


Introduction
NHS Talking Therapies for anxiety and depression (NHS TTad; formerly known as Improving Access to Psychological Therapies, IAPT) was launched in 2008 following the report of Layard et al., Reference Layard, Clark, Bell, Knapp, Meacher, Priebe and Wright2006, which highlighted the potential benefits of wider access to psychological support. The main initiative was to increase and improve treatment for anxiety and depression by offering evidence-based interventions, such as cognitive behavioural therapy (CBT), for the whole community (Clark, Reference Clark, McHugh and Barlow2012). The NHS TTad scheme intended to reduce inequalities, by being particularly responsive to those from marginalised groups and ensuring accessibility to individuals from all backgrounds (Holland, Reference Holland2009). This is important as racially minoritised people are at higher risk of mental health problems and more likely to experience inequalities and discrimination (Mental Health Foundation, 2019; Weich et al., Reference Weich, Nazroo, Sproston, McManus, Blanchard, Erens, Karlsen, King, Lloyd, Stansfeld and Tyrer2004).
Despite being more likely to be diagnosed with mental health conditions, racially minoritised groups experience inequalities in access, experiences and outcomes of psychological services (Arundell et al., Reference Arundell, Saunders, Buckman, Lewis, Stott, Singh, Jena, Naqvi, Leibowitz and Pilling2024b; NHS Race and Health Observatory, 2022; Williams et al., Reference Williams, Turpin and Hardy2006). In the UK, women from South Asian, Black African and African-Caribbean communities experience the highest rates of common mental disorders but are less likely to receive support than their White-British counterparts (NHS Digital, 2022). Between 2015 and 2022, people from the ‘White’ ethnicities were more likely to be offered therapy following an initial assessment than all other ethnic groups (Bamrah et al., Reference Bamrah, Rodger and Naqvi2025). Even after treatment has been initiated, racially minoritised groups are more likely to experience poor psychological recovery and disengage from services (Amati et al., Reference Amati, Green, Kitchin, Watt, Jones, AlRubaye, McCann and Greenfield2023; Arundell et al., Reference Arundell, Saunders, Buckman, Lewis, Stott, Singh, Jena, Naqvi, Leibowitz and Pilling2024b). Specifically, data suggest that individuals from Black ethnic groups are at the greatest risk of disengagement from NHS TTad services (Arundell et al., Reference Arundell, Saunders, Buckman, Lewis, Stott, Singh, Jena, Naqvi, Leibowitz and Pilling2024b; Murshed et al., Reference Murshed, Doherty, Mhojatoleslami, Tarabi and Rammohan2023), with one London service reporting drop-out rates of over 80% between referral, assessment and treatment (Lawton et al., Reference Lawton, McRae and Gordon2021). Racially minoritised individuals have historically been, and continue to be, under-represented in primary care mental health services (Bansal et al., Reference Bansal, Karlsen, Sashidharan, Cohen and Chew-Graham2022; Clark, Reference Clark, McHugh and Barlow2012; Lawton et al., Reference Lawton, McRae and Gordon2021).
Lack of awareness and understanding of mental health problems and treatment has been frequently cited as a contributing factor to this under-representation (Loewenthal et al., Reference Loewenthal, Mohamed, Mukhopadhyay, Ganesh and Thomas2012). A recent systematic review by Alam et al. (Reference Alam, O’ Halloran and Fowke2024) provides a more nuanced and comprehensive perspective on such findings. The review highlights cultural variation in the conceptualisation of mental health, including its interpretation through religious or spiritual frameworks, as well as differences in perceived seriousness of mental health concerns relative to physical health. It also identifies cultural norms that discourage help-seeking, such as expectations to manage difficulties privately or within the family unit, alongside a mistrust of healthcare professionals in some communities. In addition, internal and external stigma associated with mental illness, often shaped by cultural beliefs, can influence an individual’s perceptions of their symptoms and decisions to seek help. These factors may help explain why individuals from Black African, Asian, and mixed ethnic backgrounds are less likely to self-refer to NHS TTad services than White British individuals (Harwood et al., Reference Harwood, Rhead, Chui, Bakolis, Connor, Gazard, Hall, MacCrimmon, Rimes, Woodhead and Hatch2021).
The literature also indicates that people from racially minoritised communities are referred to primary and secondary mental health services less frequently by professionals, reflecting broader structural barriers to access (Devonport et al., Reference Devonport, Ward, Morrissey, Burt, Patel, Manning, Paredes and Nicholls2023). Moreover, even once referred, racially minoritised individuals are less likely to receive an assessment, and those who are assessed are less likely to be treated, indicating inequities at multiple stages of the process (Harwood et al., Reference Harwood, Rhead, Chui, Bakolis, Connor, Gazard, Hall, MacCrimmon, Rimes, Woodhead and Hatch2021). Alam et al. (Reference Alam, O’Halloran and Fowke2024) found that racially minoritised people were deterred from accessing support due to systemic issues such as limited choice, diversity, and cultural understanding within services, as well as direct negative experiences of discrimination, power imbalances and judgement. Fear of racist treatment from NHS healthcare professionals has also been cited as a deterrent to help-seeking (Bamrah et al., Reference Bamrah, Rodger and Naqvi2025). Therapists may inherit racial biases from wider society, which can translate to microaggressions within therapy settings and compromise psychological safety (Lawton et al., Reference Lawton, McRae and Gordon2021).
Barriers are likely shaped by both current and historical societal context. The concept of ethnic or racial difference has influenced healthcare research and practice across time, and contributed to stigmatisation, discriminatory practices and health inequalities for racially minoritised communities (Bryant et al., Reference Bryant, Jordan and Clark2022). Drapetomania, also known as ‘runaway slave syndrome’, was once a formal diagnosis used by white psychiatrists to pathologise enslaved Black people who attempted to escape, in order to justify their control and abuse (Lawton et al., Reference Lawton, McRae and Gordon2021). In 2021, the American Psychiatric Association (APA) issued a formal apology for upholding racist beliefs that Black people were hostile and primitive, which has had devastating impacts for their mental health treatment (APA, 2021). Recent literature suggests that statutory approaches to mental health assessment and treatment continue to be dominated by monocultural and reductionist frameworks which, alongside direct experiences of racist practice, create significant barriers to the provision of culturally responsive care (Bansal et al., Reference Bansal, Karlsen, Sashidharan, Cohen and Chew-Graham2022). Consequently, inequities are maintained through structures within services that have been developed in accordance with the needs and norms of the dominant cultural group (Pakes and Roy-Chowdhury, Reference Pakes and Roy-Chowdhury2007).
Given that constructions of psychological distress and well-being vary between cultures, normative western assumptions about how individuals with mental health issues present may not translate well to diverse populations (Roy-Chowdhury, Reference Roy-Chowdhury2013). Many psychotherapy models were developed in America or Europe, and rest on the normative pre-suppositions of these cultures. Therefore, interventions are likely not culturally appropriate for the whole community NHS TTad intended to serve (Roy-Chowdhury, Reference Roy-Chowdhury2013). A review of the literature, focusing on the utilisation of psychological support by racially minoritised groups, highlighted several limitations within service provision, including professional misunderstandings and over-reliance on Eurocentric conceptual frameworks (Williams et al., Reference Williams, Turpin and Hardy2006). South Asian women who had accessed NHS TTad spoke of disparities between the narratives of therapy and their cultural beliefs, which created a feeling of denying their culture, or ‘leaving it at the door’ (Yasmin-Qureshi and Ledwith, Reference Yasmin-Qureshi and Ledwith2020). Additionally, therapists often do not explore clients’ experiences of racism, despite these being recognised risk factors for mental health difficulties (Beck, Reference Beck2019). It is, therefore, unsurprising that clients from diverse cultural backgrounds are more likely to drop out of treatment (de Haan et al., Reference de Haan, Boon, de Jong and Vermeiren2018).
Thus, for NHS TTad to be successful in reducing inequalities and improving psychological well-being for the whole community, racism within its theories, approaches, and practices must be acknowledged (Lawton et al., Reference Lawton, McRae and Gordon2021; Patel and Fatimilehin, Reference Patel and Fatimilehin2005). To facilitate effective communication and reduce drop-out, services and therapists must consider client’s ethnic backgrounds and meaningfully engage with diverse cultural perspectives (de Haan et al., Reference de Haan, Boon, de Jong and Vermeiren2018). Research suggests that therapists can and do work in culturally sensitive ways. However, this is typically driven by individual initiative, and cultural competence is often dependent on a practitioner’s pre-existing cultural knowledge and experience (Arundell et al., Reference Arundell, Saunders, Barnett, Leibowitz, Buckman, Woodcock and Pilling2025; Bassey and Melluish, Reference Bassey and Melluish2012). Moreover, there is a growing body of literature examining how therapeutic interventions can be developed and delivered in ways that are culturally appropriate and responsive to clients’ ethnic identities (Arundell et al., Reference Arundell, Barnett, Buckman, Saunders and Pilling2021; Naz et al., Reference Naz, Gregory and Bahu2019). Specific recommendations include cultivating an anti-racist ethos at an organisational level, diversifying the workforce, community outreach, flexibility in service delivery, using culturally relevant resources and references, employing a person-centred approach, and implementing cultural adaptations (Alam et al., Reference Alam, O’Halloran and Fowke2024; Arundell et al., Reference Arundell, Barnett, Buckman, Saunders and Pilling2021; Arundell et al., Reference Arundell, Saunders, Barnett, Leibowitz, Buckman and Pilling2024a).
Despite the development and publication of guidance to support therapists and services in delivering treatment for diverse groups (Beck, Reference Beck2016; Beck et al., Reference Beck, Naz, Brooks and Jankowska2019; Rathod et al., Reference Rathod, Kingdon, Pinninti, Turkington and Phiri2015), inequalities persist (NHS Race and Health Observatory, 2022). Faheem (Reference Faheem2023) found that among 16 participants working in NHS TTad services, nine had received a single day of formal cultural competence training, whereas seven had received none. The BAME Positive Practice Guide (PPG; Beck et al., Reference Beck, Naz, Brooks and Jankowska2019) provides evidence-based recommendations and audit tools for delivering culturally sensitive and adapted therapies. However, there are no formal frameworks or dedicated funding mechanisms to support its implementation (Lawton et al., Reference Lawton, McRae and Gordon2021). Bamrah et al. (Reference Bamrah, Rodger and Naqvi2025) found that although the guide was viewed as valuable, limited resources hindered implementation, and where applied, practice varied substantially across services. This is unsurprising given that none of the 11 commissioners who reported that the guidance was being used within their service described their knowledge of it as ‘good’ or ‘excellent’, and 40% indicated having ‘little to no knowledge’. Nearly half of the commissioners (45%) also reported having no resources or funding specifically allocated to addressing ethnic inequalities within their services. Lawton et al. (Reference Lawton, McRae and Gordon2021), therefore, recommend local commissioning bodies establish a funded formalised framework, supported by relevant key performance indicators (KPIs), to ensure the PPG is implemented fully and meaningfully.
Understanding the NHS TTad experiences of racially minoritised clients is crucial for improving treatment and reducing inequalities in access and outcomes. A service evaluation was carried out to explore the experiences of clients from the ethnic group with the highest percentage of treatment drop-out, with the aim of making improvements to service delivery and increasing the rate of treatment completion. The project aimed to answer the following questions: (1) which ethnic group has the highest rate of disengagement?; (2) how is the service experienced by people from this group?; and (3) what ideas for improvement do they have, based on their experience?
Method
Statistical analysis was carried out using data from IAPTUS, the Electronic Patient Record System, to identify which ethnic group was most likely to decline service or drop out of treatment. A qualitative approach was then used to conduct a service evaluation, aimed at exploring the experiences of individuals of this ethnicity who had not completed treatment. The IAPTUS database was also used to identify individuals who met the inclusion criteria for the interviews, by generating a list of patient identification numbers based on the ‘discharge reason’ and ‘ethnicity’ categories.
Participants
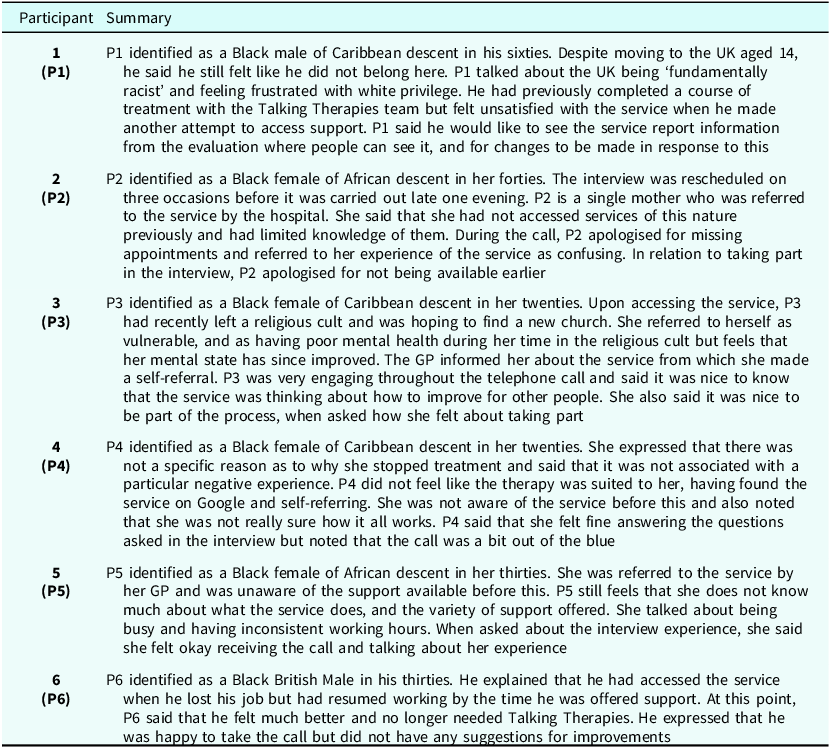
Ethnicity data were collected for 9264 patients that accessed the service between January 2020 and May 2021, excluding April and May 2020 due to the information being skewed as a result of service suspension during the COVID-19 pandemic. Six participants from the identified ethnic group, who had recently dropped out of, or declined treatment, opted to take part. All participants were over the age of 18, had been referred to the central London NHS TTad service, and had attended at least one appointment. For small projects carrying out interviews with a purposive sample, 6–10 participants are considered appropriate (Braun and Clarke, Reference Braun and Clarke2013). Recruitment and interviewing were discontinued due to the resource constraints of the project.
Procedure
Individuals were contacted by telephone in the order in which they had dropped out of treatment, starting with the most recent, and were asked if they would like to provide feedback on their experience of using the service. If clients opted to take part, a semi-structured interview was conducted either during the telephone call, or a call was scheduled for a convenient future time. Interviews were carried out between June and September 2021. These were structured using narrative inquiry to learn more about the participants lived experience of the service, and how this related to cultural context (Clandinin and Connelly, Reference Clandinin and Connelly2004). Narrative interviews involve an open-ended exploratory question (e.g. is there anything about your experience that you would like to share?), accompanied by follow-up prompts based on what was described, in the order it is discussed (e.g. you mentioned … can you tell me more about what happened?) (Wengraf, Reference Wengraf2011).
Service user involvement
The interview schedule and script used were informed by discussions with local community organisations. These groups are likely to be more representative of the clients not completing treatment, in comparison with the service user participation groups already established within the service. A focus group was held at the Dalgarno TrustFootnote 1 and verbal feedback on the draft interview script and schedule was provided by the founder of ‘Community 4 All’.Footnote 2 Upon completion of the evaluation, a summary of the findings and recommendations were shared with the organisations involved.
Ethics
As service user feedback is considered part of routine practice, and forms an important part of service development, a formal ethics review was not required. The Health Research Authority decision making tool was consulted and confirmed the project would not be considered research. The service evaluation forms part of what patient feedback should look like in better performing services, which is outlined in the NHS Talking Therapies national guidance (NHS England, 2024). Additionally, seeking feedback from communities that do not often use the service, using an outreach approach, is also part of the NHS TTad service remit. The project was supervised by the NHS TTad’s Race and Culture Lead and the Community Development Manager, and was closely overseen by the Clinical and Operational Lead.
Analysis
Quantitative
Microsoft Excel (version 16.65; Microsoft Corporation, 2023) was used for the descriptive statistics and JASP (version 0.95.4; JASP Team, 2025) was used to conduct inferential statistical analysis. A binary logistic regression was conducted to examine the association between ethnicity and disengagement. Treatment disengagement was the dichotomous dependent variable (coded 1 = disengaged, 0 = completed treatment). Ethnicity was included as a categorical predictor, with the White British group specified as the reference category. Participants with ethnicity listed as ‘not known’ or ‘not stated’ were excluded.
Qualitative
Narrative accounts were collected from six individuals from the ethnic group with the highest rate of treatment drop-out, to gain an insight into their experiences of the service. Each participant was assigned a number to maintain anonymity. Interviews were transcribed and later analysed to systematically map out the key events described, informed by structural and thematic traditions of narrative inquiry. Narrative analysis provides a vantage point that allows others to analyse and represent stories, as told by the individual with the experience (Marks and Yardley, Reference Marks and Yardley2004). This study is situated within a Critical Race Theory framework, which emphasises the importance of storytelling to foreground the lived experiences of racially minoritised individuals, consistent with narrative principles that value ordinary lived experience (Clandinin, Reference Clandinin2016; Rolón-Dow and Bailey, Reference Rolón-Dow and Bailey2021). This approach was guided by the project’s key learning aims and service needs, intending to capture participants’ individual experiences and understand how these influenced their perceptions of the NHS TTad (Rolón-Dow and Bailey, Reference Rolón-Dow and Bailey2021).
As narrative approaches involve interpretation at every stage (Josselson, Reference Josselson2006), the inquirer is not in a neutral, or objective, position to analyse what is said (Riessman, Reference Riessman1993). The author encouraged participants to speak freely without offering value judgements and initially analysed the narratives in their entirety to enhance comprehension and manage researcher bias (Mello, Reference Mello2002). Participants’ own words were then organised into tables to facilitate careful analysis and discussion with the project team, closely adhering to their narratives without extrapolating or making assumptions about their intentions (Coulter and Smith, Reference Coulter and Smith2009). Analysis involved inductively coding narrative blocks across accounts. Pattern coding was used to reduce large amounts of data into related themes, which involved identifying ‘explanatory or inferential codes’ (Miles and Huberman, Reference Miles and Huberman1994; p. 69). Blocks with the same code were re-read together and compared for similarities and differences. Codes were reviewed at meetings with the research team. To ensure the over-arching individual narratives were not lost, key comments made in relation to each code item are included as quotes alongside the relevant content. Additional remarks contributing to the narrative tone which did not fall under a code item were noted and included in the participant summaries (Table 3) to ensure participants were portrayed in a way that reflected how they chose to represent themselves (Lessard et al., Reference Lessard, Caine and Clandinin2018).
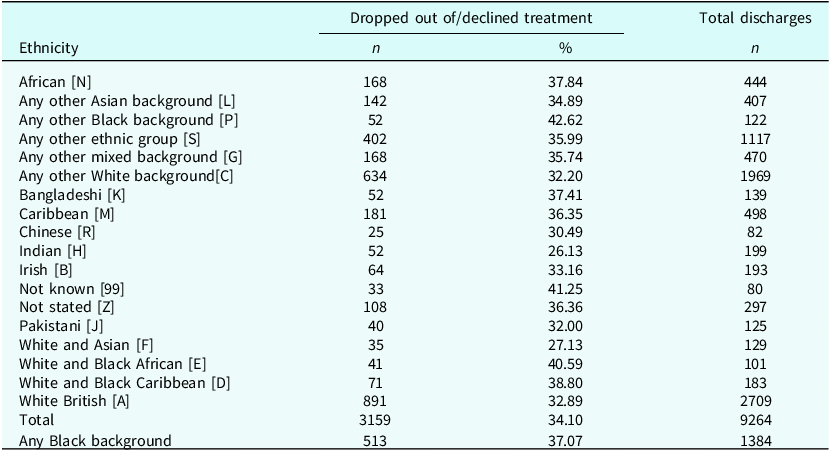
Number of clients that dropped out of or declined treatment with the NHS TTad service between January 2020 and May 2021, by ethnicity

Data from April and May 2020 was removed due to the information being skewed, as a result of service suspension during the COVID-19 pandemic.
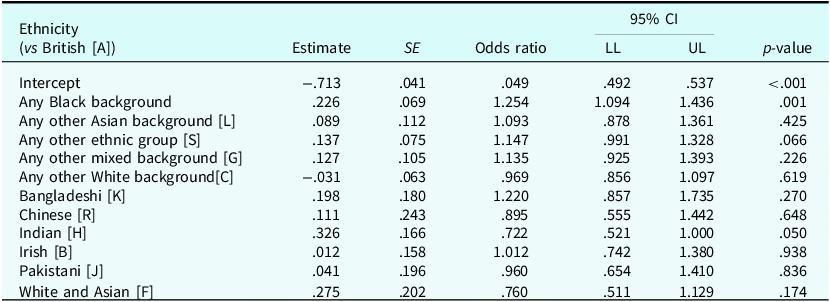
Logistic regression: associations between ethnicity and disengagement

CI, confidence interval; LL, lower limit; UL, upper limit.
Participant summaries

Reflexivity and positionality
The interviews were conducted and analysed by the first author, who at the time of data collection was a White British female trainee clinical psychologist from a working-class background, working clinically at the service. The first author was on a placement, not employed by the service, and no longer worked there at the time of writing, providing a degree of separation from participant feedback. The first author occupied an outsider position due to cultural and racial differences, which likely influenced how participants told their narratives (Dhillon and Thomas, Reference Dhillon and Thomas2019). This was likely further influenced by the power dynamics inherent in the researcher–participant relationship, potentially heightened by the author’s connection to the service (Coulter and Smith, Reference Coulter and Smith2009). The first author’s standpoint is that healthcare services are generally not adequately responsive to the diverse populations they serve, leading to the pre-supposition that there would be experiences of service inadequacies to tell (Yip, Reference Yip2023). The research team also consisted of a Black queer British male counselling psychologist from a middle-class background, working as a Senior Counsellor and the NHS TTad Race and Culture Lead; a British female of mixed Dominican and British heritage from a working-class background, working as the Community Development Lead; and a lesbian Consultant Clinical Psychologist from a White British background, working as the Clinical and Operational Lead.
Quality assurance
This study followed the Standards for Reporting Qualitative Research (SRQR) guidelines to ensure transparency and completeness in the reporting of qualitative data (O’Brien et al., Reference O’Brien, Harris, Beckman, Reed and Cook2014). Elliott et al.’s (Reference Elliott, Fischer and Rennie1999) seven guidelines for qualitative research were also adhered to, as follows: (1) disclosure of the authors’ backgrounds, assumptions and theoretical stance; (2) provision of detailed participant summaries; (3) participant quotes included in each theme; (4) regular consultation with the project team, which included individuals from racialised backgrounds similar to those of the participants; (5) inclusion of a summary table and a narrative summary to illustrate themes and sub-themes, and the relationship between them; (6) limitations of the small sample, and the implications for generalisability are discussed; (7) participant’s own words are used throughout to ensure narratives remain true to individual stories, and findings are presented with clinical recommendations in an accessible manner.
Results
Quantitative
A total of 8887 participants were included in the analysis after excluding cases with ethnicity recorded as ‘not known’ or ‘not stated’. Descriptive statistics (Table 1) shows both the number and proportion of clients that dropped out of, or declined, treatment against the total discharges for each ethnic group. After excluding individuals whose ethnicity was unknown, the six ethnic groups with the highest percentage (in descending order) were: any other Black background; White and Black African; White and Black Caribbean; African; Bangladeshi; and Caribbean. As five of the groups refer to people with a Black ethnic background, the decision was made to combine these into one singular category (any Black background) for analysis. This decision reflected the research objective to explore whether shared experiences might contribute to disengagement within these groups.
A binary logistic regression was performed to evaluate the relationship between ethnicity and treatment disengagement (Table 2). The model was statistically significant, χ2 (11, N=8875)=26.81, p=.005, although the variance explained by the model was small (Nagelkerke R 2=.004). Compared with the White British reference group, participants from Black backgrounds had significantly higher odds of disengaging from treatment (OR=1.25, 95% CI [1.09, 1.44], p=.001). Conversely, participants from Indian backgrounds had significantly lower odds of disengaging (OR=0.72, 95% CI [0.52, 1.00], p=.050). No other ethnic groups differed significantly from the White British group.
The interviewees
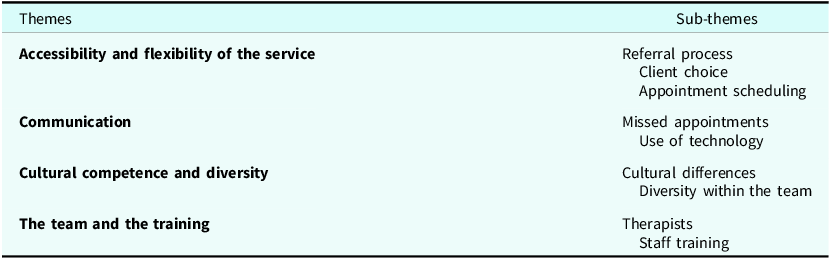
Themes and sub-themes within the narratives
Analysis of the data from the interviews yielded four main themes, consisting of nine sub-themes (Table 4).
Summary of themes and sub-themes

Accessibility and flexibility of the service
Referral process
There was a mixture of both self-referrals and GP or healthcare professional referrals across the narrative accounts. In general, individuals had not heard about the service until they had approached their GP, or conducted their own research, due to a need for support. Although most participants did not express any difficulty accessing the service once they decided to seek help, there appeared to be limited knowledge on how the referral and screening processes took place:
I feel like you are more likely to say no to an online referral than a doctor’s referral. You are more likely to trust a doctor. (P1)
Found the service on Google and self-referred, but I wasn’t aware of the service before this and not really sure about how it all works. (P4)
Most participants mentioned the length of time they had to wait for an appointment, but experiences differed between participants:
I didn’t have to wait long. (P2)
Prompt in getting the assessment done, but then there was a long waiting time. (P3)
Client choice
There was a general sense that the different therapy options available were not thoroughly explained, and the majority of participants did not feel they were given a choice:
Felt that power was taken away from me as choices were made by the service. (P1)
I felt like I was just allocated to this option, not talked through, or given other options. (P4)
I wasn’t told much about the options in the service. (P5)
Started with a phone call which moved to a video chat. I wasn’t comfortable with the video but felt awkward asking to switch back. It would have helped if I was told that this is okay and given a preference. (P4)
Appointment scheduling
A common sentiment amongst participants was that they had difficulty adhering to the scheduled appointment times, due to work patterns, changing schedules and other commitments:
Timings of the appointments were difficult, as I am a single mother. It wasn’t always the most convenient time to be able to open up. I needed it to be more flexible, with options to change appointments if my schedule changed. (P2)
It was difficult to attend appointments as if something came up and I had other commitments, I was not able to rearrange the slot. (P3)
Days and times of appointments were not convenient. I could not work this round my job and other commitments. It would have helped if the service could be more flexible. (P5)
Communication
Missed appointments
Participants expressed disappointment with the way in which communication took place regarding missed appointments. There was confusion as to who should be contacted, and how to undertake this, if they were unable to attend an appointment. Despite making contact to rearrange, participants reported receiving no follow-up from their therapist when an appointment was missed:
Tried to email and get in touch to apologise for missing the session. (P2)
I would have liked a follow-up call before they cancelled my appointments. (P2)
No-one followed up when I missed my appointments and if I ever missed a call, there would be no voicemail left, and they wouldn’t call again. (P5)
This was also cited as a reason for dropping out of treatment. It was noted that non-attendance can often be linked to the difficulties for which the individual is seeking support. Thus, participants felt that a telephone call to check the reason for missing appointments may reduce drop-out rates:
I felt I could not go back when I had been flaky due to my mental health. If someone has not attended the session, phoning them and following up to explore why would make people feel like they could come back and help with the reasons they have not attended. (P3)
Use of technology
There were differences between the narratives regarding the use of technology. Some participants felt that the use of email, to schedule appointments and collect questionnaires, was helpful and efficient: ‘I received quick responses, and it was convenient how the links were sent’ (P6). However, other participants reported encountering issues that made support harder to access:
Technological difficulties were frustrating. Emails often ended up in my junk. (P3)
Think it would have been easier face-to-face. (P3)
I found the experience confusing. (P2)
Cultural competence and diversity
Cultural differences
Participants also discussed how cultural perceptions and attitudes towards mental health affected their experience of accessing the service. Although some participants did not cite cultural differences as an issue, others talked about how stigma impacted their engagement: ‘Mental health is stigmatised in my culture, so I find it hard to talk about. Going to therapy can be embarrassing’ (P3). Participant responses indicated that cultural factors had not been acknowledged within therapy and, therefore, there was no opportunity to discuss how this may impact upon their experience: ‘It would have been helpful to discuss cultural difference, acknowledge it and have space to talk about it’ (P3). There was a common thread of finding it hard to talk about difficult or sensitive subjects, but only half of the participants linked this to cultural difference. Regardless of how it was framed, there was consensus that therapists had not asked enough questions, or the right questions, to encourage participants to engage more openly:
I felt like I needed to be asked more questions to get the conversation going and to open up. I had a problem with opening up and didn’t feel helped. (P2)
Certain subjects were difficult to talk about, and it didn’t feel like a comfortable enough space to talk about them. It didn’t feel like I was encouraged to speak about things. Only broad questions were asked, and there were not enough questions after to explore further. (P4)
Diversity within the team
Some participants felt that a better matched therapist would have made them feel more comfortable and helped them to communicate openly. At times, this was linked directly to cultural differences and feeling understood in a wider context:
The match with the counsellor wasn’t right, it didn’t work. (P2)
If it is not a physical difficulty, it is generally not talked about. It would have helped to have had someone who understood this a bit more or the option to be seen by someone from a similar background, even if that meant having to wait a bit longer. I want someone who understands my beliefs. Spirituality may be something to consider. (P3)
One participant commented on a lack of diversity in the staff team and identified this as an area for improvement: ‘The service doesn’t feel diverse. It feels very English’ (P1).
The team and the training
Therapists
Most participants described their therapists, and the other members of staff they had contact with, as friendly or empathetic. No participants reported malpractice or any issues with specific individuals working at the service:
Very friendly person I spoke to. (P6)
The clinician was friendly. (P4)
People I spoke to were empathetic. (P3)
I had no issues with the people I spoke to. (P5)
Staff training
Some participants felt that their therapists could benefit from more training. On one occasion, this was discussed in relation to supporting clients to communicate openly: ‘I feel like I needed a more trained counsellor. I didn’t know how to talk and had little guidance in sessions’ (P2). Another participant felt that the training for therapists should be more varied in nature and involve gaining experience within the community:
Staff need better training. Felt like the person on the other end of the phone was young, naive and poorly trained. It didn’t feel like they understood my experience. Training should involve going into the community or some form of community engagement rather than people just being there because they took a course. (P1)
Discussion
Which ethnic group is most likely to decline, or drop out of, treatment?
Consistent with existing literature, most racially minoritised groups at this NHS TTad service demonstrated higher rates of drop-out compared with the White British reference group. An exception was observed for individuals identifying as Indian, who were significantly less likely to disengage from treatment. The audit revealed that clients with a Black ethnic background, regardless of their specific ethnicity, comprised five of the six ethnic groups with the highest drop-out percentage. When these groups were combined for analysis, the ‘any Black background’ group was less likely to complete treatment than clients from the White British group. This project, therefore, set out to explore the experiences of NHS TTad clients with a Black ethnic background who dropped out of, or declined, treatment.
Although the logistic regression model was statistically significant, indicating a relationship between ethnicity and treatment drop-out, the variance explained by the model was small. This suggests that additional factors contribute to the observed differences, aligning with prior research demonstrating that ethnic disparities are often diminished when other sociodemographic and clinical variables are accounted for. For example, Arundell et al. (Reference Arundell, Saunders, Buckman, Lewis, Stott, Singh, Jena, Naqvi, Leibowitz and Pilling2024b) reported that differences between the White British and racially minoritised groups were substantially reduced, and sometimes disappeared entirely, following adjustment for such variables. Similarly, Amati et al. (Reference Amati, Green, Kitchin, Watt, Jones, AlRubaye, McCann and Greenfield2023) found that once occupation, social deprivation, initial morbidity, and social functioning were accounted for, only certain ethnic groups remained significant independent predictors of treatment outcome. These findings are also consistent with an intersectionality perspective (Carbado et al., Reference Carbado, Crenshaw, Mays and Tomlinson2013), which recognises that ethnicity interacts with other social and structural determinants to shape patterns of engagement.
However, Arundell and colleagues (2024b) found that controlling for other sociodemographic and clinical factors did not reduce the likelihood of treatment drop-out for Black, Asian or ‘other’ individuals. This suggests that additional mechanisms, such as stigma, mistrust, cultural incongruence, or service-level factors, linked specifically to the experiences of individuals from these ethnic groups may contribute to engagement challenges (Alam et al., Reference Alam, O’Halloran and Fowke2024) and may reflect limitations in the cultural responsiveness of services.
Together, these findings suggest that ethnicity may reflect intersecting structural and socio-economic disadvantages, rather than operating as an independent explanatory variable (Amati et al., Reference Amati, Green, Kitchin, Watt, Jones, AlRubaye, McCann and Greenfield2023). The current qualitative findings lend support to this interpretation, as participants described practical and structural barriers (e.g. employment constraints and single-parent responsibilities) that limited their capacity to engage. Although such factors are often framed as individual-level barriers, they may be more appropriately conceptualised as manifestations of broader structural inequalities, raising questions about the extent to which current service models are designed to accommodate marginalised populations. This can be understood through a structural competency lens (Metzl and Hansen, Reference Metzl and Hansen2014), which emphasises how institutional policies and service design shape patterns of access and engagement. From this perspective, disengagement reflects the interaction between service design and the lived realities of marginalised populations, rather than individual non-adherence. The findings are also interpreted using a cultural humility lens (Lekas et al., Reference Lekas, Pahl and Fuller Lewis2020), situating individual experiences within broader institutional and relational contexts.
How is the service experienced by people with a Black ethnic background?
Although participants generally described the referral process as straightforward, they also reported a limited understanding of referral pathways and available treatment options. Most participants also indicated that they had no prior knowledge of the service, or any other mental health services available in their area. This lack of awareness has been echoed in the literature (Alam et al., Reference Alam, O’Halloran and Fowke2024) and may help explain why racially minoritised people are under-represented in NHS TTad services (Bansal et al., Reference Bansal, Karlsen, Sashidharan, Cohen and Chew-Graham2022; Clark, Reference Clark, McHugh and Barlow2012; Lawton et al., Reference Lawton, McRae and Gordon2021), as well as why Black individuals are less likely to access primary mental health care (Cooper et al., Reference Cooper, Spiers, Livingston, Jenkins, Meltzer, Brugha, McManus, Weich and Bebbington2012; Harwood et al., Reference Harwood, Rhead, Chui, Bakolis, Connor, Gazard, Hall, MacCrimmon, Rimes, Woodhead and Hatch2021). Together, these findings indicate shortcomings in how services communicate and promote access.
Participants’ reports that treatment options were not fully explained or offered by therapists highlight the need to critically examine how information about the service is communicated. This includes consideration, through a structural competency lens, of whether current practices implicitly assume prior knowledge, or rely on treatment allocations, that systemically disadvantage marginalised groups. Limited choice has previously been identified as a deterrent to accessing support among racially minoritised individuals (Alam et al., Reference Alam, O’Halloran and Fowke2024) and as a contributing factor to disengagement (Murshed et al., Reference Murshed, Doherty, Mhojatoleslami, Tarabi and Rammohan2023). Arundell et al. Reference Arundell, Saunders, Buckman, Lewis, Stott, Singh, Jena, Naqvi, Leibowitz and Pilling2024b) found that individuals in the Black ethnic group had significantly lower odds of dropping out when they received a higher number of face-to-face sessions, despite being the most likely to disengage in whole-sample analyses. In combination with the findings of the current study, this suggests that the format of treatment and appointments may operate as a structural barrier to engagement and should be carefully considered during assessment and treatment planning.
Consistent with the findings reported by Arundell et al. (Reference Arundell, Saunders, Barnett, Leibowitz, Buckman and Pilling2024a), inflexibility of appointments was also highlighted as a key factor contributing to non-completion of therapy. This underscores the importance of services making deliberate efforts to ensure treatment accessibility in order to avoid exacerbating existing mental health inequalities. Additionally, in line with findings by Murshed et al. (Reference Murshed, Doherty, Mhojatoleslami, Tarabi and Rammohan2023), the handling of missed appointments emerged as an area requiring improvement. Establishing clear, well-communicated processes for cancelling or rescheduling appointments may support engagement, alongside proactive follow-up by therapists. This is particularly important given that the mental health difficulties for which clients seek treatment may themselves act as barriers to attendance. However, high referral volumes and performance targets related to access and waiting times may create a structural tension between operational performance requirements and the provision of flexible, accessible care. Viewed through a structural competency framework (Metzl and Hansen, Reference Metzl and Hansen2014), this tension reflects broader institutional priorities that may inadvertently contribute to disengagement. Addressing this tension requires an organisational response rather than placing additional expectations on individual clinicians working within already demanding roles.
Although no participants reported any impropriety regarding cultural issues, responses indicated that cultural difference was largely unacknowledged within therapy. While this may in part reflect White therapists’ fear of ‘getting it wrong’ when addressing cultural matters (Faheem, Reference Faheem2023), it also points to systemic gaps in training, supervision and organisational support for culturally responsive practice. Evidence suggests that many therapists receive little to no training in cultural sensitivity, and those who do typically receive only between one hour and half-a-day (Faheem, Reference Faheem2023). These findings align with calls for a shift from cultural competence to cultural humility (Lekas et al., Reference Lekas, Pahl and Fuller Lewis2020), which foregrounds ongoing reflexivity, attention to power differentials, and openness to learning, rather than static notions of competence. The absence of explicit cultural dialogue may reflect structural incompetence (Metzl and Hansen, Reference Metzl and Hansen2014) rather than individual inadequacy.
The importance of engaging with diverse cultural perspectives is well established in the literature and has been linked to reducing drop-out rates (de Hann et al., Reference de Haan, Boon, de Jong and Vermeiren2018). Creating space to discuss cultural difference may also provide opportunities for clients to express when particular topics feel hard to address. Developing a collaborative understanding of how culture, background, and prior experiences, shape a client’s engagement may allow therapists to adapt their approach accordingly. As with UK mental health services more broadly, therapists’ ways of working are likely to have been shaped primarily around the presentations and needs of the dominant cultural group (Roy-Chowdhury, Reference Roy-Chowdhury2013).
What ideas for improvement did participants have, based on their experience?
In line with the literature, feedback suggested that therapists’ cultural competence was dependent upon individual pre-existing cultural experience (Arundell et al., Reference Arundell, Saunders, Barnett, Leibowitz, Buckman, Woodcock and Pilling2025; Bassey and Melluish, Reference Bassey and Melluish2012). One proposed service improvement was to incorporate community and cultural learning into mandatory training requirements (Beck et al., Reference Beck, Naz, Brooks and Jankowska2019), which may enhance awareness of engagement barriers and improve therapists’ confidence and competence in initiating conversations about cultural difference. Naz et al. (Reference Naz, Gregory and Bahu2019) provide practical guidance for therapists and service managers to support this process, while the PPG (Beck et al., Reference Beck, Naz, Brooks and Jankowska2019) offers recommendations for culturally sensitive practice.
However, for such initiatives to be implemented consistently and effectively, adequate funding and the integration of relevant KPIs into service delivery are required (Bamrah et al., Reference Bamrah, Rodger and Naqvi2025; Lawton et al., Reference Lawton, McRae and Gordon2021; NHS Race and Health Observatory, 2022). In line with a cultural humility perspective (Lekas et al., Reference Lekas, Pahl and Fuller Lewis2020), developing cultural responsivity requires moving beyond time-limited training towards sustained organisational commitment, with structured opportunities for continued professional development, reflective practice, supervision, and accountability within service design. Without this embedding, training initiatives risk becoming one-off, tokenistic exercises. The recent publication of the Patient and Carer Race Equality Framework (PCREF; NHS England, 2023) is encouraging, signalling progress by outlining statutory duties for NHS Trusts and mental health providers, as well as practical steps for compliance. Consistent with the feedback in this study, the PCREF sets out national organisational competencies, including cultural awareness, and recommends incorporating anti-racism actions into ongoing staff personal development plans.
An alternative suggestion was to offer clients the option of requesting a therapist from a similar ethnic background. While service users in the current study reported that shared cultural or ethnic backgrounds would facilitate engagement, others have reported the opposite (Arundell et al., Reference Arundell, Saunders, Barnett, Leibowitz, Buckman and Pilling2024a), underscoring the importance of preserving choice. Matching clients with therapists from similar cultural backgrounds may help reduce professional misunderstandings, which has been linked to the poor utilisation of psychological support by racially minoritised groups (Alam et al., Reference Alam, O’Halloran and Fowke2024; Williams et al., Reference Williams, Turpin and Hardy2006). However, research should first explore the potential implications of this approach for staff. For example, therapists from racially minoritised backgrounds may experience increased emotional labour if routinely exposed to accounts of discrimination that resonate with their own experiences. Additionally, such an approach may also lead to an unbalanced workload distribution and extended waiting times, given that the NHS workforce does not reflect the diversity of the populations it serves (Hemmings et al., Reference Hemmings, Buckingham, Oung and Palmer2021). Services should, therefore, continue to prioritise increasing workforce diversity (Arundell et al., Reference Arundell, Saunders, Barnett, Leibowitz, Buckman and Pilling2024a), in line with commitments outlined in the Five Year Forward View (NHS England, 2015) and the NHS Mental Health Implementation Plan 2019/20 – 2023/24 (NHS England, 2019).
Limitations
This study has several limitations that should be considered when interpreting the findings. The sample consisted of six clients with a Black ethnic background from a single NHS TTad service located in London, which is a diverse urban setting. As such, the experiences described may not be representative of clients in other regions, such as rural settings or in services where racially minoritised populations comprise a smaller proportion of the community (Arundell et al., Reference Arundell, Saunders, Barnett, Leibowitz, Buckman and Pilling2024a). Gathering feedback from a larger and more varied sample, including clients from all ethnic groups, would provide a broader understanding of how services can be improved and would enable meaningful comparative analyses. Although the qualitative approach enabled the collection of rich and detailed accounts, a quantitative design would allow the service to gather data from a wider population, generate more generalisable conclusions, and reduce the influence of interpretation bias. For example, NHS TTad services could distribute a Likert-style survey to all clients, or specifically to those who disengage, which could then be replicated across the UK to gather feedback on key areas, such as cultural responsiveness. The resulting data could be compared by ethnicity and across service locations, supporting services to learn from each other and to identify organisation wide training opportunities and priorities.
Furthermore, no additional sociodemographic or clinical variables (e.g. age, gender, socio-economic status) were collected or included in the statistical analysis, limiting the ability to account for factors known to influence engagement, outcomes, and experience of services. Future research and service evaluations should collect the additional variables needed to undertake more robust, adjusted analyses.
Conclusion
This study provides empirical support for existing research and recommendations, with almost all aspects of participants’ feedback reflected in the wider literature and recent practice guidance. Importantly, it extends this evidence base by foregrounding service users’ own words, illustrating why these recommendations matter and how they shape lived experiences of care. The findings are particularly aligned with Arundell et al. (Reference Arundell, Saunders, Barnett, Leibowitz, Buckman and Pilling2024a), Beck et al. (Reference Beck, Naz, Brooks and Jankowska2019), and the NHS Race and Health Observatory (2022). This combined evidence calls for clearer communication and choice in treatment options, as well as greater service flexibility and supportive handling of missed appointments. There is also a consistent theme of services requiring stronger community involvement, including proactive outreach to improve awareness and access, and co-production with community organisations. Findings also reflect wider recommendations urging culturally sensitive practice, a more diverse workforce, and attention to service-user preferences regarding therapist characteristics. Together, these parallels show that the areas for improvement identified in this study are well-established and widely addressed by current guidance. However, the practical application of such guidance must be prioritised, adequately funded, and monitored through meaningful KPIs to be effective.
As only a small percentage of the variance in drop-out rates was explained by ethnicity, it is likely that other socio-demographic factors are contributing, which aligns with the literature (Amati et al., Reference Amati, Green, Kitchin, Watt, Jones, AlRubaye, McCann and Greenfield2023; Arundell et al., Reference Arundell, Saunders, Buckman, Lewis, Stott, Singh, Jena, Naqvi, Leibowitz and Pilling2024b). This does not negate the relevance of culture but suggests that while cultural adaptation of therapy is necessary, it is not sufficient to achieve equitable outcomes (Amati et al., Reference Amati, Green, Kitchin, Watt, Jones, AlRubaye, McCann and Greenfield2023). Services must work collaboratively with racially minoritised communities to ensure their needs are meaningfully and holistically integrated into service development (Beck and Naz, Reference Beck and Naz2019).
Key practice points
-
(1) Increase community engagement: improve the service’s visibility and approachability by establishing a presence in the local community, offering accessible information to raise awareness and build trust.
-
(2) Provide opportunities and training to increase cultural awareness in the workforce: encourage staff to take part in community engagement initiatives and relevant training to improve their cultural sensitivity and confidence.
-
(3) Enhance service accessibility and communication: services should review current delivery practices to facilitate greater flexibility and clearer communication regarding service processes, including how to manage missed appointments.
-
(4) Increase diversity in the workforce: recruitment initiatives should prioritise attracting clinicians from diverse cultural backgrounds.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author.
Acknowledgements
The authors thank the Dalgarno Trust and Community 4 All for providing advice and consultation.
Author contributions
Hannah Shaw: Conceptualization (equal), Formal analysis (lead), Investigation (lead), Methodology (lead), Project administration (lead), Writing - original draft (lead), Writing - review & editing (equal); Lucy Wilson-Shaw: Conceptualization (equal), Formal analysis (supporting), Methodology (supporting), Project administration (supporting), Supervision (equal), Writing - review & editing (equal); Anthony Newton: Conceptualization (equal), Project administration (equal), Supervision (equal), Writing - review & editing (equal); Michelle Poponne: Conceptualization (equal), Methodology (supporting), Project administration (supporting), Supervision (equal), Writing - review & editing (equal).
Financial support
There is no funding or sponsorship relating to this study.
Competing interests
The authors declare that they have no competing interests.
Ethical standards
As service user feedback is considered part of routine practice, a formal ethics review was not required. Authors have abided by the Ethical Principles of Psychologists and Code of Conduct as set out by the BABCP and BPS.

 Open access
Open access
Comments
No Comments have been published for this article.