly makes an IUD or contraceptive implant feel like their only choice. They weigh the risks: a pregnancy they cannot terminate in their home community without overcoming seismic barriers; the logistical challenges of seeking abortion in another state; the stigma attached to their potential abortion, adoption, and parenting options; the risks of pregnancy-related morbidity and mortality; the financial strain of raising a child without adequate social supports; and their fear that upcoming legal decisions may further restrict their access to abortion and contraception in the months and years to come. Their decision to seek LARC may appear voluntary, yet it is shaped by structural forces that constrain options and amplify risk.
While scholars have examined interpersonal and clinical forms of reproductive coercion, legal and policy forces remain undertheorized. This commentary introduces and defines sociolegal reproductive coercion as a distinct construct. Recent legal and policy shifts — such as the 2022 Dobbs decision that removed federal abortion protections, subsequent proliferation of state-level abortion bans, and 2025 Trump administration social safety net reductions — make this concept urgent for reproductive health research, especially where decision-making and clinical care are studied. In the following sections, we define the construct, situate it within existing scholarship, propose a conceptual framework, and outline implications for research, practice, and policy.
Defining Sociolegal Reproductive Coercion
Sociolegal reproductive coercion occurs when individuals feel pressured or constrained in their reproductive choices due to legal and policy landscapes that are reinforced and reified by social and cultural forces. Laws and policies that restrict reproductive health care — often framed by their proponents as neutral or protective — can exert coercive pressures. Unlike interpersonal coercion occurring within intimate relationshipsReference Grace, Anderson, Miller, Silverman and McCauley 1 or clinical settings,Reference Swan and Cannon 2 sociolegal reproductive coercion does not involve a single identifiable actor. Rather, it emerges from structural conditions that shape perceived and actual options. These forms of coercion are distinct but deeply intertwined: sociolegal pressures often interact with partner-perpetrated behaviors and provider practices, creating layered constraints on autonomy.
In the post-Roe United States, individuals may feel compelled to adopt highly effective contraceptive methods, even if otherwise unwanted, because pregnancy now carries heightened legal, social, and health risks — risks that have long been higher for Black people, Indigenous people, people of color, and people with low incomes.Reference Bach and Wasilczuk 3 Further, well-meaning healthcare providers may adjust their counseling with these risks in mind, amplifying patients’ perceptions of coercion and unintentionally constraining patient decision-making at multiple levels. Similarly, cuts to social safety net programs like the Supplemental Nutrition Assistance Program (SNAP) and Head Start may lead people who wish to parent to delay childbearing, fearing economic insecurity. Conversely, Medicaid cuts can create barriers to contraceptive access, discouraging use and leaving individuals vulnerable to unintended pregnancy. Abortion restrictions further limit options, reinforcing a sense of constrained choice. Sociolegal reproductive coercion is reinforced through clinical practice, as restrictive laws or institutional policies, such as abortion bans, force providers to alter what options, information, and guidance they can legally offer.
Legal and policy restrictions rarely operate in isolation. Instead, they interact with social and cultural forces — including norms and stigma surrounding sexuality, pregnancy, parenting, contraception, and abortion — amplifying coercive pressures. For example, religious norms, internalized stigma about young or single parenting, and intensive mothering ideologies may intersect within sociocultural power structures, like racism and ableism, to make certain choices feel obligatory rather than freely chosen. Importantly, these sociolegal dynamics are layered onto a historical and ongoing context of reproductive coercion disproportionately experienced by people of color, shaped by social, structural, and institutional racism both within and beyond clinical settings.Reference Brandi, Fuentes, Moniz, Harris and Wolfe 4 As noted in critiques of tiered-effectiveness counseling, provider bias and systemic inequities have long targeted marginalized communities for paternalistic contraceptive practices, particularly through promotion of provider-controlled methods like LARC, perpetuating racialized reproductive oppression under the guise of public health goals.Reference Brandi, Fuentes, Gomez, Fuentes, Allina and Donnelly 5 As such, we theorize that gender and sexual minority groups, people who live with disabilities and chronic health conditions, and young people also face disproportionate sociolegal reproductive coercion, alongside racial and ethnic minority communities.
Theoretical Positioning
This construct builds on and extends several existing frameworks that consider the structural and legal influences on reproductive decision-making. Jenny Higgins and colleagues have recently applied the dual control model of sexual responseReference Bancroft, Janssen, Janssen, Bancroft, Janssen and Nagoski 6 to abortion decision-making, highlighting how structural forces, alongside personal factors, act as brakes and accelerators to abortion access.Reference Higgins 7 Katrina Kimport’s work applies constrained choice theoryReference Bird, Rieker, Kahn, Moore, Glazer, Rieker and Read 8 to reproductive decision-making, illustrating how people navigate limited options that can lead them to “unchoose” abortion.Reference Kimport 9 Katie Watson uses the term “legislative coercion” to describe how laws governing abortion and adoption constrain pregnant people’s decision-making.Reference Watson 10 She argues that laws frame pregnancy as a profound ethical obligation rather than a personal choice, imposing new identity and ethical responsibilities onto pregnant people and forcing them into motherhood.Reference Watson 11 Building on these insights, sociolegal reproductive coercion extends beyond abortion and parenting choices to include contraception and pregnancy planning, highlighting how legal, policy, social, and cultural forces collectively constrain reproductive autonomy.
Social control theory also provides a useful backdrop for understanding how policy shapes decision-making. Classic formulations, such as those by HirschiReference Hirschi 12 and later extensions by Black,Reference Black 13 conceptualize social control as mechanisms that regulate conduct and maintain social order. Policies often function as instruments of governance, deliberately structuring incentives and constraints to encourage compliance. However, these frameworks primarily emphasize regulation and conformity rather than the lived experience of coercion. This critique echoes Foucault’s argument that law, policy, and institutions, such as medicine, function as coercive mechanisms of social control, disciplining individuals under the guise of care and governance.Reference Foucault and Foucault 14 While these theories explain why rules exist and how they maintain order, they do not interrogate how individuals experience these rules as coercive forces in deeply personal domains such as reproduction.
Sociolegal reproductive coercion builds on this foundation but adds critical nuance. It shifts the focus from abstract compliance to embodied autonomy, showing how structural forces jointly operate to constrain reproductive decision-making under the guise of choice. While social control theory recognizes that norms and sanctions influence behavior, it rarely addresses the intersection of legal mandates and cultural stigma in shaping intimate decisions. By naming sociolegal reproductive coercion, we foreground the normative and structural pressures that compel individuals toward or away from contraception, pregnancy, parenting, or abortion — not through overt prohibition alone, but through a web of legal and policy restrictions and social judgments that make certain choices feel obligatory. Importantly, these pressures reverberate in clinical settings, where providers — responding to the same sociolegal environment — may alter their practice in ways that unintentionally perpetuate coercion and constrain patient autonomy, either paternalistically or in compliance with legal and policy mandates.
Recent scholarship has laid important groundwork for understanding structural pressures on reproductive decision-making. Brian and colleagues theorize how policy operates as a form of “subtle coercion,” framing reproductive choices within systems of power and inequality and situating these dynamics within broader structures of reproductive oppression.Reference Brian, Grzanka and Mann 15 Recently, empirical research has demonstrated how the post-Dobbs legal and policy environment influences clinicians’ counseling practices, showing that, in response to abortion restrictions, providers often adjust their clinical recommendations in ways that overemphasize pregnancy prevention and LARC use.Reference Bullington 16 These shifts, while intended to protect patients, risk compounding coercion by narrowing the range of options presented and framing certain choices as more responsible or necessary. They also contribute to moral injury among clinicians committed to patient-centered care, as providers navigate tensions between professional ethics and restrictive laws.
Building on these contributions, the framework of sociolegal reproductive coercion offers conceptual clarity by explicitly naming and defining the coercive mechanisms embedded in law and policy. While the above works illuminate structural constraints and their impact on agency, sociolegal reproductive coercion consolidates these insights under a unified construct that captures legal, policy, and sociocultural dimensions of coercion. This framework extends prior scholarship by theorizing how legal and policy landscapes and social norms interact to pressure reproductive decision-making, creating conditions where choices feel compelled rather than freely made. Importantly, this approach is patient-centered: it reflects how individuals experience coercion in real-world contexts. Patients often describe coercion not only as overt force but as subtle pressures that make certain options feel nonviable.Reference Higgins, Kramer, Ryder, Senderowicz and Niles 17 By centering these lived experiences, sociolegal reproductive coercion provides a conceptual tool that aligns with how patients understand autonomy and constraint, bridging theoretical insight with clinical and policy relevance.
Conceptual Model
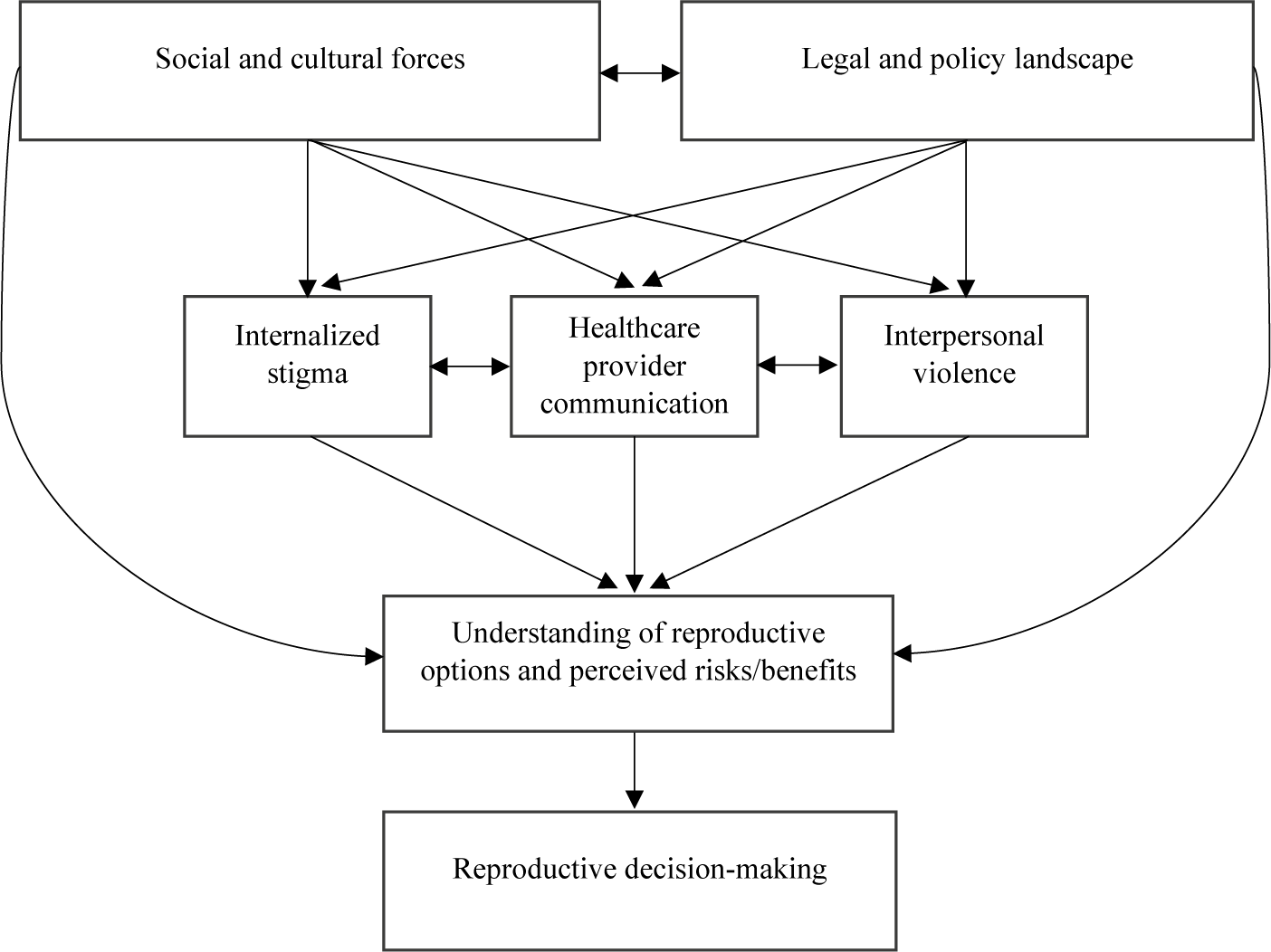
As shown in Figure 1, the sociolegal landscape functions through interconnected pathways. Laws, policies, and sociocultural forces shape one another and, together, create conditions that can amplify stigma and influence communication between healthcare providers and their patients. In some cases, these shifts in norms and policy contribute to coercion from healthcare providers, who may alter contraceptive counseling practices or omit abortion information, ultimately impacting patients’ reproductive decision-making. For those in violent or controlling interpersonal relationships, these sociolegal forces make it more difficult to leave or exercise autonomy. Moreover, changes in policy or law can embolden perpetrators of these behaviors. These dynamics shape how people understand and weigh the risks and benefits of different reproductive options, as individuals anticipate legal, financial, social, and health consequences of their choices. These perceptions create pressure, making choices feel compelled rather than voluntary. This sense of constraint can lead to outcomes such as using a nonpreferred contraceptive method, avoiding pregnancy, or seeking abortion under duress. Over time, these pressures can contribute to mental health challenges, substance use, adverse pregnancy outcomes, and downstream effects on infant and child health. This model is embedded in a society with hegemonic power structures, meaning that some groups experience greater constraint, surveillance, and risk than others.
Conceptual model of the sociolegal reproductive coercion process.

Figure 1. Long description
The flowchart is organized into four vertical layers.
* Top layer: Two boxes labeled Social and cultural forces and Legal and policy landscape are connected by a horizontal double-headed arrow.
* Second layer: Three boxes labeled Internalized stigma, Healthcare provider communication, and Interpersonal violence. Horizontal double-headed arrows connect the center box to the two outer boxes.
* Third layer: A single box labeled Understanding of reproductive options and perceived risks forward slash benefits.
* Bottom layer: A final box labeled Reproductive decision-making.
Flow of influence: Downward arrows from both top-layer boxes point to each of the three boxes in the second layer. Additionally, two long curved arrows bypass the second layer, originating from the top-layer boxes and pointing directly to the third-layer box. All three boxes in the second layer have downward arrows pointing to the third-layer box. Finally, a single downward arrow connects the third-layer box to the bottom-layer box.
Implications for Research, Practice, and Policy
Empirical work must examine how policy changes alter reproductive intentions and decisions. Researchers should investigate how perceptions of legal risk shape reproductive decision-making and analyze how power and privilege mediate experiences of sociolegal coercion. This is a methodologically challenging task, as structural constraints, social dynamics, and individual motivations are profoundly interwoven in reproductive decision-making. Developing validated instruments to assess perceived sociolegal pressure and its impact on autonomy is essential.
Healthcare providers must recognize structural pressures shaping their practice and their patients’ choices. In contexts of sociolegal reproductive coercion, directive approaches risk compounding coercion. Providers should prioritize patient-centered care that explicitly acknowledges systemic constraints and avoids framing certain options as inherently more responsible. Training and guidance should help clinicians navigate these tensions, ensuring that clinical decision-making remains evidence-based and autonomy-preserving even under restrictive policy environments.
Advocates and policymakers must confront how legislation can function as coercion, undermining bodily autonomy and violating principles of reproductive justice.Reference Ross and Solinger 18 Policies should promote health, wellness, and autonomy — not restrict them. Reforms should include expanding Medicaid coverage for comprehensive reproductive care, safeguarding abortion accessibility, affordability, acceptability, and quality of care, funding comprehensive contraception and (in)fertility services, and strengthening social safety nets. Policy initiatives should support people’s rights to parent, to choose not to parent, and to raise families safely in their communities. Echoing Higgins and colleagues’ application of the dual control model to abortion decision-making,Reference Higgins 19 just as structural forces can serve as brakes, policies that affirm autonomy (e.g., universal coverage for reproductive care, robust parental leave, and protections against discrimination) can actively enable and accelerate individuals’ ability to make freely chosen reproductive decisions.
Conclusion
In the wake of seismic legal and policy shifts at the state and national levels, theorizing sociolegal reproductive coercion is critical for safeguarding reproductive autonomy. This construct illuminates how laws, policies, and social and cultural dynamics can operate as coercive forces, shaping both the practice of reproductive care and people’s decisions under structural constraints. Interdisciplinary research is urgently needed to validate and operationalize this framework, ensuring that reproductive autonomy remains a central tenet of medicine, health, and policy.
Disclosures
The authors have nothing to disclose.

 Open access
Open access