

Twin-to-twin transfusion syndrome (TTTS) is one of the most critical and life-threatening conditions in fetal medicine and poses a significant challenge for obstetricians and neonatologists worldwide (Glennon et al., Reference Glennon, Shemer, Palma-Dias and Umstad2016; Spruijt et al., Reference Spruijt, Lopriore, J. Steggerda, Slaghekke and Van Klink2020). TTTS complicates approximately 5–15% of monochorionic twin pregnancies and, if left untreated, results in a perinatal mortality rate as high as 90% (Duncan et al., Reference Duncan, Denbow and Fisk1997; Urig et al., Reference Urig, Clewell and Elliot1990). This syndrome arises from vascular connections between the twins in the monochorionic placenta, leading to an imbalance in blood flow between the fetuses, which results in an aberrant intravascular volume status along with compensatory physiological responses in both twins. In the recipient twin, the atrial natriuretic peptide and brain natriuretic peptide are released, due to the rise of cardiac preload from the increased venous return. These hormones facilitate diuresis, which leads to polyhydramnios; whereas the donor develops hypovolemia, resulting in reduced urine production and subsequent oligohydramnios. Additionally, the monochorionic twins can also experience twin anemia-polycythemia sequence (TAPS), marked by red blood cell transfusion causing one fetus (the donor) to develop anemia and a lack of amniotic fluid, while the other (the recipient) experiences polycythemia and excess amniotic fluid (Ling et al., Reference Ling, Phelps, Tate, Adefisoye, Mehra and Prazad2023; Miller, Reference Miller2021). These hemodynamic disturbances in utero significantly increase the risk of brain injury, fetal death, congenital heart disease, premature delivery, intraventricular hemorrhage (IVH), kidney failure, hydrops fetalis, and polycythemia hyperviscosity syndrome in the recipient, and anemia in the donor. Additionally, TTTS can lead to long-term neurodevelopmental impairments, profoundly affecting infants’ quality of life (Cho et al., Reference Cho, Shin, Jun, Shin, Kim, Kim, Kim and Kim2019; Gijtenbeek et al., Reference Gijtenbeek, Haak, Huberts, Middeldorp, Klumper, Slaghekke, Lopriore, Oepkes and Van Klink2020; Ling et al., Reference Ling, Phelps, Tate, Adefisoye, Mehra and Prazad2023; Miller, Reference Miller2021; Spruijt et al., Reference Spruijt, Lopriore, J. Steggerda, Slaghekke and Van Klink2020).
Fetoscopic laser ablation (FLA) is currently the gold-standard treatment for advanced-stage TTTS (Quintero stage ≥ 2) (Society for Maternal-Fetal Medicine [SMFM] & Simpson, Reference Simpson2013; Spruijt et al., Reference Spruijt, Lopriore, J. Steggerda, Slaghekke and Van Klink2020) The primary objective of laser ablation is to divide the placenta effectively into two separate areas, with each area supporting one twin (SMFM & Simpson, Reference Simpson2013). While complications such as fetal demise and preterm prelabor rupture of membranes (PPROM) remain concerns after the procedure (Yamamoto et al., Reference Yamamoto, El Murr, Robyr, Leleu, Takahashi and Ville2005), survival outcomes have improved significantly over the past 25 years. Reports indicate that the survival rate of both twins has increased from 31% (1990–1995) to 62% (2011–2014), whereas the probability that at least one twin survives has increased from 70% to 88% (Akkermans et al., Reference Akkermans, Peeters, Klumper, Lopriore, Middeldorp and Oepkes2015; Spruijt et al., Reference Spruijt, Lopriore, J. Steggerda, Slaghekke and Van Klink2020). This study aimed to evaluate fetal survival and neonatal outcomes following fetoscopic laser ablation for TTTS.
Methods
This retrospective cross-sectional study included all twin and triplet pregnancies that received fetoscopic laser ablation for TTTS from January 2016 to January 2025 at Harapan Kita Women and Children Hospital, a national center of Women and Children’s Health in Indonesia. The exclusion criteria were patients whose Quintero stage was not documented and patients with a twin reversed arterial perfusion (TRAP) sequence without TTTS who received fetoscopic laser ablation.
Maternal and neonatal clinical characteristics were collected from electronic medical records and charts and from the neonatal registry at the neonatal intensive care unit (NICU). Information from maternal patients and their newborns born at external facilities was limited to the records found and was gathered by contacting maternal contacts. Fetal survival after the procedure was determined as survival for at least 48 hours postprocedure. Neonatal outcomes were assessed at birth and 28 days postpartum. The diagnosis of TTTS requires two criteria: pregnancy being monochorionic diamniotic (MCDA) and an imbalance in amniotic fluid levels, with one sac exhibiting oligohydramnios (a maximal vertical pocket [MVP] of ≤2 cm) and the other exhibiting polyhydramnios (MVP of ≥8 cm; Magann et al., Reference Magann, Doherty, Ennen, Chauhan, Shields, Gjesdal and Morrison2007). TTTS Quintero staging is classified on the basis of ultrasound parameters: Stage 1 is defined by an amniotic fluid discordance with MVP <2 cm in the donor sac and >8 cm in the recipient sac; Stage 2 involves the absence of the donor twin’s bladder on ultrasound for ≥60 minutes; Stage 3 is identified by abnormal Doppler findings, and Stage 4 indicated fetal hydrop (Quintero et al., Reference Quintero, Morales, Allen, Bornick, Johnson and Kruger1999)
Protocol of FLA in our unit consist of three operators, all qualified as Maternal Fetal Medicine (MFM) subspecialists, who have completed formal training in invasive fetal procedures. Pre-operatively, an ultrasound (USG) examination was performed to evaluate fetal viability, the location of placental vascular anastomoses, and assess the appropriate insertion point of the fetoscope. Spinal anesthesia was used in all patients. Intra-operatively, the technique used was Solomon approach for placental anastomosis coagulation. Postoperative fetal monitoring and outcome assessment were performed through USG.
Preterm premature rupture of the membrane (PPROM) was defined as the rupture of membranes with amniotic fluid leakage occurring before 37 weeks of gestation (Siegler et al., Reference Siegler, Weiner and Solt2020). Fetal growth restriction (FGR) is diagnosed when one fetus has an estimated fetal weight (EFW) <3rd percentile. In monochorionic twin pregnancies, FGR can also be identified if at least two of the following conditions are met: EFW <10th percentile in one fetus, abdominal circumference <10th percentile in one fetus, EFW discordance is 25% or more, and umbilical artey UA pulsality index of the smaller fetus >95th percentile (Khalil et al., Reference Khalil, Beune, Hecher, Wynia, Ganzevoort, Reed, Lewi, Oepkes, Gratacos, Thilaganathan and Gordijn2019). Initial cranial USG screening was performed in all TTTS infants born at < 37 weeks, between 3−5 days after birth, and follow-up during the second week of life. Compared with their peers in the same group, delayed milestones determine whether they fail to meet developmental milestones based on Denver II instruments, which are assessed by trained pediatric rehabilitation physicians during follow-up visits offered to all infants with neonatal complications, particularly those with abnormal cranial USG findings (Frankenburg & Dodds, Reference Frankenburg and Dodds1967).
The Mann‒Whitney U test was used to evaluate continuous variables and are presented as the means with standard deviations. Categorical variables were assessed using the chi-square test, and Fisher’s exact test was applied when more than 20% of the cells were expected to have frequencies of less than 5. Statistical significance was defined as a p value less than .05. IBM Statistical Package for Social Sciences (SPSS) software version 26 (IBM Corp., Armonk, NY, US) was used for data entry and statistical analysis.
This study received ethical approval from Harapan Kita Women and Children Hospital (approval number IRB/12/02/ETIK/2025). Consent requirements were waived, as the study involved secondary data usage. For infants delivered outside our hospital, neonatal survival status was confirmed by contacting the mothers. During these calls, the purpose of the study was explained and verbal informed consent for using the infant’s outcome data was obtained with the approved study protocol and institutional ethical guidelines.
Results
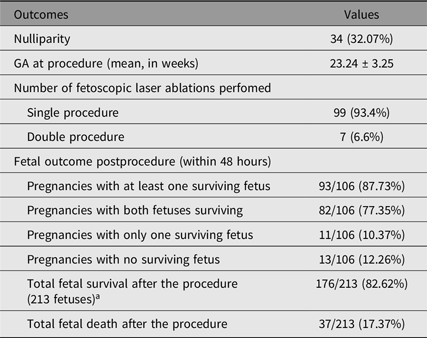
As show in the flowchart (Figure 1), a total 114 pregnancies were retrieved from the medical records. Of those, 8 were excluded because they were classified as Quintero stage 5 or had no documented Quintero staging, yielding 106 pregnancies that underwent FLA. Fetal outcomes of 106 TTTS patients following FLA are presented in Table 1. A total of 213 fetuses were identified from 106 pregnancies, including one triplet gestations. The mean gestational age (GA) at the time of the procedure was 23.24 ± 3.25 weeks. Among these patients, 34 (32.07%) were nulliparous. The majority of procedures were performed as a single intervention (99 cases, 93.4%), whereas a small subset required a double procedure (7 cases, 6.6%). Among the 106 pregnancies, 93 (87.73%) had at least one surviving fetus; 82 (77.35%) had both fetuses survive, whereas 11 (10.37%) had only one survivor. Thirteen pregnancies (12.26%) had no surviving fetuses. Among the 82 cases in which both fetuses survived, one fetus experienced IUFD after a second fetoscopic procedure. The total number of surviving fetuses after the procedure was 176 out of 213 (82.62%). Complications and maternal factors for each pregnancy following FLA are presented in Table 2. The incidence of PPROM is more frequent in pregnancies with double fetal death compared with at least one fetal survival.
Flowchart of fetal inclusion, fetal survival, and 28-day neonatal outcomes following FLA for TTTS.

Figure 1. Long description
The flowchart begins with 114 pregnancies identified between January 2016 and January 2025. Eight pregnancies are excluded due to Quintero stage V and no documented Quintero staging, leaving 106 pregnancies undergoing fetal laser ablation, including one triplet pregnancy with 213 fetuses. The flowchart then branches into three outcomes: both fetuses survived in 82 pregnancies (77.35%), single fetal survival in 11 pregnancies (11.38%), and double fetal death in 13 pregnancies (12.26%). The fetuses surviving to birth total 112. The next step evaluates the 28-day neonatal survival outcome, where 70 fetuses (62.5%) survived at 28 days and 42 fetuses (37.5%) did not. For the survivors, long-term neurodevelopmental follow-up is available for 8 infants, with delayed milestones identified using Denver II in 2 infants.
Fetal outcomes of 106 TTTS patients following fetoscopic laser ablation

Table 1. Long description
The table presents fetal outcomes for 106 TTTS patients after fetoscopic laser ablation. It includes data on nulliparity, gestational age at procedure, number of procedures performed, fetal outcomes post-procedure, and survival rates. The table has 11 rows and 2 columns. Key data points include 34 nulliparous patients, a mean gestational age of 23.24 weeks, 99 single procedures, and 7 double procedures. Post-procedure outcomes show 87.73% of pregnancies with at least one surviving fetus, 77.35% with both fetuses surviving, and 12.26% with no surviving fetuses. Total fetal survival after the procedure is 82.62%, with 17.37% fetal death.
Note: GA, gestational age. a106 pregnancies (1 triplet; 213 fetuses) underwent ablation procedures.
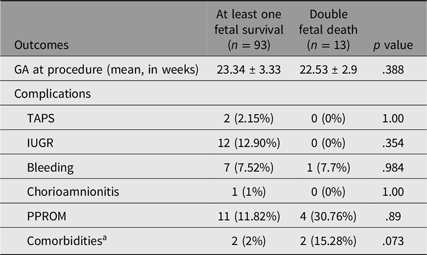
Complications and maternal factors for each pregnancy based on fetal survival within 48 hours after the procedure (106 pregnancies)
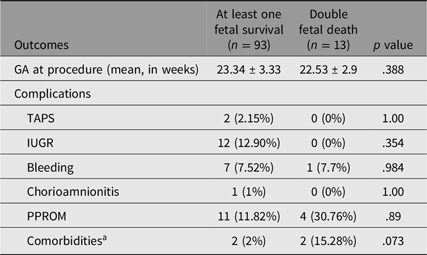
Table 2. Long description
A table with four rows and six columns compares complications and maternal factors for pregnancies based on fetal survival after FLA procedure. The columns are labeled Outcomes, At least one fetal survival (n = 93), Double fetal death (n = 13), and p value. The rows include GA at procedure (mean, in weeks), Complications, TAPS, IUGR, Bleeding, Chorioamnionitis, PPROM, and Comorbidities. The table shows mean gestational age, percentages of complications, and p values for each category. Notable trends include higher percentages of chorioamnionitis and PPROM in pregnancies with double fetal death compared to those with at least one fetal survival.
Note: GA, gestational age; TAPS, twin anemia-polycythemia sequence; IUGR, intrauterine growth restriction; PPROM, preterm premature rupture of membranes.
a Comorbidities, such as pulmonary embolism, herpes simplex, and anemia, in 2 cases of double fetal death.
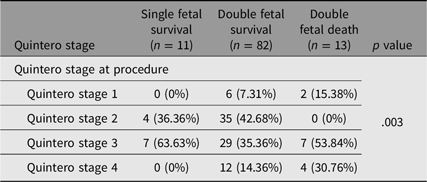
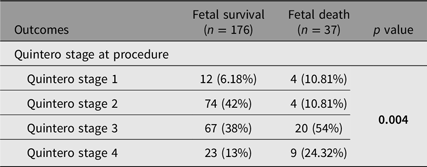
Analysis of the Quintero stage at the time of the procedure and fetal survival per pregnancy revealed a significant relationship with fetal survival (p = .003) as presented in Table 3. Among pregnancies with at least one surviving fetus, the highest proportion of double fetal survival was observed in Quintero stage 2 pregnancies (35 cases, 42.68%). In contrast, double fetal death was most frequently observed in Quintero stage 3 (7 cases, 53.84%) and Quintero stage 4 (4 cases, 30.76%) patients. Additionally, the Quintero stage and total fetal survival also demonstrated a significant relationship (p =.004), shown in Table 4, with 74 of 176 surviving fetuses classified under stage 2 (42%), while the highest proportion of fetal deaths occurred in stage 3 (54%).
Quintero stage for each pregnancy on the basis of fetal survival within 48 hours after the procedure (106 pregnancies)
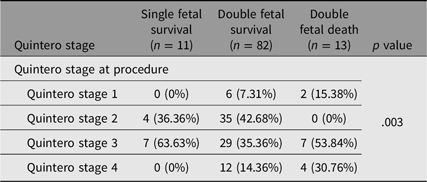
Table 3. Long description
The table presents data on the relationship between Quintero stage at the time of the procedure and fetal survival per pregnancy. It includes columns for Quintero stage, single fetal survival, double fetal survival, double fetal death, and p value. The table has five rows corresponding to different Quintero stages and a total of five columns. Among pregnancies with at least one surviving fetus, the highest proportion of double fetal survival was observed in Quintero stage 2 pregnancies with 35 cases representing 42.68%. In contrast, double fetal death was most frequently observed in Quintero stage 3 with 7 cases representing 53.84% and Quintero stage 4 with 4 cases representing 30.76%. The p value for the relationship between Quintero stage and fetal survival is 0.003, indicating a significant relationship. Additionally, the Quintero stage and total fetal survival also demonstrated a significant relationship with a p value of .004, with 74 of 176 surviving fetuses classified under stage 2 representing 42%, while the highest proportion of fetal deaths occurred in stage 3 representing 54%.
Quintero stage based on the overall fetal survival rate within 48 hours after the procedure (213 fetuses)
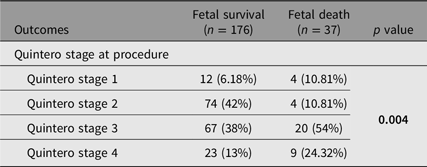
Table 4. Long description
The table presents data on fetal survival and fetal death rates across different Quintero stages. It includes four rows and five columns. The columns are labeled Outcomes, Fetal survival (n = 176), Fetal death (n = 37), and p value. The rows are labeled Quintero stage at procedure, Quintero stage 1, Quintero stage 2, Quintero stage 3, and Quintero stage 4. The data shows the number and percentage of fetal survival and fetal death for each Quintero stage. Notably, Quintero stage 2 has the highest fetal survival rate at 42%, while Quintero stage 3 has the highest fetal death rate at 54%. The p value indicates a significant relationship between Quintero stage and fetal survival.
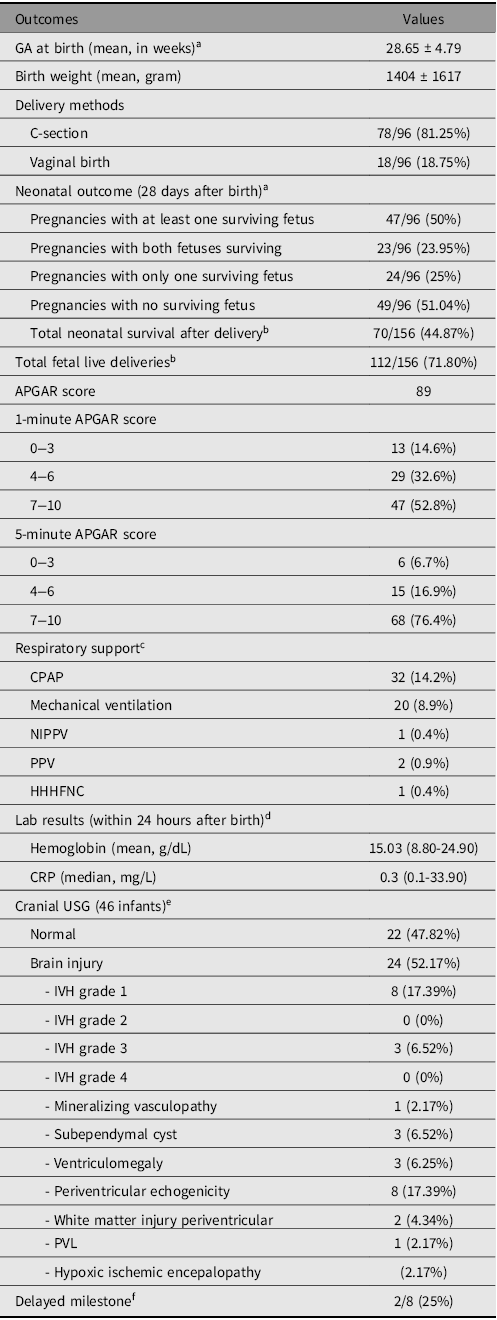
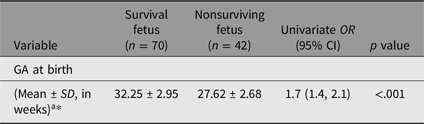
Among the 176 fetuses that survived after the procedure, 20 fetuses were excluded due to delivery at an outside facility or the pregnancy was ongoing, leaving 156 fetuses. Out of 156 fetuses, 112 fetuses survived to birth and 44 did not. Among the 112 fetuses followed to delivery, the mean GA at birth was 28.65 ± 4.79 weeks (see Table 5 ). Neonates who survived at 28 days were delivered at a significantly higher mean GA than those who did not survive (32.25 ± 2.95 vs. 27.62 ± 2.68 weeks, p < .001; OR 1.70, 95% CI [1.40, 2.10]; see Table 6. The overall rate of live births was 112 out of 156 neonates (71.80%). With respect to delivery methods, the majority of cases were delivered via the C-section (78 out of 96 pregnancies, 81.25%), whereas 18 out of 96 pregnancies (18.75%) were delivered vaginally. The mean birth weight was 1402 ± 1617 grams. At 28 days postbirth, at least one neonate survived in 47 out of 96 pregnancies (50%). Among these, both twins survived in 23 pregnancies (23.95%), whereas 24 cases (25%) resulted in only one surviving neonate. A total of 49 pregnancies (51.04%) resulted in neonatal death of both fetuses. Among the 112 live-born infants, 70 survived through 28 days of life and 42 did not survive to 28 days, resulting in an overall 28-day neonatal survival rate 70 out of 112 live-born infants (62.5%) and 70 out of 156 procedure-surviving fetuses (44.87%). Apgar scores were available for 93 neonates. Some neonates were born outside the facility, and their survival was confirmed through phone interviews with mothers, but Apgar scores were not recorded.
Neonatal outcomes of 96 TTTS patients following fetoscopic laser ablation (at delivery and 28 days postbirth)\
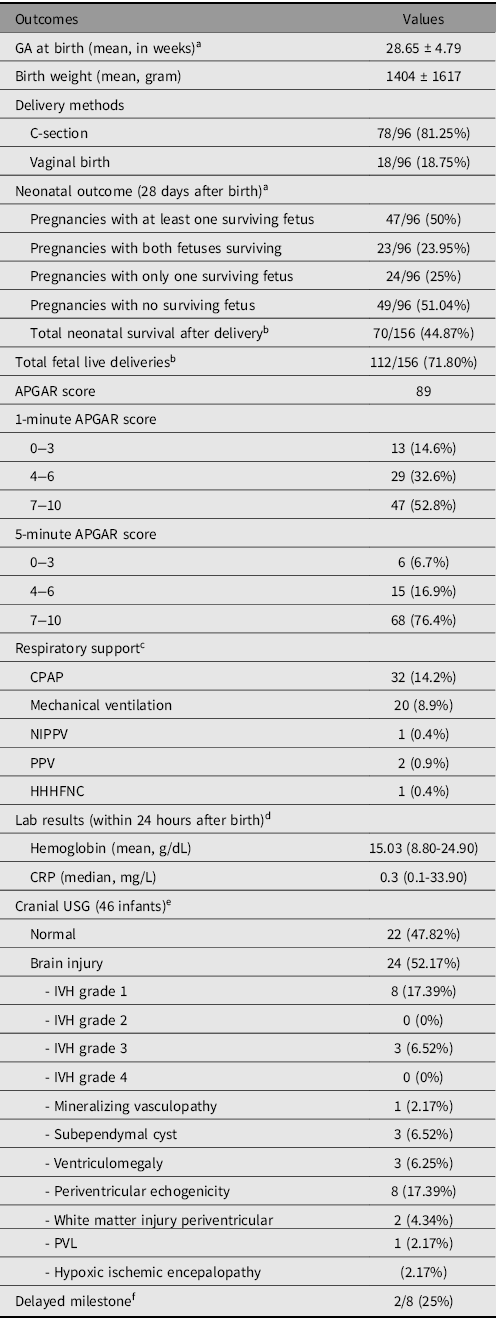
Table 5. Long description
The table presents data on neonatal outcomes for 96 TTTS patients who underwent fetoscopic laser ablation. It includes details such as gestational age at birth, birth weight, delivery methods, and survival rates at 28 days postbirth. Key data points include a mean gestational age at birth of 28.65 weeks, a mean birth weight of 1402 grams, and a 71.80% overall live birth rate. The majority of deliveries were via C-section (81.25%), with a 28-day neonatal survival rate of 62.5%. The table also provides APGAR scores and details on respiratory support and cranial ultrasound results.
Note: CPAP, continuous positive airway pressure; NIPPV, noninvasive positive pressure ventilation; PPV, positive pressure ventilation; HHHFNC, humidified high-flow nasal cannula; CRP, C-reactive protein; USG, ultrasonography; IVH, intraventricular hemorrhage; PVL, periventricular leukomalacia.
a Among 106 cases, 10 cases were excluded due to delivery at an outside facility, loss to follow-up, or ongoing pregnancy.
b Among 176 fetuses that survived after the procedure, 20 fetuses were excluded due to delivery at an outside facility, loss to follow-up, or ongoing pregnancy.
c Not all neonates have complete documentation of respiratory support methods.
d Not all neonates have hematological labs obtained upon delivery.
e Each infant may have multiple findings.
f Data based on infants with available long-term follow-up; most data were unavailable owing to retrospective data, incomplete documentation, and lack of routine follow-up by parents.
Gestational age at birth in surviving versus nonsurviving neonates at 28 days

Table 6. Long description
The table presents data on gestational age at birth for surviving and nonsurviving neonates at 28 days. It includes four columns: Variable, Survival fetus, Nonsurviving fetus, and Univariate OR with p value. The table has two rows of data. The first row shows the gestational age at birth with a mean of 32.25 weeks and a standard deviation of 2.95 weeks for surviving fetuses, and a mean of 27.62 weeks and a standard deviation of 2.68 weeks for nonsurviving fetuses. The univariate odds ratio is 1.7 with a 95% confidence interval of 1.4 to 2.1, and a p value of less than 0.001.
Note: GA, gestational age.
a Neonatal outcomes were analyzed among 156 fetuses alive 2 days post-fetoscopy. Of these, 112 survived to birth and 44 did not. Among the 112 liveborn infants, 70 survived to 28 days and 42 did not.
* per 1-week increase
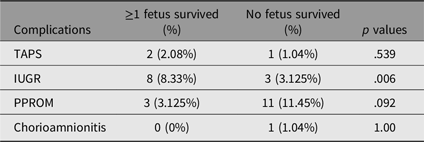
Laboratory tests performed within 24 hours of birth revealed a relatively wide range of hemoglobin (Hb) levels, from 8.80 g/dL to 24.90 g/dL, with a mean of 15.03 g/dL. Most samples exhibited low C-reactive protein (CRP) levels, reflected by a median of 0.30 mg/L and a mean of 1.72 mg/L. Cranial USG examinations were performed on 46 infants. Among these patients, 24 (52.17%) had brain injury. The most common abnormalities observed included intraventricular hemorrhage (IVH) grade 1 in 8 patients (17.39%), IVH grade 3 in 3 patients (6.52%), and periventricular echogenicity in 8 patients (17.39%). Other findings included subependymal cysts (3 cases, 6.52%), ventriculomegaly (3 cases, 6.25%), white matter injury (2 cases, 4.34%), periventricular leukomalacia (1 case, 2.17%), and hypoxic-ischemic encephalopathy (1 case, 2.17%). Only 8 infants had available neurodevelopmental follow-up records. Among these 8 infants, two were recorded as having delayed milestones. The first case of delay was identified at a chronological age of 4.5 months (corrected age 2.5 months), and the second at a chronological age of 13 months (corrected age 10 months). Pregnancies complicated by IUGR were identified in 11 pregnancies, of which 8 cases (8.33%) resulted in at least one neonate surviving to 28 days, while 3 cases (3.125%) had no neonatal survival at 28 days (p = .006); see Table 7.
Pregnancy complication versus 28-days neonatal survival in twin-to-twin transfusion syndrome
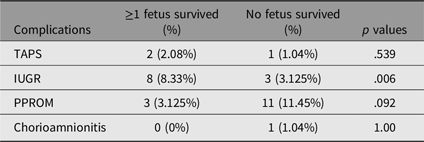
Table 7. Long description
The table presents data on pregnancy complications and their impact on 28-day neonatal survival in twin-to-twin transfusion syndrome. It includes four rows and four columns, with headers for Complications, >=1 fetus survived (percentage), No fetus survived (percentage), and p values. The complications listed are TAPS, IUGR, PPROM, and Chorioamnionitis. For TAPS, 2.08% of cases had at least one fetus survive, while 1.04% had no survival, with a p value of 0.539. For IUGR, 8.33% had at least one fetus survive, while 3.125% had no survival, with a p value of 0.006. For PPROM, 3.125% had at least one fetus survive, while 11.45% had no survival, with a p value of 0.092. For Chorioamnionitis, 0% had at least one fetus survive, while 1.04% had no survival, with a p value of 1.00. The table highlights that IUGR has a significant impact on neonatal survival, as indicated by the p value of 0.006.
Note: Percentage calculated based on 96 pregnancies. TAPS, twin anemia-polycythemia sequence; IUGR, intrauterine growth restriction; PPROM, preterm premature rupture of membranes.
Discussion
This study represents Indonesia’s first and most comprehensive 9-year experience with FLA for TTTS, conducted at the country’s national referral center for maternal and child health, provides valuable insights into fetal and neonatal outcomes in the context of a developing healthcare system.
The mean GA at the time of the procedure was 23.24 ± 3.25 weeks, similar to other reports, which reported a mean of 20.9 ± 1.9 weeks and 20.52 ± 2.42, respectively (Akkermans et al., Reference Akkermans, Peeters, Klumper, Lopriore, Middeldorp and Oepkes2015; Kweon et al., Reference Kweon, Lee, Cho, Park, Park and Jun2019). The post-procedure fetal outcomes revealed survival of both fetuses in 77.35% of cases and at least one surviving fetus in 87.73%, similar to those reported in other studies (Kweon et al., Reference Kweon, Lee, Cho, Park, Park and Jun2019; Spruijt et al., Reference Spruijt, Lopriore, J. Steggerda, Slaghekke and Van Klink2020; Yang et al., Reference Yang, Leung, Kee, Chen, Chan and Lau2010). These improved survival rates are likely multifactorial, potentially reflecting advancements in laser techniques, increased surgical expertise, greater referral systems, and improvements in neonatal care (Spruijt et al., Reference Spruijt, Lopriore, J. Steggerda, Slaghekke and Van Klink2020). In our study, preterm prelabor rupture of membranes (PPROM) occurred in 11.82% of the cases in which at least one fetus survived, whereas it occurred in 30.76% of the cases in which double fetal death occurred, which aligns with previous reports that PPROM occurs in as many as 30% of cases following laser surgery (Malshe et al., Reference Malshe, Snowise, Mann, Boring, Johnson, Bebbington, Moise and Papanna2017; Spruijt et al., Reference Spruijt, Lopriore, J. Steggerda, Slaghekke and Van Klink2020). Fetal death and PPROM are the most common complications after laser surgery (Ling et al., Reference Ling, Phelps, Tate, Adefisoye, Mehra and Prazad2023; SMFM & Simpson, Reference Simpson2013; Spruijt et al., Reference Spruijt, Lopriore, J. Steggerda, Slaghekke and Van Klink2020; Yamamoto et al., Reference Yamamoto, El Murr, Robyr, Leleu, Takahashi and Ville2005). Fetal death occurs in approximately 13% to 33% of cases, which is consistent with our finding of 17.37% following fetoscopy (Spruijt et al., Reference Spruijt, Lopriore, J. Steggerda, Slaghekke and Van Klink2020).
The mean GA at birth of surviving neonates was 32.25 weeks. The neonatal survival rates for at least one twin, a single twin, and both twins were 50%, 25%, and 23.95%, respectively, which are slightly lower than those reported in other studies (Akkermans et al., Reference Akkermans, Peeters, Klumper, Lopriore, Middeldorp and Oepkes2015; Kweon et al., Reference Kweon, Lee, Cho, Park, Park and Jun2019). Several factors may have contributed to these outcomes, including restricted fetal growth; premature labor or PPROM; surgical complications, such as recurrent TTTS or TAPS; GA; abnormal Doppler findings; and the Quintero stage (Kweon et al., Reference Kweon, Lee, Cho, Park, Park and Jun2019; SMFM & Simpson, Reference Simpson2013). Among all factors influenced in the present study, Quintero stage showed most statistically significant association with with fetal survival after fetoscopy. Meanwhile, 28-day neonatal survival was significantly associated with GA at birth (32.25 ± 2.95 weeks in neonates who survived vs. 27.62 ± 2.68 weeks in those who did not; 95% CI for survival odds: 1.4-2.1) and with IUGR (8.33% in pregnancies with at least one 28-day survivor vs. 3.13% in pregnancies without 28-day neonatal survival; p = .006), suggesting that both prematurity at delivery and growth restriction remain key determinants of early neonatal outcomes after procedure. The Quintero stage 2 group demonstrated the most favorable prognosis, with all patients resulting in the survival of at least one fetus. Quintero stages ≥3 were more likely to lead to intrauterine fetal death (IUFD), although fetal survival was still possible, as reported in a previous study (Kweon et al., Reference Kweon, Lee, Cho, Park, Park and Jun2019). A greater risk of single fetal demise in advanced TTTS Quintero staging may be explained by the hemodynamic effects of FLA accentuate cardiovascular strain in both donor and recipient twins. In donor fetuses with stage 3 TTTS, irregular umbilical artery blood flow could lead to significant placental insufficiency following FLA of the placental vascular connections, specifically arterio-arterial anastomoses causes growth-restricted donor fetuses (Nassr et al., Reference Nassr, Hessami, Espinoza, Donepudi, Cortes, Belfort and Shamshirsaz2022).
It is important to emphasize that routine serial USG every two weeks, starting at approximately 16 weeks until delivery is recommended for all twins with MCDA placentation, considering the possibility progression from stage 1 or 2 TTTS to more advanced stages. This approach may facilitate earlier detection and intervention for TTTS, thereby improving the likelihood of perinatal survival. Even after FLA, the needed for monitoring remains crucial because not all anastomoses are ablated during the FLA. The residual anastomoses that were either initially missing, undiagnosed, or revascularized have been found in as many as one-third cases in post-laser evaluations, and their persistence may contribute to recurrent or reversed TTTS or TAPS. (SMFM & Simpson, Reference Simpson2013; Yang et al., Reference Yang, Leung, Kee, Chen, Chan and Lau2010)
Even though the FLA is recommended in Quintero stage ≥2, a randomized trial and several meta-analyses for Quintero stage 1 showed no significant difference intact survival between immediate surgery and expectant management, emphasizing the stage 1 may not benefit as clearly from intervention (Nassr et al., Reference Nassr, Hessami, Zargarzadeh, Krispin, Mostafaei, Habli, Papanna, Emery and Shamshirsaz2023; Stirnemann et al., Reference Stirnemann, Slaghekke, Khalek, Winer, Johnson, Lewi, Massoud, Bussieres, Aegerter, Hecher, Senat and Ville2021).
The preterm birth of TTTS survivors puts them at increased risk for consequences, such as respiratory issues, necrotizing enterocolitis, retinopathy of prematurity, and brain injury (Gijtenbeek et al., Reference Gijtenbeek, Haak, Huberts, Middeldorp, Klumper, Slaghekke, Lopriore, Oepkes and Van Klink2020; Ling et al., Reference Ling, Phelps, Tate, Adefisoye, Mehra and Prazad2023; SMFM & Simpson, Reference Simpson2013; Spruijt et al., Reference Spruijt, Lopriore, J. Steggerda, Slaghekke and Van Klink2020). In the present study, the mean GA at delivery was 28.65±4.79 weeks, the average birth weight was 1404 ± 1617 g, with most common cranial ultrasound screening manifestation was periventricular echogenicity (17.39%) followed by IVH grade 1 (17.39%). Preterm birth and low birth weight both of which fall within the high-risk range for prematurity-related complications (Ling et al., Reference Ling, Phelps, Tate, Adefisoye, Mehra and Prazad2023; Spruijt et al., Reference Spruijt, Steggerda, Rath, van Zwet, Oepkes, Walther and Lopriore2012; Spruijt et al., Reference Spruijt, Lopriore, J. Steggerda, Slaghekke and Van Klink2020). Previous studies reported that GA is a risk factor for severe cerebral injury, which is particularly concerning given that such cerebral injury has a significant long-term implications for the infant (Cho et al., Reference Cho, Shin, Jun, Shin, Kim, Kim, Kim and Kim2019; Spruijt et al., Reference Spruijt, Steggerda, Rath, van Zwet, Oepkes, Walther and Lopriore2012). In our study, infants who underwent head USG screening had a neurodevelopmental injury risk of 54.17%, which is higher than that reported in other studies (Cho et al., Reference Cho, Shin, Jun, Shin, Kim, Kim, Kim and Kim2019; Spruijt et al., Reference Spruijt, Lopriore, J. Steggerda, Slaghekke and Van Klink2020). Delayed milestones were recorded in 15.38% of infants, which is consistent with findings from other studies reporting rates of 14%, 9.7%, and 13.7%, respectively (Hessami et al., Reference Hessami, Nassr, Sananès, Castillo, Castillo, Sanz Cortes, Espinoza, Donepudi, Sun, Krispin, Belfort and Shamshirsaz2021; Knijnenburg et al., Reference Knijnenburg, Lopriore, Oepkes, Vreeken, Tan, Rijken and van Klink2020). Regular long-term monitoring is highly advised for all twins affected by TTTS, particularly those with deteriorating Doppler flow patterns. Routine imaging of the neonatal brain-scan facilitate early identification of neurological injury and cardiac abnormalities, as other studies have shown that changes in fetal hemodynamics in TTTS survivors has been associated with both brain and cardiac outcomes (Cho et al., Reference Cho, Shin, Jun, Shin, Kim, Kim, Kim and Kim2019).
This study has the typical limitations of a retrospective design. Some data were incomplete for mothers and their babies who received care at other hospitals after the procedure. Cranial USG was routinely used for detecting cranial brain injury rather than superior magnetic resonance imaging (MRI) in our center, and long-term outcomes of neurodevelopmental impairments could not be fully assessed because of data limitation. Despite these limitations, our study provides the largest reported FLA dataset and the first 9-year experience of TTTS management in Indonesia, providing important insight from a developing healthcare system.
Conclusions
In summary, laser therapy can effectively treat TTTS with minimal maternal complications. These results highlight the importance of early detection and prompt intervention to improve pregnancy outcomes, particularly for stages 2 and above. Owing to the low follow-up rates, improving follow-up attendance is important, especially for monitoring infants at risk of neurodevelopmental delay. Moreover, further research is needed to improve these outcomes.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author, RAK. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Acknowledgments
The authors would like to express their gratitude to the staff of the Department of Obstetrics and Gynecology, Harapan Kita Women and Children Hospital, West Jakarta, for their valuable assistance and support.
Financial support
The research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
None.
Ethical standards
This study received ethical approval from Harapan Kita Women and Children Hospital (approval number IRB/12/02/ETIK/2025). Consent requirements were waived, as the study involved secondary data usage. For infants delivered outside our hospital, neonatal survival status was confirmed by contacting the mothers. During these calls, the purpose of the study was explained and verbal informed consent for using the infant’s outcome data was obtained with the approved study protocol and institutional ethical guidelines.


 Open access
Open access