


Introduction
Within UK National Health Service (NHS) community mental health services, long waiting times for psychological therapy have prompted the introduction of brief psychological interventions (BPIs). BPIs are structured, evidence-based interventions that can be delivered by trained and supervised non-specialists. Typically, they include components of longer-term evidence-based psychological interventions such as cognitive behavioural therapy (CBT) and dialectical behaviour therapy (DBT), and are delivered over fewer sessions, by staff with less specialised training (paraprofessionals). These paraprofessionals are typically trained in BPIs over two days, supervised by clinical psychologists and may be employed in roles such as support time recovery workers, peer support workers and assistant psychologists (Roberts et al., Reference Roberts, Travers-Hill, Coker, Troup, Casey, Parkin and Kim2021).
Mental health systems worldwide are under mounting pressure due to rapidly increasing demand and an insufficient workforce of qualified professionals. The British Medical Association (BMA) reports that although demand for mental health services in England increased by 21% between 2016 and 2019, the specialist workforce has scarcely grown and many staff groups remain under-resourced (BMA, 2024). In countries with the greatest need, the workforce deficit is dramatic. A review of 58 low- and middle-income countries estimated an average shortage of 22.3 full-time equivalent mental health professionals per 100,000 population in low-income countries and of 26.7 professionals per 100,000 population in middle-income countries to meet current need (Bruckner et al., Reference Bruckner, Scheffler, Shen, Yoon, Chisholm, Morris, Fulton, Dal Poz and Saxena2011). These trends underscore the urgency of implementing scalable models of care, including BPIs, to extend reach in settings where specialist capacity is limited. Integrating paraprofessionals into healthcare settings has the potential to decrease reliance on accredited therapists and broaden access to services while reducing treatment costs, particularly in under-served populations (Morrison et al., Reference Morrison, Chang, Xie and Kim2025).
BPIs have been shown to be effective in primary care settings (Wakefield et al., Reference Wakefield, Kellett, Simmonds-Buckley, Stockton, Bradbury and Delgadillo2021) and with specific populations such as refugees (de Graaff et al., Reference de Graaff, Cuijpers, Acarturk, Bryant, Burchert, Fuhr, Huizink, de Jong, Kieft, Knaevelsrud, McDaid, Morina, Park, Uppendahl, Ventevogel, Whitney, Wiedemann, Woodward and Sijbrandij2020), families affected by addiction (Bhatia et al., Reference Bhatia, Velleman, Velleman, Garber, Catalano and Nadkarni2022) and people with money, employment or housing problems (Barnes et al., Reference Barnes, Haase, Scott, Linton, Bard, Donovan, Davies, Dursley, Williams, Elliott, Potokar, Kapur, Hawton, O’Connor, Hollingworth, Metcalfe and Gunnell2018). Evidence regarding their effectiveness in secondary care settings is beginning to emerge in small studies. BPIs in anxiety and behavioural activation delivered by mental health workers without core therapeutic training were associated with meaningful improvements in wellbeing and functioning and reduction in symptoms of low mood and anxiety in the 39 participants with pre and post data (Roberts et al., Reference Roberts, Travers-Hill, Coker, Troup, Casey, Parkin and Kim2021). As little as 6–10 sessions enabled approximately one-third of 160 treatment completers to be discharged from secondary care services (Casey et al., Reference Casey, Parkin, Maciag, Page, Masson and Kim2019). An evaluation of a BPI in distress tolerance delivered to 43 clients with moderate to severe mental health conditions reported significant improvements in distress tolerance, low mood, anxiety, well-being and functioning with medium to large effect sizes (Wright et al., Reference Wright, Travers-Hill, Gracey, Troup, Parkin, Casey and Kim2020).
Distress tolerance skills have been shown to reduce emotional reactivity, crisis behaviours, self-harm, and substance-use relapse across a range of clinical populations, including borderline personality disorder, mood disorders and post-traumatic stress disorder (PTSD) (Linehan, Reference Linehan1993; Neacsiu et al., Reference Neacsiu, Rizvi and Linehan2010). In obsessive compulsive disorder (OCD), emotional regulation deficits have been linked with obsessive beliefs (Berman et al., Reference Berman, Shaw and Wilhelm2018) and patients with lower distress tolerance have been found to have higher depression symptomatology (Ellis et al., Reference Ellis, Vanderlind and Beevers2013). Increasing an individual’s ability to withstand temporary psychological discomfort and confront difficult emotions is considered a key mechanism through which healthier behavioural change is achieved (Hayes et al., Reference Hayes, Wilson, Gifford, Follette and Strosahl1996). Despite a good theoretical basis for interventions targeted at improving distress tolerance, there is relatively little empirical evidence reporting effectiveness as a stand-alone manualised intervention. Brief distress tolerance interventions have been associated with improved outcomes in treatments for substance use (Bornovalova et al., Reference Bornovalova, Gratz, Daughters, Hunt and Lejuez2012; Langdon et al., Reference Langdon, Scherzer, Ramsey, Carey, Rich and Ranney2021; Macatee et al., Reference Macatee, Albanese, Okey, Afshar, Carr, Rosenthal, Schmidt and Cougle2021; Stein et al., Reference Stein, Herman, Moitra, Hecht, Lopez, Anderson and Brown2015), adolescents with and without anorexia nervosa (Miranda et al., Reference Miranda, Matheson, Datta, Whyte, Yang, Schmiedmayer, Ravi, Aalami and Lock2025), attention deficit hyperactive disorder (ADHD) (Ulusoy et al., Reference Ulusoy, Bilican and Gormez2025), hypertension (Boostani et al., Reference Boostani, Ezadikhah and Sadeghi2017) and problematic internet use (El-Ashry et al., Reference El-Ashry, Hussein Ramadan Atta, Alsenany, Farghaly Abdelaliem and Abdelwahab Khedr2023). Distress tolerance skills training has also been shown to be a mechanism for change in depression, suicidal behaviour (Yardley et al., Reference Yardley, McCall, Savage and Newton2019), anxiety and anger control (Neacsiu et al., Reference Neacsiu, Rizvi and Linehan2010).
Despite these findings regarding effectiveness of the brief interventions in distress tolerance, little is known about which clients are most likely to benefit. The current study builds on the findings reported by Wright et al. (Reference Wright, Travers-Hill, Gracey, Troup, Parkin, Casey and Kim2020) of the first year of routinely collected data in a Community Mental Health Team (CMHT) between 2017 and 2018. Since then, the intervention has been offered to hundreds of clients and a review is now timely.
The Cambridgeshire and Peterborough CMHT provides NHS, multi-disciplinary, secondary care for adults with moderate to severe mental health conditions. Care includes assessment, care planning, psychological and pharmacological interventions, and social and functional rehabilitation. Manualised BPIs are offered in behavioural activation, anxiety management and distress tolerance (Maciag et al., Reference Maciag, Travers-Hill, Morrison and Kim2023). The CMHT works closely with primary care, crisis services, and specialist teams to create integrated pathways, although rising demand and waiting times continue to pose challenges to service capacity and continuity of care. High caseloads, high vacancy rates in nursing, and long wait times particularly for psychology have been identified (Care Quality Commission, 2024). An informal audit of data from 2020 indicates that the average waiting time in the service as a whole from referral to treatment was 27 months, and from referral to reprocessing work for PTSD/complex PTSD was 29 months (unpublished service data). Treatment for severe mental health conditions is not equally accessible and in rural or poorly connected areas, the physical location of CMHT bases (which operate only during working hours) can make attendance logistically difficult (Cambridgeshire & Peterborough Insight, 2025). BPIs are well placed to target some of these challenges due to flexibility of delivery and fewer sessions than other models.
Given the challenges described above, it is vital that the service makes the best use of capacity by offering interventions to those who will benefit most. The current study aimed to (1) assess the completeness of outcome data, (2) evaluate the effectiveness of the intervention, and (3) identify characteristics of responders versus non-responders to inform clinical decision-making and maximise benefit for clients.
Method
Design
Data were obtained retrospectively from standard NHS clinical records based on measures routinely completed during care. The quality of the data was then evaluated by reviewing the completion of the measures at two time points: pre- and post-intervention.
A within-subject, repeated measures design was used to compare pre to post scores on one of the two measures of distress tolerance, depending on data completion. This comparison was then used to calculate reliable change scores (Jacobson and Truax, Reference Jacobson and Truax1991) and identify clients either as ‘responders’ or ‘non-responders’. Responders were defined as those clients who had clinically significant change in the direction of improvement with 95% confidence on either the Distress Tolerance Scale (DTS) or Difficulties in Emotion Regulation Scale (DERS). A between groups design was used to compare responders versus non-responders on the pre-intervention measures.
Participants
The service consists of two adult CMHTs within one county, offering BPIs across pathways for affective disorders and psychosis. The affective pathway includes individuals with moderate to severe mood and anxiety disorders, OCD, or PTSD, while the psychosis pathway serves those with schizophrenia-spectrum and bipolar disorders with psychotic features. The BPI in distress tolerance is offered trans-diagnostically across both pathways. Exclusions for BPI include substance use problems, need for further assessment, ongoing psychological intervention, previous lack of engagement with BPI, overwhelming current personal difficulties or better suitability of another service. Participants were all clients referred to the intervention between 2017 and 2023 (n=463). The demographic profile of the sample was broadly comparable to that reported in the first year of data collection (Wright et al., Reference Wright, Travers-Hill, Gracey, Troup, Parkin, Casey and Kim2020). The mean age of participants was 31 years (range=17–64 years), and 72.4% were female, compared with 29.9 years and 84.2% female in the earlier evaluation. The inclusion criteria for the responder analysis were (1) client identified by the service as having completed the BPI, and (2) client completed at least one measure of distress tolerance at both pre- and post-BPI time points.
Clients receiving NHS care are informed that information about them is routinely collected to support their treatment and may also be used to improve services or support research. Individuals can choose whether or not to allow their data to be used for research via the National Data Opt-Out system.
Distress tolerance intervention
The DT BPI manual was developed by two senior clinical psychologists in the service. It consists of self-help modules (Saulsman and Nathan, Reference Saulsman and Nathan2012) and DBT concepts (Linehan, Reference Linehan1993) aimed at increasing distress tolerance skills. The typical structure is 6–8 sessions lasting one hour covering psychoeducation, coping strategies for tolerating distress and regulating emotions, and action plans for both distress tolerance and emotional regulation. Training in BPIs consists of two half-days with additional ‘top-up’ sessions, and supervision is provided by clinical psychologists. Further detail on the development and delivery of the BPIs has been reported elsewhere (Roberts et al., Reference Roberts, Travers-Hill, Coker, Troup, Casey, Parkin and Kim2021; Wright et al., Reference Wright, Travers-Hill, Gracey, Troup, Parkin, Casey and Kim2020). The healthcare providers delivering the BPI were a mix of qualified psychologists and paraprofessionals including trainee clinical psychologists, assistant psychologists, clinical associate psychologists, support workers and nurses.
Measures
All the measures described are routinely collected as part of the DT BPI in the service and requested from all clients pre- and post-intervention. The service aims for consistent completion and requests measures at least twice if required.
The dataset includes two measures of distress tolerance. The Difficulties in Emotion Regulation Scale (DERS) (Gratz and Roemer, Reference Gratz and Roemer2004) has 36 items with a total score range of 36–180. Higher scores indicate more problems with emotion regulation. The authors report high internal consistency (Cronbach’s alpha=0.93), good test–retest reliability (r=0.88) and adequate construct and predictive validity. Excellent internal consistency (Cronbach’s alpha=0.95) and good construct validity (r=0.7 correlation with the Acceptance and Action Questionnaire) have also been reported in an in-patient sample (Fowler et al., Reference Fowler, Charak, Elhai, Allen, Frueh and Oldham2014).
The Distress Tolerance Scale (DTS) (Simons and Gaher, Reference Simons and Gaher2005) has 15 items, rated from 1 (strongly agree) to 5 (strongly disagree). Higher scores indicate greater ability to tolerate distress. It consists of four subscales: tolerance, absorption, appraisal and regulation. The authors report good internal consistency (Cronbach’s alpha=0.82) and moderate test–retest reliability (r=0.61). Significant negative associations were found with substance use coping, negative affect, and expectancy of negative consequences. Anxiety was measured using the Generalised Anxiety Disorder Assessment (GAD-7) (Spitzer et al., Reference Spitzer, Kroenke, Williams and Lowe2006), a 7-item measure scored on a 4-point Likert scale with a range of 0–21. Higher scores indicate higher levels of anxiety and the authors reported good internal consistency (Cronbach’s alpha=0.92) and test–retest reliability (0.83) in a primary care population. Validity was indicated by strong correlation with clinician-administered diagnostic interviews (r=0.83) and the Beck Anxiety Inventory (r=0.72). Depression was measured using the Patient Health Questionnaire (PHQ-9), a 9-item measure on a 4-point Likert scale with a total score range of 0–27, in which higher scores indicate greater levels of depression symptoms. In primary care populations, it has diagnostic validity for major depressive disorder, good internal reliability (Cronbach’s alpha=0.89) and responsiveness to change (Kroenke et al., Reference Kroenke, Spitzer and Williams2001). Convergent validity with the Hospital Anxiety and Depression Scale’s depression subscale has been reported as 0.68 (Cameron et al., Reference Cameron, Crawford, Lawton and Reid2008).
The Short Warwick–Edinburgh Mental Wellbeing Scale (SWEMWBS) is a 7-item measure of mental wellbeing and functioning scored on a 5-point Likert scale with total scores ranging from 7 to 35. Higher scores indicate greater wellbeing (Bartram et al., Reference Bartram, Sinclair and Baldwin2013). The SWEMWBS has shown good internal reliability (Cronbach’s alpha=0.90) in an out-patient population experiencing anxiety, depression and schizophrenia, and convergent validity with the Satisfaction with Life Scale (Vaingankar et al., Reference Vaingankar, Abdin, Chong, Sambasivam, Seow, Jeyagurunathan, Picco, Stewart-Brown and Subramaniam2017).
The Work and Social Adjustment Scale (WSAS) is a 5-item measure of impaired functioning in daily life with a total score range of 0–40, in which higher scores indicate greater impairment. It has been found to have good internal reliability (Cronbach’s alpha=0.79 to 0.94), test–retest reliability (0.73) and good sensitivity to change (Mundt et al., Reference Mundt, Marks, Shear and Greist2002).
Analysis
Data completion
Data completion was reviewed pre- and post-intervention. Frequencies and percentages missing for each measure and demographic were reported and patterns of missing data observed.
Reliable and clinical change analysis
Reliable change scores were calculated for both the DTS and DERS total scores using the Reliable and Clinical Change Generator for Windows (Devilly, Reference Devilly2005), based on methodology outlined by Jacobson and Truax (Reference Jacobson and Truax1991). This requires the pre and post difference score, divided by the standard error of the difference (SEdiff), which accounts for measurement error and test reliability. If the resulting value is greater than ±1.96, the change is considered statistically reliable at the 95% confidence level. A measure of internal consistency of the measure, rather than test–retest reliability, was adopted in both cases, as it is considered most in line with classical reliability theory (Lambert and Bailey, Reference Lambert, Bailey and Cooper2012). It also excludes expected change over the testing interval (Evans et al., Reference Evans, Margison and Barkham1998). Internal consistency coefficients could not be calculated within the sample due to the absence of item-level data. Instead, published reliability estimates from the original scale developers were adopted. The developers of the DTS and DERS report an alpha co-efficient of 0.89 (sample SD=0.76) (Simons and Gaher, Reference Simons and Gaher2005) and 0.93 (sample SD=19.8) (Gratz and Roemer, Reference Gratz and Roemer2004), respectively. While sample-specific reliability is desirable in that it reflects precision of measurement in the local context, using coefficients from a published sample avoids the instability that can arise when reliability is estimated from small or homogeneous clinical samples (Morley and Dowzer, Reference Morley and Dowzer2014).
Clinical pre-intervention means and SD values were drawn from the current sample, as recommended by Evans et al. (Reference Evans, Margison and Barkham1998) (DTS M=2.13, SD=0.79, n=243; DERS M=123.79, SD=27.63, n=236). Pre-intervention mean scores for a non-clinical sample were taken for the DTS from a study of 650 undergraduate students (M=3.48, SD=0.84, n=650) (Sandín et al., Reference Sandín, Simons and Valiente2017) and for the DERS from a study recruiting from the community (M=78.03, SD=23.95, n=482) (Bjureberg et al., Reference Bjureberg, Ljótsson, Tull, Hedman, Sahlin, Lundh, Bjärehed, DiLillo, Messman-Moore, Gumpert and Gratz2016). A cut-off point accounting for both the clinical and non-clinical samples could then be adopted. As the normal and clinical distributions intersected, clinical cut-off C (the score where they intersect) was used to determine clinically significant change (Jacobson and Truax, Reference Jacobson and Truax1991).
Responder analysis
t-tests and chi-square tests were used to compare responders versus non-responders on the pre-intervention measures (demographics, DERS, DTS, PHQ-9, GAD-7, SWEMWBS, WSAS). Additionally, responders were compared with all other participants, i.e. non-responders and response unknown due to incomplete data or client disengagement, in order to shed light on differences between responders and all other clients offered the DT BPI.
Results
The flow of participants is described in Fig. 1 using information provided by the service regarding completion, disengagement and a change in circumstances for the client which rendered the BPI no longer suitable. At the time of analysis, all those referred had been discharged from the BPI. Overall, there is considerable attrition in clients referred for the BPI: only 242 of 463 clients (52.3%) were marked as ‘intervention complete’ by the service. Around a third of the sample disengaged from the BPI overall (28.7%). Approximately 16% of those referred did not attend a first session. Of those who attended at least one session, 64.4% are known to have completed the BPI. The majority (85.1%) of those who started but did not complete, reportedly did so due to ‘patient disengagement’ or the BPI no longer being considered suitable.
Flow of participants.

Data completion
Data completion is reported in Table 1. Demographic data completion ranged from 88.6% to 100%. Outcome data completion ranged from 57.4% to 78.1%, with the WSAS appearing to be the least commonly used/completed measure within the service. There was little difference between the completion rates pre-BPI (individual measures completion rates of 57.4 to 75%) and post BPI (57.4 to 78.1%). Data were less complete for outcome measures specific to the DT BPI (DTS and DERS) compared with outcome measures collected across all BPIs (SWEMWBS, PHQ-9, GAD-7 and WSAS).
Data completion rates for distress tolerance BPI

DNA, did not attend; sWEMWBS, Short Warwick–Edinburgh Mental Wellbeing Scale; PHQ9, Patient Health Questionnaire 9 items; GAD7, Generalised Anxiety Disorder Assessment 7 items; WSAS, Work and Social Adjustment Scale; DTS, Distress Tolerance Scale, DERS, Difficulties in Emotion Regulation Scale.
*Of those who attended at least one session (n = 463).
**Of those marked “intervention completed” by the service (n = 242).
Reliable and clinically significant change
Reliable and clinically significant change status was calculated for the DTS and DERS for those participants identified by the service as having completed the BPI (n=242) who also had pre and post total score data. The results are shown in Table 2. Of those with complete pre and post DTS data, approximately one-third had reliable improvement, a little over half had no reliable change and a small percentage showed reliable deterioration. Clinically significant improvement (only possible in the context of reliable improvement) was noted for around a quarter of the sample. Of those with complete pre and post DERS data, approximately half had reliable improvement, approximately one-third had no reliable change and for the DTS, a small number had reliable deterioration. Clinically significant improvement was noted for just over one-quarter of the sample.
DTS and DERS reliable and clinically significant change analysis

DTS, Distress Tolerance Scale; DERS, Difficulties in Emotion Regulation Scale.
Responder analysis
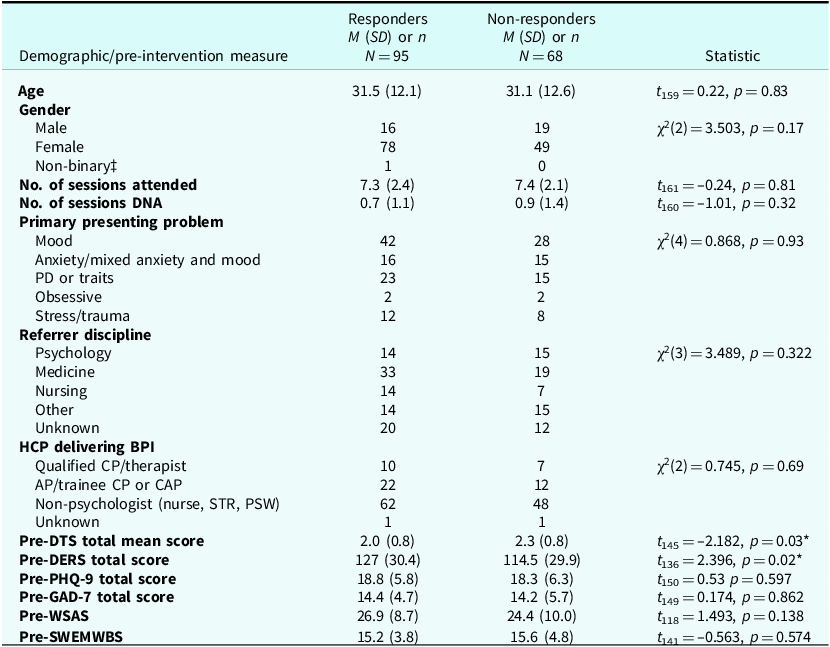
Participants were classified as responders if they had reliable improvement pre- to post-intervention on either the DTS or the DERS. They were classified as non-responders if they had reliable deterioration or no change. It was possible to classify 163 participants as responder/non-responder, based on them having a reliable change score for either the DTS or DERS. Demographics and baseline measures are reported for responders versus non-responders (Table 3) and responders versus the rest of the sample, i.e. those who did not respond and those where the response could not be calculated (Table 4).
Comparison of pre-intervention measures for responders versus non-responders

sWEMWBS, Short Warwick–Edinburgh Mental Wellbeing Scale; PHQ9, Patient Health Questionnaire 9 items; GAD7, Generalised Anxiety Disorder Assessment 7 items; WSAS, Work and Social Adjustment Scale; DTS, Distress Tolerance Scale, DERS, Difficulties in Emotion Regulation Scale; M, mean; SD, Standard Deviation; DNA, did not attend; PD, Personality Disorder; HCP, Healthcare Professional; STR, Support Time and Recovery Worker; PSW, Personal Support Worker; CPN, CP: Clinical Psychologist; CBT, Cognitive Behavioural Therapy; CAP, Trainee Clinical Associate Psychologist; AP, Assistant Psychologist; CI, confidence interval.
‡Not included in Chi Square analysis.
*p<0.05.
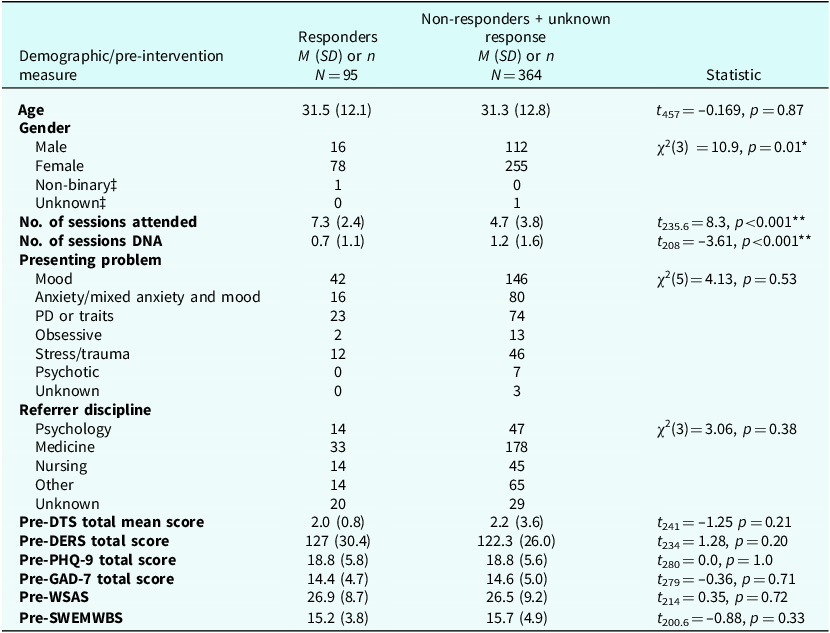
Comparison of pre-intervention measures for responders versus non-responders + unknown response

sWEMWBS, Short Warwick–Edinburgh Mental Wellbeing Scale; PHQ9, Patient Health Questionnaire 9 items; GAD7, Generalised Anxiety Disorder Assessment 7 items; WSAS, Work and Social Adjustment Scale; DTS, Distress Tolerance Scale, DERS, Difficulties in Emotion Regulation Scale; M, mean; SD, Standard Deviation; DNA, did not attend; PD, Personality Disorder; CI, confidence interval.
‡ Not included in Chi Square analysis.
*p<0.05; **p<0.01
No significant differences between responders and non-responders were identified on any of the demographic and baseline measures, except for distress tolerance. Responders were found to have significantly lower DTS total scores (p<0.05) and significantly higher DERS total scores (p<0.05) pre-BPI compared with non-responders.
When responders were compared with the rest of the sample (non-responders and those where response could not be calculated), significant differences were found for gender, number of sessions attended and DNA. A chi-square test of independence performed to evaluate the relationship between responder status and client gender found that the relationship between these variables was significant, χ2 (d.f.=3, n=463)=10.9, p=0.01. Disproportionately fewer than expected males were classified as responders. Responders were significantly more likely to have attended a greater number of sessions (t 235.6=8.3, p<0.001) and DNA a fewer number of sessions (t 208=–3.61, p<0.001) than the rest of the sample. No significant difference between responders and the rest of the sample was found for age, presenting problem, referrer discipline, the role of the HCP delivering the BPI, pre-treatment depression, anxiety, well-being or distress tolerance scores.
A steady decline in referrals for DT BPI was noted since data collection began in 2017 (106 referrals) to 2023 (7 referrals). The percentage of referrals classified as responder (Fig. 2) rose from 17.9% to 31.4% in the first year. The percentage of responders fell below 20% between 2019 and 2021, followed by a sharp increase to 75% in 2022.
Responders as a percentage of referrals by year.

Discussion
BPIs offer services a way to meet the rising demand for therapeutic support by enabling a wider range of healthcare professionals, including paraprofessionals, to deliver structured, evidence-based interventions. Expanding access in this way is particularly important for over-stretched services, given the persistent global shortage of mental health professionals and the growing pressure on mental health systems to provide timely, effective care. Evidence supporting the effectiveness of BPIs in secondary care mental health settings in the UK is emerging, although it remains limited.
An initial evaluation of the DT BPI within this service (Wright et al., Reference Wright, Travers-Hill, Gracey, Troup, Parkin, Casey and Kim2020) reported significant improvements in distress tolerance, mood, anxiety, wellbeing, and functioning among 43 clients, with medium to large effect sizes. Since then, the intervention has been implemented at scale, providing an opportunity to examine engagement, outcomes, and predictors of response in a much larger cohort. The present study extends this earlier evaluation by analysing six years of routinely collected data (2017 to 2023) to assess the completeness of demographic and outcome data, estimate the proportion of clients showing reliable improvement in distress tolerance; and explore demographic and clinical factors associated with response.
Referrals for the BPI within the service have declined substantially since 2017, with a marked reduction in 2020–2021 coinciding with the COVID-19 pandemic, during which services were limited and largely delivered remotely. This shift may partly explain the reduction in both referrals and response rates observed in this period, as clients and clinicians adjusted to virtual delivery formats. The subsequent opening of two new local services in 2022 to 2023, offering psychological support for interpersonal difficulties without a personality disorder diagnosis, likely also diverted potential referrals.
Approximately half of clients referred for a BPI in distress tolerance in this service did not complete the intervention (attrition = 47.7%), although this figure includes both those who declined or for whom the intervention became unsuitable, and those who disengaged after starting. Among clients who attended at least one session, attrition was notably lower (35.6%). These rates are broadly comparable to, although slightly higher than, those reported in the earlier evaluation (Wright et al., Reference Wright, Travers-Hill, Gracey, Troup, Parkin, Casey and Kim2020), which found 39.4% of referrals did not complete. The modest increase in attrition may be explained by the COVID-19 pandemic, which resulted in BPIs being offered online more frequently and likely placed additional demands on clients, including illness, caring responsibilities, and other pandemic-related stressors.
Compared with prior literature, drop-out rates in this sample remain higher than those typically reported for general psychotherapy, where meta-analyses have estimated rates between 19.7% (Swift and Greenberg, Reference Swift and Greenberg2012) and 46.7% (Wierzbicki and Pekarik, Reference Wierzbicki and Pekarik1993). However, these figures vary substantially depending on how drop-out is defined, whether non-attendance before treatment begins is included, and the clinical complexity of the population studied. The current results are consistent with rates observed in community mental health settings, where engagement is often influenced by symptom severity, social adversity, and service pressures. Improving the consistency and detail of attrition recording, for example, distinguishing between pre- and post-treatment drop-out, would enable more meaningful comparisons across services and inform strategies to improve engagement. Routine collection of follow-up data from non-completers would also help estimate rates of spontaneous recovery and clarify the added value of the BPI.
In terms of data completion, demographic data were recorded well (88–100% completion), but outcome data were less consistent, with 20 to 40% missing across measures. Measures routinely used within the service (SWEMWBS, PHQ-9, GAD-7) had higher completion rates than BPI-specific tools (WSAS, DTS, DERS), suggesting a need for clearer processes to ensure that intervention-specific measures are collected. This might be addressed through simpler electronic data capture or clinician prompts within digital care systems.
The percentage of referrals classified as responders has improved from 17.9% in 2018 to approximately 42.9% in 2023, suggesting either improvement in delivery or in referral suitability. The notable dip in response rates during 2020–2021 likely reflects the challenges of remote delivery, increased general distress during the pandemic, and disruptions in staff training and supervision. The apparently remarkable increase in the percentage of responders in 2022 is also notable. Perhaps the social contact after a long period of time on the waitlist and isolation during the pandemic may account for a better response. Random error also cannot be discounted given the low numbers of referrals in 2022 and 2023.
Among clients for whom reliable change could be calculated (n=163), 58.3% were classified as responders on either the DTS or DERS, comparable to the 60.2% reliable improvement rate for CBT across all diagnoses in IAPT services (NHS England Digital, 2022). This is encouraging, given the brevity of the BPI (mean = 7.3 sessions) which is likely to be half that of a course of CBT.
Discrepancies between DTS and DERS outcomes (reliable improvement 38.0% vs 55.3%) likely reflect differences in the constructs assessed and the psychometric properties of each measure. The DERS demonstrated stronger internal consistency (α=0.93) and captures a broader range of emotion regulation difficulties, including awareness and clarity (core targets of the intervention), making it more sensitive to change in this context. In contrast, the DTS focuses narrowly on distress tolerance, a dimension that may shift less readily over the course of brief skills-based therapy. These differences suggest that observed improvements may reflect gains in general emotion regulation capacities rather than distress tolerance alone. From a service delivery perspective, the added burden of administering both scales should be weighed against their utility, with consideration given to selecting a single validated measure that best aligns with the intervention’s primary focus.
No significant differences in treatment response were observed across age, presenting problem, or baseline anxiety and depression, suggesting the intervention may have broad transdiagnostic utility. However, male clients were under-represented among responders, consistent with documented gender disparities in psychological treatment engagement, with men less likely to seek, engage with, or remain in therapy (Addis and Mahalik, Reference Addis and Mahalik2003; McManus et al., Reference McManus, Bebbington, Jenkins and Brugha2016). Distress tolerance interventions and measurement may also be vulnerable to gender bias: while the DTS and DERS were validated in mixed samples, the original studies did not explicitly test measurement invariance by gender, and evidence suggests men are less likely to report or describe emotional experiences (Nolen-Hoeksema, Reference Nolen-Hoeksema and Aldao2011). Moreover, much of the distress tolerance research underpinning the BPI, DTS, and DERS is based on Linehan’s (Reference Linehan1993) work with predominantly female participants diagnosed with borderline personality disorder. In our study, clients with higher baseline distress showed greater improvement, a finding consistent with other brief skills-based interventions (Scholten et al., Reference Scholten, Seldenrijk, Hoogendoorn, Bosman, Muntingh, Karyotaki, Andersson, Berger, Carlbring, Furmark, Bouchard, Goldin, Kampmann, Morina, Kocovski, Leibing, Leichsenring, Stolz, van Balkom and Batelaan2023; Uckelstam et al., Reference Uckelstam, Philips, Holmqvist and Falkenström2019). Higher initial distress may reflect both greater potential for change and heightened motivation to engage actively with therapeutic tasks, thereby facilitating more substantial progress. This pattern may also help explain why male clients were less well represented among responders: if men tend to report lower levels of distress at baseline, they may consequently have less scope for measurable improvement.
Unmeasured variables may also have influenced engagement or response. Factors such as risk status, chronicity of difficulties, and co-occurring conditions including neurodivergence, parallel changes in medication, additional sociodemographic factors and non-random missing data could have shaped outcomes in ways not captured by routine measures. Future evaluations should examine whether these factors influence outcomes, to guide targeted engagement strategies.
Encouragingly, response rates did not differ by referrer role and crucially HCP role. These findings align with extensive evidence that structured psychological interventions delivered by paraprofessionals, when appropriately trained and supervised, produce outcomes in common mental health difficulties comparable to those achieved by qualified mental health professionals (Richards et al., Reference Richards, Ekers, McMillan, Taylor, Byford, Warren, Barrett, Farrand, Gilbody, Kuyken, O’Mahen, Watkins, Wright, Hollon, Reed, Rhodes, Fletcher and Finning2016; Roberts et al., Reference Roberts, Travers-Hill, Coker, Troup, Casey, Parkin and Kim2021; Singla et al., Reference Singla, Kohrt, Murray, Anand, Chorpita and Patel2017; van Ginneken et al., Reference van Ginneken, Tharyan, Lewin, Rao, Meera, Pian, Chandrashekar and Patel2013).
Limitations
Interpretation of these findings is limited by the uncontrolled design – causality cannot be inferred without a comparison group. Nonetheless, the pattern of results aligns with prior research demonstrating the transdiagnostic effectiveness of distress tolerance interventions across clinical populations (Boostani et al., Reference Boostani, Ezadikhah and Sadeghi2017; Bornovalova et al., Reference Bornovalova, Gratz, Daughters, Hunt and Lejuez2012; El-Ashry et al., Reference El-Ashry, Hussein Ramadan Atta, Alsenany, Farghaly Abdelaliem and Abdelwahab Khedr2023; Langdon et al., Reference Langdon, Scherzer, Ramsey, Carey, Rich and Ranney2021; Macatee et al., Reference Macatee, Albanese, Okey, Afshar, Carr, Rosenthal, Schmidt and Cougle2021; Neacsiu et al., Reference Neacsiu, Rizvi and Linehan2010; Stein et al., Reference Stein, Herman, Moitra, Hecht, Lopez, Anderson and Brown2015; Yardley et al., Reference Yardley, McCall, Savage and Newton2019). The gender imbalance (72% female) limits generalisability, and missing outcome data may bias responder rates. Future analyses incorporating additional outcomes (e.g. mood, wellbeing, or functioning) and exploring factors associated with early drop-out would enhance understanding of treatment utility and accessibility.
The use of routinely collected clinical data provides valuable insight into real-world service delivery, but the limitations of this approach should be considered when interpreting the findings. Routine datasets can be incomplete or inconsistent which may influence estimates of improvement, particularly for measures that are less embedded in standard practice, such as the DTS and DERS. Researchers have little control over the measures used, their timing and accuracy. This limits the precision with which outcomes can be compared with those reported in randomised controlled trials. The finding that clients with higher pre-treatment distress may have a better response to the intervention should be interpreted cautiously, as routine data do not allow for causal analysis. The under-representation of certain groups (in this study, male clients) represents a potential bias, as the data may not fully capture the experience or outcomes in this population.
In conclusion, this evaluation extends previous findings from Wright et al. (Reference Wright, Travers-Hill, Gracey, Troup, Parkin, Casey and Kim2020) by providing a larger, six-year dataset showing consistent and clinically meaningful improvements in distress tolerance following a brief, transdiagnostic intervention delivered by both qualified mental health professionals and paraprofessionals. Despite challenges in data completeness and pandemic-related disruptions, the BPI continues to demonstrate promising effectiveness and scalability within routine community mental health settings. Ongoing refinement of data collection processes and exploration of demographic and delivery-related moderators will be key to optimising engagement and outcomes.
Key practice points
-
(1) Reliable improvement (58.3% of clients) for a brief distress tolerance intervention in a secondary care mental health team delivered by clinicians and paraprofessionals was comparable to reliable improvement for CBT (60.2%) with approximately half the number of sessions typically offered in a course of CBT.
-
(2) Clients with higher pre-treatment distress may have a better response to the DT BPI.
-
(3) Additional focus may be required to improve access for male clients.
Data availability statement
The data that support the findings of this study are available from Dr Dave Haggarty (dave.haggarty@cpft.nhs.uk) upon reasonable request.
Acknowledgements
We thank Anna Hudson and Sophie Rabbetts for help with data preparation. We also thank all members of the secondary adult community mental health service who supported and delivered the intervention. Sincere thanks are extended to all clients who took the time to complete outcome measures.
Author contributions
Tara McFarquhar: Conceptualization (equal), Data curation (supporting), Formal analysis (lead), Methodology (lead), Project administration (equal), Software (lead), Validation (lead), Writing - original draft (lead), Writing - review & editing (lead); Dave Haggarty: Conceptualization (equal), Data curation (equal), Formal analysis (supporting), Methodology (supporting), Project administration (equal), Resources (lead), Supervision (lead), Writing - review & editing (supporting); Peter Beazley: Conceptualization (supporting), Formal analysis (supporting), Methodology (supporting), Supervision (supporting), Writing - review & editing (supporting).
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors declare none.
Ethical standards
Authors have abided by the Ethical Principles of Psychologists and Code of Conduct as set out by the BABCP and BPS. The Clinical Effectiveness Team confirmed that NHS ethical approval was not required as the evaluation involved routinely collected clinical data and gave authorisation for a service evaluation work programme. The University of East Anglia granted ethical approval for the project ETH2324-0179.





 Open access
Open access
Comments
No Comments have been published for this article.