

Impact Statements
Findings from the study show the importance of connecting humanitarian mental health and psychosocial support (MHPSS) and shelter programming in protracted conflicts. This has implications for humanitarian practice.
For shelter programming – beyond light and medium repairs (roof, windows and repairs to the walls), consider means to provide additional resources (cash or in-kind) for internal repairs, to strengthen the well-being impact of shelter programmes and support self-recovery.
For MHPSS programming – when considering interventions in different contexts, MHPSS interventions can utilise basic services and security (layer 1 of the MHPSS intervention pyramid) and strengthened community and family support programming (layer 2) to plan community activities that leverage work within other sectors. This could involve working with communities to undertake internal and cosmetic home repairs (Shelter) in a supportive group environment (MHPSS), as well as collaborating with other sectors and actors (such as Food, Security and Livelihoods) to promote community development and revitalisation. This would serve two related goals. First, it would help build relationships with individual households and communities. Second, it would serve as a gateway to focused MHPSS support for individuals who may otherwise avoid such support due to stigma surrounding mental health support in many contexts.
Links between shelter and MHPSS programming must be context and resource-specific – based on the Medair interventions in the Kharkiv region of Ukraine, this would warrant, at a minimum, integrating the sectors to ensure people in need of shelter programmes also access lay counselling or other MHPSS support. Resource-permitting – this could include MHPSS team members attending shelter repair household visits to assess the needs and/or provide psychosocial support to people in need. All this is dependent on (a) access to and retention of relevant local and international staff and (b) availability and access to funding for the envisaged support and repair activities.
Introduction
The impact of armed conflict on the mental health of the affected populations is well evidenced (see, e.g., Carpiniello, Reference Carpiniello2023), but there is a lack of evidence on the impact of housing infrastructure damage and repair on the mental health of affected populations. However, both the humanitarian assistance programmes (Care International UK and CENDEP, 2022), as well as the WHO (2025) mental health policy and practice guidance highlight the importance of addressing social and structural factors, such as houselessness or unstable housing and/or poverty, to achieve holistic and sustainable outcomes in mental health practice. This reflects the growing conceptual clarity and research evidence on the social determinants of mental health (Braveman and Gottlieb, Reference Braveman and Gottlieb2014; Kirkbride et al., Reference Kirkbride, Anglin, Colman, Dykxhoorn, Jones, Patalay, Pitman, Soneson, Steare, Wright and Griffiths2024), as well as housing as a social determinant of health in general (Bentley et al., Reference Bentley, Mason, Jacobs, Blakely, Howden-Chapman, Li, Adamkiewicz and Reeves2025; Yan et al., Reference Yan, Gallant, Delahunty-Pike, Langley, Zsager, Abaga, Ziegler, Karabanow, Hwang and Pinto2025).
In May 2021, more than 80 international humanitarian practitioners and researchers held a learning event, Doing More and Doing Better. The aim of the event was to ‘uncover and better articulate the impacts of existing Shelter and Settlements best practice on mental health and well-being and to plot a path towards more deliberate and documented beneficial impacts’ (Care International UK and CENDEP, 2022, p. 6). Participants recommended two areas for future research. The first involves exploring definitions of ‘home’ and ‘well-being’ from a mental health perspective, with due consideration of the impact of displacement and possible impermanence on beneficiaries’ definitions of these terms. The second recommendation is for research that focuses on the impact of inadequate housing on mental health in the context of a humanitarian crisis, such as protracted conflicts.
In Ukraine, as of January 2025, the International Organisation for Migration (IOM) estimates that there are 3.6 million internally displaced people (IDPs; IOM, 2025a) and 4.2 million returnees (IOM, 2025b), following the full-scale Russian invasion since February 2022. The Kharkiv region in the East of Ukraine is the second main region of return, with 15% of returnees (after Kyiv City, where 23% of returnees; IOM, 2025b). These are predominantly older people (29% aged 60+ years; IOM, 2025b), who require support for income-earning opportunities, access to building and reconstruction materials, as well as health services (IOM, 2025b). This article presents the findings from a qualitative study that explores the impact of humanitarian shelter support provided by the humanitarian organisation Medair on the well-being of adults who suffered damage to their homes since February 2022. It was conducted in the Balakliia territorial community in the Kharkiv region of eastern Ukraine between February and October 2024.
Definitions of key concepts and approaches
This article focuses on the conceptualisation and practice in relation to mental health and housing/shelter support in humanitarian interventions, rather than mainstream mental health and housing services. Within the humanitarian sector, mental health and psychosocial support (MHPSS) is ‘a composite term for any local or external support aimed at protecting or promoting psychosocial well-being or preventing and treating mental health conditions’ (IASC MHPSS Reference Group, 2007; WHO, 2025, xii). Minimum service package for MHPSS includes the so-called intervention pyramid for MHPSS in emergencies (IASC MHPSS Reference Group, 2007, p. 12), which identifies four core layers of support, namely: basic services and security (layer 1); strengthened community and family support (layer 2); focused psychosocial support through individual, family and group interventions (layer 3); and clinical mental health and psychosocial services for people with severe symptoms, usually led by mental health professionals (layer 4). The fourth layer of support most corresponds to community mental health care as defined in the latest WHO policy guidance (WHO, 2025).
Shelter assistance is defined in The Sphere (2018, p. 211) Humanitarian Charter and Minimum Standards in Humanitarian response as ‘provided to individual households for the repair or construction of dwellings or the settlement of displaced households with existing accommodation or communities’. When such dispersed settlement is not possible, shelter is provided collectively in suitable, large public buildings or structures. Similar to MHPSS, George et al. (Reference George, Guthrie and Orr2023) stress that terminology for shelter is frequently conflated with housing and that there remains little clarity about an overarching definition.
However, Care International UK and CENDEP (2022, p. 27) stress that homemaking (such as decoration, planting flowers and vegetables or making space to host guests) can be important, even in humanitarian emergencies. George et al.’s (Reference George, Guthrie and Orr2023, vi) analysis of the global shelter aid concludes that the sector should be redefined at the policy level as ‘an enabled process to facilitate a living environment with crisis-affected communities and individuals to meet their current and future needs’. Global Shelter Cluster (2024c, p. 7) suggests that the activities in each layer of the aforementioned MHPSS support pyramid require an integrated approach to the protection and well-being of people in need. This requires interdisciplinary approaches to ensure successful integration between shelter and MHPSS programmes (Klenge, Reference Klenge2024).
Prior research on shelter and MHPSS programmes
There is limited prior research on the links between shelter and MHPSS in conflict contexts. A recent exception is a qualitative study on the relationship between housing and health in the Gaza Strip (Sabah and Abuzerr, Reference Sabah and Abuzerr2025). Participants in the study reported that the physical conditions of their homes were a key contributor to poor health outcomes, including mental health. Within the broader field of complex emergency research, Okuzono et al. (Reference Okuzono, Shiba, Zhu, Oh, Hsu, Yazawa, Hikichi, Aida, Kondo, Tiemeier and Kawachi2025) examine the emerging evidence on the links between disaster-related home loss and increased cognitive impairment among the survivors of the 2011 Great East Japan Earthquake and Tsunami. Utilising a prospective cohort study within the survivor population, the authors conclude that home loss was associated with increased depressive symptoms and decreased social connections.
There is also limited, context-specific literature on the links between housing and well-being. In Ukraine, a WHO-led, cross-sectoral MHPSS Technical Working Group provides national coordination and mapping of humanitarian efforts. Drawing on prior work in Ukraine and elsewhere, The Lancet Psychiatry Commission on Mental Health in Ukraine (Pinchuk et al., Reference Pinchuk, Leventhal, Ladyk-Bryzghalova, Lien, Yachnik, Dias, Virchenko, Szatmari, Protsenko, Chaimowitz, Chisholm, Kolokolova, Guerrero, Chumak, Myshakivska, Robertson, Hanson, Liu, De Picker, Kupchik, Pinto da Costa, Scott, Wainberg, Shevaga, Weintraub Brendel, van Voren, Feldman, Mihalopoulos, Kaminska and Skokauskas2024) stresses that the effective MHPSS delivery depends on integration with housing, social protection and humanitarian assistance systems, especially in rural areas. Drawing on this work, a recent narrative synthesis of humanitarian MHPSS coordination mechanisms in Ukraine suggests further strengthening is needed to improve accessibility in remote communities and to enhance integration with other humanitarian sectors (Nalyvaiko et al., Reference Nalyvaiko, Vus, Zotova, Kostruba and Tayeh2025).
Singh et al. (Reference Singh, Bogdanov, Doty, Haroz, Girnyk, Chernobrovkina, Murray, Bass and Bolton2021) also conducted a qualitative study on experiences of mental health and functioning among military veterans and displaced persons in this country. Their findings suggest that the IDPs in the Kharkiv region identified a lack of housing as the main problem affecting their well-being, together with problems in relation to their economic or financial well-being and struggles, and difficulties in interaction with local residents where they live in displacement. Haque (Reference Haque2025, preprint) utilised spatial and suitability modelling to assess multidimensional vulnerabilities in Ukraine during the Russian invasion, including mental health risks, environmental stressors and infrastructure disruptions to develop a multi-source conflict-related health impact database. Findings may suggest that regions with intense conflict, housing damage and resource scarcity, such as the Kharkiv region in Eastern Ukraine, faced the highest vulnerability. The author stresses that war-related health issues, including mental health problems, emerge through the interplay of conflict, environmental stressors and infrastructure damage.
Within the humanitarian aid sector, InterAction (2021, 2023) conducted a review of literature on the wider impacts of humanitarian shelter and assistance. Findings suggest that existing evidence is the strongest in terms of the impact of shelter on health (both physical and mental health) and enhanced well-being, but that the evidence is not robust due to the quality of available data.
Methodology
The Global Shelter Cluster (2024b) research agenda suggests that key research questions should focus on the wider impacts of shelter and settlements in humanitarian crises, including two of relevance for this study. First, what is the role of shelter and settlements in health/livelihoods/protection of households who have lost their shelter and settlements? Second, how do the wider impacts of supporting households who have lost their shelter and settlements indicate how support is best provided? Available literature suggests that research aiming to improve the links between humanitarian shelter and MHPSS needs to focus on people’s lived experience, building evidence from community knowledge (InterAction, 2021) and the socio-cultural, de-pathologising, contextually situated understanding of distress caused by armed conflict (Theisen-Womersely, Reference Theisen-Womersely2021). These questions and focus were selected as relevant for this study.
The aim of the study was to explore how shelter programming contributes to improving people’s psychosocial well-being, based on Medair’s work in eastern Ukraine. To enable focus on people’s lived experience (InterAction, 2021) and the socio-culturally contextually situated understanding of distress (Theisen-Womersely, Reference Theisen-Womersely2021) caused by the ongoing invasion, the study utilised an exploratory qualitative research methodology. The objectives of the study were to explore the perspectives of Medair beneficiaries regarding the impact of the invasion on their psychological distress and overall well-being; to examine the perceived role of Medair house repair programmes (including Cash for Repair and House Repair initiatives) and MHPSS services (provided by both Medair and other actors) on beneficiaries’ well-being; and to identify opportunities to strengthen the links between the MHPSS and shelter programming.
The study was conducted with people who received support from Medair in Balakliia territorial community (Hromada), a rural area of the Kharkiv region (Oblast) in eastern Ukraine, the third most populous region of the country (IOM, 2024). It continues to be one of the most conflict-affected areas of Ukraine due to its location along the frontline and border with the Russian Federation (IOM, 2024). Data gathering was organised through interviews and focus groups. Interviews with the people who received Medair shelter repair services explored their understanding of distress and well-being and the role home/shelter plays in both, as well as the impact of the improvements to their homes on participants’ well-being.
The sampling strategy aimed to identify between 20 and 30 participants, selected according to the criteria designed to ensure diversity and relevance to the study objectives. These included demographic characteristics (such as protected characteristics and socio-economic status); household composition (encompassing families with children, older people and individuals with disabilities and/or chronic illnesses); the type of shelter support received (contractor-led repairs or cash-for-repairs assistance); the level of war exposure in the region (occupied and non-occupied areas, as well as including local residents who chose to remain in their homes during the invasion); and participants’ displacement status (displaced, non-displaced or returnees).
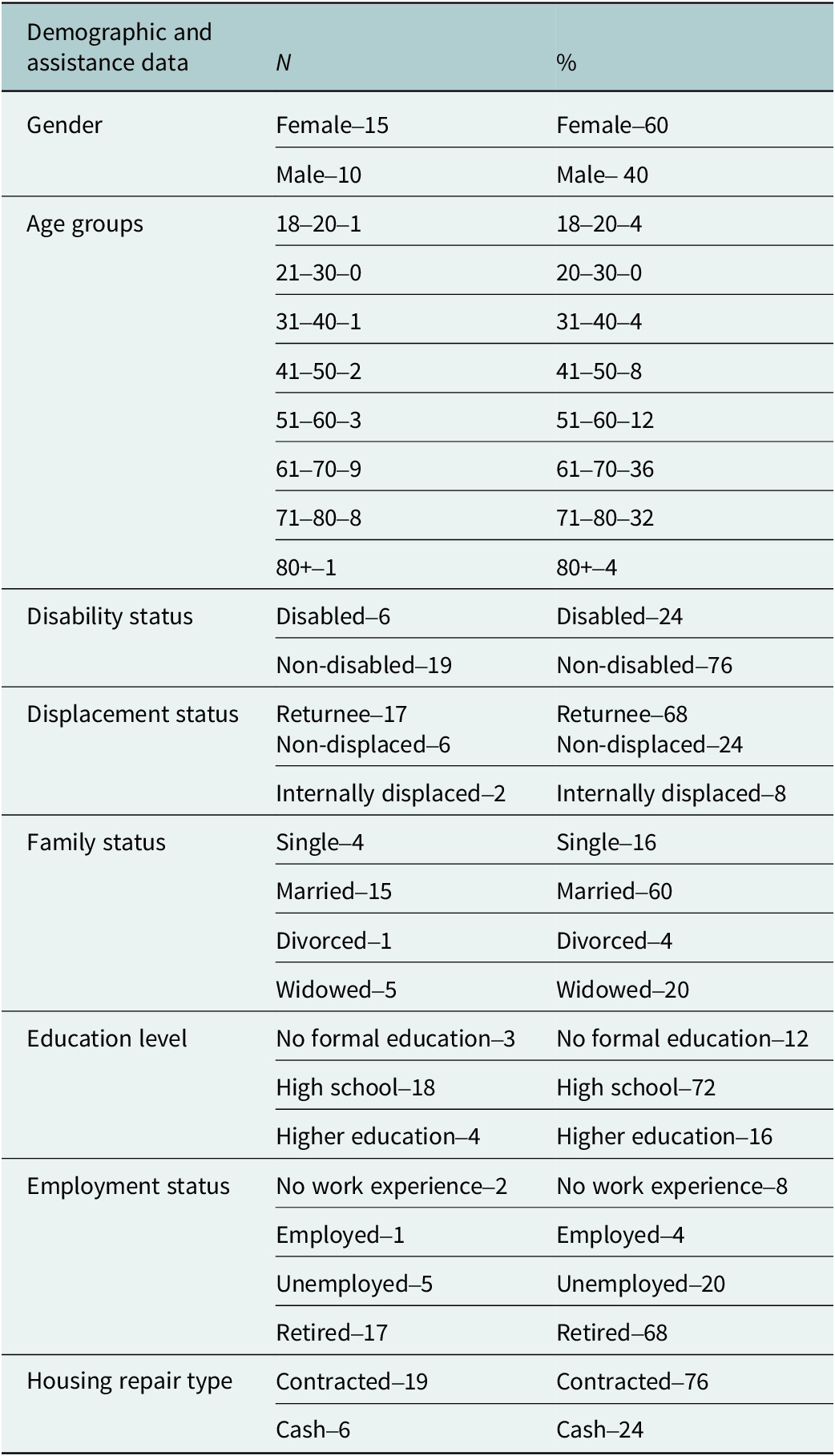
Among 60 potential households, 20 consented to take part, comprising a total of 25 individuals (see Table 1 for details). More women than men participated (15). The age range of participants was broad (18–80+ years), but the majority (18) were over the age of 60 years (mean-63.8 years; median-68 years). The study also included six disabled participants. Most participants were returnees (17; 68%) and received contractor-led (as opposed to cash) repairs (19; 76%). The sample is representative of the population in the region (IOM, 2025b).
Overview of interview participants (25 across 20 households)

A semi-structured interview guide was developed in collaboration with the Ukrainian Medair MHPSS staff who work in the Kharkiv Oblast. It was based on a semi-structured interview guide co-produced in a prior study with people who experienced distress following the war in Bosnia and Herzegovina (Maglajlic et al., Reference Maglajlic, Vejzagić, Palata and Mills2024). That study explored people’s lived experiences of distress and support to remedy distress (professional and otherwise). Use of such a broad guide (focused on the understanding of distress, well-being and support for any distress) helped to address concerns about bias and ethics of a humanitarian organisation that provides shelter and MHPSS doing research people in need who are in receipt of their support.
To further address concerns about bias, interviews were conducted by social science students from the National University of Kharkiv. A group of student volunteers was provided with training on qualitative interview skills and offered fieldwork support and supervision. Despite their initial interest, only two conducted fieldwork on the project, together with the Medair Ukrainian MHPSS team manager, who became the local research lead (Sydorenko). All participants were provided with an opportunity to check their transcripts and to retain a copy of it. Based on the current good practice guidance for international development research (Thorley and Henrion, Reference Thorley and Henrion2019), each participant also received remuneration in-kind for their time (a well-being package in the value of 25 USD).
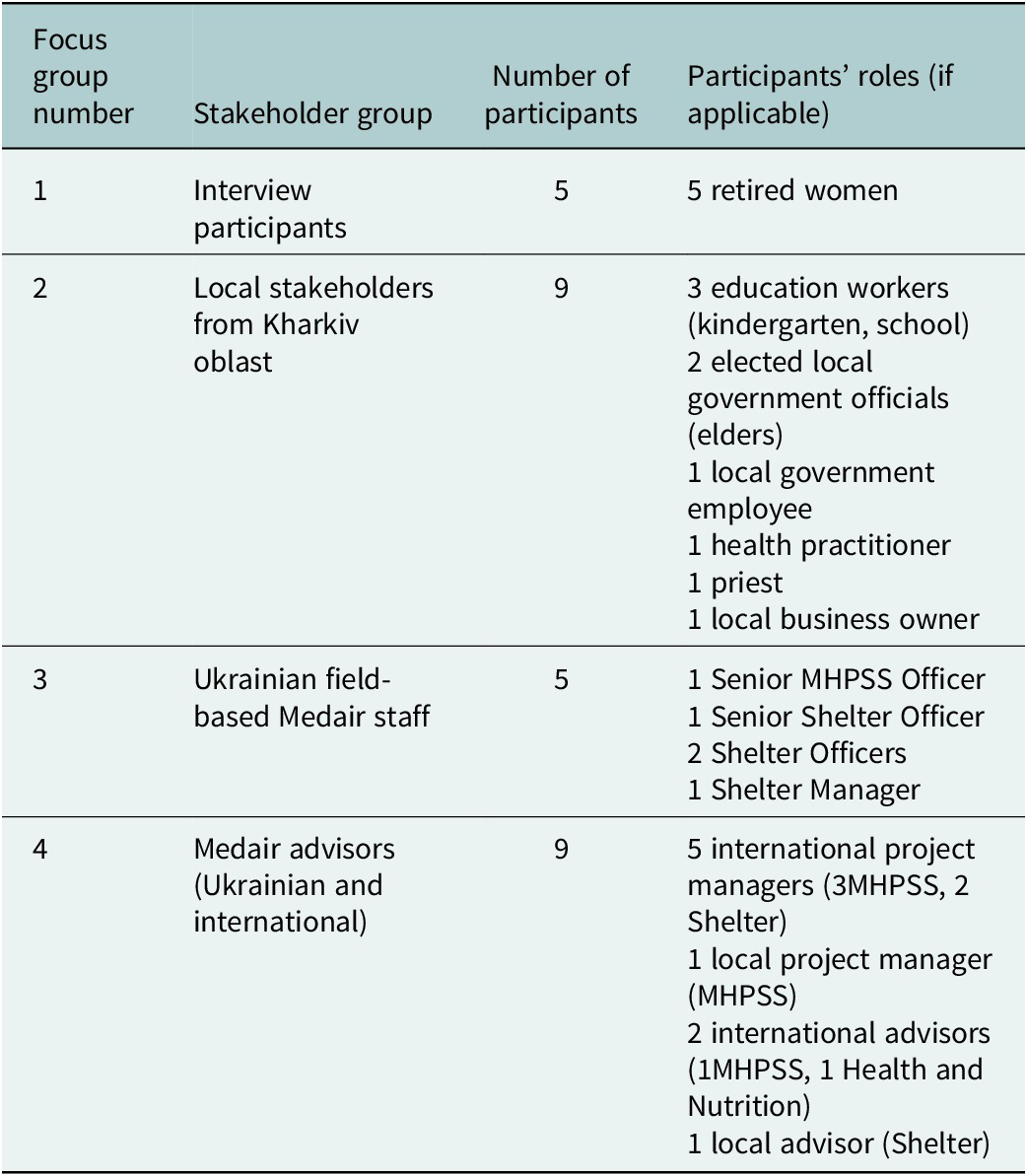
Following the initial analysis of the interviews, a focus group topic guide was developed by the main research team (Maglajlic, Sydorenko and Burnham). Four focus groups were an opportunity to review the key study findings and further explore their relevance for future programming with different stakeholder groups (representatives of interviewees, local community leaders, as well as Medair local and international advisers, managers and staff). Each focus group had 5–10 participants and lasted 60–90 min. An overview of the focus group participants is provided in Table 2. Each focus group was recorded, with key notes and conclusions agreed with the participants at the end of the focus group.
Focus group participants

The main research team, comprised of the three authors, conducted the inductive content analysis of the interview and focus group data (Pope et al., Reference Pope, Ziebland and Mays2000), bringing different perspectives to its interpretation – local knowledge and knowledge of the MHPSS (Sydorenko), knowledge of international humanitarian shelter programming (Burnham) and knowledge on war-induced distress and community-based support (Maglajlic). Team members read and re-read the transcripts from the interviews and focus groups, before comparing individual analyses to identify key themes and findings for the overall study.
Findings
Findings presented in this article focus on the impact of shelter repairs on participants’ well-being and participants’ suggestions of how to best strengthen links between the MHPSS and shelter support. Each theme is expanded upon through a quote from the study participants.
Home as an anchor and site of economic security
Findings stress the importance of shelter repairs for the study participants’ sense of well-being due to the central role home has in people’s lives. Participants described it as ‘our anchor, our life […] home is home, it’s our home, and that’s it […] It’s like a soul […] our roots are very deep, so we are very attached [to this place]’ (a female returnee in her late 60s who received contracted repairs).
Home was also identified as a site of participants’ economic security, particularly to grow their own food, as ‘it’s our way of making a living’ (internally displaced man in his 80s who received contracted repairs). When talking about their lives more generally, participants stressed how even before the invasion, people living in their region (Kharkiv) experienced joblessness, poverty and food insecurity. Food production is an important part of people’s economic well-being, as well as intertwined with the meaning of home. Invasion exacerbated the feeling of economic insecurity, which the participants noted during the study. This is also intertwined with concerns about the future and people’s well-being.
Children are graduating, graduating the universities. But it’s difficult to find job. Even if you find it – you earn only 8,000 UAH [a low salary]. How can the child of 24 build the family, to give a birth to a child and with 8,000 to feed this child? [--] And it’s happening that our specialists are going abroad [--] Who will stay in our Ukraine? Who will our Ukraine be for? (a follow up focus group with the interviewees, female participant)
Impact of home repairs on the participants’ well-being
Repairs to participants’ homes had a positive impact on their well-being and gave them ‘a new lease of life’. Participants also valued the attentive care with which the repairs were managed (if in receipt of contracted repairs).
Somehow the relation of repairs to this, this meaning of life appeared in me, [--] I was like an old woman who is broken trough [Ukrainian idiom meaning ‘completely broke’]. I did not think that I would have my own house like this. How to say, they put their soul into it, compassion. They treated me personally with such care. (a female returnee in her early 60s who received contracted repairs)
Equally, a lack of comprehensive repairs or repairs that were not done well also impacts participants’ well-being.
The main [problem I have] is the absence of the roof. It’s the most important. That side of the house will be leaking in winter when it rains. That they [repair team] glued the holes there. Summer is hot — it got unglued. (a non-displaced woman in her early 70s who received contracted repairs)
Role of MHPSS in shelter support: The hidden value of talking
During the interviews conducted in the study, only one interviewee explicitly spoke about mental health or psychosocial support services they received during their displacement. Other interviewees noted their appreciation for the visits and attentive support provided by the humanitarian staff more broadly – such as the shelter support field staff.
And then V. and A. [Medair staff] arrived [--] It was 40 days after my husband’s death. I didn’t believe that someone could help me [--]. Even on January 2, they came and wished me a Happy New Year…I was alone, it was very nice that they took care of me here. I realized that their help would really come… (a returnee woman in her early 60s who received contracted repairs)
However, there was other evidence of the value of interpersonal support for their well-being. The majority of female participants offered detailed accounts of their experiences since the invasion, even during the initial telephone contact to see if they were interested in taking part in the study. All greeted the interviewers in their home with ‘a spread,’ offering food and refreshments as when welcoming family and guests, regardless of the availability of food for the household. They wanted to be visited again and to establish relationships with the interviewers. During the interview, participants also offered detailed accounts of everything that had happened to them since the start of the invasion.
I’m talking, I was kind of very worried [about the interview]. I was very worried, I don’t know, what if I say something wrong [--] And it’s so easy to talk to you. And now I feel fine, yes, even though the memories are hard. (a returnee woman in her early 60s who received contracted repairs)
Shelter support field staff also noted that the residents they support often talked to them not just about the repairs needed, but also about their experiences during and after the invasion.
Single, elderly people [we visit] […] they need to hold your hand. She will stand near the wicket in order not to let you leave her yard. She will stand with her back to the wicket – “Here is my little cat, here is my little dog. Let’s go, I’ll show you what I’ve already done here […] And there was a hit over there. Do you want me to lead you to my neighbours?” And all of it she will tell you. And you already finished the survey and drawing. And you are standing, speaking. (Ukrainian shelter support staff member who took part in the focus group)
Beyond professional assistance, this also extends to the importance of mutual care and support in their families and communities.
When [my husband] died, I thought the life was over. I just didn’t know what to do [--]. After his death, all relatives comforted me. As soon as they are over with their stuff, they call me to check how I am. Everything is fine, emotions, I think, can be coped with. Still, it’s [--]. Sometimes I go to the garden and sit. Bad thoughts run around. Also my mother is next to me. I go to her. Still, it’s a care. You could say that by taking care of my mother, I distract myself from my bad thoughts. (a returnee woman in early 60s who received contracted repairs)
While for some participants mutual support focused on face-to-face interactions with family members and neighbours, for others it involved calls with family members and friends who were now living either in other parts of Ukraine or abroad. This highlights the importance of restoring/supporting communication services people use to maintain their family and community networks even when they are physically separated.
A1: We are on a call with our son. Every morning and evening.
A2: He says, “You care too much.”
A1: Well, it’s comforting. I heard his voice – that’s it, I’m calm now. (returnee couple in their late 50s who received cash for repairs)
Suggestions on how to strengthen links between MHPSS and shelter programming
Participants’ suggestions on how to strengthen MHPSS through shelter programming focused on two key issues. First, participants stressed the importance of internal home repairs and homemaking on their well-being. This contrasts with the primary role of humanitarian repairs that the participants received, which focuses on the light and medium repairs (e.g., to the roof and windows) to ensure people’s homes are habitable regardless of the weather conditions.
Well, it’s clear that I want to add [internal] repairs. Because NGOs do not take up internal work. None. That’s the biggest issue for me. (a returnee woman in early 60s who received contracted repairs)
Our corridor was damaged, and the ceiling, and the kitchen. We hired our people, hired and made everything with our money. The [monthly] pension we have, we collected a bit from it the whole year and repaired it somehow. (a non-displaced woman in her early 70s who received contracted repairs)
The second recommendation focuses on the importance of community revitalisation and economic regeneration. Participants stressed how important it would be to invest in community services and activities that had stopped due to the full-scale invasion. They highlighted difficulties accessing education and remote learning, as well as a lack of free-time activities for children and youth, as well as for older people. Beyond one-to-one support, such findings suggest that MHPSS should include activities focused on community revitalisation to support people’s well-being and capacity for self-recovery.
I think it would be better for my sister to study offline there. You know, communicate with people […] there are not many children here. And she stays home alone […] But she needs to somehow communicate with her peers to be more sociable. It turns out that the only friends here are our neighbours […] I would like her to go to school, like I did. I communicated with my classmates, learned to write, read, I played there, ran. But she misses all that. (a young woman in her late teens whose household received contracted repairs)
A3: Of course, I wish there were some more hobby groups for children, so that they could draw or play games. Because children have nowhere to go.
А2: Leisure, arranging leisure time for children is very important. (from the focus group with local leaders)
To successfully address these recommendations, future MHPSS programming would need to include consideration of local transportation and telecommunication, as these are disrupted due to the ongoing conflict, and important to facilitate inclusion of community reintegration activities into future MHPSS programmes. Overall, uncertainty due to the ongoing invasion and a lack of jobs impacts people’s well-being and their ability to plan for their future.
What helps is [--] The hope, that all this will be fine [--] Indeed, it will be possible to make some real plans. And now, [I have] some kind of apathy [--] What kind of plans can I make? I don’t know what will happen next month. Maybe I’ll really have to move somewhere. I really don’t want to. (a non-displaced man in his late 40s who received cash for repairs).
Discussion
This qualitative study explored perspectives of the Medair beneficiaries in a rural region of eastern Ukraine on the impacts of shelter repairs to their psychosocial well-being and opportunities to strengthen the links between the MHPSS and shelter programming. Here, we wish to explore the implications of the key findings in relation to other existing research on mental health, shelter and conflict-affected contexts such as Ukraine.
Findings highlight that shelter support alone positively contributes to the overall sense of well-being for rural communities in the East of Ukraine, giving them ‘a new lease of life.’ This corroborates the Global Shelter Cluster (2024a) assertion that shelter is a foundation for wider community outcomes. In contexts such as rural areas of the Kharkiv region in Ukraine, home is also a source of food security, as well as broader economic security. Coping with food insecurity and its impact on households has been highlighted as important for conflict-affected settings (Shemyakina, Reference Shemyakina2022). The focus on people’s lived experience in this study demonstrates the importance of understanding the socio-economic context before the conflict – how joblessness, poverty and food insecurity were pervasive even before the 2022 Russian invasion. Beyond integration between Shelter and MHPSS programmes, these findings indicate the relevance of their integration with other humanitarian sectors, such as Food, Security and Livelihoods.
Fear of further loss and destruction lingered in their accounts. Human connection and the value of talking were not made explicit during the interviews, but present throughout the study process and findings. Participants place value on mutual care and support, principally within their families, but also in their neighbourhoods – corroborated by Frankova et al.’s (Reference Frankova, Leigh Bahmad, Goloktionova, Suvalo, Khyzhniak and Power2024) analysis of mental health and psychosocial support in Ukraine. The same analysis also highlights the stigma associated with seeking formal mental health support in Ukraine. The IMPC rapid situation analysis (2022, in Frankova et al., Reference Frankova, Leigh Bahmad, Goloktionova, Suvalo, Khyzhniak and Power2024, pl. 28) noted that humour, laughter and farming/gardening are important positive coping mechanisms in the country. This highlights the importance of implementing MHPSS with community integration activities, in collaboration or alongside shelter interventions.
To maintain links with their family and friends, participants frequently relied on telecommunication. There is a limited, but slowly growing, literature on the importance of information and communication technology (ICT) for families and communities facing separation due to the invasion (Khvorostianov, Reference Khvorostianov2025) and the importance of such ICT links for mental well-being (Hakala et al., Reference Hakala, Mielityinen, Peltonen, Laajasalo and Ellonen2025).
Study findings suggest several ways to strengthen the links between MHPSS and shelter support. First, participants’ accounts stress the importance of internal repairs – already identified as an important connection between shelter and MHPSS (Global Shelter Cluster, 2024c). The second concerns the type of interventions that should be considered as a relevant form of MHPSS. Community revitalisation, implemented alongside shelter support, was suggested as a relevant way forward. Community engagement is already recognised as ‘a building block for self-recovery’ (Global Shelter Cluster, 2023, p. 24).
Operationalisation of such support needs to consider three elements. One is individual household support. Participants value talking to the humanitarian staff who visit their homes to arrange shelter support. The second concerns the need for community-level services. A community link is needed to liaise with the local residents and provide relevant support to initiate (re)development of community services – from education for children to free time activities for the whole community, such as arts activities and social gatherings. The final element concerns preparation for development, including economic regeneration, due to a lack of employment opportunities in the region. This finding is not surprising considering that poverty, inequality and corruption rates in Ukraine are among the highest in Europe (Frankova et al., Reference Frankova, Leigh Bahmad, Goloktionova, Suvalo, Khyzhniak and Power2024).
Study findings also suggest a need to address several contextual issues, including staffing, staff support, funding requirements and coordination between the local, national and international stakeholders. Relevant psychosocial support for this part of the Kharkiv region includes a range of suggested activities that are beyond the scope or remit of a single humanitarian organisation. Hence, development of support signposted as relevant would require coordination between the existing local, national and international stakeholders, as well as across humanitarian and development international initiatives. As noted by Kamali et al. (Reference Kamali, Munyuzangabo, Siddiqui, Gaffey, Meteke, Als, Jain, Radhakrishnan, Shah, Ataullahajan and Bhutta2020, p. 1), ‘multisectoral collaboration and better use of existing support networks are encouraged to increase reach and sustainability of MHPSS interventions’. In Ukraine, such cross-sectoral collaboration needs to be strengthened (Frankova et al., Reference Frankova, Leigh Bahmad, Goloktionova, Suvalo, Khyzhniak and Power2024).
Conclusion
Findings from the study contribute to the evidence of shelter support as a foundation for wider outcomes in humanitarian assistance (Global Shelter Cluster, 2024a), as well as the need for integrated and coordinated practice with other humanitarian sectors, including MHPSS and Food, Security and Livelihoods, among others. Coordination and integration should focus on the needs and context of the community it serves and the resources available. Experiences of the participants in the Balakliia Territorial community in Ukraine spotlight the importance of practice that addresses social determinants of distress through community revitalisation. Ongoing uncertainty due to the continued invasion exacerbates people’s poverty, as well as fears and concerns for the future. Stigma and isolation due to the ongoing invasion prevent engagement with other types of MHPSS support.
The study showcases the importance of using qualitative baselines and narratives in shelter and MHPSS humanitarian programming from the start of planning for humanitarian interventions (Care International UK and CENDEP, 2022). Further research that focuses on beneficiary experiences and needs across different war-affected contexts is needed to create broader and more robust evidence. This would allow evidence to consider different cultural and social contexts relevant for the integration of humanitarian assistance (Klenge, Reference Klenge2024). Context is and remains ‘everything’ not just for the shelter programming (Global Shelter Cluster, 2021, p. 5), but broader humanitarian interventions. Such studies should also include longitudinal approaches to explore people’s experiences over time, as the conflict goes on (Rizzi et al., Reference Rizzi, Ciuffo, Sandoli, Mangiagalli, de Angelis, Scavuzzo, Nych, Landoni and Ionio2022), but also into the post-conflict period. This would require collaboration between different stakeholders, beyond the Global Shelter Cluster alone.
These findings should be considered in light of study limitations. The study was conducted by a single humanitarian organisation (Medair), with the people in need in receipt of Medair shelter support, and in one region (Balakliia territorial community, Kharkiv Region). It was also conducted during the ongoing invasion, felt acutely in the east of Ukraine where the fieldwork was conducted. This presented multiple challenges to recruitment, as well as safety for the research team and the participants. The study also focused on rural areas, while urban contexts may be more challenging to self-recover (Global Shelter Cluster, 2023). Despite every effort to ensure diversity across the sample, there is also greater dominance of experiences among people who received contracted repairs, women and older adults (60+ years). This is representative of the returnee population (IOM, 2025b).
Collaboration between MHPSS and shelter sectors is dependent on the staffing, staff support, as well as donor funding conditions for humanitarian interventions. With fewer resources available for humanitarian interventions, challenges faced by humanitarian staff working in beneficiary-facing roles and their managers may become more prevalent and more impactful in terms of support available to conflict-affected communities. Advocacy to ensure more flexible funding relevant to the needs of beneficiary communities, with relevant support built in for the staff, is central to support such work.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10199.
Acknowledgements
Lilia Zotova, PhD, Associate Professor of the Department of Applied Psychology of V.N. Karazin Kharkiv National University, collaborated with the study team in training and recruiting student interviewers to engage in this work. Data collection was carried out by Daria Melnyk and Valeriia Turas, students at V.N. Karazin Kharkiv National University, Ukraine. One interview was carried out by Oksana Mykhailova, a Medair MHPSS staff member. Serhii Uzhehov, Medair Ukraine, as well as Wendy Dyment and Johan B. ten Hoeve from Medair Global, also contributed to the finalisation of the study report.
Author contribution
R.A.M. was the principal investigator for the qualitative study framework and methods. O.S., Medair Ukraine, was the in-country lead researcher, who also conducted half of the interviews, as well as being involved in shaping the study tools and the analysis. M.B., Medair Ukraine, provided in-country research support and was involved in the study analysis and the finalisation of the report. R.M. and L.L., Medair Ukraine, were involved in the commissioning of the study and preparation of its methodology. P.G. and C.A., Medair Global, were involved in the finalisation of the methodology and of the study report.
Financial support
This study was funded by the German Federal Foreign Office through Medair.
Competing interests
For all authors.
Reima Ana Maglajlic was commissioned as the Principal Investigator by Medair International. During the study, all remaining authors were employed by Medair Ukraine and Medair Global.
Ethics statement
The Institute of Public Health Policy in Ukraine provided the ethical approval for the study. Informed consent was first secured via the phone and then in person, before the start of the interview. An information sheet, as well as a verbal explanation of the study purpose, was provided to each participant. All participants were able to withdraw their participation from the study at any point.
Support for participants’ well-being during or immediately after the interview was organised by the Ukrainian MHPSS staff member who was the local research manager for the fieldwork (Sydorenko). Check-in was organised with the interviewees (and interviewee focus group participants) before and after the fieldwork visit. They were signposted to further support, if and where needed, organised through Ucare (online) support.
The main researcher (Maglajlic) supported and supervised the local research lead (Sydorenko), who, in turn, supported and supervised the local student researchers. This included regular debriefs, check-ins and supervision after each data gathering visit (for the student researchers) and throughout the study (for the local research lead).


 Open access
Open access
Comments
Dear colleagues,
This study was conducted for a humanitarian organisation Medair. Medair colleagues wanted to prepare an academic publication as a result of the study, as little is written on the topics of the study (links between the shelter and MHPSS support). It is based on a report that has been published by Medair, but they wanted to ensure it’s reach to academic audiences (https://www.medair.org/news-stories/exploring-links-between-psychosocial-well-being-and-humanitarian-shelter-support). We have suggested potential reviewers for the article.
On behalf of the authors, kind regards,
Reima Ana Maglajlic