


Qatar is an Arabic country situated on a peninsula in the Persian Gulf. The country has undergone a significant economic and demographic transition with oil and gas production, leading to an increase in per capita gross domestic product. Reference de Bel-air1 The population of Qatar (2.85 million) includes a mixed population from different countries. The health service in Qatar was mainly hospital based and significantly developed following investment in the government and private sector provisions. Mental health services started as a single psychiatric hospital in 1971, and have undergone significant development over the years to meet the needs of the growing population and improve accessibility. Reference Ghuloum and Ibrahim2,Reference Wadoo, Ahmed, Reagu, Al Abdulla and Al Abdulla3 A mental health strategy was published in 2008 to better understand the population’s mental health needs. Reference Sharkey4 However, there was no special provision to meet the needs of adults with intellectual disabilities. Reference Sharkey4 The population of Qatar has a significant number of lone migrant workers, estimated as 1 million in the National Statistics of Qatar, whereas Qatari citizens are estimated as 0.3 million. It has been difficult to estimate the non-Qatari population with intellectual disabilities; however, from the clinic attendance data, we found that the percentage of non-Qatari patients is nearly 40%. Reference El Tahir, Elhusein, Elamin, Rustom, Reagu and Bedhiaf5
This paper evaluates the specialist service for adults with intellectual disabilities developed in Qatar, and reflects on the challenges faced.
Mental health services and intellectual disability
The mental health service in Qatar developed a wide range of specialist provisions supported by the strategic plan from the Ministry of Public Health in 2013. Service development continued to face challenges in integration with primary care and specialist provisions, 6 and barriers to accessing healthcare and poor health outcomes related to experiences of stigmatisation, discrimination and inequalities are known. Qatar has maintained a high level of funding to improve the health of its population through secondary care and tertiary specialist centre provision. 6,7 People with intellectual disabilities who had mental disorders were assessed and treated by general psychiatrists with support from professionals trained in intellectual disability. Prescribing psychotropic medication was the main intervention used by clinicians.
Intellectual disability in Qatar
The ICD-11 defines intellectual disability as significantly below average intellectual functioning and impairments in adaptive behaviour manifested during the developmental period. 8 The number of children and adults with an intellectual disability in Qatar, based on the intellectual disability classification criteria, was based on reported global prevalence rates of 1.74%. Reference Nair, Chen, Dutt, Hagopian, Singh and Du9 The prevalence rate of autism among children aged 6–14 years in Qatar has been reported as 1.14%. Reference Alshaban, Aldosari, El Sayed, Tolefat, El Hag and Al Shammari10 A special report on the intellectual disability service in Qatar was written by Professor Baroness Sheila Hollins during her visit in 2013. Baroness Hollins was invited to Qatar to advise on service development for people with intellectual disabilities. Following meetings with stakeholders, specific recommendations for future service development were made in an unpublished report. The report highlighted the requirement for a significant number of service projects needed and included 12 policy recommendations. Qatar’s strategic plan for children with disabilities improved access to healthcare, with the development of diverse and comprehensive range of services. 6 The National Autism Plan 11 supported children with intellectual disabilities and neurodevelopmental disorders to access educational and health services across mainstream and special educational provisions. Hamad Medical Corporation’s Child Development Centre and the child and adolescent mental health services both provide diagnostic and intervention services for children with intellectual disabilities and other neurodevelopmental disorders. However, the service gap for adults with intellectual disabilities has been a challenge.
Intellectual disability service development
A service development project was established by the mental health service in 2018, following the recruitment of two consultant psychiatrists specialising in intellectual disability, who had experience from working in the UK. The project team initiated the development of community outreach provisions to complement the specialist out-patient clinics. A service plan and referral system was developed in line with the mental health policies. The outreach nursing team was recruited and trained, using a specially developed intellectual disability course delivered by the psychiatrists.
The scope of service was (a) to provide assessment and consultation for patients with intellectual disabilities to meet their health needs; (b) to develop interventions to meet the individual needs; (c) to facilitate development of comprehensive, biopsychosocial, patient-centred, evidenced-based and high-quality care for adults with intellectual disabilities; and (d) to promote recovery and rehabilitation of adults with mental health and behaviours of concern related to intellectual disabiliy, to help them achieve their full potential.
The population of adults with intellectual disabilities and mental health problems or behaviours of concern were triaged for eligibility by the multidisciplinary team. The outreach team provided home treatment for adults with intellectual disabilities who were unable to attend out-patient clinics, using a criteria assessment by the nursing team.
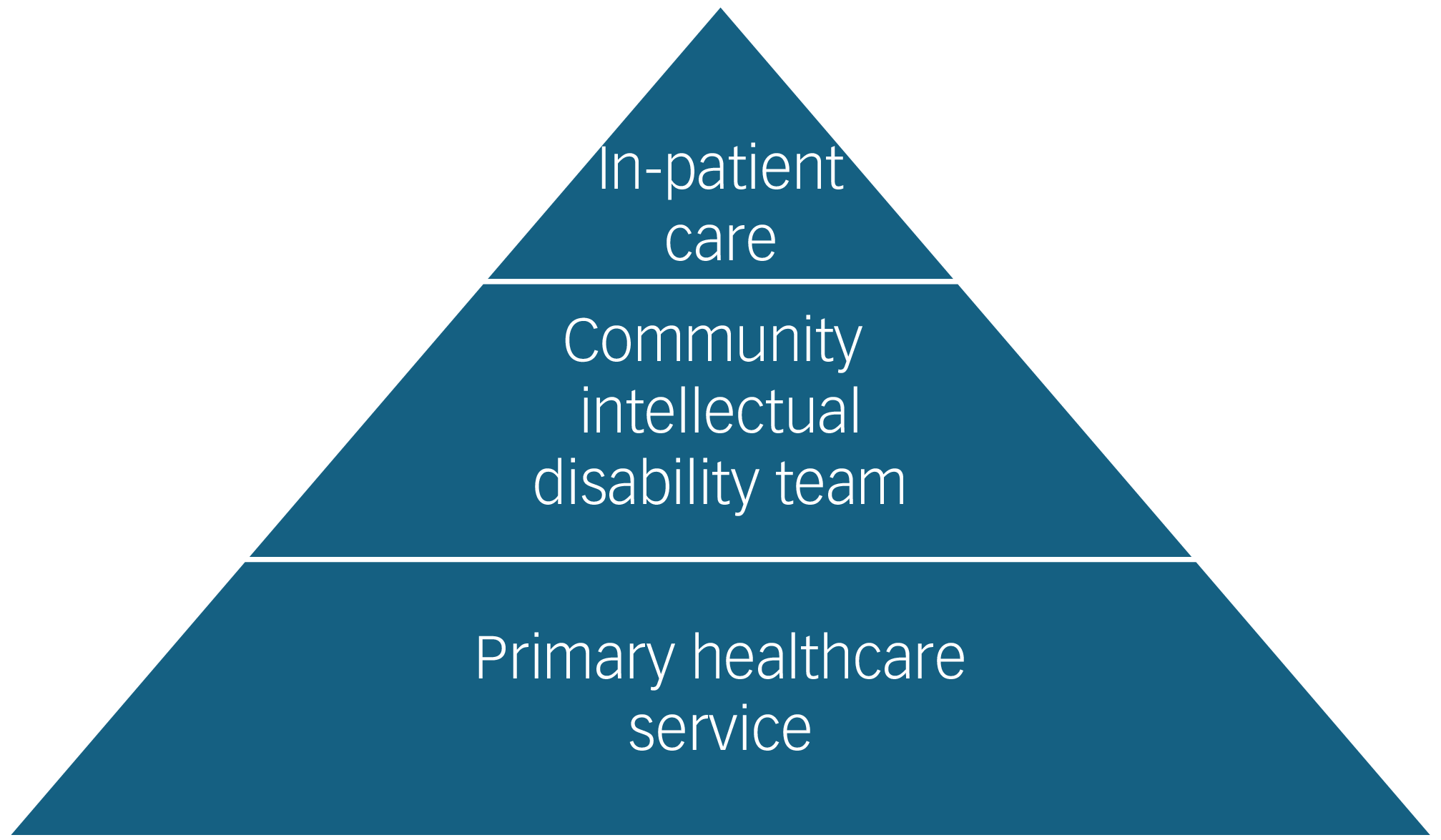
The intellectual disability service operates across different settings, including acute in-patient psychiatric units, out-patient clinics, a community outreach service and liaison with other services. The service model was based on the provision of a tiered model of care as promoted by the World Psychiatric Association. Reference Bhaumik, Kiani, Michael, Gangavati, Khan and Torales12 The service model in Fig. 1 shows the levels of care adopted, and Fig. 2 shows the referral pathway. The clinical team started with two psychiatrists, a head nurse, a charge nurse and seven community nurses, and was later joined by a clinical nurse specialist.
Service model.

Referral pathway. HMC, Hamad Medical Corporation; MDT, multidisciplinary team; MHS, mental health service; OPD, out-patient department; PHCC, primary health care centres; RBMSS, referral booking management system; Sidra, Sidra Medicine.

In the referral pathway, triage was used to ensure adherence to the referral eligibility criteria and management of resources (Fig. 2). Admission and discharge criteria were based on the ability to meet the needs of the patients. Table 1 shows the number of referrals to the service, the number of patients accepted by the outreach team and the number of discharges from the outreach service. The data collected show an increasing number of referrals over time, whereas the team capacity remains unchanged.
Number of referrals to the intellectual disability service

High-risk patients were reviewed to ensure prioritisation and risk mitigation plans were in place. The team uses a flexible approach to meet the needs of the walk-in patients. Table 2 shows the consistent increase in the number of home visits provided by the team over the years, and the increasing capacity and number of clinical appointments made.
Home visits by the intellectual disability outreach team

Secondary outcome
A foundation training programme was developed for the nursing team and a specialist course on the Positive Behaviour Support framework was planned. A continuous development programme to enhance team clinical knowledge was adopted, and a competency-based approach was used to develop nursing skills. The team developed service quality improvement projects and conducted regular clinical audits. Several research projects were completed during the past 4 years, and articles were published in peer-reviewed journals. The service provides opportunities for trainees in psychiatry and is involved in the didactic teaching for the psychiatry residency programme and the clinical teaching of medical students from Qatar University. A fellowship training programme was developed as higher training for psychiatrists, and two trainees joined the programme.
Discussion
Achievements
The achievement of the outreach service in delivering comprehensive assessments and management to meet patient needs is reflected in the increasing number of consultations over the past 5 years (Table 2). Specialist clinical liaison has been provided to support in-patient assessment and management, and facilitate discharge. Patients with intellectual disabilities and behaviours of concern access generic emergency services and are often admitted to in-patient units. Referrals to the service are increasing (Table 1) and are seen through out-patient clinics.
Challenges
In-patient care
In-patient care for adults with intellectual disabilities and comorbid mental health or behaviours of concern is provided in an acute psychiatric hospital ward under the care of untrained staff. Liaison support from the intellectual disability service facilitates assessment and preparation of management plans. However, it has been a challenge to support the development of comprehensive behavioural management plans for those with behaviours of concern.
Community provision
Lack of daytime care provision for adults with intellectual disabilities and behaviours of concern makes it challenging to support the development of behavioural management plans using the Positive Behaviour Support framework.
Support for families
Families rely on expensive private provisions to meet the daytime care needs. The intellectual disability service has limited resources and support from psychology, speech therapy and occupational therapy to meet the increasing demands (Table 2). Social care provision in Qatar is based on providing families with financial support so that they can commission the care they need. However, this support is not available for non-Qataris, who need to rely on their own resources. Lack of respite care for families during times of difficulty often leads to admission to hospital as an alternative. Feedback from patients and families needs exploration through a structured format to enhance future development.
Children’s transition to adult service
The intellectual disability children’s services have been developed with valuable resources, but the transition to adult services is lacking, leading to families feeling frustrated when their adolescents leave the service. Stress levels among families and carers of adults with intellectual disabilities have been reported as high during the transition period. Reference El Tahir, Elhusein, Elamin, Rustom, Reagu and Bedhiaf5 It is challenging to develop single transition plans with scattered children’s services.
Future work to enhance services
Strengthening the current provision with more professionals will help to address some of the challenges. Involvement of stakeholders in developing the strategic action plan for mental health supports the inclusion of intellectual disability projects for future service expansion. Collaboration between health and social care will facilitate a better approach to developing community services that meet the needs of this population.
Professionals’ attitudes and expertise could be enhanced by raising awareness about the needs of intellectual disability population. Hospital’s emergency departments need to adopt a flexible approach to ensure easy access, to meet their needs. Community service expansion with the addition of other professionals will help to meet the increasing demands in the community. National plans with a cross-governmental approach to developing policies to meet health, education, rehabilitation, family affairs, work and pension needs for adults with intellectual disabilities have been recommended, and this needs action. A gap in the diagnostic service for adults with autism spectrum disorders has been considered a priority requiring clinical development according to the Autism National Strategic Action Plan 2025. 11
Conclusions
The mental health service in Qatar developed specialist clinics and an outreach team to meet the needs of adults with intellectual disabilities. The service made significant contribution to improve the mental health needs of adults with intellectual disabilities. However, demands are increasing because of the high number of referrals, with limited resources available. This paper reflected on the achievements and discussed the challenges in the provision of in-patient care, community provision, support for families and transition to adult services. The service needs further enhancement through a collaborative approach between health and other agencies, to improve the care provisions and become an example in the region.
Acknowledgements
We acknowledge the support of colleague Dr James Currie from the Mental Health Service at Hamad Medical Corporation.
Author contributions
M.E.T.: drafting, reviewing and submitting. H.R.: drafting and reviewing.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.




 Open access
Open access
eLetters
No eLetters have been published for this article.