


Severe mental illnesses (SMI; conditions such as schizophrenia, schizoaffective disorder and bipolar disorder) are associated with a significant reduction in life expectancy, known as the mortality gap. Reference Fiorillo and Sartorius1 On average, people with SMI die 15–20 years earlier than those who do not have SMI. Reference Fiorillo and Sartorius1,Reference Siddiqi, Doran, Prady and Taylor2 Although a portion of this variation is attributable to suicide and accidental death, the main contributory factor to this inequality is the largely preventable poor physical health of people with SMI. Reference Fiorillo and Sartorius1–Reference Hayes, Marston, Walters, King and Osborn3 This includes higher rates of long-term physical health conditions and poorer outcomes from those conditions. Reference Formánek, Krupchanka, Perry, Mladá, Osimo and Masopust4–Reference Vancampfort, Correll, Galling, Probst, De Hert and Ward7
Chronic kidney disease (CKD) is a progressive condition that is often asymptomatic in the early stages, and is characterised by a sustained reduction in kidney function, typically staged by estimated glomerular filtration rate (eGFR). Reference Kalantar-Zadeh, Jafar, Nitsch, Neuen and Perkovic11 There are five stages of CKD according to the Kidney Disease Improving Global Outcomes guidelines and, in the latest stage (stage 5), kidney function is severely impaired, necessitating kidney replacement therapies including dialysis or renal transplantation. Reference Kalantar-Zadeh, Jafar, Nitsch, Neuen and Perkovic11 According to recent global health estimates, CKD affects approximately 843.6 million individuals worldwide, a figure that continues to rise due to population ageing, increasing rates of diabetes and hypertension and other potentially modifiable risk factors. Reference Kovesdy12 Projections indicate that, by the year 2040, CKD will rank as the fifth leading cause of life-years lost globally, highlighting its growing impact on public health systems. Reference Foreman, Marquez, Dolgert, Fukutaki, Fullman and McGaughey13
Cardiovascular death is the leading cause of mortality among individuals living with SMI, accounting for approximately 70% of all deaths in those diagnosed with bipolar disorder or schizophrenia. Reference Nielsen, Banner and Jensen5 Epidemiological studies have shown that individuals with SMI have a significantly elevated risk of both sudden cardiac death and overall cardiovascular mortality. Reference Nielsen, Banner and Jensen5,Reference Correll, Solmi, Veronese, Bortolato, Rosson and Santonastaso8 Cardiovascular mortality is also the leading cause of death among people with CKD. Reference Ndumele, Rangaswami, Chow, Neeland, Tuttle and Khan9,Reference Jankowski, Floege, Fliser, Böhm and Marx10 Although the relationship between SMI and long-term physical health conditions such as cardiovascular disease and type 2 diabetes has been relatively well documented, Reference Nielsen, Banner and Jensen5,Reference Vancampfort, Correll, Galling, Probst, De Hert and Ward7,Reference Han, Doran, Holt, Hewitt, Jacobs and Prady14,Reference Osborn, Wright, Levy, King, Deo and Nazareth15 CKD has not attracted the same attention despite available evidence suggesting that it may disproportionately impact people with SMI. Reference Carswell, Cogley, Bramham, Chilcot, Noble and Siddiqi16
Several medications used in the treatment of SMI can increase the risk of CKD. Reference Schoretsanitis, de Filippis, Brady, Homan, Suppes and Kane17 Lithium, a highly effective mood stabiliser used in the management of bipolar disorder and schizoaffective disorder, is associated with a range of renal side-effects, Reference Gupta and Khastgir18 including nephrogenic diabetes insipidus, tubulo-interstitial nephritis and long-term decline in glomerular function. Reference Schoretsanitis, de Filippis, Brady, Homan, Suppes and Kane17 Acute kidney injury (AKI) can also occur in cases of lithium toxicity, when serum lithium levels are elevated beyond the narrow therapeutic range. Reference Grünfeld and Rossier19 Antipsychotic medications, although not exhibiting the same renal side-effects, are known to induce or exacerbate metabolic syndrome, a cluster of conditions including obesity, dyslipidaemia, insulin resistance and hypertension, all of which are independently associated with increased risk of CKD. Reference Abosi, Lopes, Schmitz and Fiedorowicz20
Antipsychotic medications also contribute to the development of other conditions, such as type 2 diabetes mellitus and hypertension, which are well-established risk factors for CKD. Reference Hansrivijit, Chen, Lnu, Trongtorsak, Puthenpura and Thongprayoon21,Reference Webster, Nagler, Morton and Masson22 Additionally, health risk behaviours associated with CKD are more prevalent among people with SMI – including high rates of smoking, diets high in saturated fats, sugars and sodium and high levels of sedentary behaviour. Reference Kuma and Kato23 Social determinants of health, including poverty, housing insecurity and reduced access to preventive health services, may exacerbate these risks and contribute to poorer health outcomes in this population, including a higher risk of CKD. Reference Grant, Salim, Lees and Stevens24,Reference Reilly, Olier, Planner, Doran, Reeves and Ashcroft25
The early identification and proactive management of CKD are critical to mitigate progression to kidney failure and reduce cardiovascular mortality risk. Reference Okpechi, Caskey, Gaipov, Tannor, Noubiap and Effa26,Reference Neuen, Jun, Wick, Kotwal, Badve and Jardine27 Timely intervention, including identification of deteriorating eGFR and management of hypertension and diabetes, could slow CKD progression and improve survival outcomes. Reference Okpechi, Caskey, Gaipov, Tannor, Noubiap and Effa26,Reference Whaley-Connell, Nistala and Chaudhary28 To contribute to improved identification and appropriate care for people with coexisting SMI and CKD, the epidemiology of this comorbidity, including its prevalence and incidence, needs to be better understood. To date there has been no systematic review or meta-analysis on the risk of CKD among people with SMI. Reference Carswell, Cogley, Bramham, Chilcot, Noble and Siddiqi16 Therefore, we conducted a systematic review to describe the prevalence, incidence and risk of kidney disease among people with SMI.
Objectives
This review had two overarching objectives:
-
(a) Estimate the prevalence and incidence of CKD among people with SMI.
-
(b) Compare the prevalence and incidence of CKD among people with SMI with those in the general population or those who do not have SMI.
Method
This systematic review protocol was prospectively published Reference Carswell, Bramham, Chilcot, Jacobs, Osborn and Siddiqi29 and registered in the International Prospective Register of Systematic Reviews, no. CRD42024527215. Reference Carswell, Chilcot, Jacobs, Siddiqi, Osborn and Nisbet30
Search strategy
We initially searched Medline, Embase, PsycINFO, CINAHL, Scopus and Web of Science from conception until June 2024, and re-ran the search in February 2025. We used search terms specific to the population (people with SMI), outcome (CKD) and study design (epidemiological studies). The full search strings for the electronic databases can be found in the supplementary materials. We also carried out forwards-and-backwards citation searches to identify any relevant records not included in the database search, and searched the archives of subject-specific journals.
Study selection
Studies were included if they were epidemiological observational studies that reported the prevalence or incidence of CKD (any stage) in a population of adults with SMI. SMI was defined as any condition that can present with psychosis, including schizophrenia, schizoaffective disorder, bipolar disorder and depression with psychosis.
Studies were excluded if the denominator population did not consist of people with SMI, or of a majority with SMI (>50% of the denominator population). If studies did not report the proportion of people with SMI, these were also excluded. Studies were also excluded if they included participants who were under the age of 18 years (unless data for participants over the age of 18 could be extracted and analysed separately).
Studies were also excluded if they reported only the prevalence or incidence of AKI, or if they did not differentiate AKI from CKD.
Data extraction (selection and coding)
Screening and identification of included records was conducted using Covidence Veritas Health Innovation, Melbourne, Australia (www.covidence.org). Title, abstract and full-text screening was completed by C.C., R.E.N., J.K., A.H. and Z.P., with two independent reviewers reviewing each of the records at both stages and any disagreements resolved through discussion and consensus or, if needed, by consultation with an independent author.
Data extraction started on 5 September 2024. The data extraction table was piloted by C.C. and R.E.N., and data were extracted for each article by two of five independent reviewers (C.C., R.E.N., J.K., Z.P. and A.H.). The extracted data included author, year, publication type, aim of the study, country, World Bank designation, setting, study design, study duration, year(s) of data collection, sample size, participant demographics, SMI diagnostic tool, SMI diagnoses, psychiatric medication, data collection procedures, CKD stages and definition and prevalence and incidence of kidney disease. Studies that included a comparison group of the general population or a population without SMI had additional data extracted on the demographics of comparator groups, the prevalence or incidence of CKD in the comparator group and any risk, odds or hazard ratios reported.
Risk of bias
The risk of bias for each included study was assessed by two of five independent reviewers (C.C., R.E.N., J.K., Z.P. and A.H.) using the appropriate Joanna Briggs Institute (JBI) critical appraisal tools. Where discrepancies arose between scores or the choice of checklist, this was resolved through discussion and consensus and, if needed, referred to a third independent reviewer. Each study was scored based on the total number of items that applied to that study. Because there is no validated categorisation of quality within JBI critical appraisal tools, for this review, studies with no items checked as ‘no’ or ‘unclear’ were assessed as high quality, those with one item checked as ‘no’ or ‘unclear’ were assessed as moderate quality and those with two or more items checked as ‘no’ or ‘unclear’ were assessed as low quality.
Data analysis
Narrative synthesis
The characteristics of the included studies were summarised and described to provide an overview of the evidence.
Meta-analyses
Random-effect models were used in the meta-analyses to account for the high level of heterogeneity. As per the protocol, clinically heterogeneous studies were excluded from the meta-analyses due to the lack of similarity of patient cohorts (for example, studies that reported only the prevalence of CKD among people with SMI and a specific comorbidity were excluded from the analysis). Studies were also excluded if their study design did not result in reporting prevalence or incidence in a way that would allow pooling. In the meta-analyses of ratios, studies were included only if the comparison was between the prevalence or incidence of CKD in people with SMI and people without SMI or the general population. Comparisons with other populations, such as people with other mental health conditions (e.g. anxiety or depression), or between different types of psychiatric drugs, were not pooled.
Five meta-analyses were conducted:
-
(a) the pooled prevalence of CKD among people with SMI;
-
(b) the pooled incidence risk of CKD among people with SMI;
-
(c) the pooled incidence rate of CKD among people with SMI, per 1000 person-years, at risk;
-
(d) the pooled odds ratio of CKD among people with SMI compared with the general population;
-
(e) the pooled hazard ratio of CKD among people with SMI compared with the general population.
Sensitivity analyses
Where possible, sensitivity analyses were conducted to determine whether the method of identifying CKD influenced the pooled result. The methods of identification of CKD were categorised into the following:
-
(a) diagnostic code
-
(b) eGFR calculation
-
(c) eGFR calculation and albuminuria
-
(d) eGFR calculation and kidney biopsy
-
(e) self-report.
Sensitivity analyses involved removal of those studies that used self-report, albuminuria or kidney biopsy from the meta-analyses where relevant (because some of the meta-analyses did not include studies that used these methods of CKD identification), and examined the impact on the overall results. Finally, we conducted a subgroup analysis to explore whether pooled prevalence estimates differed according to the use of diagnostic codes or eGFR calculations.
Certainty of evidence
We used the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach to determine the certainty of the synthesised evidence. GRADE is used predominantly to assess the certainty of evidence on the effectiveness of interventions. Although it has not been formally adapted for systematic reviews of prevalence or incidence, we used an approach recommended by Borges Migliavaca et al Reference Borges Migliavaca, Stein, Colpani, Barker, Munn and Falavigna31 for applying GRADE to baseline risk or prognosis reviews.
Results
Figure 1 shows the Preferred Reporting Items for Systematic reviews and Meta-Analyses flow diagram. Following the removal of duplicates (n = 2350), 14 677 records were screened at the title and abstract stage, with 199 full-text articles screened for eligibility. At this stage, 151 articles were excluded. Reasons for exclusion included reporting wrong outcomes (n = 68), wrong patient population (n = 34) and wrong study design (n = 22). Records were also excluded if the full text was unavailable after contacting authors and requesting inter-library loans, including studies available only as conference abstracts (n = 22). In total, 48 studies were identified for inclusion in the review.
Preferred Reporting Items for Systematic reviews and Meta-Analyses flow diagram.

Description of included studies
Table 1 shows the characteristics of the included studies. The sample size of participants with SMI in the included studies ranged from 61 to 848 058, with a mean of 27 379. Publication dates ranged from 2003 to 2025, with more than half published between 2020 and 2025. Most studies used a cohort design (n = 30, 62.5%) and were published in high-income countries (n = 45, 94%). The countries most commonly reported were the UK (n = 10, 20.8%), USA (n = 7, 14.6%), Denmark (n = 6, 12.5%) and Sweden (n = 5, 10.4%). The majority of studies used population-level data (n = 31, 64.6%), with seven studies collecting data in a community setting (14.6%) and four collecting data in in-patient settings (8.3%).
Overview of included studies

SMI, severe mental illness; WB, World Bank; CKD, chronic kidney disease; JBI, Joanna Briggs Institute; HIC, high-income country; ESRD, end-stage renal disease; NR, not reported; UMIC, upper-middle income country.
a. Denominator sample size for reporting prevalence or incidence (excluding controls used in any comparisons).
In terms of the denominator population, 17 studies collected data only from people with bipolar disorder (35.4%), and 11 included only people with schizophrenia (22.9%). Six studies included people with bipolar disorder and schizoaffective disorder (12.5%), and the remaining studies collected data from a population with mixed SMI diagnoses (n = 14, 29%). Thirteen studies collected data only from people who had been exposed to lithium (27.1%), and 13 collected data from populations with mixed exposure to lithium (27.1%), where a proportion of people were prescribed lithium and others were not. The remaining 22 studies (45.8%) did not report the proportion of the population prescribed lithium.
Among studies reporting the prevalence or incidence of CKD according to different stages, 27 (56.3%) used the catch-all term ‘chronic kidney disease’ without defining specific stages or eGFR thresholds to report the prevalence, and 13 (27.1%) reported stage 3 and above, typically defined as eGFR <60 mL/min/mL2. Most studies used medical records to identify CKD, either through diagnostic codes (n = 20, 62.5%) or eGFR calculations based on data from medical records (n = 14, 29.2%).
Meta-analysis of prevalence
Of the included studies, 25 were included in the meta-analysis of prevalence. Reference Reilly, Olier, Planner, Doran, Reeves and Ashcroft25,Reference Carney, Jones and Woolson32–Reference Na, Lee, Sohn, Yang, Park, Sim and Lee55 A sensitivity analysis was conducted to evaluate the impact of inclusion of the study conducted by Boivin et al, Reference Boivin, Le Daré, Bellay, Vigneau, Mercerolle and Bacle56 which reported a very high prevalence of 98%. That study was excluded from the meta-analyses because it altered the size and precision of the results, having focused only on patients who were hospitalised and prescribed lithium. The outcomes of the sensitivity analysis are included in the supplementary materials.
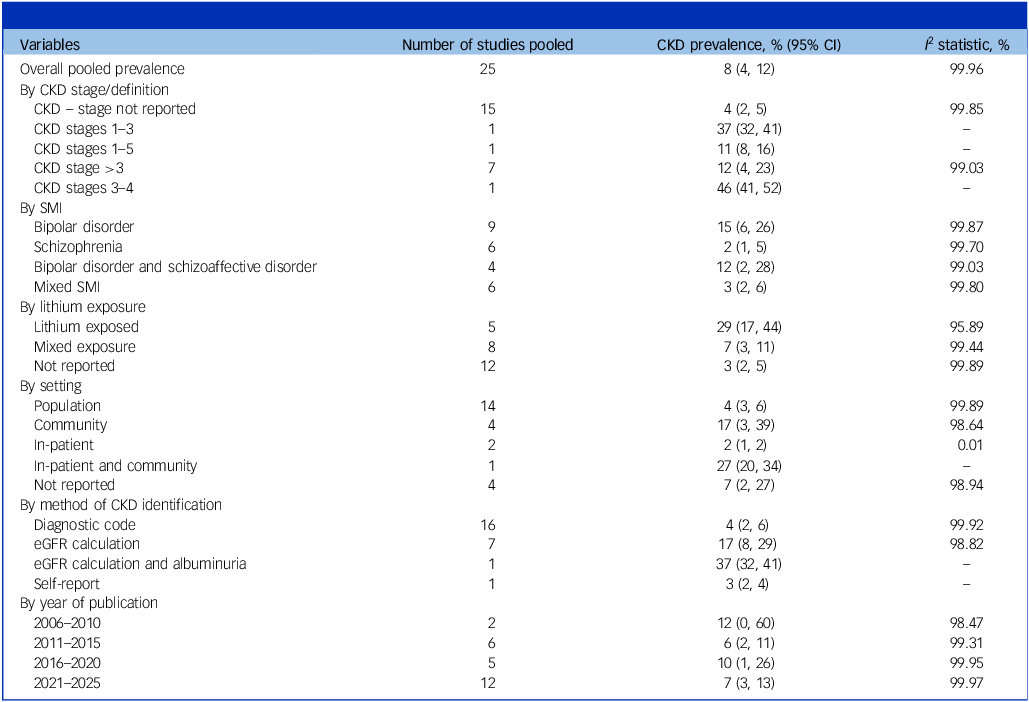
Table 2 shows the pooled prevalence of CKD among people with SMI. Subgroup analyses were conducted to examine how prevalence differed across CKD stage, SMI diagnoses, lithium exposure, setting and year of publication. The overall pooled prevalence of CKD among people with SMI was 8% (95% CI 4%, 12%). Studies that collected data only from people with schizophrenia had the lowest prevalence of CKD (2%, 95% CI 1%, 5%) compared with those where data were collected only from people with bipolar disorder (15%, 95% CI 6%, 26%). Additionally, studies reporting on the prevalence of CKD only among people with SMI exposed to lithium had a substantially higher prevalence (29%, 95% CI 17%, 44%) compared with those reporting mixed-exposure cohorts (7%, 95% CI 3%, 11%). A further sensitivity analysis was conducted to determine whether the exclusion of studies that used albuminuria or self-report to identify CKD influenced the results, but this had little effect (7%, 95% CI 4%, 11%).
Pooled prevalence of chronic kidney disease (CKD) among people with severe mental illness (SMI)

eGFR, estimated glomerular filtration rate.
The forest plot for the meta-analysis of prevalence, divided by year of publication, is shown in Fig. 2.
Pooled prevalence of chronic kidney disease (CKD) among people with severe mental illness (SMI). REML, restricted maximum likelihood.

Meta-analysis of incidence risk
Thirteen studies were included in the meta-analysis of incidence risk. Reference Hayes, Marston, Walters, Geddes, King and Osborn39,Reference Close, Reilly, Mason, Kripalani, Wilson and Main57–Reference Parsaik, Chaudhary, Sharma, Delgoffe, Gabor and Singh68 A sensitivity analysis was conducted to determine whether the exclusion of studies that used biopsy or self-report to identify CKD influenced the results. However, this did not result in a substantial change in the estimate (4%, 95% CI 0%, 11%).
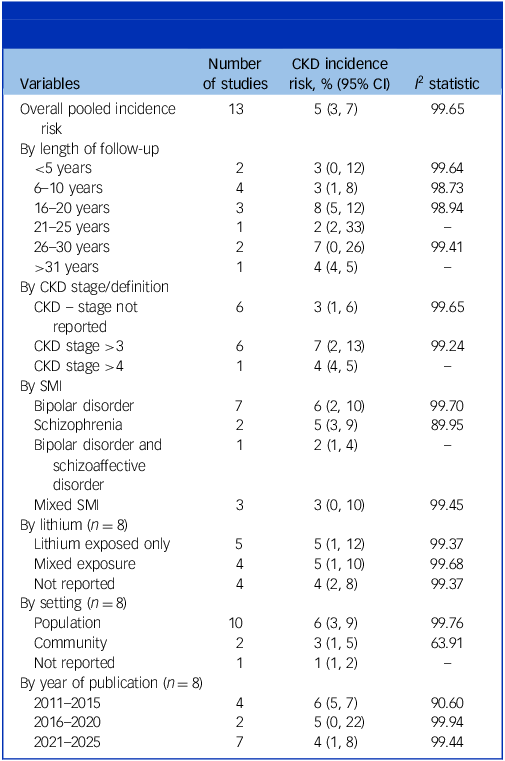
Table 3 reports the pooled incidence risk of CKD among people with SMI. Subgroup analyses were conducted to examine how incidence differed across length of follow-up, CKD stage, SMI diagnoses, lithium exposure, setting and year of publication. The overall pooled incidence risk of CKD among people with SMI was 5% (95% CI 3%, 7%). Studies reporting the incidence of CKD stage 3 and above had a higher incidence risk (7%, 95% CI 2%, 13%) compared with those that reported the incidence of CKD and did not specify a stage (3%, 95% CI 1%, 6%). Incidence risk was highest at 16–20 years’ (8%, 95% CI 5%, 12%) and 26–30 years’ follow-up (7%, 95% CI 0%, 26%), although most studies had fewer than 20 years of follow-up.
Pooled incidence risk of chronic kidney disease (CKD) among people with severe mental illness (SMI)

Figure 3 shows the forest plot for the meta-analyses of incidence risk of CKD, according to the length of follow-up.
Pooled incidence risk of chronic kidney disease (CKD) among people with severe mental illness (SMI).

Meta-analysis of incidence rates
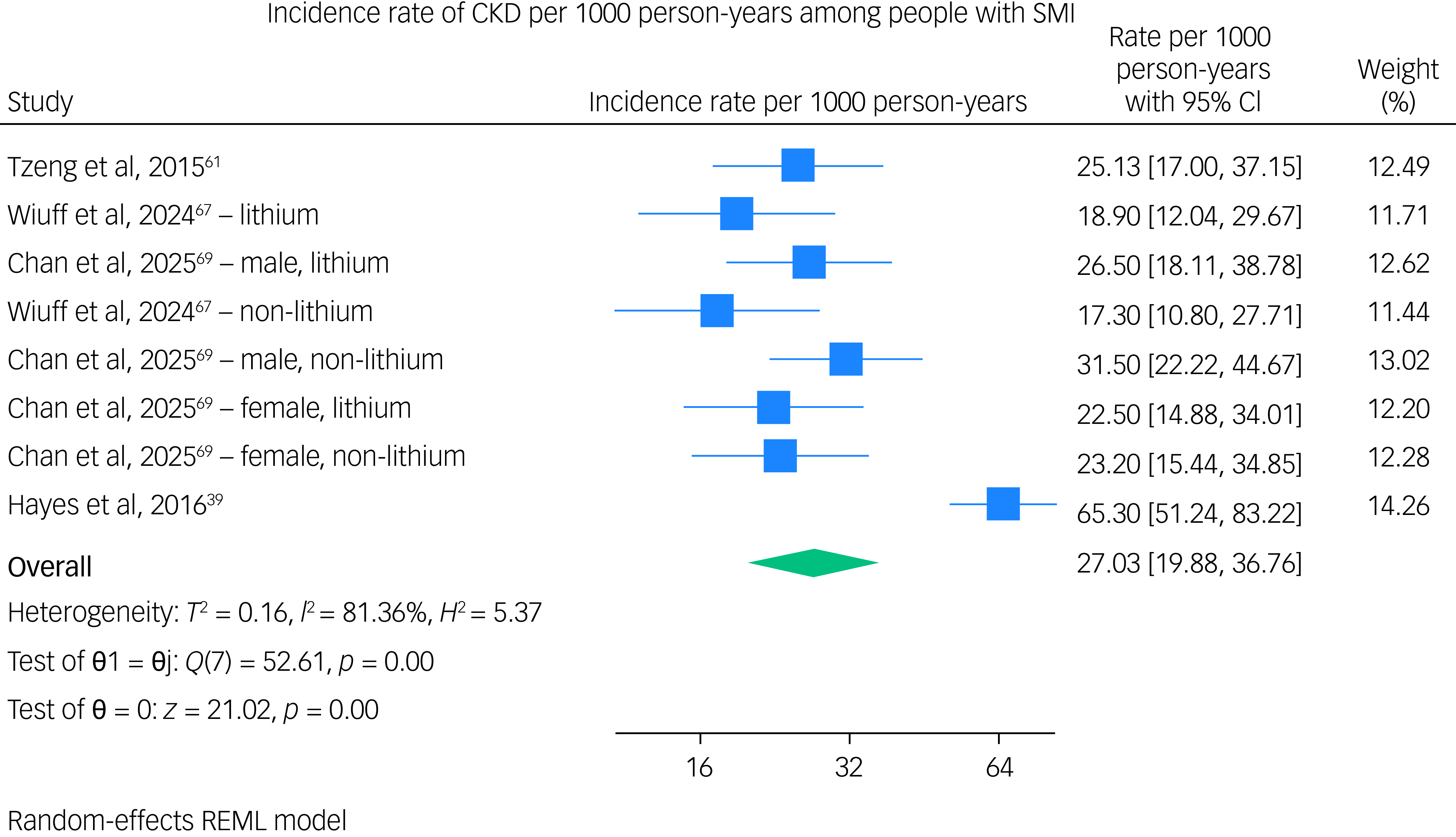
Four studies were pooled in a meta-analysis of incidence rates, Reference Hayes, Marston, Walters, Geddes, King and Osborn39,Reference Tzeng, Hsu, Ho, Kuo, Lee and Yin61,Reference Wiuff, Rohde, Jensen, Nierenberg, Østergaard and Köhler‐Forsberg67,Reference Chan, Solmi, Correll, Man Wong, Lo and Lai69 with one reporting rates specifically in people exposed to lithium and not exposed to lithium, Reference Wiuff, Rohde, Jensen, Nierenberg, Østergaard and Köhler‐Forsberg67 and another reporting incidence rates specific to lithium exposure and gender. Reference Chan, Solmi, Correll, Man Wong, Lo and Lai69 Therefore, eight different rates were pooled across four studies. The pooled incidence rate was 26.83 cases (95% CI, 18.66–38.58) per 1000 person-years. Figure 4 shows the forest plot for the meta-analyses of incidence rates.
Pooled incidence rates (per 1000 person-years) of chronic kidney disease (CKD) among people with severe mental illness (SMI).

Meta-analysis of odds ratios
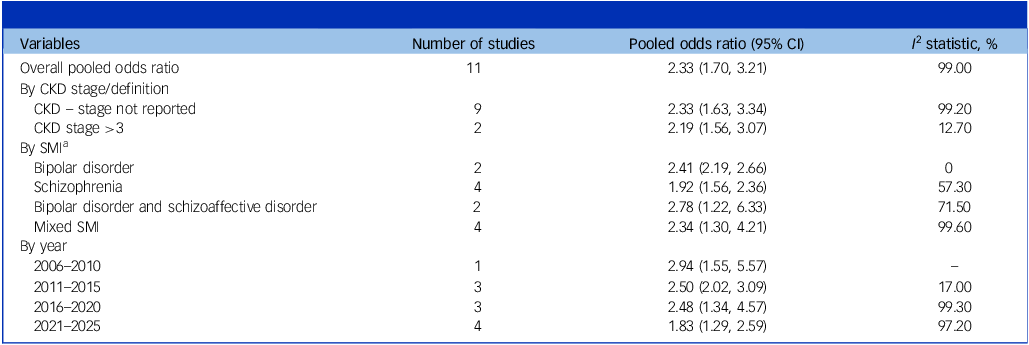
Eleven studies were included in the meta-analysis of odds ratios for the prevalence of CKD among people with SMI. Reference Carney, Jones and Woolson32,Reference Smith, Martin, McLean, Langan, Guthrie and Mercer36–Reference Schoepf, Uppal, Potluri and Heun38,Reference Iwagami, Mansfield, Hayes, Walters, Osborn and Smeeth41,Reference Tzur Bitan, Krieger, Berkovitch, Comaneshter and Cohen43,Reference Fransson, Werneke, Harju, Öhlund, de Man Lapidoth and Jonsson47,Reference Spooner, Afrazi, de Oliveira Costa and Harris48,Reference Taloyan, Alinaghizadeh, Wettermark, Jan Hasselström and Bertilson53,Reference Na, Lee, Sohn, Yang, Park, Sim and Lee55,Reference Bahorik, Satre, Kline-Simon, Weisner and Campbell70 Table 4 reports the pooled odds ratio of CKD among people with SMI compared with those without SMI or the general population. Subgroup analyses were conducted to examine how odds differed across CKD stage, SMI diagnoses and year of publication. Only one study reported the odds of CKD among people with SMI and lithium exposure compared with a population without SMI, Reference Iwagami, Mansfield, Hayes, Walters, Osborn and Smeeth41 and only one study reported the odds of CKD in an in-patient population with SMI compared with people without SMI; Reference Schoepf, Uppal, Potluri and Heun38 therefore, a subgroup analysis of odds ratios could not be conducted across lithium exposure and setting. A sensitivity analysis was performed to determine whether removal of self-reporting of CKD diagnosis influenced the pooled odds ratio, Reference Forty, Ulanova, Jones, Jones, Gordon-Smith and Fraser37 but this had a minimal effect (pooled odds ratio 2.25, 95% CI 1.62, 3.11).
Pooled odds ratios of chronic kidney disease (CKD) among people with severe mental illness (SMI) compared with those without SMI

a. Bahorik et al Reference Bahorik, Satre, Kline-Simon, Weisner and Campbell70 reported odds ratios separately for bipolar disorder and schizophrenia, whereas Iwagami et al Reference Iwagami, Mansfield, Hayes, Walters, Osborn and Smeeth41 reported odds ratios separately for those exposed to lithium and those not exposed.
The overall pooled odds ratio showed significantly higher odds of CKD among people with SMI than for those without (2.34, 95% CI 1.68, 3.25). These increased odds were observed across all subgroup analyses.
Figure 5 shows the forest plot for the meta-analyses of odds ratios.
Pooled odds ratio (OR) of chronic kidney disease (CKD) among people with severe mental illness (SMI) compared with the general population. DL, DerSimonian-Laird.

Meta-analysis of hazard ratios
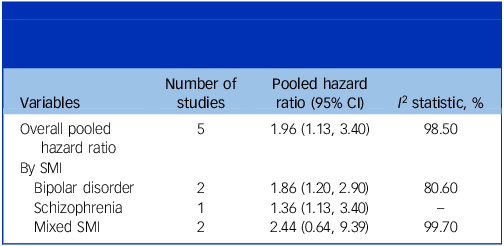
Table 5 reports the pooled hazard ratios of CKD among people with SMI. Reference Ponzer, Millischer, Schalling, Gissler, Lavebratt and Backlund52,Reference Kessing, Gerds, Feldt-Rasmussen, Andersen and Licht59,Reference Tzeng, Hsu, Ho, Kuo, Lee and Yin61,Reference Garriga, Robson, Coupland and Hippisley-Cox62,Reference Wiuff, Rohde, Jensen, Nierenberg, Østergaard and Köhler‐Forsberg67 Due to the limited number of studies that provided hazard ratio data (n = 5), only one subgroup analysis was conducted to explore the overall pooled hazard ratio for CKD among people with SMI, which was 1.96 (95% CI 1.13, 3.40).
Pooled hazard ratios for chronic kidney disease among people with severe mental illness (SMI) compared with the general population

Figure 6 shows the forest plot for the meta-analyses of hazard ratios according to SMI diagnosis.
Pooled hazard ratio (HR) for chronic kidney disease (CKD) among people with severe mental illness (SMI) compared with the general population. ESKD, end-stage kidney disease; DL, DerSimonian-Laird.

Studies excluded from meta-analyses
In total, eight studies were included in the review but excluded from the meta-analyses, Reference Presne, Fakhouri, Noël, Stengel, Even and Kreis71–Reference Fransson, Werneke, Öhlund, Jonsson and Ott78 the primary reason being clinical heterogeneity (n = 5). Of these five, Reference Chan, Solmi, Correll, Man Wong, Lo and Lai69,Reference Attar, Wester, Koul, Eggert, Polcwiartek and Jernberg72,Reference Toender, Vestergaard, Munk-Olsen, Larsen, Kristensen and Laursen73,Reference Scheuer, Kosjerina, Lindekilde, Pouwer, Carstensen and Jørgensen77,Reference Fransson, Werneke, Öhlund, Jonsson and Ott78 three reported the incidence of diabetic kidney disease among people with SMI and type 2 diabetes. Chan et al Reference Chan, Wong, Or, Chen and Chang75 found an incidence risk of 6.1% for diabetic kidney disease among people with schizophrenia, which was lower among people with diabetes who did not have schizophrenia (adjusted odds ratio 0.91, 95% CI 0.82–1.01). By contrast, Scheuer et al Reference Scheuer, Kosjerina, Lindekilde, Pouwer, Carstensen and Jørgensen77 found that people with SMI (either bipolar disorder or schizophrenia) had an incidence rate of 30.55 per 1000 person-years for diabetic kidney disease. The incidence rate ratio (IRR) was significantly higher compared with those without severe mental illness (IRR 1.15, 95% CI 1.12–1.18), even after adjusting for substance use and comorbidities (IRR 1.08, 95% CI 1.05–1.12).
The three remaining studies were excluded from the analysis because of methodological heterogeneity, which included reporting the incidence of kidney failure only among a cohort of people with SMI who already had CKD, Reference Presne, Fakhouri, Noël, Stengel, Even and Kreis71 reporting ratio comparisons that could not be pooled Reference Uju, Kanzaki, Yamasaki, Kondo, Nanasawa and Takeuchi74 and used hospitalisation episodes as the denominator (as opposed to the population sample size or person-years at risk). Reference Henriques, Ferreira, Gonçalves-Pinho, Freitas and Fernandes76
Quality of evidence: GRADE
We judged the overall quality of evidence available to be low. The risk of bias in individual studies was assessed as low, because most included studies were of high or moderate quality. However, our judgement was downgraded due to the indirectness of the evidence (with over half of the studies not having a primary aim to determine the prevalence or incidence of CKD in people with SMI); and also to the high level of heterogeneity in the included studies, the imprecision across confidence intervals of the included studies and the lack of representation of prevalence estimates from important settings (such as from low- and middle-income countries (LMICs)) and estimates according to specific factors including ethnicity, gender and antipsychotic medication prescriptions.
Discussion
This is the first systematic review to evaluate CKD prevalence, incidence and risk among people with SMI. We found that there was an 8% prevalence of CKD (all stages) in included studies, with the highest prevalence among populations with either a history of lithium exposure (29%) or a diagnosis of bipolar disorder (15%). The pooled incidence risk of CKD was 5%, and the pooled incidence rate was 26.8 per 1000 person-years.
The pooled prevalence of CKD in this meta-analysis is lower than that in meta-analyses of prevalence among the general population, where the estimated prevalence of CKD is approximately 10.8%. Reference Hill, Fatoba, Oke, Hirst, O’Callaghan and Lasserson79 In this review, the incidence risk is hard to compare because most studies report only the incidence risk as a proportion without contextualising it within a specific follow-up time; however, the pooled incidence rate of 26.8 per 1000 person-years is higher than findings from epidemiological studies conducted in the general population: for example, a study conducted in the Netherlands reported an incidence rate for CKD of approximately 12.13 per 1000 person-years. Reference van Blijderveen, Straus, Zietse, Stricker, Sturkenboom and Verhamme80
A further contrast to the lower pooled prevalence of CKD in comparison with the literature on the general population is that in studies where there were direct comparisons between the general population and people with SMI, the latter consistently had higher odds of CKD. The pooled odds ratio for CKD was 2.33 and, although this was highest in studies focused on populations with bipolar disorder and schizoaffective disorder (odds ratio 2.78), studies that focused only on people with schizophrenia also had significantly higher odds of CKD (odds ratio 1.98, 95% CI 1.56, 2.36). One reason for the comparatively low pooled prevalence estimate, but consistently higher odds and hazard, of CKD among people with SMI compared with the general population could be the method of identification of CKD. Most included studies relied on ICD diagnostic codes within population-level data (such as medical records and registries) to identify cases of CKD. Although this approach allows the collection of data from a representative sample over long periods of follow-up, it has been shown to underestimate the prevalence or incidence of CKD, Reference Ramagopalan, Leahy, Stamp and Sammon81,Reference Sundström, Bodegard, Bollmann, Vervloet, Mark and Karasik82 especially in underserved and marginalised groups who do not have opportunistic testing. It is therefore recommended that a combination of clinical values, such as eGFR calculations and albuminuria based on medical records, be used in conjunction with diagnostic codes to ensure a more accurate estimate of the prevalence or incidence of CKD at a population level. Reference Ramagopalan, Leahy, Stamp and Sammon81
The prevalence of CKD differed according to the staging of CKD, which could also reflect the methods of identification required for staging. In studies where the stage was not reported (typically population-level research using diagnostic codes) the pooled prevalence was 4%, whereas that for CKD stage 3 and above was 12%. This was also reflected in the pooled incidence risk, which for non-specified CKD was 3%, whereas for CKD stage 3 and above the incidence risk was 7%. CKD stage 3 and above has a lower prevalence and incidence than CKD of any stage in the general population, Reference Kovesdy12 probably due to better identification when staging CKD in epidemiological studies.
The higher odds of CKD among people with SMI compared with the general population probably resulted from a multitude of different factors. We found that the odds were highest among populations where mood stabilisers, such as lithium, would be indicated (for example, bipolar disorder and schizoaffective disorder). This is not surprising considering the established risk of lowered kidney function in long-term lithium treatment Reference Schoretsanitis, de Filippis, Brady, Homan, Suppes and Kane17 and the associated risk of AKI. Reference Grünfeld and Rossier19 Additionally, increased screening in that population may lead to increased detection of CKD, particularly in the earlier stages, which is underdiagnosed in the general population. Reference Iwagami, Mansfield, Hayes, Walters, Osborn and Smeeth41 Importantly, the higher odds remained in populations where patients may not be exposed to lithium, such as in schizophrenia. One study, conducted by Iwagami et al, Reference Iwagami, Mansfield, Hayes, Walters, Osborn and Smeeth41 highlighted that the relative increased prevalence of CKD among people with SMI compared with the general population remained even when patients with any history of lithium exposure were excluded. This provides evidence that other risk factors are contributing to this risk. Second-generation antipsychotics have been associated with an increased risk of CKD, Reference Højlund, Lund, Herping, Haastrup, Damkier and Henriksen83 while studies examining the relative risk of CKD across first- and second-generation antipsychotics identified combination treatment as being associated with the highest risk. Reference Wang, Huang, Feng and Tsuang84 Although there is a lack of research evaluating the contributory factors associated with CKD risk among people with SMI, some studies identified in the present review suggest that higher rates of conditions like diabetes are not solely responsible for this increase in CKD risk, with Scheuer et al finding a significantly higher rate of diabetic nephropathy even after adjusting for substance use and multimorbidities. Reference Scheuer, Kosjerina, Lindekilde, Pouwer, Carstensen and Jørgensen77 Therefore, further research is needed to understand the factors driving this increased risk, and to identify effective strategies for reducing it.
Despite this increased risk of CKD among people with SMI, there is evidence that people with SMI and CKD experience worse outcomes compared with those without SMI or in the general population. Reference Carswell, Cogley, Bramham, Chilcot, Noble and Siddiqi16 This includes higher mortality risk among people with SMI and kidney failure, Reference Kimmel, Fwu, Abbott, Moxey-Mims, Mendley and Norton85 limited access to specialist kidney care, Reference Hsu, Cheng, Ouyang, Lin, Huang and Hsu86 transplant assessment Reference Boyle, Fehr, Deering, Raza, Harhay and Malat87,Reference Bayat, Frimat, Thilly, Loos, Briançon and Kessler88 and kidney replacement therapies, Reference Tzur Bitan, Krieger, Berkovitch, Comaneshter and Cohen43 and higher rates of emergency hospitalisation. Reference McPherson, Barbosa-Leiker, Daratha, Short, McDonell and Alicic89 There is also evidence to suggest that people with SMI and CKD experience worse outcomes than those with SMI who do not have CKD, including associations between CKD and suicide risk. Reference Chen, Tsai, Pan, Chen, Chang and Su90,Reference Germack, Bizhanova and Roberts91
Strengths and limitations
There are several strengths and limitations in this review, as well as in the overall evidence base. There was a relatively small number of articles included in the meta-analyses, particularly for meaningful subgroup analysis. Therefore, the confidence intervals in the meta-analyses lacked precision, although we were able to demonstrate an increased risk of CKD across studies reporting relevant ratios. There was a lack of research conducted in LMICs, and most studies did not provide a breakdown of CKD prevalence, incidence or risk according to SMI diagnoses, antipsychotic medication, gender, age, body mass index or multimorbidities, limiting our ability to explore potential contributory factors to the risk of CKD. However, we were able to conduct subgroup analyses according to method of CKD identification, lithium exposure and staging of CKD, highlighting some potential limitations in the evidence base that can be addressed in future research. We were able to conduct separate meta-analyses to report prevalence, incidence risk and incidence rate, in addition to odds and hazard ratios, to provide a more comprehensive overview of the epidemiological literature on this relationship. Several pooled studies were conducted in the same country (for example, the UK), and the reliance on national data-sets may have resulted in overlapping samples that could have led to an inaccurate measure of precision for the pooled estimates.
This review was also focused specifically on studies that included people diagnosed with SMI. We did not include all studies that reported the risk of CKD among people receiving lithium treatment (if they did not report the diagnoses of included participants). Additionally, not all included studies consistently reported lithium exposure or provided a breakdown of CKD risk across lithium-exposure groups (although this was analysed when available). Therefore, the findings reported in this review may not accurately reflect the degree of risk associated with lithium exposure per se. Finally, the studies did not account for the impact of screening in prevalence estimates of CKD, which is particularly important in studies focused on people receiving lithium treatment, where regular screening of kidney function is part of the care pathway. Reference Schoretsanitis, de Filippis, Brady, Homan, Suppes and Kane17 Despite these limitations, this is the first systematic review to provide a pooled prevalence estimate of CKD among people with SMI.
Although the prevalence estimates in this review are lower than in the general population, meta-analyses of incidence rates, odds and hazard ratios demonstrate that people with SMI are at a significantly higher risk of CKD compared with those without SMI. Lithium is known to play a role in the increased risk among people with bipolar and schizoaffective disorders. The evidence for the relationship between CKD and SMI in general is limited and imprecise and, although psychiatric medication and high rates of type 2 diabetes may contribute to the risk, the drivers of this inequality are under-researched. Further research is needed to identify any potentially modifiable risk factors and establish the global prevalence and incidence of CKD in people with SMI.
Supplementary material
The supplementary material for this article is available online at https://doi.org/10.1192/bjp.2026.10659
Data availability
Data availability is not applicable because no new data were created or analysed in this study.
Acknowledgements
The authors thank all members of the study’s Patient and Public Involvement (PPI) panel who have provided guidance on the focus of this study. They also thank the librarians and Health Sciences subject area specialists at the University of York, who reviewed and provided guidance on the search strategies.
Author contributions
All authors have reviewed and revised the manuscript and given approval for the final version to be published. C.C., K.B., J.C., R.J., D.P.O. and N.S. contributed to the conception and design of the work. C.C., R.E.N., J.K., Z.P. and A.H. contributed to acquisition and analysis, including screening and data collection. All authors contributed to data interpretation.
Funding
This study was funded by an NIHR Advanced Fellowship (no. NIHR303182); overview of the award can be found here: https://fundingawards.nihr.ac.uk/award/NIHR303182. This funding is a personal Career Development Award received by C.C. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Declaration of interest
None.









 Open access
Open access
eLetters
No eLetters have been published for this article.