


Introduction
Advances in technology and medicine have led to an improvement in life expectancy, thus increasing the population of older individuals aged 50 years and older, including those within the criminal justice system.Reference Reynolds, Jeste, Sachdev and Blazer1 Understanding the unique attributes and needs of older adults involved in the criminal justice system is increasingly becoming important in forensic psychiatric contexts to ensure an accurate formulation of their needs or risk to public safety and develop effective management, albeit these needs can easily be overlooked.Reference Di Lorito, Dening and Völlm2-Reference Ferencz, Chaimowitz, Giroux, Hategan, Bourgeois, Hirsch and Giroux5 More often, patients in the forensic systems are treated and rehabilitated for a reasonable period to ensure that they are released at a point when their risk to the public is managed and are less likely to reoffend.Reference Kumar and Simpson3, Reference Ferencz, Chaimowitz, Giroux, Hategan, Bourgeois, Hirsch and Giroux5 While a considerable proportion of individuals in the criminal justice system in Ontario are older adults at the time of their index offense, over half of these older adults entered the correctional system at a younger age, especially before 50 years, and transitioned into older adults following a prolonged time in detention.Reference Iftene6 Such lengthy stays in the criminal justice system are often associated with noticeable changes in health and psychosocial status, including those that are due to aging.Reference Gosek, Kotowska, Rowińska-Garbień, Bartczak and Heitzman7, Reference Stoliker, Kerodal and Jewell8 For instance, older individuals within the forensic-correctional system are more likely to experience cognitive decline, mental health disorders, and complex medical conditions, all of which can heighten their needs and the unpredictability of their behavior.Reference Ferencz, Chaimowitz, Giroux, Hategan, Bourgeois, Hirsch and Giroux5, Reference Iftene6, Reference Stoliker, Kerodal and Jewell8, Reference Cipriani, Danti, Carlesi and Di Fiorino9 With age, there may be the cumulative effect of untreated psychiatric issues or a history of aggression, which, when coupled with conditions like dementia or mood disorders, can heighten the vulnerability to behavioral problems that are akin to poor judgment, erratic or even violent behaviors.Reference Ferencz, Chaimowitz, Giroux, Hategan, Bourgeois, Hirsch and Giroux5, Reference Cipriani, Danti, Carlesi and Di Fiorino9, Reference Maia, Ferreira and EMd10 Despite these risks, older individuals in the criminal justice system may not receive adequate attention in terms of their needs to address the potential risk for harmful behavior or re-offending, partly because aging is thought to reduce the likelihood of offending tendencies.Reference Cipriani, Danti, Carlesi and Di Fiorino9, Reference Maia, Ferreira and EMd10 However, their vulnerability, combined with a possible history of untreated or poorly managed psychiatric or medical conditions and other psychosocial life events, makes older adult forensic patients (OAFP) a population that requires specialized care, added support, and comprehensive risk mitigation strategies.Reference Jackson and Mallory4 This is partly supported by the level of recidivism associated with older populations, especially with over 50% of older individuals above 50 years in Ontario’s correctional system detained for re-offending.Reference Iftene6.
In the forensic psychiatric context, assessing the risk an individual poses to public safety is a key aspect of clinical practice that informs the decision process for disposition, community reintegration, risk mitigation strategy, and resource allocation to address psychosocial needs.Reference Ferencz, Chaimowitz, Giroux, Hategan, Bourgeois, Hirsch and Giroux5, Reference Rogers11, Reference Prins12 This risk assessment involves a detailed evaluation of clinical, behavioral, and criminal histories to formulate an individual’s risk profile, with the goal of identifying factors that predict a heightened risk or threat to public safety and what care plan is needed to mitigate risk.Reference Ferencz, Chaimowitz, Giroux, Hategan, Bourgeois, Hirsch and Giroux5, Reference Rogers11 Traditionally, factors such as psychiatric diagnoses, demographic characteristics, and previous risky behaviors are considered when evaluating potential threats to public safety and planning appropriate care.Reference Elbogen and Verykoukis13 However, certain characteristics, such as inpatient clinical status, younger age at first psychiatric admission, or previous history of violence, have been identified as particularly strong predictors of future risk and trajectory of their care.Reference Andreasson, Nyman and Krona14, Reference Hogan and Olver15
While the majority of research on risk assessment in forensic psychiatry has focused on younger populations, there is a growing recognition of the need to examine older adults more closely to help understand the complexity of their needs and inform nuanced approaches to their care.Reference Kumar and Simpson3, Reference Ferencz, Chaimowitz, Giroux, Hategan, Bourgeois, Hirsch and Giroux5, Reference Stoliker, Kerodal and Jewell8, Reference Nnatu, Mahomed and Shah16 With the trend in the aging of the world’s population, the burden of age-related mental and physical health issues (e.g., Alzheimer’s disease, neurodegenerative, dementia, delirium, and other organic mental disorders), and their associated behavioral and psychological problems (e.g., sexual disinhibition, frontal lobe syndrome, aggression, and agitation) among affected older adults is expected to rise.Reference Laidlaw and Pachana17-Reference Anderson and Hussey19 Taken together, the increasing burden of these age-related behavioral problems underscores the importance of understanding the needs of older adult offenders and what is needed to mitigate the risk posed to the affected individuals, their families, and public safety. While recognizing a scarcity of research on older forensic psychiatric populations, a better understanding of the unique challenges and needs associated with aging can promote accurate assessment, inform appropriate strategies, help clinicians to better manage any risk issues, and enhance community re-integration of OAFP.Reference Kumar and Simpson3 This study aims to address the gap in research by examining the predictors of change in public threat and risk among older individuals in forensic psychiatric care, providing insights that can inform the care of older adults, clinical practice, and public safety measures.
Methods
Study design
This is a retrospective study involving older individuals aged 55 years and older in the Ontario Review Board (ORB) database. All patients under the auspices of the ORB underwent forensic psychiatric assessments to support the legal determination of their forensic status. These patients are either inpatients or outpatients, depending on their disposition and clinical status. Annual progress is documented and presented to the ORB for each patient.Reference Chaimowitz, Moulden, Upfold, Mullally and Mamak20-Reference Kaggwa, Chaimowitz and Erb22
The database was created from the information curated from the annual ORB reports for the reporting years of 2014 and 2015. The data from this ORB database have been used and described in other published papers.Reference Chaimowitz, Moulden, Upfold, Mullally and Mamak20-Reference Kaggwa, Chaimowitz and Erb22 The current analysis only included older individuals whose risk profile for public safety was captured during the reporting years (2014/15) under reference and the previous year.
Study variables
Outcome variable
Change in Risk of Threat to the Public: This variable was determined by calculating the difference between the risk levels in the reference study years (2014 and 2015) and previous reporting years. This outcome is very crucial and fundamental to the core mandate of the forensic psychiatry system because according to Section 672.54 of the Criminal Code of Canada, an individual must pose a significant threat to the public to remain under the care of the forensic psychiatry system.23 A significant threat to public safety is defined as a risk of serious physical or psychological harm to members of the public, including any victim or witness of the offense, or any person under the age of 18, resulting from conduct that is criminal in nature but not necessarily violent.
Each year, the risk each patient poses to public safety is accessed and communicated in the ORB reports that are presented at the annual hearing of the ORB. Following an integrated multi-source comprehensive risk assessment, individuals in the forensic system are categorized and coded based on their risk profile as follows: None: Does not pose a significant risk to the public. Moderate: Poses a moderate threat to public safety High: Poses a significant threat to public safety.
In this study, we operationalized these different levels of risk with numerical values, such that those with no significant risk were coded as zero (0), one (1) for a moderate, and two (2) for a high significant risk for public safety. The difference between the risk levels in the reporting year under study and previous years was calculated to derive a continuous outcome variable labeled as the change in risk level for a threat to public safety. This variable can have positive or negative values, reflecting increases or decreases in risk levels. This change in risk level was used as the main outcome variable in the current study.
Model categories and variables
We considered six blocks of plausible variables within the dataset to explain the changes in the risk to public safety. These panels of risk factors are informed by factors considered essential in ORB reports, available literature regarding risk prediction, and input from clinicians with expertise in forensic psychiatry risk management.Reference Ferencz, Chaimowitz, Giroux, Hategan, Bourgeois, Hirsch and Giroux5, Reference Chaimowitz, Mamak, Moulden, Furimsky and Olagunju24-Reference Sedgwick, Young and Kumari26 These blocks included sociodemographic characteristics (Block 1), circumstances during the index offense-the crime or offense that led to their forensic status (Block 2), current clinical profile (Block 3), psychiatric history and behavioral patterns (Block 4), criminal history and legal status (Block 5), and recent violent events (Block 5).
Sociodemographic characteristics
This foundational block includes critical variables such as age, gender, employment status, level of education, and country of birth. These variables provide a baseline understanding of the individual’s background.
Circumstances during the index offense
This block captures the context of the index offense, including the age of the individual at the time of the offense, intoxication status (yes/no), the nature of the offense (violent, sexual, non-violent), victim characteristics (gender and age), the relationship to the victim (known/unknown), and the severity of injury inflicted (none, minor, hospitalization, death).
Current clinical profile
This block encompasses variables that reflect the individual’s current mental health status for the period under review (2014 and 2015), including primary diagnosis, presence of comorbid psychiatric conditions (yes/no), outpatient or inpatient status, length of stay within the forensic psychiatry system (in years), and capacity to consent to treatment (yes/no). Assessments included in the ORB reports were conducted by trained and certified forensic psychiatrists in Canada, and diagnoses were made according to the Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria. Additionally, a battery of psychological tools is administered by certified clinical psychologists to support diagnostic and capacity assessments.
Past psychiatric history and behavioral patterns
This block includes comprehensive variables such as age at first admission for mental health concerns, history of substance use, history of self-harming behaviors before the reporting year, previous instances of absconding, past risk behaviors (e.g., physical violence toward objects, people, inappropriate sexual behaviors), previous incapacity to consent to treatment, compliance with treatment, and historical response to treatment.
Criminal history and legal status
This block details the individual’s criminal background, including the number of previous convictions, history of absconding (yes/no), previous number of incarcerations, and current Ontario Review Board (ORB) status (not criminally responsible on account of mental illness [NCR] or unfit to stand trial [UST]).
Recent violent events
This final block assesses a recent involvement in a violent behavior/incident (as a perpetrator) or self-harm during the reporting year, including verbal aggression, harm to objects, harm to others, inappropriate sexual behaviors, and self-harm.
Data analysis
The data were analyzed using STATA version 17. Categorical variables were presented as frequencies and percentages, while the continuous variables (e.g., age during the reporting year, age at index offense, length of stay within the forensic system, among others) were described using either the mean and standard deviation (SD) or the median and interquartile range (IQR). Inferential statistics was assessed using analysis of variance (ANOVA) and student t-test. Changes in public threat risk were treated as a continuous variable. Hierarchical multivariate linear regression was conducted to identify predictors of increased or decreased public threat risk using the Stata command “nestreg, waldtable.” A significance level of less than 5% was considered for a 95% confidence interval.
Results
The study included 161 individuals aged 55 years and older who had information on previous and reporting years risk levels captured to allow an estimate of changes in risk levels. The median age of older participants in the forensic psychiatry program in Ontario during the reporting year was 61 years, with an interquartile range (IQR) of 58–67. Most individuals were between 55 and 65 years old (65.2%) and were predominantly males (81.4%, n = 131). The primary diagnosis for the majority was schizophrenia (68.3%) followed by bipolar disorder (9.3%) and 9.3% had a diagnosis of a neurocognitive disorder. None of the included individuals had a violent index offense. The majority (80.8%, n = 130) posed a highly significant threat to public safety during the reporting year (2014 and 2015), although this percentage was lower than the 87.5% reported in the previous year (see Table 1).
Distribution of Study Characteristics

Abbreviation: IQR, interquartile range; n, frequency; SD, standard deviation.
Changes in the risk of threat to the public
The change in the risk of threat to the public was assessed for 161 individuals who had information on their risk levels for the previous and reporting year assessed. Outpatient clinical status (p-value <0.001) and a lack of capacity to consent to treatment (p-value = 0.033) were significantly correlated with a decreased risk of threat to the public statistically (see Table 1).
Predictive models for factors associated with change in risk to public safety
Table 2 presents a multiple hierarchical linear regression analysis with six models predicting the changes in the risk of posing a significant threat to public safety among 161 individuals with data on previous and current risks during the period under study.
Predictive Models of Increase in Risk of Threat to Public
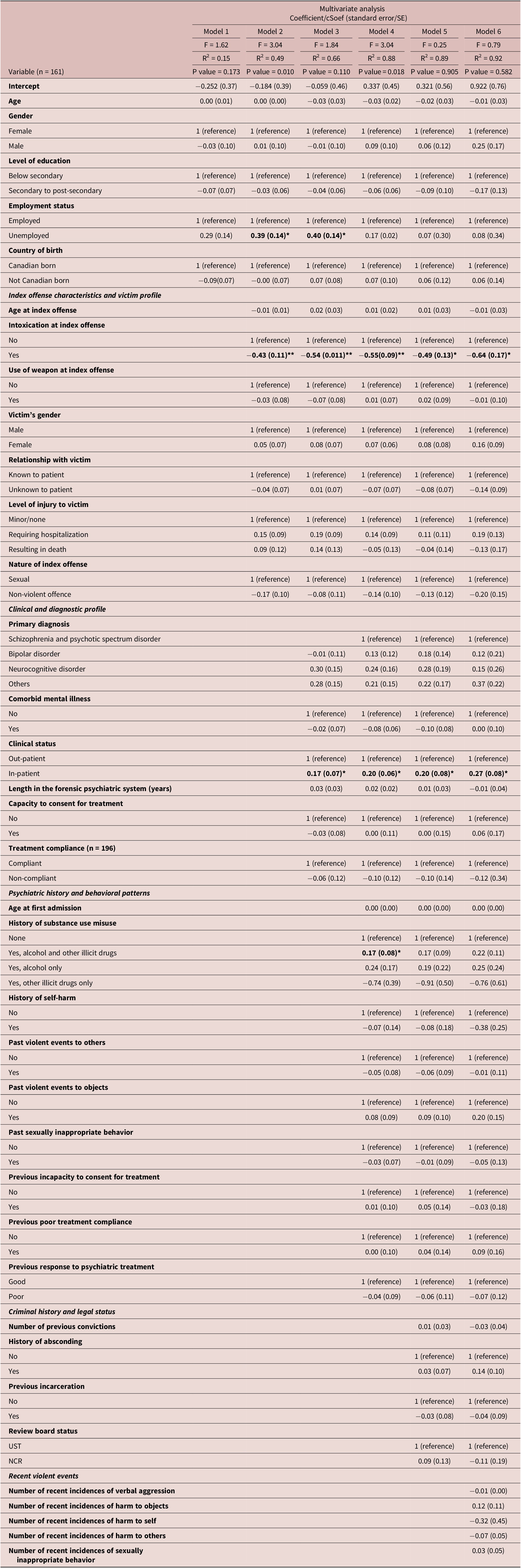
* - p-value < 0.05. ** - p-value < 0.001.
Model 1 included variables from Block 1 and accounted for 15% of the variance in change in risk to public safety (RReference Di Lorito, Dening and Völlm2 = 0.15, p = 0.173). None of these variables showed a statistically significant relationship with changes in risk.
Model 2 incorporated Block 2 variables, increasing the explained variance by 34% (RReference Di Lorito, Dening and Völlm2 = 0.49, p = 0.010). Significant predictors in this model included unemployment (adjusted coefficient [acoef] = 0.39, SE = 0.14, p = 0.008) and intoxication at the time of index offense (acoef = −0.54, SE = 0.11, p < 0.001).
Model 3 added Block 3 variables to Model 2, further increasing the explained variance to 66% (RReference Di Lorito, Dening and Völlm2 = 0.67, p = 0.144). Significant predictors remained similar to Model 2, including intoxication during the index offense (acoef = −0.51, SE = 0.10, p < 0.001) and unemployment (acoef = 0.42, SE = 0.14, p = 0.06). However, only inpatient status (acoef = 0.17, SE = 0.07, p = 0.027) was significantly associated with changes in risk level for public threat among the added variables.
Model 4, which included Block 4 variables, increased the explained variance by an additional 22% (RReference Di Lorito, Dening and Völlm2 = 0.88, p = 0.018). Unemployment was no longer a significant predictor, but a history of abuse of both alcohol and other illicit drugs (acoef = 0.17, SE = 0.08, p = 0.048) was the only significant variable among the added items. Intoxication at the index offense continued to significantly reduce risk (acoef = −0.55, SE = 0.09, p < 0.001), while inpatient status increased risk (acoef = 0.20, SE = 0.06, p = 0.003).
Adding criminal history and legal status variables (Block 5) to Model 4 resulted in a model that accounted for 89% of the variance (RReference Di Lorito, Dening and Völlm2 = 0.89, p = 0.905) in the prediction of change in risk to the public. Intoxication at the index offense remained a significant predictor of lower risk (acoef = −0.49, SE = 0.13, p = 0.003), and inpatient status continued to increase the risk (acoef = 0.20, SE = 0.07, p = 0.010). However, the use of both alcohol and other illicit drugs was no longer significant.
In the final model (Model 6), the addition of Block 6 variables (i.e., recent violent events such as verbal aggression, harm to objects, self, others, and sexually inappropriate behavior) explained an additional 3% of the variance, making the final model account for 92% of the variance in changes in risk (RReference Di Lorito, Dening and Völlm2 = 0.92, p = 0.581). Significant predictors remained similar to Model 5, with intoxication at the index offense (acoef = −0.63, SE = 0.17, p = 0.005) and inpatient status (acoef = 0.27, SE = 0.08, p = 0.010) being key factors.
Overall, Models 2 and 4 were statistically significant predictors, while Model 6 explained the most variance in public threat risk (RReference Di Lorito, Dening and Völlm2 = 0.92). Intercept values increased from −0.252 in Model 1 to 0.922 in Model 6, suggesting the inclusion of impactful variables in the later models.
Discussion
The present study investigates the changes in the reported level of risk to public safety among older individuals aged 55 years and older within the forensic psychiatry system in Ontario, Canada. The study first investigated the correlation of change in risk levels for a threat to public safety by comparing the past year to the reporting year (2014 and 2015) captured in the ORB database. The results from the present study indicate that certain factors are significantly correlated with a decreased risk of posing a significant threat to public safety. These include being an outpatient and having the capacity to consent to treatment. Individuals receiving outpatient psychiatric care are less likely to pose a high threat to public safety, which is a threshold often required for a disposition with community access and a care plan for community re-integration. This may be attributed to better-controlled mental health conditions and having been tested in the community, and they are maintained with sustained access to community resources. The capacity to consent to treatment is an indicator of an individual’s insight into their illness, and those who are deemed treatment-capable have potentially demonstrated a higher degree of insight and meet the threshold to be independent in treatment decision-making.Reference Grover, Tekkalaki, Yadawad, Patil, Chate and Patil27 In contrast to this finding, those with no capacity to consent to treatment were also associated with a reduction in the risk posed to public safety, possibly due to the effective use of substitute decision-maker programs in maintaining treatment adherence to achieve recovery.
Secondarily, this study utilized a hierarchical regression model to analyze the factors explaining variations in risk tendencies among OAFP. Of the six models included, only Models 2 and 4, which incorporated the characteristics of the index offense with victim characteristics and past psychiatric history with behavioral patterns, respectively, were statistically significant. Model 2 explained the highest variability at 34%, underscoring the importance of circumstances during the index offense in determining risk level. This finding is particularly intriguing as it suggests that the context of the index offense plays a crucial role in future risk assessment and formulation of care plans. Conventionally, individuals in the forensic psychiatric system are rehabilitated and managed based on their current mental status to achieve well-being and mitigate any threat posed to public safety. However, the forensic system still mirrors several aspects of the prison-correctional system, where rehabilitation is influenced by the circumstances surrounding the index offense. This approach may not fully align with recent principles of psychiatric rehabilitation, which emphasize the importance of dynamic individualized treatment plans based on current mental health status and needs.Reference Llewellyn-Beardsley, Rennick-Egglestone and Callard28, Reference Anthony29 The significant contribution of past psychiatric-related items and historical criminogenic attributes (Block 4) to the variance in risk (second largest explanation at 22%) highlights the forensic system’s over-reliance on historical factors in predicting risk levels and care plans among older individuals. This reliance raises important questions about the actual importance of these historical clinical factors and the circumstances during the index offense in risk prediction. Our study findings suggest a need for large follow-up studies to determine the relevance or weight of these factors (which are largely static or non-modifiable) in the rehabilitation and planning of care of OAFP. Moreover, elements of potential assessors’ bias in risk assessment need to be critically evaluated. Ensuring that risk judgments are based on dynamic and current items rather than a predominance of historical or contextual factors is crucial for fair and effective rehabilitation.Reference Penney, Marshall and Simpson30-Reference Heffernan and Ward32 The integration of dynamic, protective, and modifiable factors into the formulation of risk, disposition, care planning, and management of OAFP aligns with recent gains in traction for nuanced approaches to effective risk management and patient-center care.Reference Chaimowitz, Mamak, Moulden, Furimsky and Olagunju24
Among the predictors in Model 2, the most prominent risk factor for increasing the risk to public safety was unemployed status during the reporting year, a factor that remained significant even in Model 3, but this was not the case when other Blocks were added. Employment has long been recognized as a major protective factor against violence and other risks in the criminal justice system.Reference Takeda, Sugawara and Yamada33 However, the significance of this factor in older individuals raises concerns about its predictive validity, although the age distribution of the population analyzed in this study needs to be considered. Since older individuals are often close to retirement age or may be unable to function as effectively as younger individuals in the workforce. Many forensic patients, especially older adults have physical health morbidities, and limited education, often not exceeding post-secondary levels, which further complicates their ability to engage in common forms of employment available to those involved in the criminal justice system.Reference Kaggwa, Chaimowitz and Erb22 Also, getting employment is harder for individuals with a criminal record, especially for those who commit serious offenses.Reference Takeda, Sugawara and Yamada33 Since gaining meaningful employment, a known protective factor in younger populations, is harder for this group, there is a need for age-appropriate risk prediction factors that do not focus on employment as a contributing factor. Conversely, those who were intoxicated during their index offense had their risk level predicted as reduced, a factor that remained significant even after adding other predictors). This finding may reflect the effectiveness of forensic programs in managing substance use problems, thereby reducing the associated risks among OAFP. Substance use treatment programs within forensic settings have shown positive outcomes in reducing recidivism and the risk of substance misuse post-release.Reference Doyle, Shakeshaft, Guthrie, Snijder and Butler34, Reference Olagunju, Li, Oliveira-Picado, Sheridan, Chaimowitz and Siglag35 Interestingly, using both alcohol and other illicit drugs was significant only in Model 4. This may be due to the heightened risk of violence and impulsive activities associated with the use of both addictive substances.
Being an inpatient was significantly associated with a change in risk level following introduction to Model 3 and subsequent models, signifying the key role it plays in predicting change in risk posed by OAFP and their care plan for rehabilitation. The inpatient status may allude to the severity of the mental health conditions in the affected OAFP, warranting hospital admissions and deterring transition or discharge into the community during the period under review. More often, inpatients require intensive treatment to improve their mental health wellbeing and monitoring to mitigate risk. Additionally, inpatients are often predicted to be of higher risk to the public compared with outpatients, and thus, may not have ORB dispositions that allow community living or a change to outpatient status, reinforcing the strong and persistent relationship.Reference Simpson, Boldt and Penney36, 37
Limitations
Despite being one of the largest studies involving OAFP and the final study model achieving a high explanatory power (92%), the limited sample size is a shortcoming in this study. Additionally, the retrospective study design resulted in multiple missing values across various variables. Also, there is limited information on the inter-rater reliability or criterion validity of the risk classification used (e.g., low–moderate–high). Finally, the cross-sectional nature of the data limits the ability to draw causal conclusions. Therefore, future longitudinal studies with robust sample sizes are warranted to better understand the predictive nature of the various factors and blocks on changes in risk levels among older adults. Moreover, future research needs to capture inter-rater reliability or criterion validity of risk classification.
Conclusion and implications
This study model demonstrated a robust explanatory effect size in accounting for the variability in the changes reported in the risk profile of OAFP. It identified supervised care, inpatient status, and intoxication at the time of index offense as critical proxy factors that correlate with the degree of risk to public safety attributed to patients and the determinants of the type of care implemented. These findings highlight the need for resources, policies, and supported care, including inpatient services to manage behavioral issues and support OAFP. Furthermore, the study emphasized the significant influence of historical factors, particularly the circumstances surrounding the index offense and past psychiatric history, in the prediction of future safety concerns and the care plan of OAFP. Implicitly, these findings underscore the need for innovative practices to promote age-appropriate risk assessment and the development of rehabilitation strategies that incorporate dynamic and protective factors. Effective management of OAFP requires interventions tailored to the unique needs and capabilities of individual patients. Future research should focus on developing and validating risk prediction and care planning models for OAFP taking into consideration individual patients’ specific circumstances, dynamic factors, and the need for optimal risk management and care plan strategies. It is also imperative that the reliance of risk formulation and care planning on historical factors among OAFP needs to pave the way for innovative risk management and care models. Such models should involve a better integration of dynamic and protective factors.
Data availability statement
Due to the sensitivity of the population being explored, the datasets will be made available to appropriate academic parties on request from the corresponding author after approval by GAC.
Acknowledgments
The team appreciates the efforts of the Forensic Psychiatry Research Institute of McMaster University/St. Joseph’s Healthcare Hamilton and the Ontario Review Board.
Author contribution
MMK and ATO were involved in conceptualizing the research idea. GAC was vital in the data collection process. MMK, JA, and ATO were involved in the data analysis process. MMK and JA drafted the initial manuscript and GAC, AD, JMWB, AL, RFM, PA, and ATO provided substantial intellectual contribution in the subsequent revisions. ATO and MMK supervised the various stages involved in this current manuscript writing. ATO, JA, AD, and MMK were involved in the visualization of the current manuscript. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Financial support
This work received no funding.
Competing interests
The authors do not have anything to disclose.
Ethical approval and consent
The data used in the present study was collected in accordance with the Declaration of Helsinki. Data collection commenced following approval by the Hamilton Integrated Research Ethics Board (HiREB), reference number #15564. HiREB waived the need for informed consent since the study involved de-identified retrospective data and individual consent could not practically be fully obtained.
Data statement
The data has not been previously presented orally or by poster at scientific meetings.



 Open access
Open access