


• Perceived stigma mediates the link between symptom burden and social ties.
• Higher symptom burden leads to increased stigma among cancer patients.
• Stigma negatively affects the quality of social relationships.
• Lung cancer patients report the highest symptom burden and stigma.
• Reducing stigma can help preserve social connectedness in cancer care.
Introduction
Cancer, a global health challenge, significantly impacts not only the physical health of patients but also their psychological and social well-being (Fujisawa and Hagiwara Reference Fujisawa and Hagiwara2015). Despite many treatment options and improved survival rates, cancer continues to be stigmatized in many societies (Vrinten et al. Reference Vrinten, Gallagher and Waller2019). Stigmatization is a process of discrimination and exclusion directed at individuals based on stereotypes, arising from their perceived deviation from societal norms (Goffman Reference Goffman2009). This stigma, stemming from an individual’s health status, is a social process characterized by “exclusion, rejection, blame, and/or devaluation” (Hatzenbuehler et al. Reference Hatzenbuehler, Phelan and Link2013).
Cancer survivors may be exposed to stigmatization in different dimensions. In perceived public stigma, individuals have discriminatory, marginalizing, exclusionary feelings, stereotypes, and behaviors against cancer patients (Koller et al. Reference Koller, Kussman and Lorenz1996). Sensed or perceived stigma occurs when the individual is aware of these prejudices and societal stereotypes toward their disease (Jiang et al. Reference Jiang, Zhang and Zhao2022). In contrast, internalized or self-stigma arises when cancer patients internalize and accept discriminatory stereotypes such as self-blame, shame, depression, and fear of discrimination. Through the indirect effect of social stigmas, internalized stigma leads to psychosocial consequences, including low self-esteem, heightened depressive symptoms, and reduced quality of life in cancer patients (Kao et al. Reference Kao, Lien and Chang2016). Stigmatization in cancer patients has been associated with depression, feelings of inferiority, decreased hope, and a heavy perceived burden (Li et al. Reference Li, Zhang and Hu2024). Recent data show that cancer-related symptoms are determinants of the stigmatization form in cancer patients; physical cancer-related symptoms have been significantly associated with stigma levels across all stages of lung cancer (Johnson et al. Reference Johnson, Schreier and Swanson2019). Furthermore, the side effects of chemotherapy and radiotherapy, such as hair loss and dermatitis, may negatively affect the patient’s physical appearance and potentially exacerbate feelings of stigmatization (Li et al. Reference Li, Zhang and Hu2024).
Beyond individual distress, the experience of stigmatization turns into a social disadvantage for cancer survivors, affecting their social status and social relationships (Hatzenbuehler et al. Reference Hatzenbuehler, Phelan and Link2013). Internalized stigma contributes to feelings of shame and guilt in cancer patients, and they may consider the disease as a punishment and evaluate themselves as inferior to other people (Watt et al. Reference Watt, Suneja and Zimba2023). In the case of “smoker’s guilt” felt by some lung cancer patients or women with sexually transmitted cervical cancer, this onus is heightened (Akin-Odanye and Husman Reference Akin-Odanye and Husman2021). Here, people who are thought to have contributed to the occurrence of cancer with their behavior, experience more stigmatization (Lebel and Devins Reference Lebel and Devins2008). The feeling of shame leads cancer patients to avoid seeking and/or accepting treatment. As a direct consequence of stigmatization, cancer patients are exposed to social exclusion and isolation (Yilmaz et al. Reference Yilmaz, Dissiz and Usluoglu2020; Li et al. Reference Li, Zhang and Hu2024). Social isolation is higher in people with lung and brain cancers depending on the disease severity (Yilmaz et al. Reference Yilmaz, Dissiz and Usluoglu2020). Social isolation and disrupted social ties are among the most prominent consequences of stigma. While other psychosocial domains, such as psychological distress or patient–provider communication, are also important, the quality of social relationships directly demonstrates how stigma shapes patients’ everyday lives. Cancer patients may also withdraw from social relationships and activities due to the fear of being excluded, discriminated against, or judged. This situation causes deterioration in the quality of life in cancer patients (Jiang et al. Reference Jiang, Zhang and Zhao2022; Xu et al. Reference Xu, Gao and Ji2025). Again, cancer patients may experience discrimination, such as rejection from health services, exclusionary treatment, job loss, or being unable to return to work post diagnosis (Akin-Odanye and Husman Reference Akin-Odanye and Husman2021). In the workplace, cancer patients often face discrimination from employers or coworkers (Yilmaz et al. Reference Yilmaz, Dissiz and Usluoglu2020).
All these factors – shame, guilt, social isolation, and discrimination – affect the social relationships of cancer patients. This can result in social withdrawal, avoidance by others, diminished social support, and challenges in communication and disclosure (Akin-Odanye and Husman Reference Akin-Odanye and Husman2021; Lei et al. Reference Lei, Tian and Jin2021; Li et al. Reference Li, Zhang and Hu2024). In contrast, strong social relationships act as a buffer against stigmatization (Lim et al. Reference Lim, Son and Han2024). Similarly, effective communication by healthcare providers may help reduce stigmatization. Therefore, recognizing the role of perceived stigma in social relationships – encompassing family, social environment, and patient–provider communication – is crucial for fostering a supportive environment centered on interpersonal and health communication. Previous studies have examined the effects of stigma on the quality of life and social interactions of cancer patients (Jiang et al. Reference Jiang, Zhang and Zhao2022; Lim et al. Reference Lim, Son and Han2024). However, this study examined how stigma is not limited to these 2 factors but rather plays a mediating role in the impact of cancer-related symptoms on social relationships. The mediation analysis in this study, based on cross-sectional data, does not allow for causal inferences. By elucidating this mechanism, we may provide valuable insights into the psychosocial challenges faced by the cancer patient population in Türkiye and enable the development of targeted interventions to reduce stigma and improve social outcomes for cancer survivors.
Research question
Does perceived stigma mediate the relationship between cancer-related symptoms and social relationships in cancer patients undergoing chemotherapy?
Theoretical framework
Drawing upon Goffman’s conceptualization of interactional stigma and the multilevel “stigma as a fundamental cause” framework proposed by Hatzenbuehler et al. (Reference Hatzenbuehler, Phelan and Link2013), this study explores the interplay between cancer-related symptoms, perceived stigma, and social relationships in everyday life (Goffman Reference Goffman2009; Hatzenbuehler et al. Reference Hatzenbuehler, Phelan and Link2013). According to Goffman, the manifestation of symptoms can amplify the visibility of illness, thereby accentuating the “patient” identity. This, in turn, can engender devaluation and impose limitations on social participation. Hatzenbuehler and colleagues emphasize that stigma is created across structural, interpersonal, and individual levels, and that it contributes to health inequities over time.
Within this broader context, the present analysis focuses on a proximal pathway that can be measured with the available data. As cancer-related symptoms intensify, individuals may anticipate negative judgements or self-blame. This perceived stigma is then likely to weaken social relationships through withdrawal, concealment, and reduced help-seeking (Johnson et al. Reference Johnson, Schreier and Swanson2019; Jiang et al. Reference Jiang, Zhang and Zhao2022). It is therefore hypothesized that 2 associations will be observed: firstly, a negative correlation between symptoms and perceived social relationships; and secondly, a positive correlation between symptoms and perceived stigma. It is further hypothesized that perceived stigma will mediate the relationship between symptoms and social relationships.
Theory also provides a framework for the measurement of each construct. Cancer-related symptoms are captured with validated symptom scores; perceived stigma with instruments assessing anticipated and internalized devaluation relevant to cancer; and social relationships with established measures of network embeddedness and functional support. Despite the fact that our conceptual framing acknowledges the significance of structural stigma, we do not directly observe structural indicators in this dataset. Consequently, the empirical test is situated at the individual/interpersonal level, with the absence of structural measures noted as a limitation. It is recommended that subsequent research incorporates policy and service-environment indicators, in addition to population-attitude measures. This will facilitate the testing of cross-level processes and the evaluation of whether contextual stigma modifies the symptom-perceived-stigma pathway proposed in the current study (Hatzenbuehler et al. Reference Hatzenbuehler, Phelan and Link2013).
Methods
Study design and setting
A descriptive, cross-sectional design was employed. The study was conducted between January and March 2025 at an oncology training and research hospital in Ankara, Türkiye. Before the main data collection began, the instruments were administered to 20 patients who met the inclusion criteria in order to evaluate their clarity, comprehensibility, and simplicity. Based on the feedback received from these patients, no revisions were required. The data obtained from these patients were not included in the final analysis.
Participants
To our knowledge, no similar studies exist, and the literature describing this relationship is therefore, limited. A power analysis was conducted based on the estimated small effect size; a hypothesis testing regression method was utilized, with a 95% confidence interval, a Type I error rate of 0.05, and a power of 0.95. The estimated effect size was set at r 2 = 0.10. The number of independent variables was considered to be 2, namely symptoms and stigma. Based on the power analysis, the minimum required sample size was calculated to be 143. However, to increase the generalizability of the study and ensure the inclusion of diverse patient profiles, the research was completed with 250 participants, taking potential data loss into account.
The inclusion criteria were: (1) 18 years of age or older (2) having received at least 2 cycles of chemotherapy. (3) having Turkish as the native language, and (4) willingness to voluntarily agree to participate in the study.
The exclusion criteria were: (1) individuals with psychosis, severe mental disorders, or inadequate cognitive functioning and (2) individuals who discontinued chemotherapy for any reason during the study.
A total of 32 patients were excluded from the study for not having completed at least 2 sessions of chemotherapy. Additionally, 8 patients were excluded due to language barriers, 13 declined to participate, and 12 were excluded for failing to complete the survey. The study was completed with 250 patients.
Data collection
Four data collection instruments were utilized: (1) Questionnaire Form, (2) Nightingale Symptom Assessment Scale (N-SAS), (3) Cancer Stigma Scale (CSS), and (4) Social Relationship Scale (SRS).
Questionnaire form
This form, developed by the researchers in accordance with the existing literature, comprises 12 questions pertaining to the participants’ sociodemographic characteristics such as age, gender, marital status or education level, and cancer-related factors such as cancer type or year of diagnosis (Yilmaz et al. Reference Yilmaz, Dissiz and Usluoglu2020; Elmokhallalati et al. Reference Elmokhallalati, Alaloul and Shatat2022; Tang et al. Reference Tang, Yusuf and Jia2023). In this questionnaire, participants provided self–perceived ratings of both symptom severity and experienced stigma using separate 0–10 numerical scales. These measures were collected to quantitatively capture participants’ subjective perceptions and to contextualize the descriptive characteristics of the sample. The resulting scores were not used for inferential analyses; rather, they were presented exclusively as descriptive data under Table 2.
Nightingale Symptom Assessment Scale (N-SAS)
The scale, developed by Can and Aydiner (Reference Can and Aydiner2011), to identify symptoms experienced by cancer patients. The scale comprises a total of 38 items, which are distributed across three subdimensions: physical well-being, social well-being, and psychological well-being. The data collection instrument employed a 5-point Likert scale, with responses being assigned the following scores: The scale employed ranged from “0” for no experience, “1” for very little, “2” for a little, “3” for quite a lot, and “4” for very much. The total and subscale scores are calculated by summing the item scores and dividing the result by the number of items. The total score ranges from 1 to 4, with higher scores indicating a higher level of impact from the problems caused by the disease/treatment and a lower general quality of life. The Cronbach’s alpha coefficient of the scale was reported as 0.93 (Can and Aydiner Reference Can and Aydiner2011). In this study, the Cronbach’s alpha value for the Nightingale Symptom Assessment scale (N-SAS) was calculated as 0.97.
Cancer Stigma Scale (CSS)
This scale, originally developed by Cataldo et al. (Reference Cataldo and Brodsky2013) measures the perceived stigma experienced by outpatient lung cancer patients (Cataldo and Brodsky Reference Cataldo and Brodsky2013). Doganavsargil-Baysal et al. (Reference Doganavsargil-Baysal, Senol and Coskun2019) conducted a Turkish validity and reliability study for the short form of the scale (Doganavsargil-Baysal et al. Reference Doganavsargil-Baysal, Senol and Coskun2019). The authors reported that the revised Cataldo Lung Cancer Stigma Scale (CLCSS), consisting of 21 items, is “a valid and reliable scale that can be used for all cancer types.” The scale comprises 3 subdimensions: shame and guilt, social isolation, and discrimination; elevated scores on the scale are indicative of heightened levels of perceived cancer stigmatization among patients. The Cronbach’s alpha coefficient of the scale was reported as 0.89 (Doganavsargil-Baysal et al. Reference Doganavsargil-Baysal, Senol and Coskun2019). In this study, the Cronbach’s alpha value for the CLCSS was calculated as 0.96.
Social Relationship Scale (SRS)
This scale, developed by Köse et al. (Reference Köse, Özgür and Coşgun2020), is composed of three subdimensions: family relations, kinship/neighbourhood relations, and friendship relations, with a total of 10 items (Köse et al. Reference Köse, Özgür and Coşgun2020). The items are evaluated using a 5-point Likert scale, ranging from “Very distant (1)” to “Very close (5).” The total score on the scale is derived by calculating the sum of the item scores and dividing this by the number of items in the scale. Scores on this scale range from 1 to 5, with higher scores indicating the presence of close social relationships. The Cronbach’s alpha coefficient of the scale was reported as 0.79 (Köse et al. Reference Köse, Özgür and Coşgun2020). In this study, the Cronbach’s alpha value for the SRS was calculated as 0.82.
Ethical considerations
The necessary ethics committee approval for conducting the research was obtained from the Ankara Yıldırım Beyazıt University Health Sciences Ethics Committee (01.07.2024-06/802). Following ethics committee approval, research permission was granted by the hospital where the study was to be carried out. Participants were informed about the purpose and significance of the study. A voluntary consent form was provided to the subjects, and both written and verbal consent were obtained. Participants were assured that their responses would remain confidential, that data would be anonymized and stored securely, and that only the research team would have access to the data. They were also informed of their right to withdraw from the study at any time without any negative consequences. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Statistical analysis
All statistical analyses were performed using IBM SPSS v27.0 and DataTab web-based analysis platform. Descriptive statistics were used to summarize sample characteristics. Prior to conducting parametric tests, the normality of continuous variables was assessed using the Kolmogorov–Smirnov and Shapiro–Wilk tests. Primary mediation model, exploratory subgroup analyses were conducted to examine potential differences in perceived stigma, cancer-related symptoms, and social relationships across demographic and clinical variables (e.g., education, marital status, cancer type). For normally distributed data, parametric tests were used (independent sample t-test, one-way ANOVA with post-hoc analyses), while for non-normally distributed data, non-parametric tests were applied (Mann–Whitney U test, Kruskal–Wallis test with Dunn’s post-hoc comparisons). Pearson’s correlation analysis was conducted to evaluate relationships between continuous variables. Mediation analysis was also performed to examine the indirect effect of cancer-related symptoms on social relationships through stigma perception. For the mediation analysis, data obtained from the N–SAS, the SRS, and the CSS were used. The 0–10 self–perceived stigma and symptom severity ratings were presented only within the descriptive findings (Table 1). These ratings were analyzed solely to provide a quantitative representation of participants’ subjective perceptions and to contextualize the descriptive characteristics of the sample. A p-value < .05 was considered statistically significant.
Sociodemographic and disease-related characteristics of patients

Results
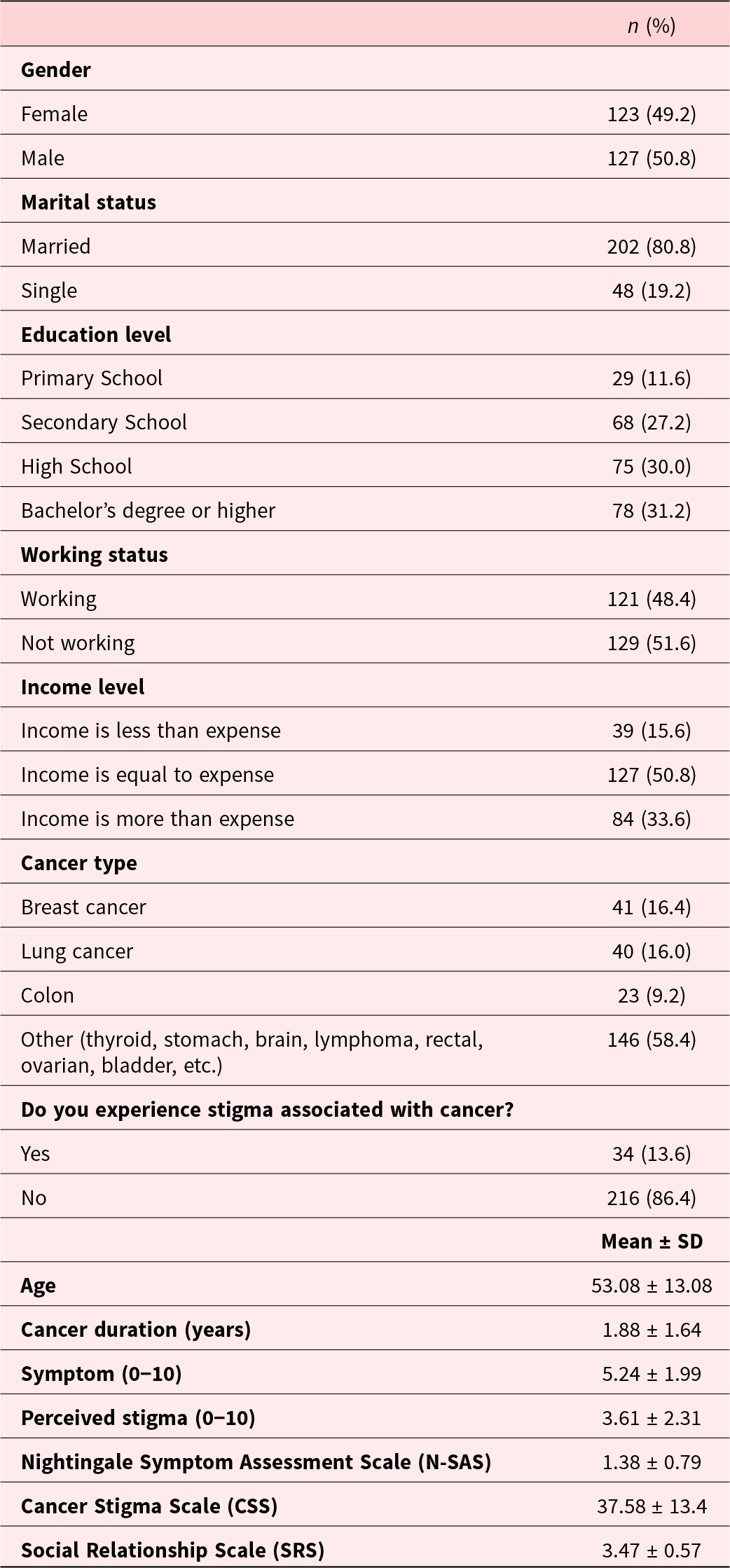
Table 1 presents the sociodemographic and disease-related characteristics of the study participants. A total of 250 patients were included in the study, with a near equal gender distribution. The majority of participants were married (80.8%), and 31.2% had attained a bachelor’s degree or higher. With respect to employment status, 48.4% of participants were currently working, while 51.6% were not working. Regarding income level, 50.8% of participants reported an income equal to their expenses, while 33.6% indicated that their income exceeded their expenses, and 15.6% stated their income was insufficient to cover their expenses. The most prevalent cancers diagnosed in participants were breast cancer (16.4%) and lung cancer (16.0%), while 58.4% of participants had other cancer types, including thyroid, stomach, brain, lymphoma, rectal, ovarian, and bladder cancer. With regard to cancer-related stigma, 13.6% of participants reported experiencing stigma, whereas 86.4% did not perceive stigma associated with their diagnosis. The mean age of the participants was 53.08 years (± 13.08 years), with an average cancer duration of 1.88 years (± 1.64 years). The mean symptom severity score (on a 0–10 scale) was 5.24 ± 1.99, while the mean perceived stigma score was 3.61 ± 2.31. The mean scores with standard deviations for the N-SAS, CSS, and SRS were 1.38 ± 0.79, 37.58 ± 13.4, and 3.47 ± 0.57, respectively.
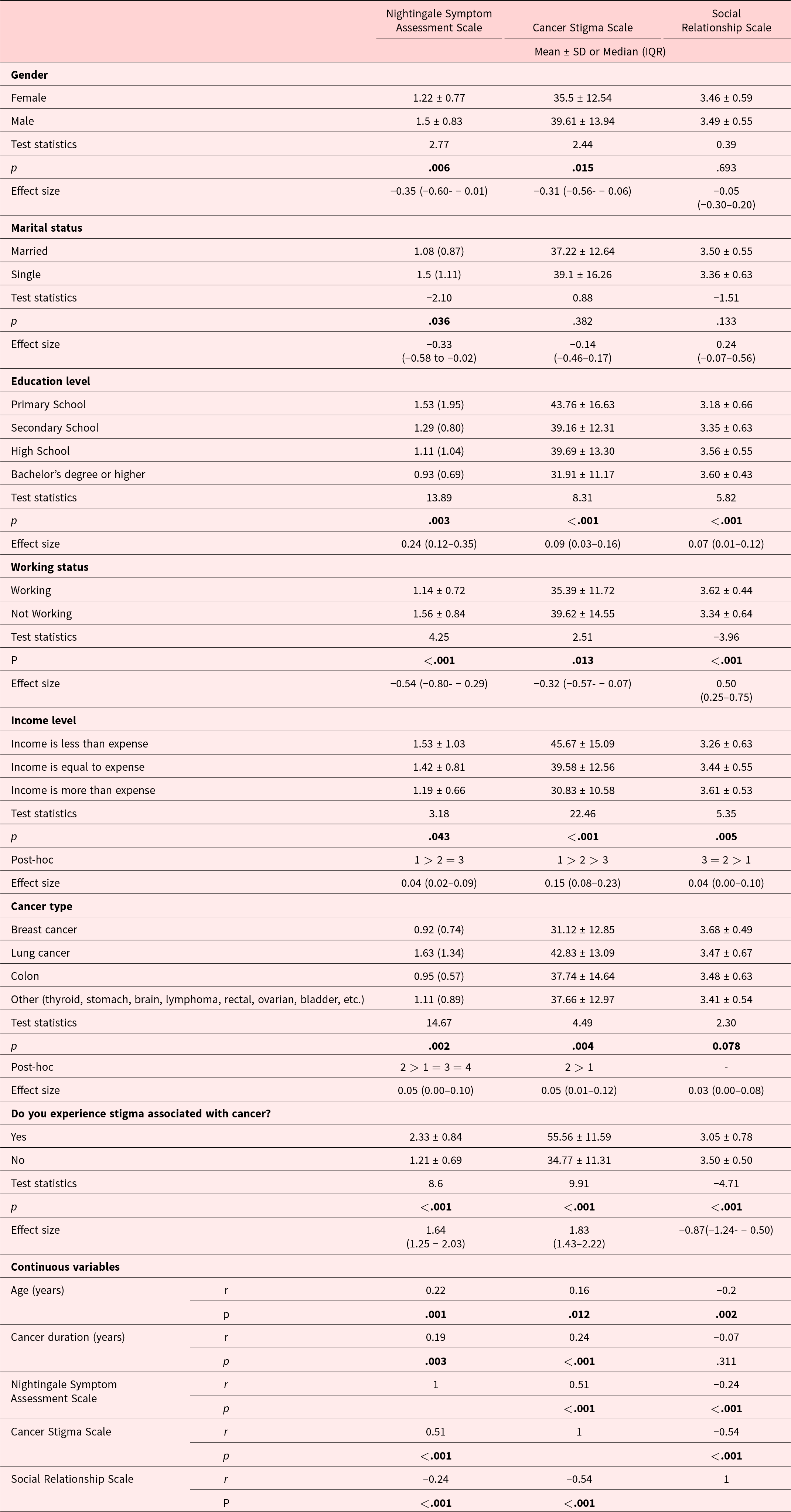
Table 2 presents a comparison of cancer-related symptoms (N-SAS), stigma perception (CSS), and social relationships (SRS) across various sociodemographic and disease-related variables.
Comparison of the mean scores of N-SAS, CSS, and SRS between groups

The analysis showed that males reported a significantly higher cancer-related symptoms (p = .006) and stigma perception (p = .015) than females, while no significant difference was observed in social relationship scores (p = .693). Single individuals had significantly higher cancer-related symptoms compared to married individuals (p = .036), although stigma perception and social relationship scores did not differ significantly by marital status.
Education level significantly affected all 3 outcomes. Participants with higher education levels had lower cancer-related symptoms (p = .003), lower stigma perception (p < .001), and better social relationships (p < .001). Post-hoc analysis showed that individuals with a bachelor’s degree or higher had significantly more favorable scores on all scales compared to those with lower education levels.
Participants who were not working reported significantly higher cancer-related symptoms (p < .001), higher stigma perception (i = .013), and lower social relationship scores (p < .001) than those who were employed.
Income level also showed a significant association with all outcomes. Those with lower income levels reported higher cancer-related symptoms (p = .043), greater stigma perception (p < .001), and poorer social relationships (p = .005). Post-hoc comparisons indicated that participants whose income was less than their expenses had significantly worse outcomes compared to those with equal or greater income.
Patients with lung cancer exhibited the highest cancer-related symptoms (p = .002) and stigma perception (p = .004). Post-hoc analysis revealed significantly higher cancer-related symptoms in lung cancer patients compared to other cancer types, and higher stigma perception in lung cancer patients compared to breast cancer patients. However, social relationship scores did not differ significantly across cancer types (p = .078).
Patients who reported experiencing stigma related to cancer had significantly higher cancer-related symptoms (p < .001) and stigma perception (p < .001), along with significantly lower social relationship scores (p < .001) compared to those who did not perceive stigma.
A positive correlation was found between age and both cancer stigma (r = 0.16, p = .012) and cancer-related symptoms (r = 0.22, p = .001), while age was negatively correlated with social relationship scores (r = −0.2, p = .002). Cancer duration was positively associated with cancer-related symptoms (r = 0.19, p = .003) and stigma perception (r = 0.24, p < .001), but not significantly correlated with social relationships (p = .311).
Cancer-related symptoms showed a strong positive correlation with stigma perception (r = 0.51, p < .001), and a moderate negative correlation with social relationships (r = −0.24, p < .001). Similarly, stigma perception was strongly negatively associated with social relationships (r = −0.54, p < .001), indicating that increased cancer-related symptoms and stigma perception are linked with weakened social connections.
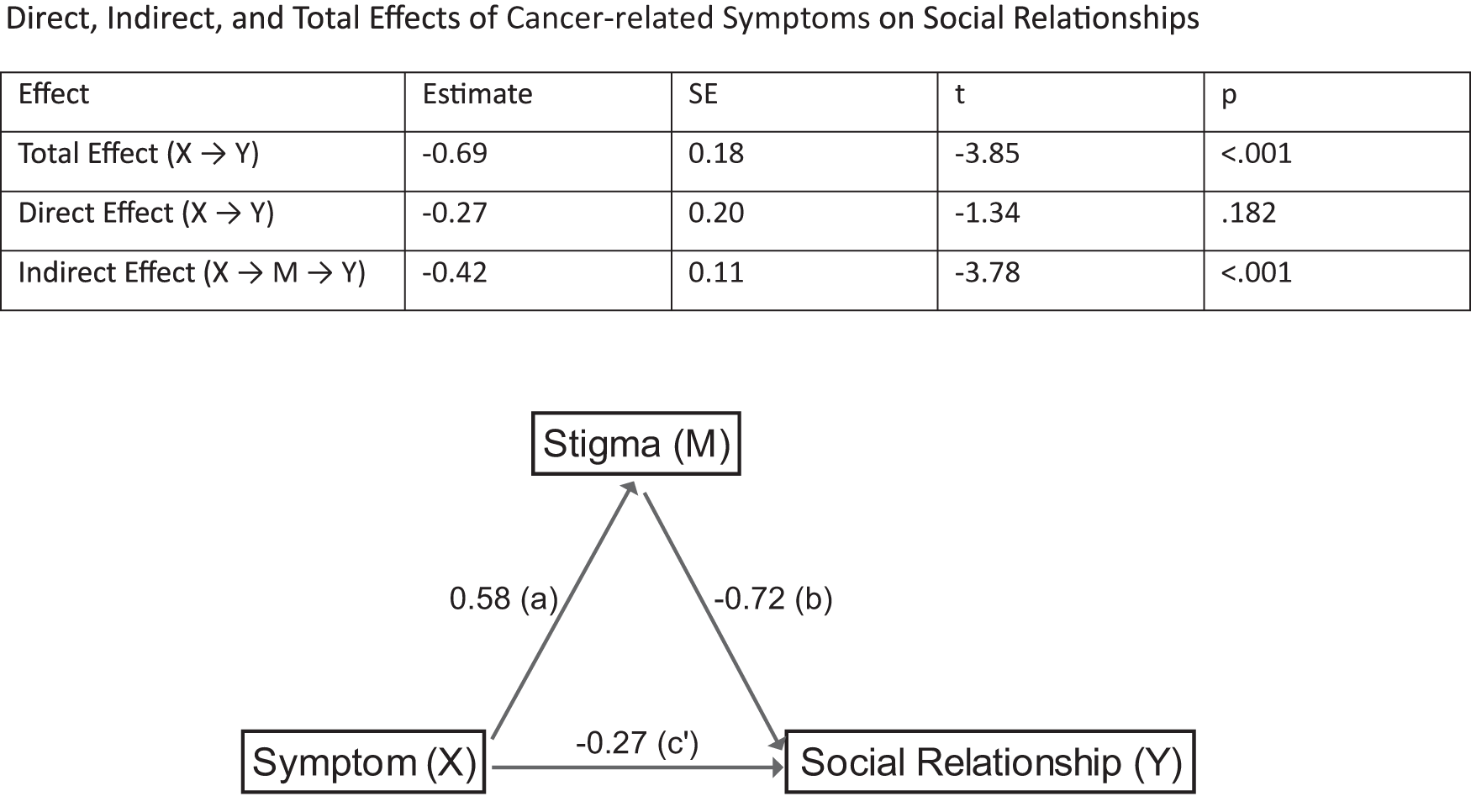
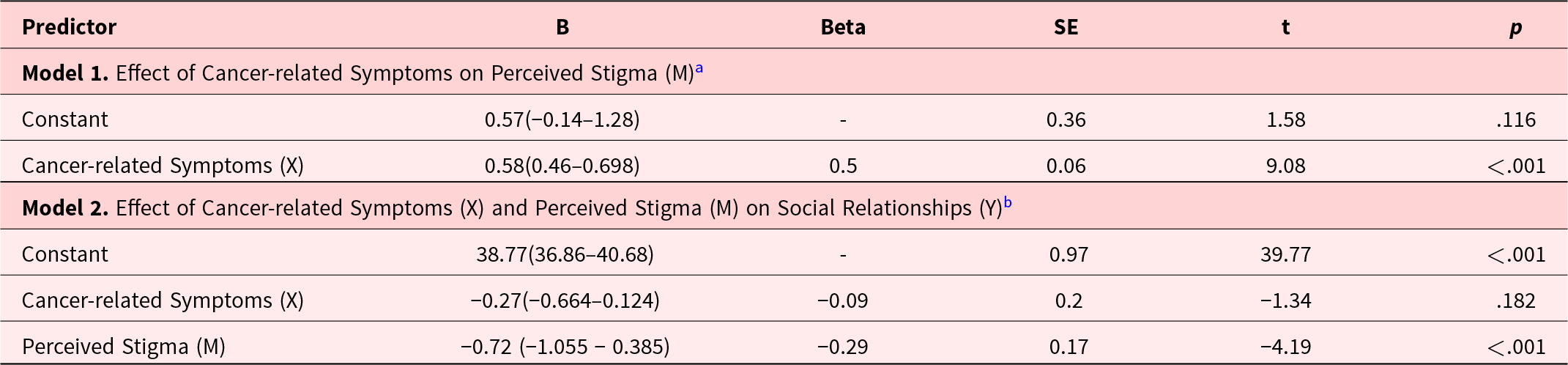
The mediation analyses indicate that cancer-related symptoms significantly predicts perceived stigma (B = 0.58, p < .001), explaining 25% of the variance in stigma perception (R 2 = 0.25) (Figure 1). This finding suggests a positive correlation between heightened cancer-related symptoms and increased perceived stigma. In the subsequent regression model, both cancer-related symptoms and perceived stigma were included as predictors of social relationships. The mediation analysis revealed a significant negative relationship between perceived stigma and social relationships (B = −0.72, p < .001), while the direct effect of cancer-related symptoms alone did not reach statistical significance (B = − 0.27, p = .182) (Figure 1). The model accounted for 12% of the variance in social relationships (R 2 = 0.12). The total effect of cancer-related symptoms on social relationships was found to be significant (B = −0.69, p < .001); however, the direct effect was not (B = −0.27, p = .182) (Table 3). The indirect effect mediated by perceived stigma was statistically significant (B = –0.42, p < .001), indicating that perceived stigma mediates the association between cancer–related symptoms and social relationships in this sample. This mediation effect should be interpreted within the analytical conditions of the present study, as no adjustments for potential confounders were applied. These findings underscore the pivotal role of stigma in associating cancer-related symptoms with social relationship challenges, thereby suggesting that interventions targeting stigma reduction may help mitigate the adverse social consequences of cancer-related symptoms.
Mediator analysis on symptom, stigma and social relationship.

Mediator Analysis Results

a Model Summary: R = 0.50, R2 = 0.25, Adjusted R2 = 0.25, F(1,248) = 82.43, p < .001
b Model Summary: R = 0.35, R2 = 0.12, Adjusted R2 = 0.11, F(2,247) = 16.69, p < .001
Discussion
This study found that perceived stigma may statistically mediate the association between cancer-related symptoms and social relationships among cancer patients. Although an elevated cancer-related symptom was initially observed to be associated with a disruption to social connections, this relationship appeared to be partly explained by stigma. The results of this study highlight that stigma may represent a potential pathway influencing social well-being in the context of oncology care. However, given the cross-sectional design, these associations should be interpreted as correlational rather than causal, and further longitudinal or experimental research is required to confirm causality.
The mean age of the participants was 53.08 ± 13.08 years, which is consistent with the global epidemiological data (Sung et al. Reference Sung, Ferlay and Siegel2021) and aligns with the findings of previous studies conducted on individuals diagnosed with cancer (Yilmaz et al. Reference Yilmaz, Dissiz and Usluoglu2020). In this study, breast and lung cancers were the most prevalent types, which is also consistent with global prevalence patterns as documented by Sung et al. (Reference Sung, Ferlay and Siegel2021).
Our findings emphasize the relationship between perceived stigma and social relationships. However, considering Hatzenbuehler’s structural stigma theory, it is important to acknowledge that not only individual perceptions but also societal-level policies, norms, and practices play a significant role. It is noteworthy that a relatively modest yet significant proportion (13.6%) of participants reported encountering cancer-related stigma. As highlighted in the extant literature, the repercussions of cancer stigma on patients’ well-being, empowerment, and capacity to seek social support represent a pivotal aspect within their patient experience (Watt et al. Reference Watt, Suneja and Zimba2023). The results of the current study underscore the importance of targeted interventions designed to address cancer-related stigma and to provide support to patients in terms of their psychosocial well-being.
The findings of the study demonstrated that male subjects exhibited significantly higher levels of cancer-related symptoms (p = .006) and stigma perception (p = .015) in comparison to female subjects. However, earlier research has found no significant gender differences in the cancer-related symptoms experienced by cancer patients (Elmokhallalati et al. Reference Elmokhallalati, Alaloul and Shatat2022), yet the higher levels of stigma perception observed in men are consistent with existing literature suggesting that men experience greater cancer-related stigma than women (Huang et al. Reference Huang, Yu and Wu2021; Gershfeld-Litvin et al. Reference Gershfeld-Litvin, Halabi and Bellizzi2023). This situation can be explained within the context of Turkey’s gender roles and masculinity norms. In the patriarchal structure of Turkish society, masculinity is identified with qualities such as courage, strength, success, and being in control (Yeniasır and Gökbulut Reference Yeniasır and Gökbulut2020). The expression of emotions by men, such as showing sadness or crying, is not considered socially acceptable. This “restricted emotionality” can hinder men from seeking emotional and social support, even from their spouses (Tekke et al. Reference Tekke, Ghani and Kassim2020). Furthermore, men hold more negative attitudes towards seeking psychological support compared to women (Koydemir-Özden Reference Koydemir-Özden2010). Consequently, the pressure of the prevailing “strong, self-sufficient man” ideal in Turkish society reduces men’s help-seeking behaviors and weakens their coping strategies for health problems, which may lead to a higher perception of stigma. Moreover, the present study has indicated that individuals diagnosed with breast cancer reported the lowest cancer-related symptoms and perceived stigma in comparison with those diagnosed with lung cancer, colon cancer, and other types. Breast cancer is a prevalent condition that predominantly affects the female population. It was assumed by the researchers that gender disparities in cancer types might contribute to differences in both the cancer-related symptoms and the perception of stigma.
The present analysis reveals a significant association between single status and elevated cancer-related symptoms, with a p-value of .036. This finding contrasts with married individuals, who exhibited lower cancer-related symptoms. A substantial body of research has repeatedly identified marital status as a significant prognostic factor in cancer outcomes. In general, the survival rate of married cancer patients is higher than that of unmarried patients. This phenomenon has been observed in various types of cancer, including breast, prostate, gastric and non-small cell lung cancer (Aizer et al. Reference Aizer, Chen and Mccarthy2013; Jin et al. Reference Jin, Wang and Dai2016; Shi et al. Reference Shi, Qu and Lu2016; Liu et al. Reference Liu, Wang and Yang2019; Chen et al. Reference Chen, Yin and Zheng2020). Culturally, the concept of family in Türkiye possesses a close-knit and collectivistic structure, encompassing not only the nuclear family (spouse and children) but also extended family members such as spouses’ mothers, uncles, and aunts. In this context, the Turkish family structure emerges as a critical social support mechanism in coping with problems (Koydemir-Özden Reference Koydemir-Özden2010).
On the other hand, single men are often characterized by negative attributes such as being irresponsible, profligate, and weak. Studies conducted on this topic in Türkiye have revealed that perceived social support from a spouse and family exhibits a buffering effect on psychological problems, physical adjustment, and quality of life. Patients who receive high levels of family support report feeling less loneliness and experiencing lower levels of hopelessness, which facilitates adjustment to the illness and enhances the quality of life (Pehlivan et al. Reference Pehlivan, Ovayolu and Ovayolu2012). Conversely, it has been determined that cancer patients living alone in Türkiye have lower levels of perceived social support (Yilmaz et al. Reference Yilmaz, Piyal and Akdur2017). Furthermore, the social support provided by a spouse has been shown to enhance healthcare-seeking behavior and improve adherence to treatment protocols (Aizer et al. Reference Aizer, Chen and Mccarthy2013; Jin et al. Reference Jin, Wang and Dai2016; Liu et al. Reference Liu, Zhong and Zhang2020; Zhu and Lei Reference Zhu and Lei2023). Married patients are more likely to receive definitive therapies, such as surgery, chemotherapy, and radiotherapy, which are critical for improving survival. The efficacy in reducing the psychological burden of cancer has been demonstrated, with the potential to mitigate the severity of symptoms and enhance quality of life (Aizer et al. Reference Aizer, Chen and Mccarthy2013; Jin et al. Reference Jin, Wang and Dai2016; Liu et al. Reference Liu, Zhong and Zhang2020). Our findings are consistent with the relevant literature in this respect.
The present study found educational level to be significantly associated with all three outcomes. Participants with higher levels of education reported a lower cancer-related symptoms (p = .003), lower perceptions of stigma (p < .001), and better social relationships (p < .001). Individuals who have received higher levels of education have been shown to report reduced cancer-related symptoms. This may be attributed to increased access to healthcare resources, enhanced symptom management knowledge, and a more sophisticated ability to navigate the healthcare system effectively (Badger et al. Reference Badger, Segrin and Crane2023). Moreover, education has been demonstrated to serve as a protective factor against stigma (Tan et al. Reference Tan, Zhong and Mei2022; Tang et al. Reference Tang, Yusuf and Jia2023). Patients who have obtained a higher level of education frequently possess a more profound comprehension of the illness, which can assist in the dispelling of myths and the mitigation of internalization of negative stereotypes. Furthermore, an association has been demonstrated between higher education and the establishment of robust social networks and enhanced social support, both of which have been identified as being pivotal to coping with the emotional and physical challenges associated with cancer (Coleman et al. Reference Coleman, Hurtado-De-Mendoza and Montero2024). The findings, when considered collectively, suggest that education play an instrumental role in shaping the experience of cancer, exerting an impact not only on health outcomes but also on social and emotional well-being.
The present study found that unemployed participants and those with lower income levels exhibited a significantly higher prevalence of symptoms, stronger perceived cancer-related stigma, and weaker social relationships when compared with their respective control groups. These findings align with previous research indicating that unemployment and lower income levels are linked to increased cancer-related stigma (Yilmaz et al. Reference Yilmaz, Dissiz and Usluoglu2020; Huang et al. Reference Huang, Yu and Wu2021) and an exacerbated cancer-related symptoms (Elmokhallalati et al. Reference Elmokhallalati, Alaloul and Shatat2022). Whilst some studies have indicated that employed patients may encounter elevated levels of stigma due to increased social exposure (Tang et al. Reference Tang, Yusuf and Jia2023), the present results suggest that both unemployment and reduced income may contribute to constrained access to supportive resources and heightened psychosocial stress. This may in turn exacerbate cancer-related symptoms, perceived stigma, and disruption in social relationships among cancer patients.
With regard to specific types of cancer, those suffering from lung cancer demonstrated the highest levels of both cancer-related symptoms (p = .002) and stigma perception (p = .004). Lung cancer patients commonly exhibit a multitude of co-occurring symptoms, encompassing a wide spectrum of physical and psychological manifestations. These include, but are not limited to, fatigue, dyspnea, pain and insomnia. The collective manifestation of these symptoms is associated with considerable cancer-related symptoms (Vogt et al. Reference Vogt, Beyer and Sistermanns2021). The heightened levels of cancer-related symptoms experienced by such patients may further intensify their perceptions of stigma, as they may view themselves as more vulnerable due to their physical limitations and associated symptoms.
Cancer patients are exposed to different levels and forms of perceived stigmatization. Perceived stigmatization and psychological distress are especially high in lung cancer patients with higher survival rates compared to other cancers (Lehto Reference Lehto2014). Studies show that 1 out of every 4 lung cancer patients experiences depression or psychosocial problems (Carlsen et al. Reference Carlsen, Jensen and Jacobsen2005). In this regard, lung cancer patients feel a heavy perceived stigma as lung cancer is strongly associated with smoking behavior in society (Lehto Reference Lehto2014). Cataldo et al. (Reference Cataldo, Jahan and Pongquan2012) found that lung cancer patients, whether smokers or non-smokers, felt similar levels of perceived stigma and that this was associated with depression and impaired quality of life (Cataldo et al. Reference Cataldo, Jahan and Pongquan2012). In a qualitative study, Chapple et al. (Reference Chapple, Ziebland and Mcpherson2004) also found that lung cancer patients, whether smokers or non-smokers, felt guilt and shame due to smoking-related stigma in the community (Chapple et al. Reference Chapple, Ziebland and Mcpherson2004). This indicates a social mechanism of perceived stigma that is independent of smoking behavior. On the other hand, perceived or internalized stigma behaviors of individuals may vary according to smoking status. More internalized stigma was found in patients who had recently quit smoking (Hamann et al. Reference Hamann, Ostroff and Marks2014). Similarly, perceived or internalized stigma was found to be higher in smokers or recent smokers compared to never smokers (Williamson et al. Reference Williamson, Kwon and Riley2020). Additionally, the elevated stigma perception among lung cancer patients may be influenced by internalized guilt stemming from previous tobacco use. Research has shown that the psychological distress and stigma experienced by smokers are often aggravated by feelings of guilt and shame related to smoking (Webb et al. Reference Webb, Kane Mcdonnell and Arp Adams2019; Lebel and Devins Reference Lebel and Devins2008). This phenomenon can be attributed to patients attributing their illness to their own behaviors, thereby exacerbating the stigma they experience. It is recommended that further studies be conducted in order to ascertain the relationship between previous tobacco use and self-blaming among lung cancer patients.
The present study demonstrates that as individuals age, they are more likely to experience heightened cancer-related symptoms (r = 0.22, p = .001) and an increased sense of stigma (r = 0.16, p = .012). Simultaneously, a decline in social relationships (r = −0.2, p = .002) is often observed with advancing age. This finding is consistent with prior research, which has highlighted the distinct challenges faced by older cancer survivors. With advancing age, there is an increased probability of concomitant health conditions and an elevated risk of social isolation; these factors may potentially exacerbate both the severity of symptoms and the psychological impact of the disease (Badger et al. Reference Badger, Segrin and Crane2023). Furthermore, the perception of illness and the ageing process itself has the capacity to influence the management of symptoms and the overall perception of quality of life in older adults (Osmialowska et al. Reference Osmialowska, Stas and Chabowski2022). In the context of stigma, younger patients, particularly those diagnosed with advanced cancer, frequently encounter unique social and emotional pressures. A significant proportion of this population is currently engaged in either the process of establishing their careers or forming interpersonal connections. It has been observed that the experience of a serious illness during this phase of life when younger patients may be in the process of establishing their careers and forming interpersonal connections, can contribute to feelings of stigma and disconnection from one’s peers (Sun et al. Reference Sun, Pang and Lee2023). In contrast, older adults may internalise stigma in a different manner, perhaps shaped by experiences of frailty, loss of independence, or other age-related changes. In both groups, factors such as depression and self-esteem appear to influence how stigma is experienced. Furthermore, social relationships are known to evolve in different ways across different age groups. As demonstrated by Sun et al. (Reference Sun, Pang and Lee2023), younger individuals may encounter difficulties in sustaining close relationships, owing to the disruption that illness can cause (Sun et al. Reference Sun, Pang and Lee2023). Conversely, older adults may become susceptible to social isolation due to physical limitations or life transitions, such as retirement or menopause (Zhang et al. Reference Zhang, Wei and Zhang2025). Regardless of age, it is evident that robust social support functions as a significant mitigating factor against stigma, thereby enhancing both emotional well-being and quality of life (Tang et al. Reference Tang, Yusuf and Jia2023; Li et al. Reference Li, Zhang and Hu2024). Further longitudinal and stratified research is warranted to more precisely elucidate the interplay between age, cancer-related symptoms, perceived stigma, and social functioning in individuals with cancer.
This study highlights the strong negative correlation between perceived stigma and social relationships (r = −0.54, p < .001), emphasizing that cancer-related stigma weakens social relationships. According to the findings, increased cancer-related symptoms and stigma in individuals with cancer are associated with weakened ties with family, friends, and broader social networks. There are studies in the literature that parallel our findings (Mohabbat-Bahar et al. Reference Mohabbat-Bahar, Bigdeli and Mashhadi2017; Kang et al. Reference Kang, Kim and Kim2020). A qualitative study examining stigma in individuals with cancer also highlights that patients limit their self-expression, restrict social interaction, and withdraw from social relationships to avoid shame and negative evaluation (Mohabbat-Bahar et al. Reference Mohabbat-Bahar, Bigdeli and Mashhadi2017). The erosion of social relationships can weaken access to emotional and functional support, thereby increasing the negative effects of both symptoms and stigmatization. This indicates that multidisciplinary teams working in oncology should go beyond the individual symptom management of cancer patients and include targeted efforts aimed at rebuilding and protecting their social networks.
To the best of our knowledge, this is the first study report that perceived stigma statistically mediated the relationship between cancer patients’ perceived cancer-related symptoms and their social relationships. Specifically, the cancer-related symptoms exhibited a significant indirect effect on social relationships via stigma (B = −0.42, p < .001), while the direct effect of cancer-related symptoms proved to be statistically insignificant (B = −0.27, p = .182), thereby indicating a statistical mediation in this model. These findings suggest that deterioration in patients’ social ties may not only reflect the physical impact of cancer symptoms, but may also be reflection of the psychosocial interpretation of those symptoms, particularly in terms of perceived stigma. One potential explanation for this mediating pathway is to be found in the visibility and interpretation of symptoms. Cancer-related symptoms, including but not limited to hair loss, fatigue, and weight changes, have been shown to function as social signals of illness. These symptoms have the potential to attract unwanted attention, evoke feelings of pity or judgment, and reinforce patients’ sense of being “different” or “marked.” This may result in the internalization of negative societal attitudes, a more pessimistic interpretation of social interactions, and a gradual withdrawal in order to avoid potential rejection. It is important to note that, over time, such avoidance behaviors and internalized beliefs may erode the patient’s social network, even if the initial cancer-related symptoms diminish. These findings highlight the potential value of multidimensional cancer care that addresses the physical, emotional, and social consequences of treatment in a simultaneous and integrated manner. However, symptoms, stigma, and social relationships are complex phenomena that may be influenced by various confounding factors not fully accounted for in the present study. Therefore, further research is warranted to examine how potential confounders may shape this relationship.
There is currently no national policy or standardized practice aimed at reducing cancer-related stigma among patients in Türkiye. Despite the existence of limited efforts to address this issue, which primarily consist of specific, restricted initiatives carried out by non-governmental organizations (NGOs) focusing on breast cancer and HIV-positive individuals, further research is required in this area. (Akyürek and Kalaycı Reference Akyürek, Kalaycı, E., M. and M. D.2022). Consequently, there is a clear need in Türkiye to integrate psychosocial support comprehensively into the treatment protocol for cancer patients and to provide awareness training for healthcare professionals, particularly nurses. Furthermore, public service announcements must be developed to counter social stigma and discrimination, and the dissemination of health communication courses aimed at university students should be encouraged. The central role of the family within Turkish society suggests that integrating family-based interventions could have a positive effect on the social isolation experienced by cancer survivors. The preservation of patients’ social relationships may function as a protective buffer, being associated with enhanced resilience, psychological well-being, and, in some cases, treatment outcomes.
Limitations
Despite the contributions of this study, several limitations should be acknowledged. The cross-sectional design restricts causal inferences. Given this design, the findings presented here strictly represent correlations and potential associations rather than confirmed developmental or causal pathways between age, cancer-related symptoms, perceived stigma, and social functioning.
Another limitation concerns the use of self-report instruments, which may be subject to social desirability bias and self-perception errors. Participants may have underreported or overreported their symptoms, perceived stigma, or quality of social relationships due to personal or cultural sensitivities. Moreover, psychological comorbidities – particularly depression and anxiety – were not controlled for in this study. The Social Relationship Scale provides valuable insights into the role of family, kinship, and friendship in the social dynamics of cancer survivors, but it does not address other important social dynamics such as workplace and community relationships. In the Turkish context, interactions with coworkers, neighbors, and members of the wider community can influence the experience of stigmatization. Therefore, this scale may underestimate the full social impact of cancer-related stigmatization.
Additionally, the study was conducted in a single hospital setting, which may limit the generalizability of the findings to other cancer patient populations. Future research could explore longitudinal effects of stigma and cancer-related symptoms and include more diverse healthcare settings. It is recommended that further studies be conducted in larger populations. Another limitation is that the Cancer Stigma Scale was originally developed for lung cancer patients. Although the Turkish adaptation study has demonstrated its validity and reliability across all cancer types, further psychometric evaluations in different cancer groups would help to strengthen its broader applicability. Another limitation is that the mediation analysis was conducted without adjusting for potential confounding factors such as depression, disease stage, or treatment type. The absence of these controls may have influenced the observed associations, and future studies should address this by incorporating relevant covariates into the analytic models.
Conclusion
The study revealed that perceived stigma mediates the relationship between cancer-related symptoms and social relationships in cancer patients undergoing chemotherapy. Specifically, cancer-related symptoms significantly increased the perception of stigma, which in turn negatively impacted social relationships. These findings highlight the crucial role of stigma in shaping the psychosocial well-being of individuals with cancer and emphasize the need for comprehensive care models that address both physical and psychosocial aspects of illness. Addressing stigma appears vital to improving social interactions, psychological resilience, and overall quality of life. Healthcare professionals should be cognizant that patients experiencing more severe cancer-related symptoms may also struggle with reduced social connectedness, a condition indirectly shaped by perceived stigma. Therefore, psychosocial interventions should consider both the direct and indirect effects of cancer-related symptoms on social functioning.
Future research should employ longitudinal and intervention-based designs to clarify causal pathways and test the effectiveness of stigma-reduction strategies. Additionally, culturally sensitive approaches to assessing and addressing stigma are needed to capture how these dynamics manifest across different healthcare and societal contexts. Such work will validate and extend the current findings while guiding the development of tailored, evidence-based interventions that enhance social functioning and psychological well-being in cancer care.
In Türkiye, there is currently no systematic national policy aimed at reducing stigma among cancer patients. Therefore, cancer treatment protocols – both in Türkiye and globally – should be redefined through a biopsychosocial perspective that integrates physical, psychological, and social dimensions of care. Expanding psychosocial support opportunities within oncology services is crucial to ensure holistic and equitable cancer care.
Availability of data and materials
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We would like to express our sincere gratitude to the cancer patients who voluntarily agreed to participate in this study. The authors would like to express their gratitude to Professor Annie Young for her invaluable contribution and supervision during the writing and editing process of the paper.
Author contributions
T.B.: Writing – original draft, Conceptualization, Methodology, Data curation, Supervision; I.T.: Writing – original draft, Conceptualization, Formal analysis, Methodology, Supervision; Y.Ş: Writing – original draft; E.V.: Conceptualization, Writing – original draft; E.A.: Conceptualization, Writing – review & editing, Supervision; A.D.: Conceptualization, Data curation. All authors read and approved the final manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
The necessary ethics committee permission to perform the research was obtained from the Ankara Yıldırım Beyazıt University Health Sciences Ethics Committee (06/802). Following this approval, institutional permission was secured from the hospital where the study was conducted. Participants were informed about the purpose and significance of the study, and both written and verbal informed consent was obtained. The study was conducted in accordance with the principles outlined in the 2024 revision of the Declaration of Helsinki.
Consent for publication
Not applicable.

 Open access
Open access