


Introduction
Radiotherapy (RT) uses high-energy radiation to destroy cancer cells. Reference Lievens, Borras and Grau1 Around 40% of cancer patients in the United Kingdom (UK) receive RT at least once during their treatment, 2 with 103,348 RT episodes delivered in England in 2020. Reference Powell, Kulakiewicz and Baker3 RT aims to deliver high doses of radiation to cancer cells while maintaining low doses to healthy tissues, thereby reducing side effects. Reference Lievens, Borras and Grau1 Modern RT technologies provide greater conformity, reducing the dose to healthy tissues and therefore the risk of side effects. Reference Barazzuol, Coppes and van Luijk4
Therapeutic radiographers (TR) are healthcare professionals who possess skills and proficiency in the technical and clinical aspects of radiation planning and delivery. Reference Joyce, Jackson, Skok, Peet and McNair5 Recognised by the Health and Care Professions Council (HCPC) as an allied health profession within the UK, Reference Joyce, Jackson, Skok, Peet and McNair5,Reference Ketterer, Callender, Warren, Al-Samarraie, Ball and Calder6 TRs carefully monitor and manage patients’ side effects throughout the treatment and coordinate multidisciplinary and auxiliary care. Reference Joyce, Jackson, Skok, Peet and McNair5 TRs play a pivotal role in meeting cancer patients’ needs and delivering patient-centred care. Reference Joyce, Jackson, Skok, Peet and McNair5
The HCPC provides educational standards for registering as a TR, requiring a bachelor’s or master’s degree with honours, accredited by the HCPC and the College of Radiographers. 7,8 The three-year undergraduate programme equips students with theoretical knowledge and clinical skills needed to meet the HCPC Standards of Proficiency (SoPs). 7,9 These standards ensure TRs maintain current professional practice standards and work safely and effectively. 9 Clinical placements comprise 50% of the curriculum, a mandatory requirement for pre-registration RT programmes. Reference Ketterer, Callender, Warren, Al-Samarraie, Ball and Calder6,Reference Newton, Lee and Brito10 This enables students to experience professional behaviour and develop clinical skills in a healthcare setting. Reference Ketterer, Callender, Warren, Al-Samarraie, Ball and Calder6 RT students in the UK must be fluent in English and have adaptive communication skills to meet the unique needs of cancer patients. 7,Reference Kelly, Thompson, Surjan, Rinks and Warren-Forward11 As a professional body, the Society of Radiographers (SOR) provides guidance for both pre-registration and post-registration TRs, thereby supporting students in preparing for their careers. 12
Internationalisation significantly impacts healthcare education by promoting the movement of students and global competence. Reference Korhonen, Tuomikoski, Oikarainen, Kääriäinen, Elo and Kyngäs13 It is closely related to culturally and linguistically diverse (CALD) students, Reference Korhonen, Tuomikoski, Oikarainen, Kääriäinen, Elo and Kyngäs13 with ‘cultural diversity’ referring to the variation in societal characteristics and ‘linguistic diversity’ referring to differences in the language spoken by the majority. Reference Korhonen, Tuomikoski, Oikarainen, Kääriäinen, Elo and Kyngäs13 The UK was the third largest host country for CALD students in 2019. 14 According to the Higher Education Student Agency, approximately 679,970 CALD students were studying at UK universities in 2021-22, making up 22% of the total student population. 15,16
CALD students may encounter unique challenges on clinical placements, including language barriers, unfamiliar accents, colloquialisms and verbal expressions. Reference Newton, Lee and Brito10,Reference Battaglia, Flynn and Brown17 According to Lalor et al. Reference Lalor, Yu, Brown and Thyer18 these factors can impede their adaptation to professional environments and effective patient communication, placing them at a disadvantage compared to non-CALD students. Reference Newton, Lee and Brito10,Reference Lalor, Yu, Brown and Thyer18 Studies indicated that such challenges may result in stress, loss of self-confidence and anxiety, ultimately impacting their well-being and learning outcomes. Reference Mikkonen, Elo, Kuivila, Tuomikoski and Kääriäinen19–Reference Anthony21
These challenges can also impact clinical tutors, who may require additional time to support CALD students in developing their communication skills and orientating them to local customs and systems. Reference Newton, Lee and Brito10,Reference Pack22,Reference Ross, Ta and Grieve23 Ross et al. Reference Ross, Ta and Grieve23 suggested that these challenges arise from inadequate guidelines regarding supervising CALD students and insufficient supervisor training. However, supportive clinical staff attitudes can enhance CALD students’ placement experience. Reference Mikkonen, Elo, Kuivila, Tuomikoski and Kääriäinen19,Reference McPake24
University international student support services can improve CALD students’ clinical placement experiences through the promotion of physical, mental and social well-being and cultural adaptation. Reference Mikkonen, Elo, Kuivila, Tuomikoski and Kääriäinen19,Reference Wawera and McCamley25 However, some students may refrain from engaging with such services due to social anxiety. Reference Wawera and McCamley25 The International Advice and Guidance team supports CALD students in adapting to British culture, socialising and improving their English language skills. 26 The Quality Assurance Agency for Higher Education developed support guidance for those who interact with CALD students to enhance their experience in higher education. 27
Although various literature reviews have discussed challenges faced by CALD students on clinical placement, few studies have surveyed or interviewed CALD students directly. Reference Mikkonen, Elo, Kuivila, Tuomikoski and Kääriäinen19,Reference Law, Masterson-Ng and Pollard28–Reference Johnson, Gitay, Abdel-Salam, BenSaid, Ismail and Al-Tameemi32 While support strategies in RT and other healthcare placements have been explored, Reference Pienaar, Orton and Botma33–Reference Armstrong-James, Khine, Thorne, Tuckey and Bennett35 none focus on RT clinical placements from CALD students’ perspectives in the UK. Gaining insight into clinical placement experiences is crucial to fostering diversity and cultural competence within healthcare. Reference Ropponen, Kamau, Koskenranta, Kuivila, Oikarainen and Isakov36
Research question
A quantitative descriptive study was conducted using a survey design to collect data from CALD students to evaluate their experiences of clinical placements on pre-registration RT programmes across the UK.
Aim and objectives
The aim of this study was to gain a comprehensive understanding of the clinical placement experience, challenges and perspectives of CALD students enrolled in pre-registration RT programmes at UK universities. Four objectives are illustrated in Figure 1.
Research objectives.

Methods
Ethical considerations
Ethical approval for this study was obtained from the University Research Ethics Committee (approval number 13143). Participant information sheets and consent forms were provided on the first page of the electronic survey. All responses were fully anonymised through the Microsoft (MS) Forms software and participation was voluntary. As reflecting on experiences may raise emotional concerns, participants were advised to speak to placement coordinators, clinical tutors, lecturers or university support staff. Debriefing materials were included at the end of the survey.
Study population
All CALD students enrolled in pre-registration undergraduate RT degree programmes at UK universities who had attended at least one clinical placement were invited to participate. The number of CALD students at each university was unknown; therefore, the response rate was not calculated.
Data collection
An electronic survey was developed using MS Forms, including Likert-scale questions based upon evidence from an initial literature review (survey questions are available within the Supplementary Material). Open-ended questions were excluded, as this risked discussion of sensitive topics without the ability to offer support due to anonymity. An invitation email including the consent form, participant information sheet and a survey link was sent to the Society of Radiographers Heads of Radiography Education (HRE) Group for dissemination to Professional Leads at all UK universities offering BSc Therapeutic Radiography programmes. Professional Leads were asked to disseminate the survey to all BSc Therapeutic Radiography student cohorts. It was clearly specified within the invitation email and the participant information sheet that only international students should complete the survey. The survey remained open for four weeks. At the end of the survey, a separate link allowed participants to enter into a prize draw to win a £50 Amazon voucher, which was specified in the participant information.
Data analysis
Descriptive statistics were used to analyse questionnaire responses, including the calculation of means and frequencies. Inferential statistical tests were not conducted, as the small sample size would not have provided sufficient statistical power. Reference Mishra, Pandey, Singh, Keshri and Sabaretnam37
Results
17 CALD students completed the survey. Three students were first-year (18%), and 14 were third-year (82%). All participants were female. Six participants were aged 18–21, and 11 were aged 22–25 years.
Challenges experienced during clinical placements
Participants reported a range of challenges (Figure 2). Language barriers were a highly prevalent issue; 12% (n = 2) of all participants strongly agreed, whilst 71% (n = 12) agreed with this statement. Isolation also emerged as a common challenge, with 35% (n = 6) of all participants indicating that they strongly agreed with this; interestingly, 66% (n = 2) of the first-year students alone (n = 3 in total) disagreed that feelings of isolation and cultural differences were challenging.
Challenges CALD students reported facing during their clinical placement.

Discrimination during clinical placement
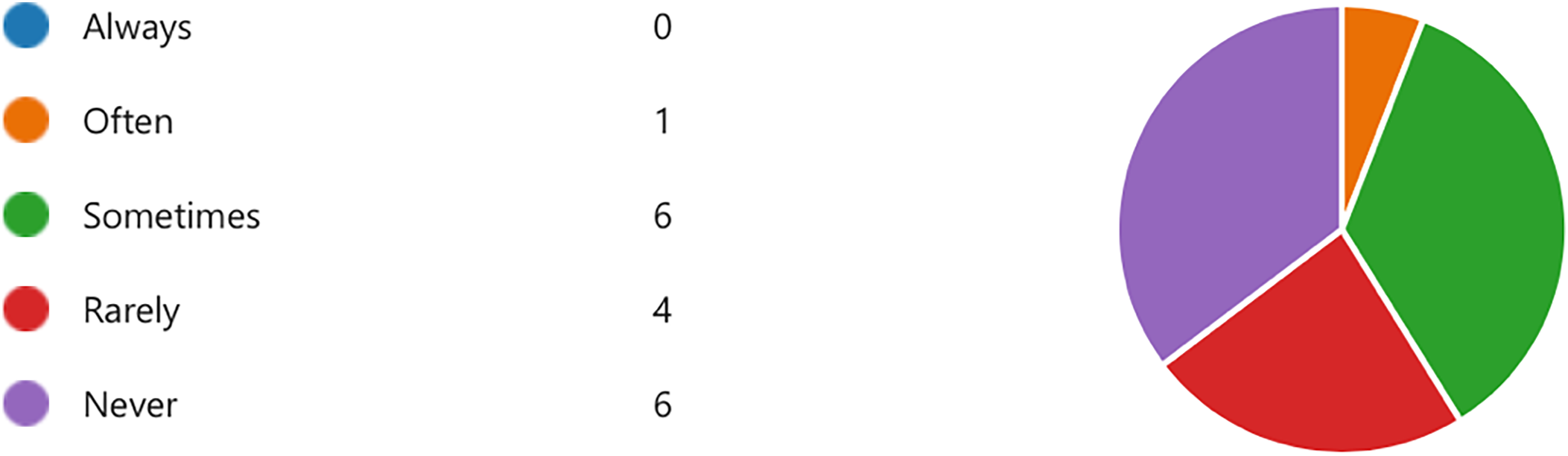
Responses regarding discrimination during clinical placement varied (Figure 3). None of the students indicated that they ‘always’ experienced discrimination, while one student (n = 1) reported experiencing this ‘often’. Six students (n = 6) stated that they experienced discrimination ‘sometimes’, and four students (n = 4) reported it ‘rarely’. An equal number of students (n = 6) indicated that they had ‘never’ experienced discrimination.
Frequency with which CALD students reported experiencing discrimination during clinical placement.

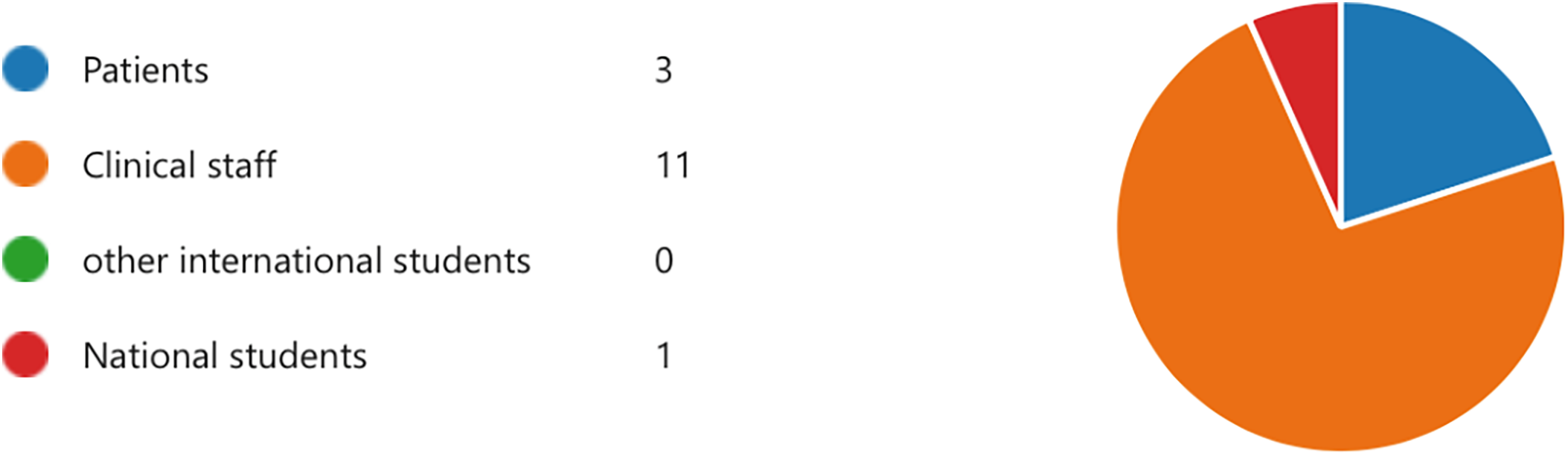
Fifteen participants reported the groups of individuals with whom they had interacted when they experienced discrimination (Figure 4). Of these, 11 participants (73%) reported experiencing discrimination when interacting with clinical staff, compared with 3 participants (20%) reporting experiencing discrimination when interacting with patients. One participant (7%) reported discrimination during interactions with national students.
Groups of individuals with whom CALD students interacted when they reported experiencing discrimination during clinical placement.

Support offered to CALD students
Within this sample, participants stated that they were mostly supported on placement by other international students, clinical tutors/mentors and University link tutors (Figure 5). Two students (12%) indicated that no support was offered.
The group of people/support services that CALD students were supported by when experiencing issues during clinical placements.

Clinical placement experience
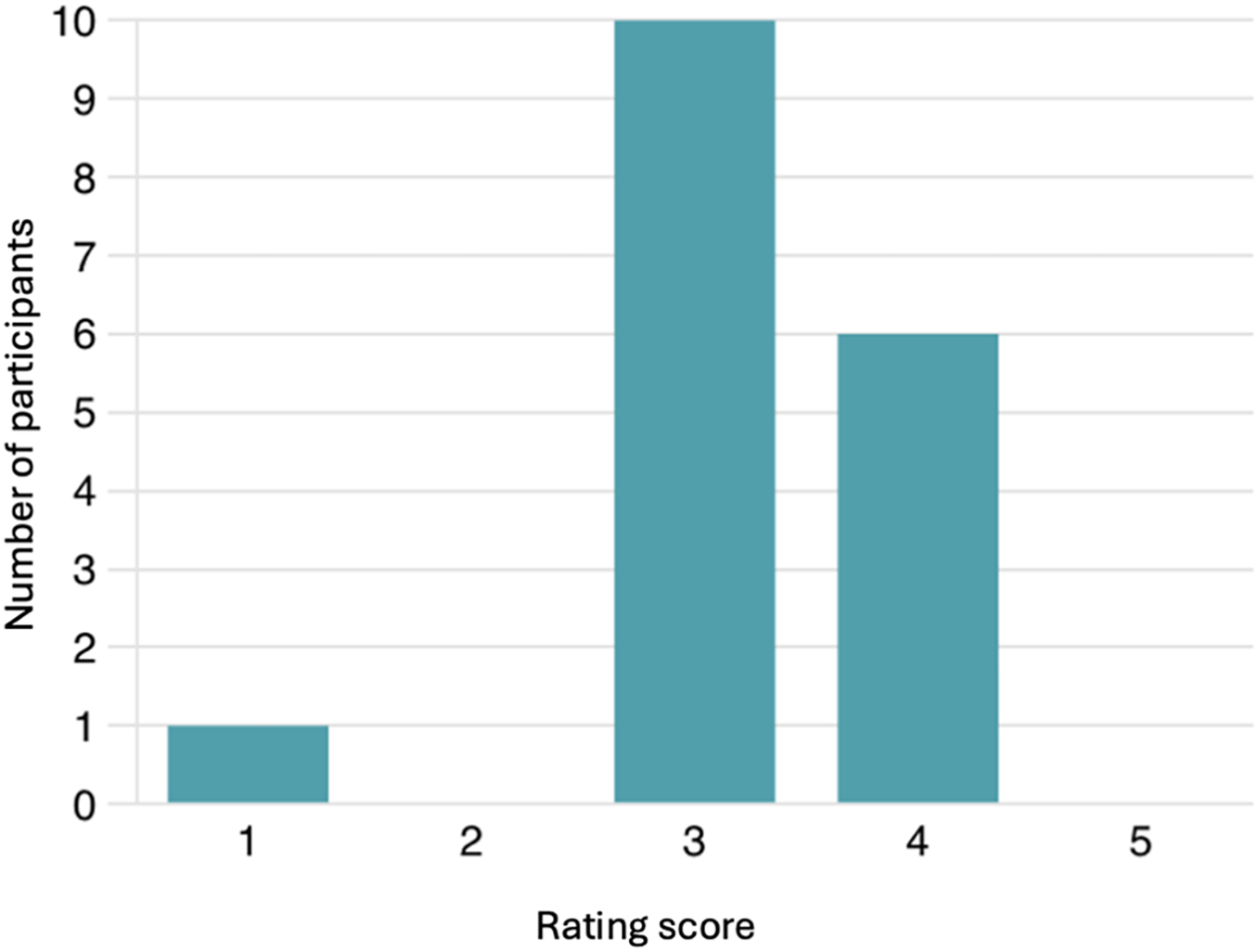
Overall, the mean rating of the participants’ experience of clinical placements was 3.24/5 (Figure 6).
CALD students’ rating of their overall clinical placement experience (1= lowest rating, 5 = highest rating).

Discussion
This study sought to evaluate CALD students’ experiences of RT placements in the UK and the support offered to them. The findings revealed four key challenges: language barriers, cultural differences, familiarity with the UK healthcare system and feelings of isolation. However, the generalisability of these findings is limited by the small, all-female sample (n = 17), which should be considered when interpreting the results. Given the participant demographics, it could be considered that these findings reflect the intersectionality of being both a CALD student and a female within a highly technical healthcare environment, which may result in different experiences compared to male CALD students. However, as RT is a female-dominated profession, it is unlikely that this would result in significant additional challenges; further research is required to explore any gender-based differences.
Language barriers
Language barriers were the most frequently reported challenge amongst CALD students on RT clinical placements (Figure 2). These findings are consistent with those cited in previous studies involving occupational therapy and medical CALD students, who encountered challenges with verbal communication linked to local slang, accents and varying interpretations of words. Reference Law, Masterson-Ng and Pollard28,Reference Morgan38 However, our data suggest this challenge persisted even in final-year students, indicating that difficulties may not diminish over time. Second language anxiety among CALD students can lead to stress, reduced self-confidence and feelings of inadequacy. Reference Khawaja, Chan and Stein20
Effective communication is one of the HCPC SoPs, 9 requiring TRs to communicate verbally and non-verbally with service users, carers and colleagues. In clinical practice, RT students should use professional language to explain medical information and colloquial language to build rapport. Reference Kelly, Thompson, Surjan, Rinks and Warren-Forward11 Effective communication supports the delivery of high-quality care by addressing patients’ needs and concerns. Reference Kelly, Thompson, Surjan, Rinks and Warren-Forward11 Mattarozzi et al. Reference Mattarozzi, Fino, Panni, Agostini, Morganti and Russo39 reported that greater patient satisfaction with communication correlated with a lower intensity of pain experienced during RT. However, CALD students often face difficulty with clinical communication skills such as introducing themselves, engaging in small talk with patients, and interpreting non-verbal cues. Reference Brewer, Jackson and Bartle40 A scoping review by Brewer et al. Reference Brewer, Jackson and Bartle40 found that pre-placement interventions, including videos, role-play, simulated patients and feedback, enhanced CALD students’ confidence and prepared them well for clinical placement. The HCPC requires TRs whose first language is not English to provide certified evidence of the International English Language Testing System (IELTS) tests with a minimum score of 7.0. 41 These tests aim to forecast students’ ability to study in an English-speaking educational environment and minimise language barriers. Reference Ross, Ta and Grieve23 However, these assessments may not accurately reflect language proficiency, requiring further support throughout the programme. Reference Ross, Ta and Grieve23
Cultural differences
Around half of the participants ‘strongly agreed’ or ‘agreed’ that cultural differences posed challenges (Figure 2). This supports findings reported by Goodwin and Mbah, Reference Goodwin and Mbah42 whereby CALD students’ self-confidence levels and placement experiences were negatively affected by their unfamiliarity with UK workplace values and practices. Reference Goodwin and Mbah42 This aligns with findings reported by Högstedt et al., Reference Högstedt, Engström, Eriksson and Jansson43 whereby CALD nursing students in Sweden faced challenges adapting to a new culture and clinical environment.
The RT workplace culture impacts TRs and service users, directly affecting the quality of care. Reference Lohikoski, Roos and Suominen44 As data on participants’ backgrounds were not collected, any relationships between cultural differences could not be explicitly identified. CALD students may face cultural shock when adjusting to new clinical placements, depending on the differences from their home culture. Reference Law, Masterson-Ng and Pollard28 Law et al. Reference Law, Masterson-Ng and Pollard28 found that occupational therapy CALD students from Confucian-based backgrounds exhibited greater cultural shock during clinical placements in the UK, struggling to set objectives and adapt to the shift from didactic educational environments to self-directed learning approaches. To overcome cultural differences, CALD students are encouraged to engage with national, academic and clinical cultures. Reference Law, Masterson-Ng and Pollard28
Following the Equality Act, 9 individuals with protected characteristics and cultural differences must be treated equally and with dignity. In this study, participants’ protected characteristics included their different nationalities, races, beliefs and religions. During placements, qualified TRs should respect students’ cultural differences, including values, beliefs and personal biases. 9 Despite this, a qualitative study by Korhonen et al. Reference Korhonen, Tuomikoski, Oikarainen, Kääriäinen, Elo and Kyngäs13 found that many CALD students experienced mistreatment by staff or mentors, often attributed to a lack of cultural competence. Cultural competence enables safe, comprehensive care that addresses cultural differences and supports non-discriminatory practice, as highlighted by the HCPC SoPs. 9,Reference Reeve and Lavery45 Although the HCPC standards include equality, diversity and inclusion principles to promote cultural competence among staff, 46 CALD students are not particularly specified. Ross et al. Reference Ross, Ta and Grieve23 also noted a lack of guidelines regarding how to support, assess and interact with CALD students. Mikkonen et al. Reference Mikkonen, Elo, Tuomikoski and Kääriäinen31 emphasised the role of positive intracultural mentoring in creating a welcoming environment for CALD students and mediating cultural differences to reduce social isolation. Reference Mikkonen, Elo, Tuomikoski and Kääriäinen31
Familiarity with the UK healthcare system
Responses regarding familiarity with the NHS varied (Figure 2), which may reflect different levels of preparation across institutions. Unfamiliarity with the healthcare system is a common challenge for CALD students in healthcare professions. Reference Law, Masterson-Ng and Pollard28 Law et al. Reference Law, Masterson-Ng and Pollard28 reported that occupational therapy CALD students (n = 6) lacked prior NHS experience and encountered a healthcare context that differed from their home countries. Many participants had to learn the systems and the policies themselves, indicating the need for greater orientation to the host country’s healthcare context. Reference Law, Masterson-Ng and Pollard28 Baker et al. Reference Baker, Rylance-Graham and Keane47 surveyed CALD healthcare students and emphasised the need to understand the NHS healthcare system prior to attending clinical placements. Despite these findings, the UK Council for International Student Affairs provides guidance to support CALD students in familiarising themselves with the UK healthcare system; 48 however, this may not be regularly utilised.
Simulated RT environments can improve students’ confidence and familiarity with the healthcare system prior to attending clinical placement. Reference Bridge, Giles, Williams, Boejen, Appleyard and Kirby49 Several studies have demonstrated improvements in students’ levels of confidence and communication skills within simulated RT cohorts compared to traditional teaching methods. Reference Ketterer, Callender, Warren, Al-Samarraie, Ball and Calder6,Reference Kelly, Surjan, Rinks and Warren-Forward50 However, Cahu et al. Reference Chau, Arruzza and Johnson51 emphasised that simulation should complement, not replace, clinical placement.
Feelings of isolation
Half of the participants reported isolation during placement (Figure 2), which can negatively impact CALD students’ well-being; Reference Korhonen, Tuomikoski, Oikarainen, Kääriäinen, Elo and Kyngäs13 however, the small, gender-homogenous sample may underrepresent other perspectives. Interestingly, first-year undergraduate students within this study reported lower levels of isolation compared to third-year students, which contrasts with previous research that demonstrated that first-year RT students struggled to manage professional socialisation in unfamiliar environments, leading to feelings of isolation. Reference Kelly, Thompson, Surjan, Rinks and Warren-Forward11 CALD students have attributed social isolation to language barriers and discomfort in speaking to staff or patients. Reference Korhonen, Tuomikoski, Oikarainen, Kääriäinen, Elo and Kyngäs13,Reference Mitchell, Del Fabbro and Shaw52 Although social activities can significantly reduce isolation, CALD students may still experience loneliness due to language and cultural barriers; Reference Mitchell, Del Fabbro and Shaw52 however, Cheng et al. Reference Cheng, Taylor, Fitzgerald, Kuo and Graves53 reported no significant difference in baseline isolation scores between national and CALD medical students, despite national students sharing language and culture. Alshaharani et al. Reference Alshahrani, Cusack and Rasmussen54 identified three coping strategies utilised by nursing students to reduce isolation within their first clinical placements: debriefing sessions, observing staff-patient interactions and sharing the experience with friends and family. Wijbenga et al. Reference Wijbenga, Duvivier, Driessen, Ramaekers and Teunissen55 emphasised that effective communication with clinical staff is essential in preventing isolation.
Discrimination in clinical placement
This study showed varied responses to discrimination during clinical placement (Figure 3), with most participants attributing this to interactions with clinical staff (Figure 4). Discrimination and bullying were also reported by CALD students in an earlier study by Korhonen et al., Reference Korhonen, Tuomikoski, Oikarainen, Kääriäinen, Elo and Kyngäs13 however, the source was not specified. Juntunen et al. Reference Juntunen, Kamau, Oikarainen, Koskenranta, Kuivila and Ropponen56 highlighted the negative impact of discrimination on CALD nursing students’ learning experiences and career prospects, stressing the importance of a student-centred approach to foster a safe learning environment. They addressed six categories for supporting CALD students: competence-building, ethics and equality, cultural diversity, student-centred orientation, encouragement and supportive environments. Reference Juntunen, Kamau, Oikarainen, Koskenranta, Kuivila and Ropponen56 The variation in reported experiences may reflect broader structural factors, including unconscious bias, workplace pressures or insufficient staff training. Previous studies on students’ experiences of bullying during clinical placements have explored the concept of organisational culture within the healthcare environment, with the hierarchical structure present in many professions considered to be a contributing factor. Reference Zhou, Wang, Zeng, Zeng, Liu and Tan57 It is postulated that such hierarchical cultures result in a reluctance to challenge staff in senior positions, leading to an acceptance of bullying behaviours within nursing and midwifery placements. Reference Zhou, Wang, Zeng, Zeng, Liu and Tan57,Reference Capper, Muurlink and Williamson58
Recent research suggests that unconscious bias within healthcare settings can negatively impact students’ placement experiences. Reference Joseph, Flint, Raymond-Williams, Awadzi and Johnson59,Reference Dafny, Snaith, McCloud, Waheed, Cooper and Champion60 Within a study involving UK student nurses, participants from ethnic minority backgrounds described experiencing discrimination related to their race, culture or language. Reference Walker, Gunasinghe, Harwood, Ehsan, Ahmed and Dorrington61 CALD students studying medicine in Australia similarly reported that language barriers impacted their relationships with qualified physicians; Reference Colenbrander, Causer and Haire62 however, a similar study exploring nursing students’ experiences reported that UK CALD students experienced increased discrimination during placements compared to native English speakers, yet this was not reported by Australian participants. Reference Birks, Cant, Budden, Russell-Westhead, Ozcetin and Tee63 Discrimination experienced by CALD healthcare students is a complex issue, impacting students within various professions and countries. Further research into the organisational culture contributing to bullying and discrimination is required, with a particular focus on the qualitative experiences of CALD students within RT.
In the UK, the NHS mandates staff training that includes modules on unconscious bias, equality, diversity and inclusion; 64 to practically address the issues reported here, structured mentorship and further staff training on cultural competence and bullying in the workplace are required.
Support offered for CALD students
Around half of the participants were supported by other CALD students (Figure 5), while fewer received support from clinical mentors and supervisors. Previous studies have also concluded that CALD students often shared placement challenges with other CALD friends and family, yet rarely informed their clinical supervisors and internationalisation officers. Reference Wijbenga, Duvivier, Driessen, Ramaekers and Teunissen55
Clinical mentors play a significant role in shaping positive clinical placement experiences for CALD students. Reference Korhonen, Tuomikoski, Oikarainen, Kääriäinen, Elo and Kyngäs13 Pearson et al. Reference Pearson, Hill, Attrill and Copley65 showed greater satisfaction among CALD students when they had an effective relationship with clinical mentors. Key factors for constructive supervision included mentors’ ability to provide feedback, motivation and cultural competence. Reference Pearson, Hill, Attrill and Copley65 Luukkonen et al. Reference Luukkonen, Kuivila, Kaarlela, Koskenranta, Kaučič and Riklikiene66 reported that mentors’ cultural competence levels varied from intermediate to high, and were positively associated with greater years of experience.
Few CALD students in this study received support from their university, suggesting the need to develop universities’ international student support services. Reference Zhang67 In contrast, a survey by Baker et al. Reference Baker, Rylance-Graham and Keane47 showed that 78% of CALD healthcare students at one institution believed that university support was adequate for their clinical placements. This may imply that CALD students require additional support in engaging with university services when challenges arise. Wawera and McCamley Reference Wawera and McCamley25 surveyed 61 CALD students in the UK and found that 70% of participants accessed university support services when experiencing loneliness; however, 30% did not engage with support services due to lack of time, social anxiety and fear of talking to strangers. Zile et al. Reference Zile68 argued that university support services are under-resourced and may inadequately address CALD students’ mental wellbeing. However, University International Advice and Guidance teams often provide multiple routes for students to engage with support, including online and face-to-face support for language barriers, cultural differences and feelings of isolation. 26 In addition, University Learning and Teaching Support Officers are equipped to direct CALD students to the most appropriate support to meet their needs, 69 whilst provision of social and cultural events at the University can support the integration of CALD students with the British culture. Reference Chen70
Overall clinical placement experience
CALD students within this study rated their overall placement experience as 3·.24/5 (Figure 6). Placement satisfaction has been proven to affect retention in healthcare. Reference Ropponen, Kamau, Koskenranta, Kuivila, Oikarainen and Isakov36 Ropponen et al. Reference Ropponen, Kamau, Koskenranta, Kuivila, Oikarainen and Isakov36 reported factors influencing CALD nursing students’ retention included support during placement and university studies, perceived equality, nursing competence development and social integration. Such factors impact confidence-building, adaptability and dealing with unexpected events, Reference Thomas, Thomas and McLean71 which could help healthcare CALD students develop resilience, an essential skill for protecting well-being and maintaining self-esteem. Reference Ching and Cheung72,73
Recommendations
Table 1 outlines the key recommendations from this study to enhance CALD students’ experiences during RT clinical placements.
Recommendations to enhance support available for CALD students on RT clinical placements in the UK

Limitations
The primary limitation of this study is the small sample of 17 participants, which represented only a small portion of CALD students enrolled in pre-registration RT programmes at UK universities. All participants were female, which could present a gender bias. Further research with a larger and more diverse cohort is recommended; to support recruitment of a more diverse range of participants that meet the eligibility criteria, future studies should consider disseminating the study invitation within student societies such as the Therapeutic Radiography Society, International Student Society, LGBTQ+ Society and Disabled Students Society. Dissemination of the study invitation by universities’ International Student Experience Teams may also further enhance recruitment of larger sample sizes.
It is also possible that some national students may have completed the survey in order to enter the prize draw for the voucher incentive. If so, this could have introduced response bias and compromised the accuracy of the findings, as the data may not exclusively represent CALD students’ experiences. The tool used in the present study limited the depth of data collected compared to qualitative methods; therefore, conclusions were based on quantitative data alone.
Conclusion
This study explored CALD students’ perceptions of clinical placements on undergraduate RT programmes at UK universities. Common challenges experienced by CALD students on clinical placement included language barriers, cultural differences, isolation and unfamiliarity with the NHS. These findings highlight an urgent need to embed cultural competence within RT clinical education and further develop universities’ international student support services. Addressing CALD students’ challenges not only supports individual learning but also contributes to a more diverse and culturally responsive RT workforce. In the future, larger qualitative studies are required to gain a more comprehensive understanding of the support available to CALD students during RT clinical placements.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1460396926100363.
Acknowledgements
The authors would like to thank all participants who took part in this study, their willingness to share their time and experiences was invaluable to this research.
Financial support
None.
Competing interests
None.







 Open access
Open access