


Introduction
Both within and outside hospital settings, workers may acquire occupational injuries which bring a potential risk of occupational blood exposure accidents (OBEAs) [Reference Auta1–Reference Brouillette, Quinn and Kriebel3]. The most common blood-borne viruses are hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV). According to literature, most research is done in the hospital setting, while outside the hospital scarce data are available.
The importance of non-hospital studies is increasingly evident in the context of the World Health Organization’s (WHO) 2030 goal to eliminate hepatitis and HIV. In this perspective, it is worrying that only little reduction in needle stick injuries (NSI) has been observed [Reference O’Sullivan and Gallagher4, Reference Reddy5], despite the implementation of EU regulations, including legislative safety needles. Hence, OBEAs remain a significant concern, including those occurring outside hospital settings [Reference Auta1].
In healthcare settings, the rate of HBV transmission relating to a percutaneous injury is estimated to be at an average of up to 30%: for HCV this is of 1–3% and for HIV 0.3% [Reference Kofman6]. Biting injuries seem to have only a low risk of HBV and HCV infection, whereas for a splash accident, this is thought to be lower than that of other injuries [Reference Pintilie and Brook7]. For HIV, the transmission risk after a single mucocutaneous exposure is probably less than one in thousand (0.1%) [Reference Kofman6]. There is no evidence that spitting incidents where no blood is present leads to acquisition of HIV [Reference Cresswell8, Reference O’Moore9].
Prevention of OBEA and appropriate immediate management following such accidents remain crucial to prevent acquired infections. Timely intervention is essential to reduce the impact of these viruses, as infections can lead to long-term health consequences. Vaccination against HBV is highly effective in preventing transmission [Reference Vermeiren, Hoebe and Dukers-Muijrers10]. Moreover, highly effective treatments for HBV, HCV, and HIV are now available, capable of managing or even curing these infections.
WHO estimated that sharp injuries cause about 66,000 HBV, 16,000 HCV, and 2000–5,000 HIV infections among health care workers (HCW) per year worldwide. Furthermore, NSI contribute to 39%, 37%, and 4.4% of HCV, HBV, and HIV occupational infections for HCW worldwide respectively [Reference Prüss-Ustün, Rapiti and Hutin11, 12].
In 2009, a European framework for workplace safety was established [13]. This agreement would contribute in a major way towards the improvement of working conditions of millions of HCW in the EU and beyond. A 2021 review later found a high prevalence of occupational exposure to NSI among HCW and suggests the need to improve occupational health and safety services [Reference Mengistu, Tolera and Demmu14].
Especially in lower-middle socio-demographic index (SDI) countries, pooled prevalence of OBEA for all HCW was higher (61.0%), but still substantial in high SDI (37.6%) and low SDI countries (41.6%), according to a recent systematic analysis of 83 studies. When assessing regions, the highest prevalence occurred in Southeast Asia at 58.2% [Reference Bouya15].
In the Netherlands, healthcare professionals are not universally screened for HBV, HCV, or HIV, and HBV vaccination is not legally mandatory, although employers are required under the Working Conditions Act (Arbowet) [16] to offer vaccination; since 2011, HBV vaccination has also been offered to all newborns.
The Netherlands reported annually an estimated 13,000–15,000 blood-borne accidents, of which 95% originated from the healthcare sector [Reference van Wijk17]. The majority of data and publications on OBEAs pertain to hospital staff, even though OBEA occur frequently outside the hospital [Reference Vos, Götz and Richardus18]. HCW in long-term care facilities and home care are at significant risk of these accidents [Reference Gershon19], but detailed information about its circumstances is lacking.
However, given the aging population, it is likely that more people will be working in long-term care facilities and home care. A comprehensive understanding of OBEA is essential for providing sound recommendations regarding prevention and management as well as the necessary education for employees. Moreover, the international migration of healthcare workers, coming from non-western countries with sometimes high prevalence of blood-borne viruses, is becoming a means of maintaining service quality in long-term care facilities and home care in many high-income countries [Reference Hatzakis20, Reference Eaton21]. In the Netherlands, 19% of the HCW in home care, 17% in care and nursing, 16% in mental healthcare, and 12% in care for the disabled have a migrant background already [Reference Kremer22].
To our knowledge, only a few studies included OBEA data on non-hospital settings. One study, conducted in Belgium, provided detailed data on the causes and management of OBEA specific in long-term care facilities, concluding, among other findings, that insulin pens play a prominent role in NSI among nurses and nurse assistants [Reference Kiss, de Meester and Braeckman23]. However, this study did not focus on all non-hospital settings. A Dutch study focused on the practical management of OBEAs demonstrated improvement in the management and care of workers experiencing OBEA in both the hospital and non-hospital setting when incidents were reported to an expert 24 h-counselling centre. While many different workplaces and professions were included, there was no detail about the types of injuries that occurred in different settings. Schneeberger et al. concluded that more research is needed to explore OBEA risks and to design tailored preventive measures [Reference van Wijk24, Reference Schneeberger25]. To address this knowledge gap, we conducted a 9-year retrospective descriptive analysis of nearly 1,000 registered OBEA cases occurring outside hospital settings across various professional groups.
The aim of our study was to gain a deeper understanding of the occurrence, circumstances, risks, risk groups, and post-exposure measures of work-related blood exposure accidents outside the hospital to inform recommendations on the management of OBEA for practice and policy.
Method
Under occupational health and safety legislation, employers in the Netherlands are obligated to protect the health of their employees. This includes a policy for OBEA. The management of an OBEA can be done by the care institution itself, the local PHS, or by another (national) organization that handles these accidents. Employees should report an OBEA as soon as possible to their employer. Guidelines on reporting and management are part of the employer’s OBEA policy and are based on the Dutch national guideline on needle stick accidents [26].
Data collection
All non-hospital employees who reported an OBEA to Public Health Service (PHS) South-Limburg (serving a population of about 610.000 inhabitants) during the time period January 2006 to December 2014 were included in this study. Researchers only had access to anonymized data; they could not use any personal data, as these had been removed.
For each OBEA notification, a standardized accident registration form was used to collect systematic data on sex, age and profession of the employee, hepatitis B vaccination status, workplace, times of accident and reporting, type of injury, and causal device. Risk assessment and post-exposure measures taken were also registered. Employee’s serum test results (reference serum and follow-up serum) and source’s personal data and serostatus on HBV, HCV, and HIV were collected if deemed necessary (and possible) according to the Dutch national guideline [26]. See Supplementary Appendix 1.
Interventions: Guideline on high-risk and low-risk blood exposure accidents
Each OBEA was handled by a PHS public health nurse or communicable disease consultant, following the Dutch national guideline. This guideline includes a risk assessment methodology based on the nature of the injury and its post-exposure management in practice to protect the exposed individual. OBEAs are categorized as either high risk or low risk based on the volume of blood transmitted and type of OBEA. Exposures with no risk of transmission are not part of the categorization and will not be notified to PHS. For low-risk accidents with no visible blood or blood on superficially damaged skin, measures to prevent HBV must be looked at: immunization of non-immune employees, either not (fully) vaccinated or non-responder (HBV anti-bodies <10 IU/L). For high-risk injuries involving a significant amount of blood exposure and a corresponding risk of transmission (e.g. percutaneous injuries or blood on mucous membrane), not only measures to prevent HBV but also to prevent/monitor HCV and HIV infection need to be considered. These consist of reference and follow-up serum testing on both HCV and HIV antibodies right after the accident and after 3 months and on HCV antibodies after 6 months, as well as prescribing HIV post-exposure prophylaxis for 28 days.
The need for post-exposure prophylaxis and reference and follow-up serum testing is determined by the victim’s immunity to HBV (vaccination status) and the (chance of) presence of HBV, HCV, or HIV in the source individual (e.g. known risk behaviour) [Reference van Wijk17]. When the source individual agrees to an (urgent) blood test, and the source tests negative, no serum needs to be taken from the employee, because no follow-up testing will be done. In case of an unknown, a positive or a source not willing to participate, reference and follow-up serology tests on the employee need to be performed by PHS. In case of a HIV positive or an unknown/unwilling source with possible HIV risk behaviour, the employee will be referred to the regional university hospital for risk assessment and prophylaxis.
Analysis
A descriptive analysis was conducted to examine key variables related to OBEA, including workplaces, professions, age groups, types of injury, employees’ hepatitis B vaccination status, and post-exposure management including risk assessment.
Workplaces
OBEA cases were categorized per workplace (by most reported to least reported OBEA, with the two last groups being combined due to small numbers), including long-term care facilities, home care, mental health care, disability care, police departments, dental practices, ‘medical sterilization and other non-medical care (e.g. waste collection service), and ‘ambulance and other medical care’ (e.g. midwifery).
Professions
This study included the following professional categories: nurses, nurse assistants, nurses or nurse assistants (status unknown), medical doctors, police officers, mentors, nursing students, housekeeping staff, and medical assistants. Additionally, the category of ‘Others’ included employees working, for example, in dental practices or medical sterilization.
Age groups
Participants were grouped into three age categories: under 25 years, 25–50 years, and over 50 years.
Types of injury
Injuries were classified into the following categories: intramuscular needle, subcutaneous needle, lancets, venipuncture, instruments, biting, spitting/scratching, other, and unknown needle.
Employees hepatitis B vaccination
Employees were regarded as being fully vaccinated against hepatitis B if they had received at least three doses of the hepatitis B vaccine and had undergone an immune response assessment confirming vaccination efficacy. Individuals categorized as ‘not vaccinated’ included those who had received no vaccinations, were partially vaccinated, or were non-responders (HBV anti-bodies < 10IU/L).
Post-exposure management
Post-exposure management was based on the risk assessment (low-risk or high-risk OBEA) and categorized as no measures required, HBV immunization, source testing, collection of the employee’s reference serum, follow-up serum testing when needed, and administration of HIV post-exposure prophylaxis.
This approach allowed for a comprehensive analysis of OBEA cases across different professional groups and workplace settings, providing insights into risk profiles and management practices. To test for differences by profession and workplace on circumstances and post-exposure measures, we applied chi-square analyses and t-tests. Analyses were performed with SPSS 20.0 (IBM INC., Somers, NY, USA).
For readability, only in case of statistically significant results, P-values are mentioned in the text. A P-value <0.05 was considered statistically significant.
Medical ethical statement
The Medical Ethics Committee of Maastricht University Medical Centre (MUMC+) exempted this study from official approval under prevailing laws in the Netherlands after official review of the study protocol as all data presented in this paper were retrospectively retrieved from regular infectious disease control activities and were deidentified, coded, and analysed anonymously (METC number: 2021-2901).
Results
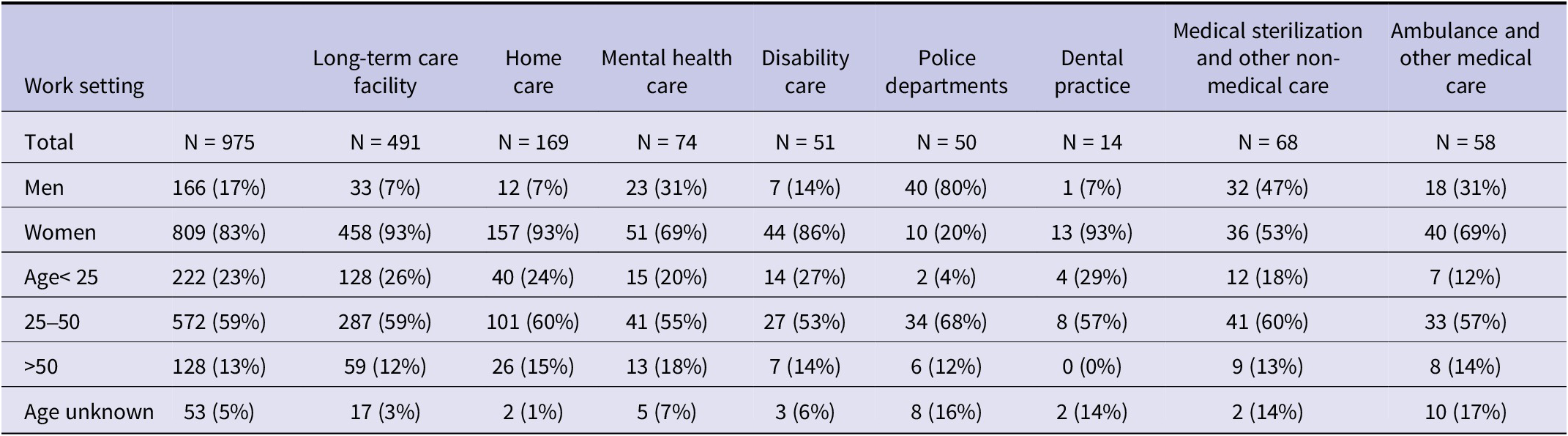
A total of 975 OBEA for non-hospital employees were included in the analyses (Table 1). The number of OBEA was consistent over time with about 115 incidents per year, with a decline within the last two years to approximately 90 OBEA per year.
Sex and age distribution of occupational blood exposure accidents (OBEA) cases for different workplaces

Workplaces
The majority (49%, N = 478) of OBEA were reported by long-term care facilities, followed by home care (17%, N = 166).
Professions
Of all OBEA-reporting employees, 68% (N = 663) were working as nurses or nurse assistants.
Table 1 shows a further breakdown of the professions and workplaces. Overall, the vast majority of OBEA were reported by women (83% N = 809). In long-term care facilities 93% (N = 458) of the reports were done by female employees, while this was 20% (N = 10) at the police departments.
Age groups
Of all employees, 25% were younger than 25 years old (n = 222), 61% were between 25 and 50 years old (n = 572), and 14% were older (>50 years old) (n = 128).
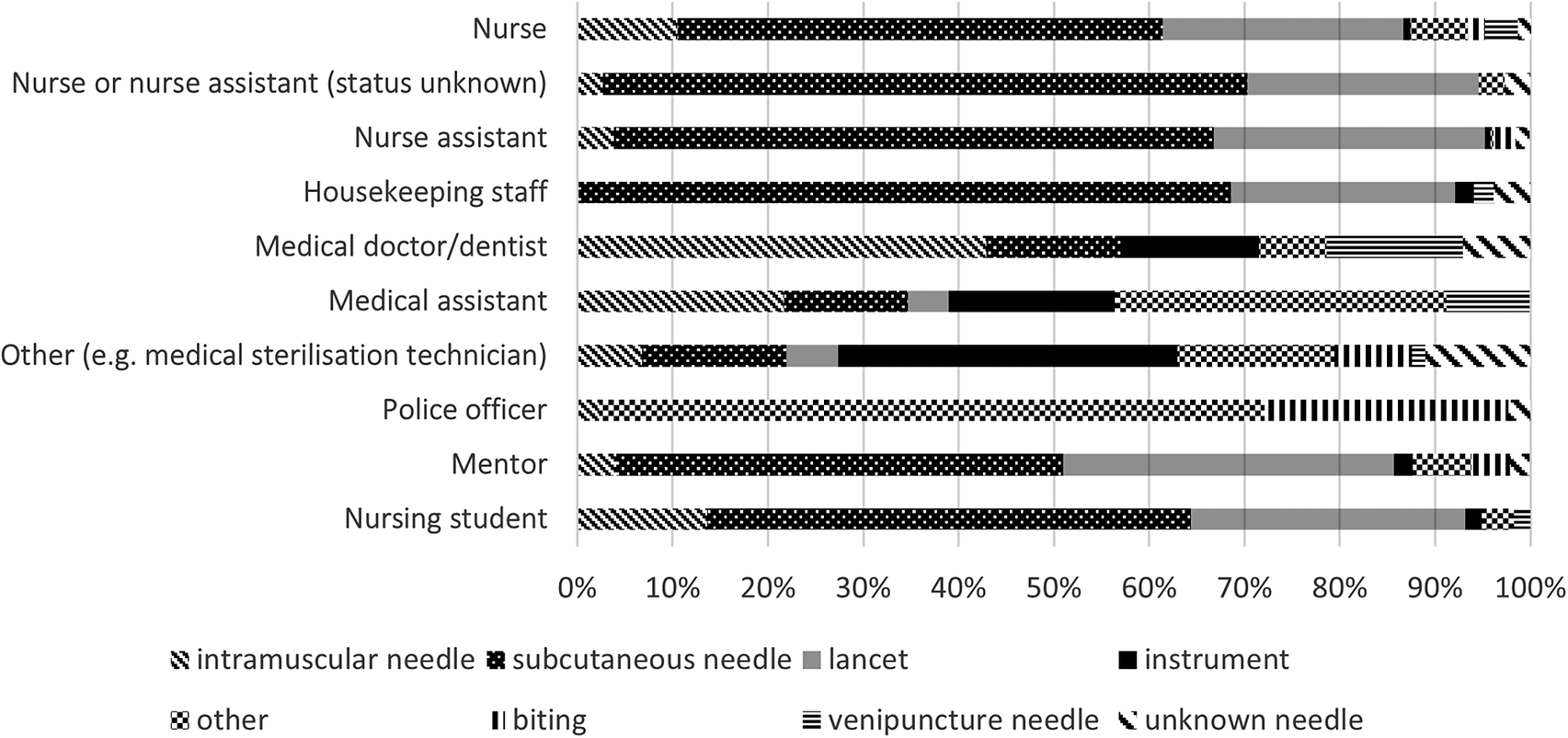
Types of injury
The type of injury reported varied across professions as shown in Figure 1. Nurses, nurse assistants, nursing students, and housekeeping staff mainly reported subcutaneous needle (51–67%) and lancet (23–28%) injury; police officers reported bite incidents (26%) and spitting/scratching (70%); medical sterilization staff reported needle (11%) or instrument-related injuries (31%).
Percentage of types of exposure for the different professions.

Employees hepatitis B vaccination
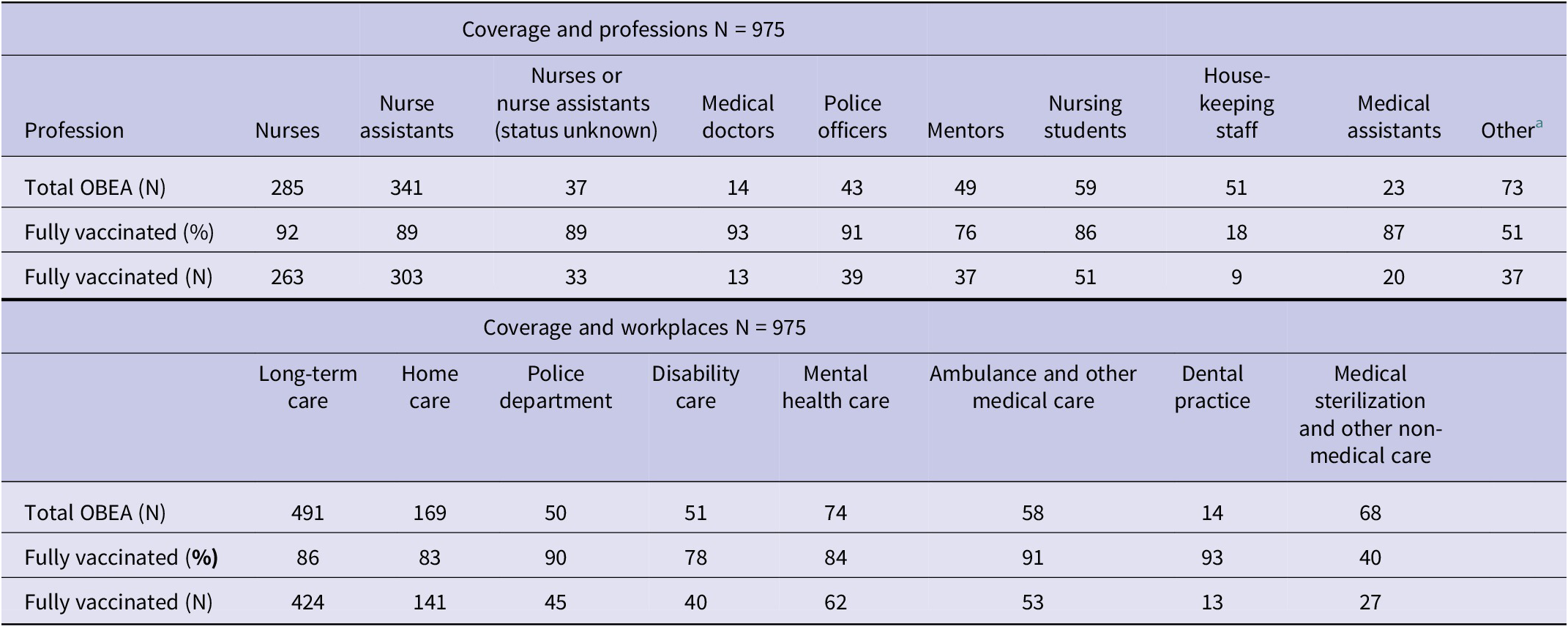
The overall HBV vaccination coverage in OBEA reporting employees was 83% (n = 805) but varied between professions; it was 18% among housekeeping staff and up to 93% among medical doctors, police officers, nurses, and nurse assistants (Table 2).
HBV vaccination coverage for the different professions and workplacesa

a Other: employee working in dental practice or medical sterilization.
Coverage also varied between workplaces. Among ‘Ambulance and other medical care’ and the police departments, this was 90–93%, while within the disability care, home care, mental health care, and long-term care, 78–86% of affected individuals were fully vaccinated. Elderly workers (age >50 years) were less often vaccinated (76%) (P < 0.05).
Non-responders were observed in 1–3% of nurses, nurse assistants, and medical sterilization staff. Vaccination coverage increased over time, from 76% of all reporting employees being fully vaccinated and 20% unvaccinated in 2006 to 90% fully vaccinated and 9% unvaccinated in 2014. Vaccination coverage among nursing students has been consistently high with 100% since 2011.
Post-exposure management
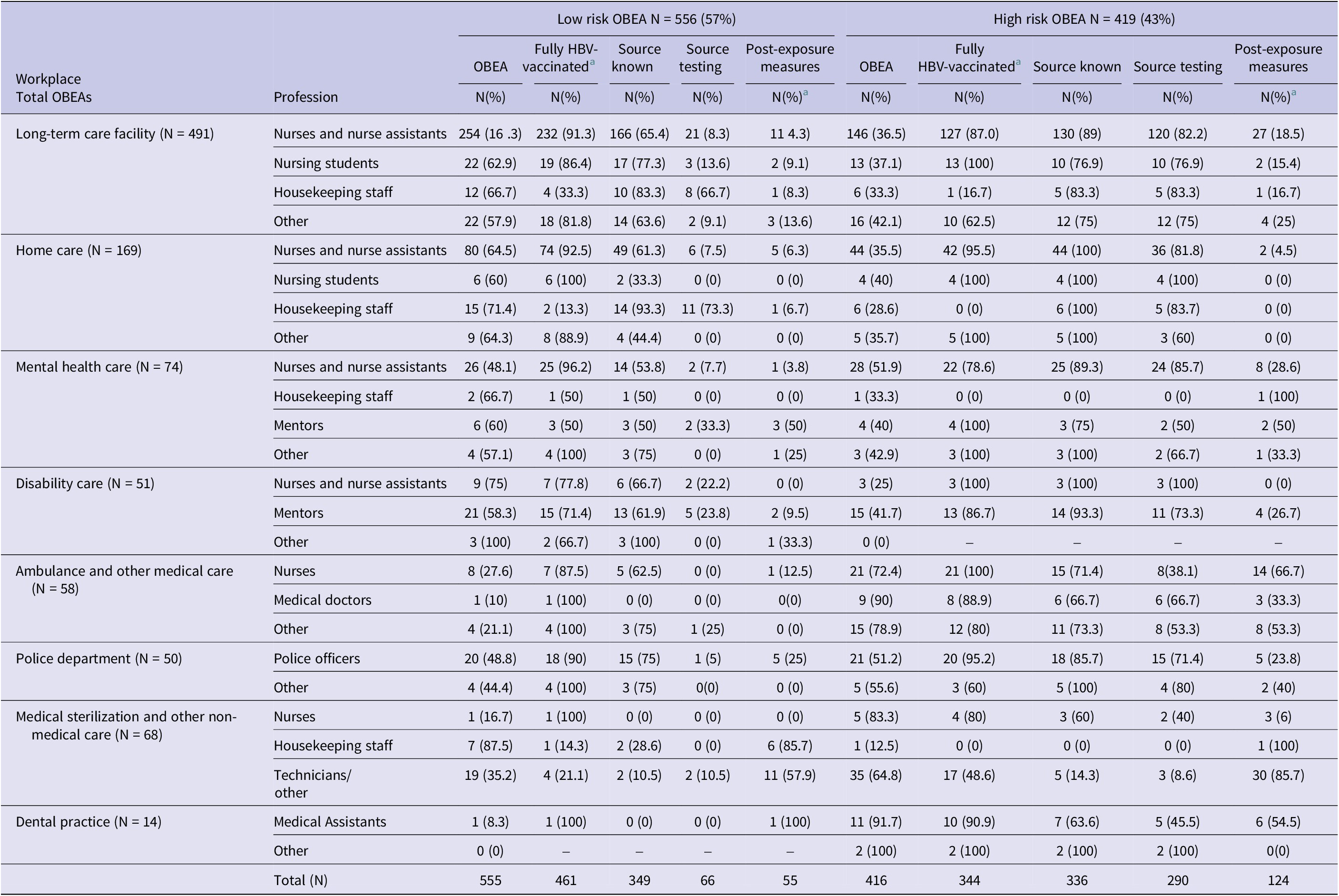
Of all reported OBEA, 419 (43%) were high-risk accidents. Within ‘Ambulance and other medical care’, ‘medical sterilization and other non-medical care’, police department and dental practice of all OBEA, more than 50% was assessed as high risk. Low-risk OBEAs were mostly seen among housekeeping staff (73%, N = 37) and nurse assistants (67% of all reporting nurse assistants, N = 228).
For more than half (52%, N = 503) of the reported OBEA, post-exposure measures were taken, comprising 392 high-risk and 111 low-risk accidents (78% and 22%, respectively).
The majority of post-exposure measures were carried out among medical assistants, while the fewest were conducted among nurses and nurse assistants (Table 3).
Post-exposure measures for the different professions

a Other: employee working in dental practice or medical sterilization.
An overview of risk assessment and post-exposure measures is depicted in Table 4. This table shows the total number of low- and high-risk OBEA reported, during the time period 2006–2014, by workplace and profession.
Total number of low and high risk OBEA reported, 2006–2014, by workplace and profession (N = 975)

a Employee was fully HBV vaccinated before reporting OBEA.
Regarding HBV immunization/post-exposure prophylaxis, hepatitis B immunoglobulins (total N = 37) were mainly administered in OBEA in housekeeping and medical sterilization staff, involving 16% of all housekeeping staff (N = 8) and 21% of all medical sterilization staff (N = 14). This is, respectively, 22% and 38% of total amount of immunoglobulins given.
HBV vaccination (total N = 62) was initiated for 33% of all medical sterilization staff (N = 22), 24% of housekeeping staff (N = 12), and 23% of mentors (N = 11).
Of all employees whose serum was taken (N = 137), post-exposure follow-up serum testing was conducted for 122 employees, more frequently among household staff (18% of all staff, N = 9), police officers (21% of all officers, N = 9), and medical sterilization staff/other non-medical care (49% of all staff, N = 36). Within 6 months, none of the employees seroconverted.
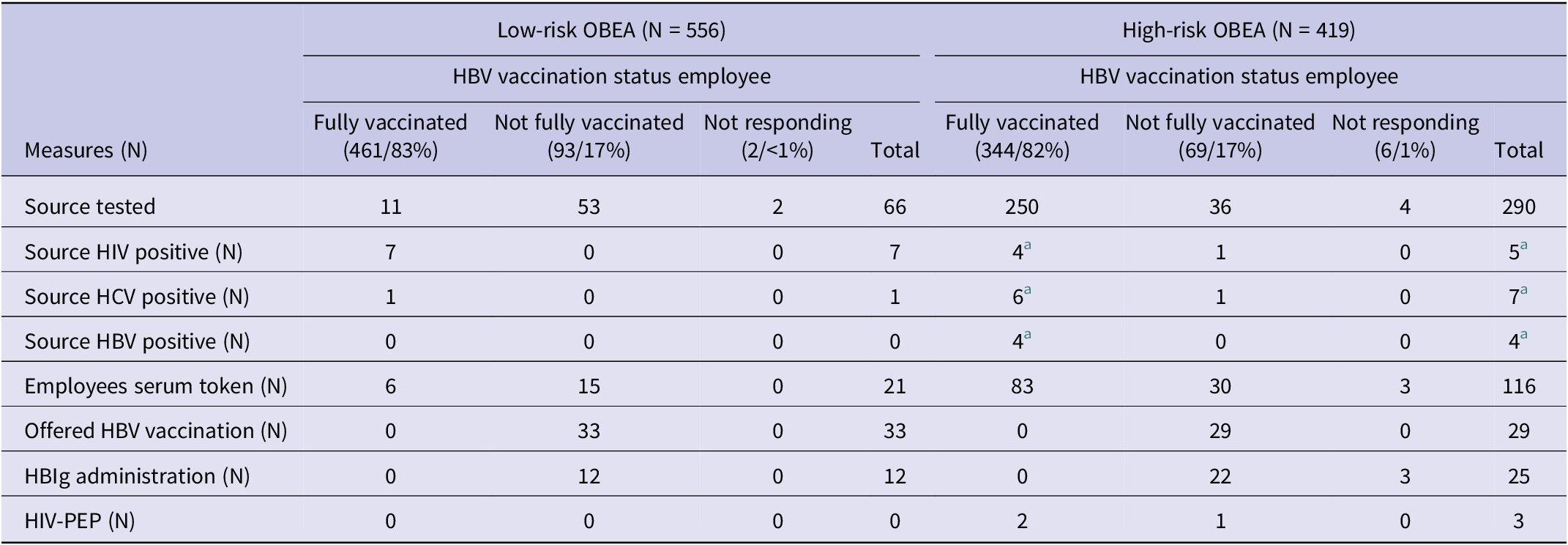
For 685 reported OBEA (70%), the source was identified, being 349 low-risk (63% of all low-risk accidents) and 336 high-risk accidents (80%). Source identification was notably high among police officers and nurse assistants (both 81%).
Source testing was conducted in 356 OBEA (37% of all reported accidents), with higher testing rates among police officers, medical assistants, and housekeeping staff (42–58% of reporting profession) and lower rates among medical sterilization staff (15% of all medical sterilization staff).
Overall, five sources tested positive for HBsAg (prevalence 1.4%) and seven for anti-HCV (2.0%). A positive HIV source was identified in 10 OBEA notifications (2.8%). However, seven simultaneous low-risk OBEA (among police officers) were linked to the same positive HIV source. In total, four unique sources tested HIV positive (prevalence 1.1%). Regarding one OBEA notification, the source tested positive for both HBV and HCV, while another one tested positive for both HBV and HIV.
HIV post-exposure prophylaxis (PEP) was provided to three employees working in police department, ambulance transport, and mental health care. See Table 5.
Post-exposure measurements taken in low- and high-risk OBEA

a Of all tested persons, we found two double infections among the sources (1 HBV/HCV pos and 1 HBV/HIV pos).
Notably, a relatively high percentage of sources were tested among housekeeping staff despite their involvement in low-risk OBEA.
Discussion
Our findings provide a comprehensive overview of the frequency, circumstances, and risk factors associated with occupational blood exposure accidents (OBEA) in non-hospital settings, highlighting critical gaps in preventive measures and post-exposure management across various professional groups. With 975 OBEA cases reported over 9 years, the data from this large study reveal significant variation in HBV vaccination coverage, types of injury, and post-exposure management across different professions and workplaces. Remarkable findings included the overall low hepatitis B vaccination coverage, the relatively low vaccination rate among older employees, and the many accidents reported by nurses and nurse assistants caused by insulin needles, insulin pens, and glucose meter needles and lancets. The results of our study emphasize the persistent vulnerability of non-hospital professionals. Outcomes also underscore the need for targeted strategies to improve preventative measures like vaccination and mitigate OBEA risks.
A striking finding was the substantial variation in hepatitis B vaccination coverage, which was generally low. This led to an increased need for post-exposure measures in low-risk OBEA, which would not be necessary with a high vaccination rate. The average vaccination rate for all employees included in this study was 80%, ranging from 18% to over 90%, despite the rollout of national vaccination guidelines and occupational immunization programmes. Vaccination rates were the lowest in housekeeping staff and highest among nurses, nurse assistants, and police officers, but among them still, nearly 10% were not fully vaccinated. Only among nursing students an increase up to 100% in vaccination coverage was observed, showing the positive results of offering vaccination during education. In contrast, older employees (>50years) were generally more often not vaccinated.
Most countries have incorporated HBV vaccination in their national immunization programmes for all children. In the Netherlands, universal hepatitis B vaccination was introduced in 2011 for children born on or after August of that year. For a longer period, occupational HBV vaccination strategies have been in place for all health care workers who may have direct contact with patients’ blood, blood-stained body fluids, or tissues [27].
Based on our study results, all employees at workplaces with a reasonable risk of exposure to blood should be offered hepatitis B vaccination (e.g. housekeeping staff).
However, employee mobility, particularly in home care settings, remain a challenge for achieving full HBV-B coverage. Workplaces should therefore be encouraged to develop an action plan for all workers, with particular attention to those above 50 years old, to support successful vaccination programme implementation.
Another noteworthy finding was the difference in occurrence and characteristics of OBEA among workplaces and professions. Housekeeping staff (in a healthcare setting) appeared to be at risk for OBEA, primarily experiencing low-risk accidents, relatively often with unknown needles. At the same time, they had the lowest HBV vaccination coverage among all groups (18%). As a result, they often required post-exposure measures that would have been unnecessary if they were properly immunized. It is essential to take actions to improve their HBV vaccination status. Additionally, housekeeping staff within healthcare should receive education and training on OBEA awareness and injury prevention [Reference Cheetham28].
Based on our study findings, mentors working in disabled care centres are also advised to increase their HBV vaccination coverage, which stood at 76%.
For employees working at medical sterilization, the observed low HBV vaccination rate (51%) requires attention as well. Mainly high-risk accidents were reported, often with an unknown source since medical instruments mostly cannot be traced back, which meant that post-exposure reference and follow-up serum testing was needed regularly.
Serum testing was more often needed for police officers because the source did not always agree (right away) to undergo serology testing. Prevalence of HBV, HCV, and HIV in detainees is higher than in the general population due to risk behaviour such as injecting drug use and unsafe sex, coupled with pre-detention social vulnerability [Reference Barreira-Díaz and Buti29, Reference Falla30]. Next to HBV vaccination, training police officers to avoid exposures remains the most critical measure for reducing transmission risks [Reference Kremer22].
Notable was the finding that a high proportion of nurses and nurse assistants reported accidents, some categorized as high-risk, specifically caused by insulin needles, insulin pens, and glucose meter needles and lancets. A possible explanation might be that nurses and nurse assistants more often perform routine procedures using medical devices linked to OBEA-risk, for example, giving an insulin injection. Kiss et al. found insulin pens indeed being the most frequent cause of NSI among nursing personnel and often being connected with unsafe needle-handling practices [Reference Mengistu, Tolera and Demmu14]. Therefore, preventive actions for nurses and nurse assistants should focus on strategies specifically avoiding these types of injuries.
In our study, the chance that a source tested positive proved to be small. Only a few source individuals tested positive for HBV, HCV, or HIV. This fits the expectation, since, in the Netherlands, the seroprevalence of HBV, HCV, and HIV is generally low. The estimated Dutch HBV prevalence is 0.2%, for HCV this is 0.1–0.4% [Reference Kiss, de Meester and Braeckman23, Reference van Wijk24]. The prevalence of HIV infection in the general population is also low (0.2%) but higher in specific sub-populations [Reference Schneeberger25]. Only a few infections are related to blood exposure accidents in the Netherlands [Reference Prüss-Ustün, Rapiti and Hutin11]. This was confirmed by our study where none of the tested employees seroconverted. It appears reasonable to consider in countries with low HBV prevalence, unnecessary source testing can be minimized by omitting tests for low-risk exposure incidents among fully vaccinated, healthy healthcare workers, while reserving testing for high-risk exposures on a case-by-case basis.
Over the last decade, the international migration of health workers has increased [Reference Drennan and Ross31] from countries in Eastern Europe, Asia, and Africa, where the prevalence of chronic HBV, as well as HCV and HIV, is considerably higher than in western/high-income countries. Globally among health care workers, the prevalence of acute hepatitis B infection is 5.3%, being more prevalent in health care workers in low-income countries, particularly in Africa, whereas the highest immunization rates against HBV in health care workers were recorded in high-income countries. [Reference Mahamat32]. It is suggested that policies for screening and vaccinating health care workers be reviewed and, where appropriate, updated in line with the existing HBV vaccination guidelines in the Netherlands.
Another point of attention is the increasing number of immunocompromised workers taking immunosuppressive drugs for the management of autoimmune inflammatory conditions, who were not addressed in this study [Reference Azoulay33]. This enables them to participate better in daily activities including work but might raise concerns regarding the immune response to HBV vaccination (non-responding) and risk for infectious diseases at the workplace. It is important that employers are aware of possibly having more non-responders at their workplace. Non-responders should not delay notifying an OBEA, since for them immediate action might be required including administering hepatitis B immunoglobulins.
One limitation of our study was the difficulty in addressing the prevalence of OBEA outside hospital settings due to insufficient data on the entire population of employees served (denominator) from which our sample of accident notifications originated. A large part of this population consisted of around 11,500 employees from long-term care facilities, home care, and police who were vaccinated by PHS South-Limburg over a period of 13 years including our study time frame [26]. This number would yield a crude OBEA prevalence estimate of 0.5%. The PHS did not exclusively receive accident notifications from the institutions mentioned above, so most likely, the total extent of its blood-borne accident care is probably larger.
Another limitation was the lack of consistent data on the specific work procedures during which the accidents occurred in some cases. However, on the accident registration forms, activities concerning the needle waste container, recapping of needles, police arrests, unexperienced nursing students performing various medical procedures, and needles left in inappropriate places such as waste or bed were regularly noted. These are valuable observations when developing customized prevention guidance.
In addition, although the data set is from some years ago, we expect the situation has not much changed. Given the richness of the dataset and the inclusion of various non-hospital workplaces, this study provides valuable outcomes. Although the data were collected from a single region, it likely reflects broader patterns across the Netherlands.
Generally, OBEA outside hospital settings are known to be largely under-reported and, thus, causing a bias in outcomes [12, 13]. Unlike in hospitals, monitoring systems to record accidents are often not in place [Reference Bouya15]. Even when reported internally at work, accidents might not be notified to a central office. High-risk OBEA needing post-exposure measures would rather be notified than low-risk accidents, leading to an over-representation of high-risk OBEA. The slight decrease in the number of accident notifications received in 2013 and 2014 compared with previous years could be related to the EU directive that came into force by the end of 2013 and required the use of safety needles [13, Reference Lu34]. Raised awareness and knowledge among employees could also play a role. However, it is still important not to underestimate the seriousness of NSI [Reference Brusini35]. Despite the implementation of EU regulations, O’Sullivan reported in 2020 no reduction in NSI but a lower incidence of NSI from ‘disposable needles with syringes’ after the implementation of the EU regulations [Reference O’Sullivan and Gallagher4].
In contrast to the current generic OBEA protocols, the high diversity in OBEA as shown by this study emphasizes the necessity of turning to profession- and workplace-specific preventive actions [Reference Schneeberger36]. This will enhance prevention and will lead to adequate post-exposure measures. While previous studies by Chen and Schneeberger suggested this as well, implementation of such targeted prevention remains a challenge [Reference Schneeberger36, Reference Chen and Jenkins37].
Conclusion
Employees outside the hospital are at risk of NSI and other OBEA. The – albeit increasing – insufficient vaccination rate and the frequent occurrence of OBEA highlight the need for sustained attention from both employees and employers, with a focus on addressing the specific issues within each occupational group, for both health care workers and non-health care workers.
Our study findings underscore the importance of offering more tailored recommendations for the prevention and management of OBEA, considering their unique circumstances within different professions and workplaces. Occupational health services must continue to play a vital role in optimizing the provision of occupational hepatitis B vaccinations. Vaccinating nursing students during their education has proven to be an effective strategy, resulting in high levels of protection within this group.
This study also raises an important consideration regarding the management of low-risk accidents. Given the extremely low number of positive sources, it may be worth revisiting the necessity of initiating follow-up procedures for certain low-risk accidents after reporting an OBEA in countries with low HBV prevalence. For fully vaccinated employees involved in low-risk incidents, it may be reasonable to forgo post-exposure measures, given the overall low risk of OBEA in settings like the Netherlands.
It remains important to notify and register OBEA in a standardized way in order to keep track of occurrence, risk groups, and circumstances of these accidents. In this way, OBEA prevention and post-exposure measures can be evaluated and OBEA protocols can be adapted accordingly.
Abbreviations
- BBV
-
blood-borne virus
- EU
-
European Union
- HBV
-
hepatitis B virus
- HCV
-
hepatitis C virus
- HCW
-
health care workers
- HIV
-
human immunodeficiency virus
- NSI
-
needle stick injuries
- OBEA
-
occupational blood exposure accidents
- PHS
-
Public Health Service
- WHO
-
World Health Organization
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/S0950268826101319.
Data availability statement
The data sets used and analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgements
The authors would like to thank the public health doctors and nurses of PHS South-Limburg for handling the blood-borne accidents and collecting the data. The authors acknowledge Helen Sijstermans for her contribution to the tables and figures.
ChatGPT (OpenAI Inc) version 5.2 was used to improve the correctness of the language and reduce the word count. All output was carefully reviewed and edited before it was added to the manuscript.
Author contribution
EB, HW, and CS analysed the data. EB and HW drafted the manuscript. ND, CdH, and CH were involved in data analysis and critically reviewed the manuscript. All authors approved the manuscript.
Funding statement
This research was supported by the Dutch National Institute for Public Health and Environment’s Research Funds for local Public Health Services (grant number 3910042010). Open access funding provided by Maastricht University.
Competing interests
The authors declare that they have no competing interests.
Ethical standard
The Medical Ethics Committee of Maastricht University Medical Centre (MUMC+) exempted this study from official approval under prevailing laws in the Netherlands after official review of the study protocol as all data presented in this paper were retrospectively retrieved from regular infectious disease control activities and were de-identified, coded, and analysed anonymously (METC number: 2021-2901). Retrospective research is not subjective to the Dutch law on scientific research with human subjects (Wet medisch-wetenschappelijk onderzoek met mensen) as stated by the National Central Committee on Research Involving Human Subjects. No additional administrative permissions were required to use the data as it is owned by the South Limburg Public Health Service.




 Open access
Open access