


Obsessive–compulsive disorder (OCD), characterised by recurrent, persistent and unwanted obsessions and/or compulsions, is a chronic and debilitating mental disorder. Reference Abramowitz and Jacoby1 OCD has a lifetime prevalence ranging from 1 to 3% worldwide, Reference Fawcett, Power and Fawcett2–Reference Ruscio, Stein, Chiu and Kessler5 and it is ranked among the top 10 most disabling illnesses in terms of lost income and reduced quality of life by the World Health Organization (WHO), 6 adversely impacting both individuals and their families. Reference Steketee7,Reference Stengler-Wenzke, Kroll, Matschinger and Angermeyer8
Psychological interventions have demonstrated a large overall effect in treating OCD. Reference Wang, Miguel, Ciharova, Amarnath, Lin and Zhao9 Currently, seven main types of psychotherapy are available for individuals with OCD, each focusing on specific aspects of treatment. Exposure and response prevention (ERP Reference Lindsay, Crino and Andrews10–Reference Bolton and Perrin12 ) involves gradually confronting anxiety-provoking situations while resisting avoidance or neutralising behaviours. Cognitive therapy Reference van Balkom, de Haan, van Oppen, Spinhoven, Hoogduin and van Dyck13,Reference Alcolado and Radomsky14 manages OCD by targeting maladaptive cognitive appraisals, and cognitive–behavioural therapy (CBT Reference Baruah, Pandian, Narayanaswamy, Bada Math, Kandavel and Reddy15–Reference Mancebo, Yip, Boisseau, Rasmussen and Zlotnick17 ) typically combines ERP and cognitive therapy. Mindfulness-based therapy (MBT Reference Mathur, Sharma, Balachander, Kandavel and Reddy18,Reference Zhang, Lu, Didonna, Wang, Zhang and Fan19 ) teaches individuals with OCD to observe their thoughts without judgement; metacognitive therapy (M Reference Glombiewski, Hansmeier, Haberkamp, Rief and Exner20,Reference Melchior, van der Heiden, Deen, Mayer and Franken21 ) focuses on modifying patients’ beliefs about the importance of intrusive thoughts and the necessity of performing rituals; acceptance and commitment therapy (ACT Reference Twohig, Hayes, Plumb, Pruitt, Collins and Hazlett-Stevens22,Reference Lee, Choi and Lee23 ) encourages patients to respond flexibly to obsessions, anxiety and uncertainty while moving towards their values rather than being driven by fears; and the inference-based approach (IBA Reference Visser, van Megen, van Oppen, Eikelenboom, Hoogendorn and Kaarsemaker24 ) helps patients trust their inner and outer senses, addressing the underlying reasoning processes and reducing obsessional doubts.
A range of randomised controlled trials (RCTs) have demonstrated the effectiveness of various psychotherapies for OCD compared with control groups, including ERP, Reference Baruah, Pandian, Narayanaswamy, Bada Math, Kandavel and Reddy15–Reference Mancebo, Yip, Boisseau, Rasmussen and Zlotnick17 cognitive therapy, Reference van Balkom, de Haan, van Oppen, Spinhoven, Hoogduin and van Dyck13,Reference Alcolado and Radomsky14 CBT, Reference Baruah, Pandian, Narayanaswamy, Bada Math, Kandavel and Reddy15–Reference Mancebo, Yip, Boisseau, Rasmussen and Zlotnick17 MBT, Reference Mathur, Sharma, Balachander, Kandavel and Reddy18,Reference Zhang, Lu, Didonna, Wang, Zhang and Fan19 MCT, Reference Glombiewski, Hansmeier, Haberkamp, Rief and Exner20,Reference Melchior, van der Heiden, Deen, Mayer and Franken21 ACT Reference Twohig, Hayes, Plumb, Pruitt, Collins and Hazlett-Stevens22,Reference Schneider, Wittekind, Talhof, Korrelboom and Moritz25 and IBA. Reference Visser, van Megen, van Oppen, Eikelenboom, Hoogendorn and Kaarsemaker24 However, to our knowledge, the comparative effectiveness and acceptability of these therapies remain unclear. Previous controlled trials have directly compared different psychotherapies for OCD, such as ERP versus cognitive therapy, Reference van Balkom, de Haan, van Oppen, Spinhoven, Hoogduin and van Dyck13,Reference Emmelkamp and Beens26,Reference Rodrigues, Fechine, Oliveira, Matos, Passarela and Hemanny27 CBT versus ERP, Reference Rector, Richter, Katz and Leybman28,Reference McLean, Whittal, Thordarson, Taylor, Söchting and Koch29 CBT/ERP versus IBA, Reference Visser, van Megen, van Oppen, Eikelenboom, Hoogendorn and Kaarsemaker24,Reference O’Connor, Aardema, Bouthillier, Fournier, Guay and Robillard30 MBT versus CBT, Reference Aardema, Bouchard, Koszycki, Lavoie, Audet and O’Connor31 MCT versus ERP Reference Glombiewski, Hansmeier, Haberkamp, Rief and Exner20,Reference Melchior, van der Heiden, Deen, Mayer and Franken21 and ACT versus ERP. Reference Twohig, Abramowitz, Smith, Fabricant, Jacoby and Morrison32 The findings from these trials are, however, inconsistent. For example, whereas one RCT reported ERP as marginally more effective than CBT, Reference McLean, Whittal, Thordarson, Taylor, Söchting and Koch29 another Reference Rector, Richter, Katz and Leybman28 found that CBT led to significantly greater symptom reduction compared with ERP. These discrepancies highlight the need for more robust and conservative estimates of the relative effectiveness of psychotherapies for OCD. The most recent meta-analysis Reference Wang, Miguel, Ciharova, Amarnath, Lin and Zhao9 examining the overall effectiveness of psychotherapies over the past 30 years found that cognitive therapy and third-wave CBT demonstrated significantly lesser effect sizes compared with CBT and ERP. Whereas that study provided important insights, its analyses were limited to direct head-to-head comparisons and excluded indirect evidence – i.e. comparisons made through a shared comparator. Incorporation of indirect comparisons is essential for estimating the relative efficacy of treatments not directly compared within individual trials, thereby offering a more comprehensive understanding of the evidence base. Furthermore, that study grouped MBT, MCT, ACT and IBA together as ‘third-wave CBT’ therapies, failing to evaluate their specific effectiveness individually.
Therefore, we aimed to conduct a network meta-analysis (NMA) to compare the effectiveness and acceptability of different psychotherapies for OCD. NMA enables the combination of both direct and indirect evidence, thereby providing a comprehensive evaluation of treatments. Reference White33 Drawing on existing knowledge, Reference Wang, Miguel, Ciharova, Amarnath, Lin and Zhao9 we hypothesise that all psychotherapies will be significantly more effective than control conditions, with no specific expectations regarding effectiveness between therapies and their acceptability.
Method
Identification and selection of studies
We utilised a living database of psychological interventions for OCD, which was built through comprehensive searches in both international (PubMed, Embase, PsycINFO, international clinical trials registry platform of WHO) and Chinese (China National Knowledge Infrastructur, WeiPu, WanFang, Chinese Clinical Trial Registry) databases, spanning the period from inception to 1 September 2024. China, as the second most populous country globally, has a substantial number of individuals suffering from OCD. 34 However, although many Chinese researchers have explored OCD, Reference Zejuan and Hailing35–Reference Yanmeng, Zhipeng and Changhai37 their work might not be accessible in international databases due to language barriers. The living database has facilitated the publication of several meta-analytic studies on OCD. Reference Wang, Miguel, Ciharova, Amarnath, Lin and Zhao9,Reference Wang, Amarnath, Miguel, Ciharova, Lin and Zhao38,Reference Wang, Duan, Cao and Xu39 Detailed search strings can be found in Appendix A. Data extraction commenced on 8 October 2024. The study protocol was prospectively registered at the Open Science Framework (https://doi.org/10.17605/OSF.IO/KG3J8) prior to initiation of the literature search and analyses.
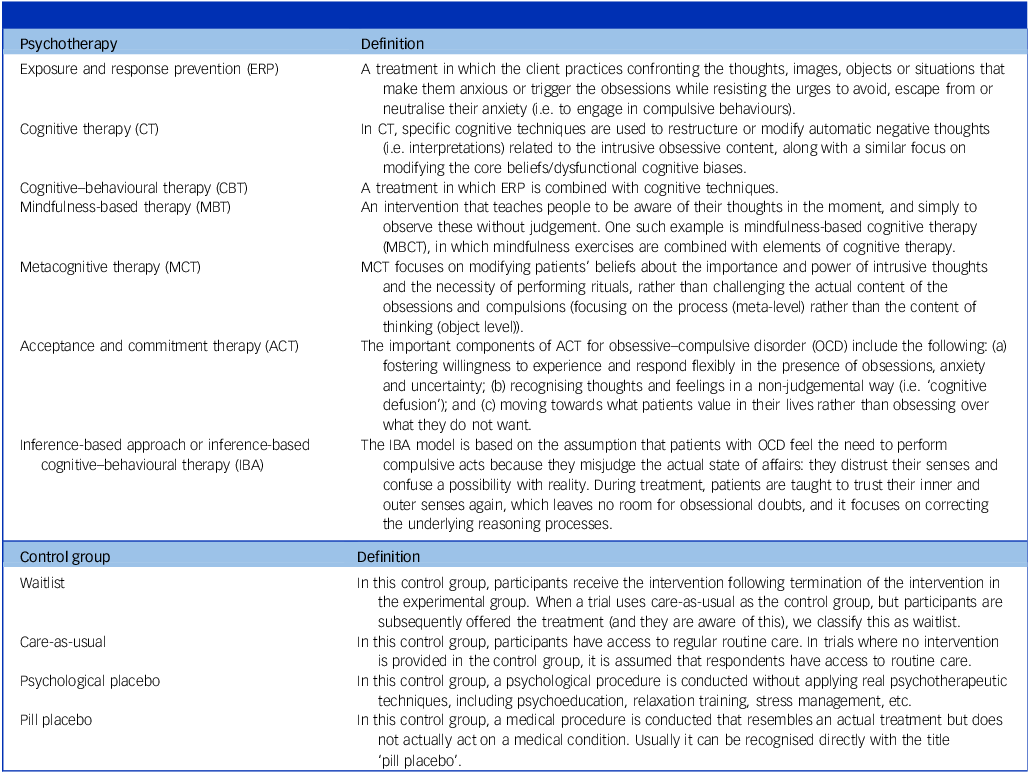
RCTs that compared psychotherapies with each other or with control groups for individuals with a primary diagnosis of OCD, as determined by valid clinical interviews, were included. The definitions of psychotherapies and control groups are detailed in Table 1. All delivery formats of psychotherapy were eligible for inclusion, except unguided self-help interventions Reference Cuijpers and Schuurmans40 in which individuals work independently on the programme/treatment protocol to learn and apply psychotherapeutic strategies. This exclusion was based on evidence indicating that unguided self-help interventions yield smaller treatment effects compared with professionally delivered interventions. Reference Pearcy, Anderson, Egan and Rees41
Definitions of psychotherapy and control groups

No restrictions were placed on gender, age or setting. There were no limitations on the duration of treatment, number of sessions or minimal number of participants. However, trials examining interventions such as stepped-care management, maintenance treatment or relapse prevention were excluded, as were comparisons of different delivery formats of the same psychotherapy. In addition, unpublished studies were not included due to concerns regarding methodological rigour, transparency and the reliability of reported outcomes.
All records were screened and selected by two independent researchers (Y.W., C.M.), with any disagreements, such as the classification of psychotherapy types, resolved through discussion or by a third senior researcher (M.B.J.T.).
Data extraction and risk of bias assessment
We extracted data across four key domains: (a) effect size calculation, including mean and standard deviation; (b) characteristics of participants, including mean age, proportion of females and proportion of participants using psychiatric medication; (c) characteristics of the intervention, including type of psychotherapy, whether the treatment was administered by trained therapists, and treatment integrity implementation; and (d) characteristics of the study, including region of study origin and recruitment method for participants.
The revised risk-of-bias tool for randomised trials (RoB 2 Reference Sterne, Savović, Page, Elbers, Blencowe and Boutron42 ) was used to assess the risk of bias in included RCTs across five domains: randomisation process, deviations from intended interventions, missing outcome data, outcome measurement and selective outcome reporting. An overall rating of ‘high risk of bias’ was assigned if any domain was rated as high risk or if three or more domains were rated as raising some concerns. An overall rating of ‘some concerns’ was given when no domains were rated as high risk and no more than two domains were rated as having some concerns. Studies were rated as ‘low risk of bias’ only if all domains were rated as low risk.
Data extraction and RoB 2 assessment were conducted by two independent researchers (Y.W., C.M.), and any disagreements were solved through discussion.
Outcomes
The main outcomes were effectiveness and acceptability at post-treatment. Effectiveness was evaluated using a single outcome measuring OCD symptom severity in each study, determined via a hierarchy algorithm (see Appendix B) based on its frequency of usage in preceding literature. Reference Wang, Miguel, Ciharova, Amarnath, Lin and Zhao9 Acceptability was operationalised as the all-cause study drop-out rate at the end-of-treatment assessment.
Statistical analyses
A series of pairwise meta-analyses were performed for all direct comparisons using a random-effects pooling model. Heterogeneity was assessed with the I 2 statistic Reference Ioannidis, Patsopoulos and Evangelou43 and its 95% confidence interval, as well as τ 2. Small-study effects were inspected visually using a funnel plot and tested with Egger’s test. Reference Egger, Smith, Schneider and Minder44 Additionally, prediction intervals were estimated to represent the 95% confidence interval of the predictive distribution of effects in future comparable trials.
Network meta-analyses were conducted to evaluate the comparative effectiveness of all treatments by combining both direct and indirect evidence. Initially, we depicted the geometry of the network of evidence using network plots. Reference Hutton, Salanti, Caldwell, Chaimani, Schmid and Cameron45 Subsequently, network meta-analyses were conducted for both effectiveness and acceptability utilising a frequentist network meta-analysis method, Reference Rücker46 with the random-effects model. Reference Higgins, Jackson, Barrett, Lu, Ades and White47 Effectiveness was estimated using standardised mean differences (SMDs), calculated by dividing the mean difference by the pooled standard deviation, with acceptability measured by relative risk with 95% confidence interval. The ranking of treatments was assessed based on the surface under the cumulative ranking curve (SUCRA Reference Salanti, Ades and Ioannidis48 ).
To assess the assumption of transitivity, we created a table of characteristics of patients and interventions for direct comparisons, verifying whether potential effect modifiers were similarly distributed across the network. Consistency of the network was checked through both local and global inconsistency tests. The net heat plot Reference Krahn, Binder and König49 visualised the degree of inconsistency within the network using colour gradients, as determined in the local test. The node-splitting method Reference Dias, Welton, Caldwell and Ades50 was employed to scrutinise consistency across the entire network of treatments, assessing the consistency assumption for each node (treatment comparison) in the network during the global test.
Three sensitivity analyses were conducted: (a) exclusion of outliers, defined as studies in which 95% confidence intervals around their effect sizes did not overlap with those of the pooled effect size in any pairwise meta-analyses; Reference Viechtbauer and Cheung51,Reference Harrer, Cuijpers, Furukawa and Ebert52 (b) restriction to studies rated as low risk of bias; and (c) exclusion of studies with comorbidities in which participants presented at least one co-occurring mental disorder.
Additionally, four post hoc analyses were conducted. First, a sensitivity analysis restricted the sample to adults with OCD; second, a sensitivity analysis excluded comparisons involving waitlist controls; and third, a sensitivity analysis excluded comparisons supported by only a single study. Finally, acceptability was assessed using odds ratios with 95% confidence intervals. These analyses were performed to explore potential factors influencing treatment effects and acceptability.
The analyses were conducted in R 4.3.3 (R Foundation for Statistical Computing, Vienna, Austria; see https://www.Rproject.org/) using the ‘netmeta’ package on Windows 11. Reference Balduzzi, Rücker, Nikolakopoulou, Papakonstantinou, Salanti, Efthimiou and Schwarzer53 The network plot and certainty of evidence for the network estimates were examined through the web application Confidence In Network Meta-Analysis (CINeMA Reference Papakonstantinou, Nikolakopoulou, Higgins, Egger and Salanti54 ; see https://cinema.ispm.unibe.ch/).
Results
Identification, inclusion and characteristics of studies
The results are reported in accordance with Preferred Reporting Items for Systematic Reviews (PRISMA) guidelines. Figure 1 presents the PRISMA flowchart of study selection and inclusion. In total, 12 449 records were identified through database searches. Following removal of duplicates, 8766 records were screened based on abstracts and titles, and 581 full-text articles were assessed for eligibility. Ultimately 68 studies Reference Lindsay, Crino and Andrews10–Reference Alcolado and Radomsky14,Reference Fals-Stewart and Schafer16–Reference Visser, van Megen, van Oppen, Eikelenboom, Hoogendorn and Kaarsemaker24,Reference Emmelkamp and Beens26–Reference Twohig, Abramowitz, Smith, Fabricant, Jacoby and Morrison32,Reference Zejuan and Hailing35,Reference Anderson and Rees55–Reference Hong, Jing and Yanyan100 were included, with 3 published in Chinese.
The Preferred Reporting Items for Systematic Reviews flowchart of study selection and inclusion.

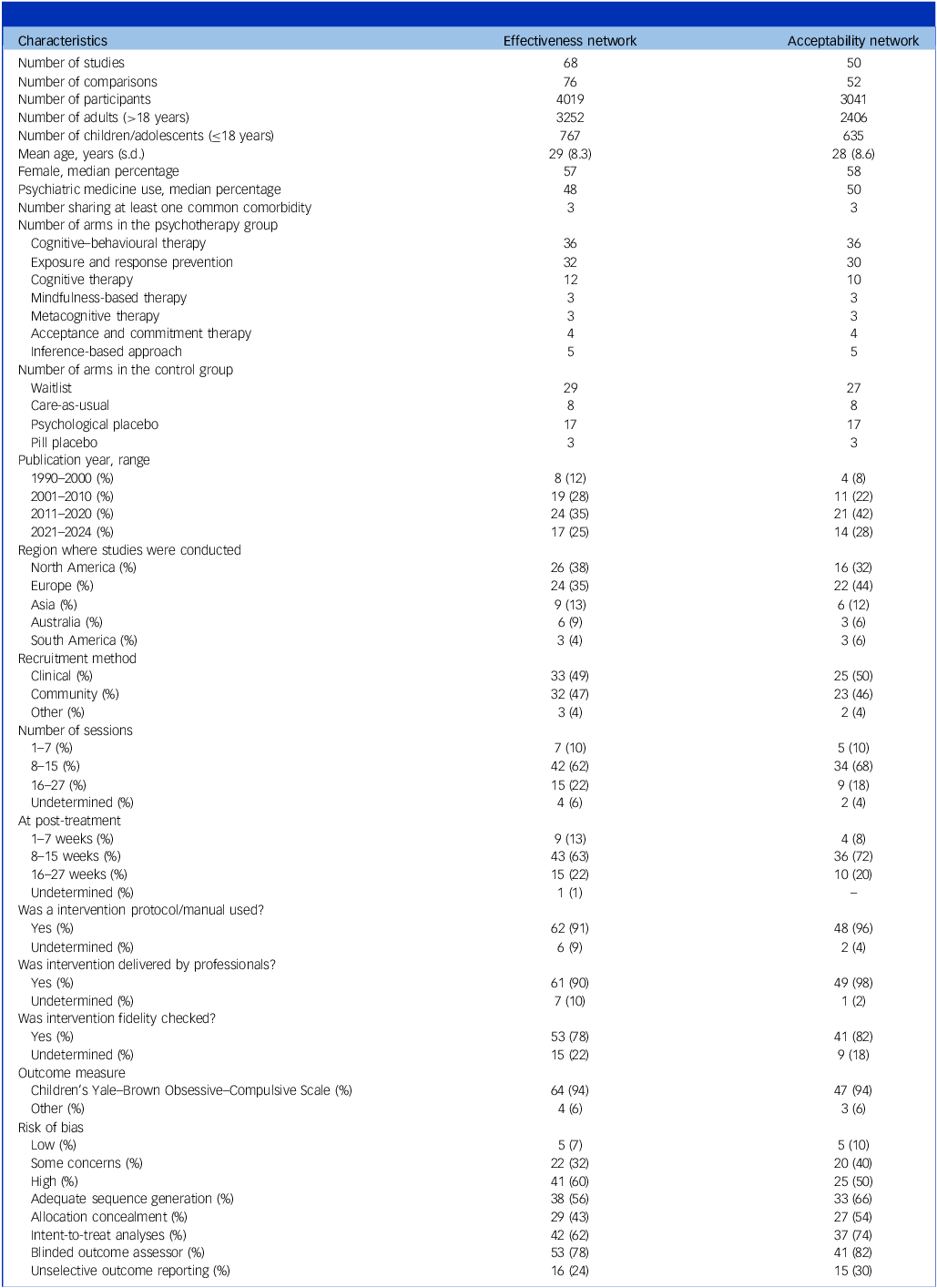
Table 2 provides an overview of the key characteristics of the included studies. The 68 RCTs contained 76 comparisons and involved 4019 patients with OCD, with a mean age of 29 years (s.d. = 8.3). Fourteen studies targeted children/adolescents, encompassing 767 patients. Regarding treatment arms, 36 were CBT, 32 were ERP, 12 were cognitive therapy, 5 were IBA, 4 were ACT, 3 were MBT and 3 were MCT. In terms of control group, 29 were waitlist, 17 were psychological placebo, 8 were care-as-usual and 3 were pill placebo. Over half of the studies (60%) were published in the past 15 years. Geographically, 26 studies (38%) were conducted in North America, 24 (35%) in Europe, 9 (13%) in Asia, 6 (9%) in Australia and 3 (4%) in South America. Participants were recruited almost evenly from clinical (49%) and community (47%) settings. Regarding treatment, the majority of interventions spanned 8–15 sessions delivered over 8–15 weeks. Most studies (91%) utilised treatment manuals or protocols, 90% delivered treatments by professionals such as clinical psychologists or licensed psychotherapists and 78% checked treatment fidelity. In terms of outcome assessment, 64 studies (94%) used the (Children’s) Yale–Brown Obsessive–Compulsive Scale ((C)Y-BOCS) to evaluate treatment effectiveness. The remaining four studies employed other measures, including the Vancouver Obsessional Compulsive Inventory, the National Institute of Mental Health Obsessive–Compulsive Scale and the Maudsley Obsessional–CompulsiveCompulsive Inventory (MOCI). Details of study and intervention characteristics can be found in Appendices C and D.
Key characteristics of the included studies

Regarding risk of bias, 7% of the included RCTs were rated as ‘low risk’, 32% as having ‘some concerns’ and 60% as ‘high risk’. Specifically, 56% of RCTs utilised adequate sequence generation, 43% employed allocation concealment, 62% performed intent-to-treat analysis and 78% reported self-reported or blinded clinician-rated outcomes. However, only 24% of RCTs reported outcomes unselectively. A detailed risk of bias assessment is provided in Appendix E.
Network plot
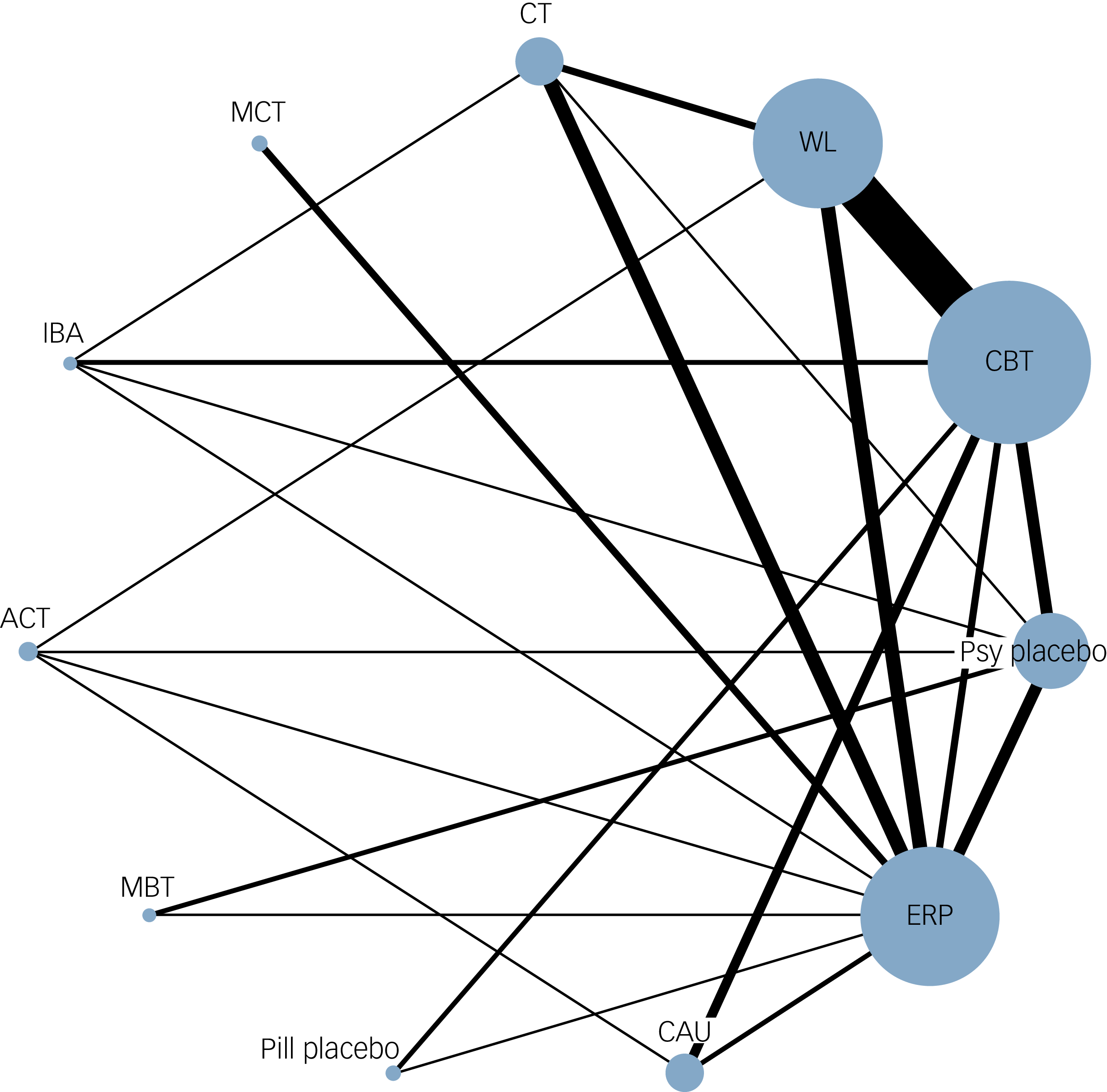
The network plot is shown in Fig. 2. Overall, the network was well connected. CBT and ERP were the psychotherapies most studied, followed by cognitive therapy. ACT, MBT, IBA and MCT were primarily connected through comparisons with ERP. Waitlist was the most connected control group, followed by psychological placebo and care-as-usual. Pill placebo was the control group least studied, with only three comparisons.
The network plot of meta-analysis. The size of node and thickness of edge were based on the number of studies on that comparison. CBT, cognitive behaviour therapy; ERP, exposure and response prevention; CT, cognitive therapy; MBT, mindfulness-based therapy; MCT, metacognitive therapy; ACT, acceptance commitment therapy; IBA, inference-based approach; WL, waitlist; CAU, care-as-usual; Psy placebo, psychological placebo.

Pairwise meta-analyses
The results of pairwise meta-analyses are presented in Appendix F. The most frequently examined head-to-head comparison was between CBT and waitlist. CBT, ERP, cognitive therapy, MBT and ACT were significantly more effective than control groups (waitlist, care-as-usual, pill/psychological placebo) in reducing OCD symptom severity (SMD −1.62 to −0.42). Additionally, no significant differences were observed among the psychotherapies.
Network meta-analyses
Figure 3 shows the results of NMAs on effectiveness and acceptability (without adjustment for modifiers). Regarding effectiveness, all psychotherapies were significantly more effective than waitlist: CBT (SMD −1.20, 95% CI [−1.42, −0.98]; SUCRA, 45.1%; low certainty); ERP (SMD −1.39, 95% CI [−1.68, −1.10]; SUCRA, 58%; low certainty); cognitive therapy (SMD −1.40, 95% CI [−1.79, −1.01]; SUCRA, 27%; low certainty); MBT (SMD −0.96, 95% CI [−1.60, −0.33]; SUCRA, 37%; moderate certainty); MCT (SMD −1.32, 95% CI [−1.95, −0.70]; SUCRA, 75%; moderate certainty); IBA (SMD −1.14, 95% CI [−1.68, −0.59]; SUCRA, 83%; moderate certainty); and ACT (SMD −1.09, 95% CI [−1.60, −0.57]; SUCRA, 64%; low certainty). Global heterogeneity across the network was moderate to high (I 2 = 65.7%). All psychotherapies were also significantly more effective than pill placebo (SMD −1.44 to −1.00). Except for MBT, all psychotherapies were significantly more effective than both psychological placebo (SMD −0.95 to −0.63) and care-as-usual (SMD −0.95 to −0.76). Additionally, psychological placebo was significantly more effective than waitlist (SMD −0.45, 95% CI [−0.78; −0.13]). However, no significant differences were identified among psychotherapies. In regard to acceptability, no significant differences were observed between psychotherapies and control groups or among psychotherapies themselves. Additionally, in a post hoc analysis in which acceptability was calculated using odds ratios, the findings were generally consistent with those based on relative risks, showing no significant differences among psychotherapies. However, CBT (odds ratio 1.75, 95% CI [1.19, 2.58]), IBA (odds ratio 2.73, 95% CI [1.23, 6.08]) and psychological placebo (odds ratio 1.94, 95% CI [1.14, 3.31]) were significantly more acceptable than waitlist controls (see Appendix G).
Network meta-analyses of psychotherapies for obsessive–compulsive disorder. Standardised mean differences (SMDs) and 95% confidence intervals (CIs) for effectiveness are reported below the diagonal. SMDs lower than 0 favour the column-defining treatment, with 95% CIs not including the point of no difference (0) highlighted in bold. Relative risks (RRs) and 95% confidence intervals for acceptability are reported above the diagonal. RRs greater than 1 favour the row-defining treatment, with 95% CIs not including the point of no difference (1) highlighted in bold. CBT, cognitive behaviour therapy; ERP, exposure and response prevention; CT, cognitive therapy; MBT, mindfulness-based therapy; MCT, metacognitive therapy; ACT, acceptance commitment therapy; IBA, inference-based approach; CAU, care-as-usual; Psy placebo, psychological placebo; WL, waitlist.

Ranking of psychotherapies
In regard to effectiveness, ERP and cognitive therapy ranked highest, followed by MCT, CBT, IBA, ACT and MBT. In terms of acceptability, IBA ranked highest, followed by MCT, ACT, ERP, CBT, MBT and cognitive therapy. The ranking forest of psychotherapies relative to waitlist – the most frequently used comparator – can be found in Appendix H, along with a scatterplot combining effectiveness and acceptability. Regarding confidence in the quality of evidence assessed through CINeMA, none of the comparisons were rated as ‘high confidence’, primarily due to within-study bias. Confidence in the estimate ranged from moderate to low (see Appendix I).
Consistency examination
Visual inspection of the distribution of potential effect modifiers indicated that potential modifiers were similarly distributed across the comparisons in the network (see Appendix J). Both local and global tests generally demonstrated substantial consistency between direct and indirect evidence. However, some comparisons – such as CBT versus ERP – were informed by a limited number of studies, which may reduce the reliability of consistency assumptions for those specific comparisons due to low statistical power (see Appendix K).
Sensitivity analyses
Sensitivity analyses excluding outliers and studies with comorbidities yielded results consistent with the main analyses. Similarly, post hoc sensitivity analyses restricted to adults with OCD, those excluding waitlist comparisons and those excluding comparisons supported by only a single study produced comparable findings. In the sensitivity analysis for studies with a low risk of bias, 13 comparisons were identified and the results were generally similar, with minor deviations from the main analyses. No significant differences were found among psychotherapies. All psychotherapies, except for MBT and IBA, were significantly more effective than waitlist. Detailed results of sensitivity analyses can be found in Appendix L.
Discussion
To our knowledge, this network meta-analysis is the largest study to date to simultaneously evaluate the effectiveness and acceptability of various psychotherapies for OCD. All psychotherapies were significantly more effective than control conditions. No significant differences were found among the psychotherapies in terms of either effectiveness or acceptability, and these findings were robust across most sensitivity analyses. Although minor deviations emerged in the analysis restricted to studies rated as low risk of bias, these differences may reflect the limited number of studies included. Although the findings offer valuable insights for research and clinical practice, they should be interpreted with caution due to substantial heterogeneity, high risk of bias across the included studies and their limited statistical power to detect differences between psychotherapies.
In terms of effectiveness, CBT and ERP remain the most extensively studied psychotherapies for OCD, and demonstrated large significant effects consistent with prior research. Reference Wang, Miguel, Ciharova, Amarnath, Lin and Zhao9–Reference Rosa-Alcázar, Sánchez-Meca, Gómez-Conesa and Marín-Martínez101 Cognitive therapy demonstrated effect sizes comparable to CBT and ERP, which aligns with an earlier meta-analysis. Reference Rosa-Alcázar, Sánchez-Meca, Gómez-Conesa and Marín-Martínez101 However, those findings contrast with a more recent meta-analysis Reference Wang, Miguel, Ciharova, Amarnath, Lin and Zhao9 that found lesser effects of cognitive therapy compared with CBT and ERP. Notably, these two analyses were limited to direct comparisons within individual studies and included a small number of cognitive therapy studies. MBT, MCT, ACT and IBA showed significant effectiveness in reducing OCD symptom severity, corroborating earlier research. Reference Evey and Steinman102–Reference Trent, Guzick, Viana and Storch105 Additionally, these approaches demonstrated effects comparable to CBT, ERP and cognitive therapy. These findings position cognitive therapy, MBT, MCT, ACT and IBA as potential alternatives to the widely recognised CBT and ERP. However, they also raise a critical question: should further research efforts prioritise novel psychotherapies when current evidence does not suggest superior outcomes in treating OCD? Nonetheless, because the current evidence may be influenced by limited statistical power – largely stemming from the predominance of RCTs on CBT and ERP and the relatively small number of trials investigating other approaches, as well as a high risk of bias across studies – further methodologically rigorous research is required to draw definitive conclusions. Moreover, comparable efficacy across psychotherapies does not necessarily imply uniform effectiveness in practice. Effect sizes may be influenced by potential moderators, such as individual characteristics. For instance, IBA has shown potential advantages for OCD patients with extremely poor insight. Reference O’Connor, Aardema, Bouthillier, Fournier, Guay and Robillard30 Future research should focus on identifying specific populations or individuals who may derive the greatest benefit from specific psychotherapies. This effort would help optimise treatment strategies and enhance personalisation in OCD management, ultimately improving patient outcomes. Regarding control groups, although waitlist was used as the reference comparator due to its prevalence across studies, we also evaluated the effects of psychotherapies relative to other control conditions, including psychological placebo, care-as-usual and pill placebo. The consistent superiority of psychotherapies across these comparisons supports their specific efficacy beyond non-specific treatment effects. Additionally, psychological placebo demonstrated significantly greater effectiveness than waitlist. This finding aligns with a meta-analysis in depression, Reference Michopoulos, Furukawa, Noma, Kishimoto, Onishi and Ostinelli106 but contrasts with a more recent meta-analysis Reference Wang, Miguel, Ciharova, Amarnath, Lin and Zhao9 which found that psychological placebo yielded the smallest effects compared with waitlist, care-as-usual and pill placebo. These discrepancies highlight the need for further research examining how different types of control conditions influence effect size estimates in psychotherapy trials.
The development of various psychotherapies is closely associated with the limitations of ERP. Although ERP demonstrates strong efficacy, an estimated 62% of participants are classified as ‘non-responders’. Reference Cuijpers, Miguel, Ciharova, Harrer, Basic and Cristea107 Moreover, the nature of ERP, which requires that participants resist anxiety-reduction behaviours when confronted with anxiety-provoking situations, leads to treatment refusal in 25–30% of participants, Reference Ong, Clyde, Bluett, Levin and Twohig108 with an attrition rate of 18.7%. Reference Ong, Clyde, Bluett, Levin and Twohig108 Practical barriers, such as the limited availability of trained clinicians and the intensive time commitment required for ERP, further restrict its applicability. Reference Hirschtritt, Bloch and Mathews109 As a result, clinicians and researchers are actively seeking more treatment options for OCD. Our results indicate that, although these therapies demonstrate effects similar to ERP, no significant differences were found regarding acceptability (drop-out rates). Given the absence of significant differences among psychotherapies in terms of both effectiveness and acceptability, treatment rankings should be interpreted as general guidance rather than definitive conclusions. Other important considerations – such as cost-effectiveness – also play a critical role in treatment selection. Ultimately, when multiple evidence-based options are available, the choice of therapy should be guided by patient preference, clinical characteristics and contextual factors to optimise care. Importantly, the findings may be affected by the limited number of studies on these therapies. Future research focusing on treatment adherence is needed to validate these results. Additionally, studies examining patient-level predictors and moderators of treatment adherence are highly recommended, because they will help refine treatment strategies and improve outcomes for OCD patients.
The current study offers important strengths and implications. Methodologically, it combined both available direct and indirect evidence of comparison of different psychotherapies, providing an overview of the psychotherapy field for OCD. Notably, it analysed recently developed interventions – MBT, MCT, ACT and IBA – individually, rather than aggregating them under the broad category of third-wave CBT, thus offering more specific insights into their individual effectiveness. The findings also yield key implications for research and clinical practice. First, whereas cognitive therapy and ERP demonstrate efficacy similar to CBT, the unique advantages of CBT – where it integrates both cognitive therapy and ERP – remain to be fully explored. Second, given the current literature predominantly centred on CBT and ERP, more studies evaluating other psychotherapies such as cognitive therapy, MBT, MCT, ACT and IBA, as well as head-to-head comparisons, are needed to validate and expand current findings. Third, most existing studies focus on adults, highlighting the need for further research on the effectiveness of psychotherapies in children and adolescents with OCD. Fourth, the results emphasise the importance of identifying which psychotherapies are most effective for specific subgroups, thereby promoting more personalised treatment strategies. Fifth, detailed reporting of clinical characteristics – such as psychiatric medication use – is encouraged to better identify moderators and predictors of treatment outcomes. Sixth, cost-effective research is needed to guide evidence-based resource allocation in mental health services. Seventh, although psychotherapies show broadly comparable efficacy, future studies should examine how these interventions can be effectively implemented and adapted across diverse cultural and healthcare systems to improve accessibility and impact. Additionally, more rigorous assessment of potential adverse effects is essential to ensure treatment safety and support informed clinical decisions. Lastly, future studies should adopt methodologically robust designs to minimise heterogeneity and reduce the risk of bias, thereby improving the validity and reliability of findings in this field.
However, several limitations should be acknowledged. First, the transitivity assumption underlying network meta-analysis cannot be fully guaranteed, given the limited number of direct comparisons and the substantial heterogeneity observed across several comparisons. This heterogeneity reflects potential clinical or methodological variability among studies with similar designs and may affect the validity of indirect evidence. Future research using more methodologically rigorous designs is needed to examine the influence of potential effect modifiers, particularly clinically relevant variables such as baseline OCD severity. Second, the high risk of bias across included studies, primarily due to selective reporting, may compromise the validity, reliability, confidence and statistical power of the findings, thereby necessitating cautious interpretation. Third, although we selected a single effect size per comparison per study – a common approach in network meta-analyses – most studies used (C)Y-BOCS, with a few employing other instruments such as MOCI. This variation in measurement tools may affect the validity of the results. Future studies are recommended to examine the independence among multiple outcomes or the specific effects of different measurement instruments on treatment effects, using methodologies explicitly designed for this purpose, such as multivariate or three-level meta-analytic models. Fourth, we used drop-out rates as a proxy for treatment acceptability; however, this measure may not capture the full complexity of patient experiences or decision-making. Future studies should consider incorporating more direct and multidimensional assessments of acceptability, such as the proportion of planned sessions completed, patient-reported satisfaction or engagement metrics. In addition, discrepancies in acceptability findings based on relative risks versus odds ratios may partly reflect the limited number of available studies, underscoring the need for both further research on treatment acceptability and methodological investigations examining the impact of different analytic approaches. Fifth, the study did not assess the long-term effects of psychotherapies due to limited follow-up data, leaving uncertainty regarding the durability of treatment effects and highlighting the need for future research on sustained outcomes. Lastly, by including only published or in-press studies and excluding unpublished studies, the analysis may be subject to publication bias, potentially affecting the comprehensiveness and robustness of the findings. Taken together, although this study offers valuable insights into the comparative effectiveness and acceptability of psychotherapies for OCD, the interpretation of its findings should be tempered by these limitations.
In conclusion, psychotherapies are similarly effective and acceptable for treating OCD. However, the limited statistical power, substantial heterogeneity and high risk of bias across most included studies highlight the need for more rigorous, methodologically robust research to validate these findings. Ensuring the effective and acceptable application of psychotherapies across diverse populations and settings is crucial for optimisation of OCD management.
Supplementary material
The supplementary material is available online https://doi.org/10.1192/bjp.2026.10651
Data availability
The data that support the findings of this study are available from the corresponding author Y.W., upon reasonable request.
Acknowledgements
We thank C.M., M.C., A.A., J.L. and R.Z. for their contribution to data collection.
Author contributions
Y.W., S.Y.S., L.M.d.W. and P.C. designed the study. Y.W. conducted analyses and prepared the draft manuscript. Y.W., C.M., M.C., A.A., J.L. and R.Z. contributed to data collection. C.M., M.B.J.T., M.C., J.L., R.Z., S.Y.S., L.M.d.W. and P.C. provided critical and intellectual comments on the draft. All authors reviewed and approved the final manuscript.
Funding
Y.W. is financially supported by the Chinese Scholarship Council (grant no. 202108330055) for her PhD. The funding source had no role in the design of the research. Open Access funding is provided by Vrije Universiteit Amsterdam.
Declaration of interest
All authors declare there are no conflicts of interest. P.C. is member of the British Journal of Psychiatry editorial board and did not take part in the review or decision-making process of this paper.





 Open access
Open access
eLetters
No eLetters have been published for this article.