


Introduction
Coxiella burnetii is a zoonotic intracellular gram-negative bacterium transmitted by aerosols from infected livestock. Reference Anderson, Bijlmer and Fournier1 Chronic infection may involve prosthetic valves, vascular grafts, aneurysms, or bone. Reference Anderson, Bijlmer and Fournier1 Vascular infection with vertebral osteomyelitis has been reported. Reference Fournier, Casalta, Piquet, Tournigand, Branchereau and Raoult2,Reference Virk, Mahmood and Kalra3 Diagnosis may be missed because symptoms are indolent, blood cultures are typically negative, and exposure history may not be elicited early. Serology remains the diagnostic standard, while PCR is specimen- and timing-dependent. Reference Anderson, Bijlmer and Fournier1 Plasma microbial cell-free DNA sequencing (mcfDNA-seq) is a noninvasive adjunct for selected culture-negative infections when the differential includes fastidious organisms. Reference Blauwkamp, Thair and Rosen4,Reference Park, Chang and Ledeboer5 Prior reports describe mcfDNA-seq detection of C. burnetii in culture-negative endocarditis and acute Q fever. Reference Kondo, Dalai and Venkatasubrahmanyam6,Reference Ranganath, Khodadadi and Abu Saleh7 We present a case in which mcfDNA-seq unexpectedly redirected evaluation toward chronic Q fever, while emphasizing confirmatory testing and limitations.
Clinical case
A 69-year-old man from Kansas with prior thoracoabdominal aortic aneurysm repair was transferred on hospital day 0 for suspected aortic endograft infection after 1 year of back pain and several months of chills. His history included rheumatoid arthritis treated with prednisone 5 mg daily and tobacco use. Before transfer, he had undergone outpatient spine injections and a nerve block. At an outside hospital on day-7, L1 bone biopsy showed fibrosis/chronic inflammation without malignancy; blood cultures and bacterial/acid-fast bacilli cultures from bone biopsy and psoas abscess pus had no growth. He took amoxicillin for a dental abscess before transfer. After the mcfDNA-seq result, a focused exposure history revealed work in an oil field, residence near cattle, and walks near cattle and sheep excretions.
Magnetic resonance imaging showed thoracolumbar discitis/osteomyelitis from T10 through L2 with T12 and L1 compression fractures and paraspinal/psoas inflammatory signal (Figure 1(A)). F-18 fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT) demonstrated intense linear uptake along the thoracoabdominal endograft, hypermetabolic paraspinal soft tissue involvement extending from T10 through L4, and intense uptake in the left psoas muscle corresponding to abscess formation (Figure 1(B)). These findings supported aortic endograft infection with contiguous osteomyelitis and psoas abscess.
Multimodal imaging of aortic endograft infection with contiguous vertebral osteomyelitis and psoas involvement. (A) Sagittal short tau inversion recovery magnetic resonance image of the thoracolumbar spine shows abnormal marrow signal from T10 through L2 with endplate irregularity, disc involvement, T12 and L1 compression fractures, and paraspinal/psoas inflammatory signal. (B) Coronal fused F-18 fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT) image shows linear hypermetabolic activity along the thoracoabdominal aortic endograft, paraspinal soft tissue involvement, vertebral body uptake, and focal left psoas uptake. (C) Sagittal fused FDG PET/CT image shows hypermetabolic activity along the aortic endograft and adjacent anterior vertebral bodies. (D) Adjacent sagittal fused FDG PET/CT image shows hypermetabolic thoracolumbar vertebral and paraspinal soft tissue uptake. (E) More lateral sagittal fused FDG PET/CT image shows hypermetabolic uptake extending to the psoas compartment. Physiologic uptake is present in the brain, renal collecting systems, and urinary bladder.

Figure 1. Long description
Panel A: Sagittal short tau inversion recovery magnetic resonance image of the thoracolumbar spine shows abnormal marrow signal from T10 through L2 with endplate irregularity, disc involvement, T12 and L1 compression fractures, and paraspinal/psoas inflammatory signal. Panel B: Coronal fused F-18 fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT) image shows linear hypermetabolic activity along the thoracoabdominal aortic endograft, paraspinal soft tissue involvement, vertebral body uptake, and focal left psoas uptake. Panel C: Sagittal fused FDG PET/CT image shows hypermetabolic activity along the aortic endograft and adjacent anterior vertebral bodies. Panel D: Adjacent sagittal fused FDG PET/CT image shows hypermetabolic thoracolumbar vertebral and paraspinal soft tissue uptake. Panel E: More lateral sagittal fused FDG PET/CT image shows hypermetabolic uptake extending to the psoas compartment. Physiologic uptake is present in the brain, renal collecting systems, and urinary bladder.
Vancomycin and piperacillin-tazobactam were started empirically. Q fever was not the working diagnosis when plasma mcfDNA-seq (Karius Test; Karius, Inc., Redwood City, CA) was sent on day 1 for culture-negative endograft infection. On day 3, mcfDNA-seq detected low-level C. burnetii (<50 molecules/microliter), prompting doxycycline plus hydroxychloroquine, exposure reassessment, and serology (Supplementary Table 1). Q fever serology sent on day 5 resulted on day 8: phase I IgG 1:65,536, phase II IgG 1:4,096, and phase I/II IgM negative. With compatible imaging, this met Dutch consensus criteria for proven chronic Q fever vascular infection. Reference Kampschreur, Wegdam-Blans and Wever8 C. burnetii PCR was not performed on blood or tissue. Transesophageal echocardiography showed no vegetation or evidence of endocarditis.
On day 27, he underwent explantation of infected thoracoabdominal endografts, debridement, and graft reconstruction. Operative findings included infected aortic graft material, psoas abscess, T10-L2 osteomyelitis, and empyema. Operative cultures grew Eikenella corrodens; ceftriaxone was given for 10 days while doxycycline-hydroxychloroquine continued. He later developed acute-on-chronic subdural hematoma and hypotension requiring vasopressors and died on day 48.
Diagnostic stewardship implications
This case is not an example of inaccessible specimens or a stand-alone mcfDNA-seq diagnosis. Its incremental role was diagnostic reframing: C. burnetii was not considered during the prior evaluation, and the mcfDNA-seq result preceded serology by 5 days, prompting exposure reassessment and pathogen-directed therapy. The result did not replace serology, targeted PCR or sequencing, echocardiography, operative cultures, or surgical source control. The later E. corrodens result from local source-control specimens should be interpreted as complementary, temporally distinct microbiology rather than a direct measure of day-1 plasma-test sensitivity.
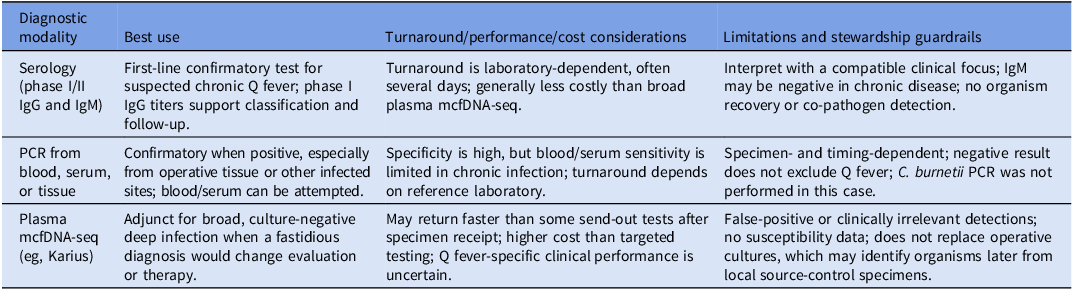
Stewardship should begin with the syndrome and intended actionability. For suspected chronic Q fever, targeted serology remains first-line and provides titers for follow-up; blood or tissue PCR can confirm infection when positive. Plasma mcfDNA-seq may be defensible when cultures are negative, prior antibiotics may reduce yield, the differential remains broad, and a fastidious diagnosis would change evaluation or treatment. However, it is costly relative to targeted testing, Q fever-specific clinical performance data are limited, and false-positive or clinically irrelevant detections can mislead care. Reference Kaur, Shaw and Multani9 Results require correlation with serology, imaging, cultures, operative findings, and infectious diseases consultation (Table 1).
Diagnostic stewardship comparison for suspected chronic Q fever with vascular graft or vertebral involvement

C. burnetii, Coxiella burnetii; IgG, immunoglobulin G; IgM, immunoglobulin M; mcfDNA-seq, microbial cell-free DNA sequencing; PCR, polymerase chain reaction.
Discussion
Chronic Q fever should be considered in culture-negative vascular graft infection or aneurysm infection, particularly with back pain, psoas involvement, immunosuppression, and livestock exposure. FDG PET/CT may localize C. burnetii vascular graft infection, but imaging establishes anatomy rather than etiology. Reference Merhej, Cammilleri, Piquet, Casalta and Raoult10 In this case, serology and imaging confirmed the mcfDNA-seq signal; absence of C. burnetii PCR from blood or tissue limits assessment of organism burden at the operative site. The fatal outcome precludes outcome-benefit claims.
Advanced diagnostics are most useful when ordered with a specific management question and interpreted conservatively. In suspected chronic Q fever with endovascular or vertebral involvement, plasma mcfDNA-seq may accelerate recognition when Q fever has not yet been considered, but it should be paired with confirmatory serology and tissue-based testing whenever possible. This approach preserves the diagnostic benefit of molecular testing while minimizing unnecessary antimicrobial exposure, false-positive or irrelevant detections, and low-yield testing.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/ash.2026.10782.
Data availability statement
Deidentified clinical details supporting this case report are not publicly available because of patient privacy considerations.
Acknowledgments
The authors thank the clinical teams involved in the care of this patient. OpenAI ChatGPT (GPT-5.5 Pro) was used solely for minor editorial assistance related to grammar and language clarity. All content, analysis, and conclusions were developed by the authors.
Author contribution
Conceptualization: A.J., M.A.A. Data curation: A.J. Formal analysis: A.J. Investigation: A.J., S.K., R.S., A.H., A.A.F. Methodology: T.L. Project administration: M.A.A. Supervision: M.A.A. Visualization: A.A.F. Writingoriginal draft: A.J. Writing—review and editing: T.L., S.K., R.S., A.H., A.A.F., M.A.A. All authors reviewed and approved the final manuscript.
Financial support
None reported.
Competing interests
S.K. and M.R.S. report honoraria or consulting fees from Karius Inc. A.J., A.H., T.L., A.A.F., and M.A.A. report no conflicts of interest relevant to this article.
Patient consent
This case report was reviewed by the Baylor College of Medicine Institutional Review Board and determined to meet criteria for exemption; separate patient consent for publication was not required. No identifiable patient information is included.




 Open access
Open access