


Many adult mental health, neurodevelopmental, and physical health disorders have their roots in childhood (Betts et al., Reference Betts, Williams, Najman and Alati2016; Daines et al., Reference Daines, Hansen, Novilla and Crandall2021; Misiak et al., Reference Misiak, Stańczykiewicz, Pawlak, Szewczuk-Bogusławska, Samochowiec, Samochowiec, Tyburski and Juster2022; Mulraney et al., Reference Mulraney, Coghill, Bishop, Mehmed, Sciberras, Sawyer, Efron and Hiscock2021; Pine & Fox, Reference Pine and Fox2015). National surveys indicate that the number of children affected by neurodevelopmental disorders and poor physical health is high, increasing, and associated with significant economic and emotional costs (Hughes et al., Reference Hughes, Ford, Bellis, Glendinning, Harrison and Passmore2021; Ling et al., Reference Ling, Chen, Zahry and Kao2023; Reinert et al., Reference Reinert, Fritze and Nguyen2024; Tkacz & Brady, Reference Tkacz and Brady2021). Meta-analyses show that as many as 1 in 5 children and adolescents have a mental health diagnosis (Polanczyk et al., Reference Polanczyk, Salum, Sugaya, Caye and Rohde2015; Sacco et al., Reference Sacco, Camilleri, Eberhardt, Umla-Runge and Newbury-Birch2024). Moreover, a study conducted in 2024 with 70,000 youth across the United States (U.S.) indicated that 10.1% of adolescents have had serious thoughts of suicide, 15.4% reported a major depressive event, and 41.9% reported symptoms of generalized anxiety disorder (Anderer & Rekito, Reference Anderer and Rekito2025). Similarly, prevalence rates of childhood obesity present a major public health concern, affecting nearly 20% of U.S. children — more than 14.7 million children (Centers for Disease Control and Prevention, 2024).
Developmental scientists have made tremendous advances regarding our understanding of risk and promotive factors that undermine or support physical health, mental health, and psychological wellbeing across childhood, adolescence, and adulthood (Crone & van Duijvenvoorde, Reference Crone and van Duijvenvoorde2021; Lynch et al., Reference Lynch, Sunderland, Newton and Chapman2021; Oldehinkel & Ormel, Reference Oldehinkel and Ormel2023; Tung et al., Reference Tung, Hipwell, Grosse, Battaglia, Cannova, English, Quick, Llamas, Taylor and Foust2024). Further, advances in genetic tools and methodologies have facilitated new insights into genetic contributions to wellbeing across development (Moyakhe et al., Reference Moyakhe, Dalvie, Mufford, Stein and Koen2023; van de Weijer et al., Reference van de Weijer, Pelt, Baselmans, Ligthart, Huider, Hottenga, Pool and Bartels2024; van de Weijer et al., Reference van de Weijer, Pelt, van Beijsterveldt, Willemsen and Bartels2022). Yet, the translation of these scientific and methodological advances has not led to parallel advances in child and adolescent mental and physical health outcomes. Reasons for the lack of translation from science to practice include concerns about replicability and reproducibility, partially caused by smaller sample sizes, unique sample characteristics, lack of rigorous mechanistic frameworks, and/or publication biases that reduce the generalizability of findings (e.g., Bogdan, Reference Bogdan2025; Nosek et al., Reference Nosek, Hardwicke, Moshontz, Allard, Corker, Dreber, Fidler, Hilgard, Kline Struhl, Nuijten, Rohrer, Romero, Scheel, Scherer, Schönbrodt and Vazire2022; Visscher et al., Reference Visscher, Yengo, Cox and Wray2021).
Based on the public health consequences of mental and physical health problems in childhood and adolescence and our interest in furthering the basic science to practice pipeline, the Early Growth and Development Study (EGDS) was launched in 2002, originally through the George Washington University (GWU), Oregon Social Learning Center, and Iowa State University. Currently, EGDS is led by researchers at GWU, University of Oregon, and Penn State University. EGDS was designed to test mechanistic hypotheses related to environmental and genetic contributions to child development via a longitudinal prospective parent-offspring adoption study that includes linked adoptive and birth parents and adoptees. The study was later expanded to include a second cohort of adoptive families, and then expanded again to include a third cohort of siblings in both birth and adoptive parents’ homes. In keeping with EGDS longitudinal design, the adoptees in both cohorts, along with their adoptive and biological siblings, and their birth and adoptive parents, have been followed in regular intervals since enrollment.
Historically, psychological research has typically focused on parents, often only mothers, raising their own biological offspring. Such research designs are limited in their ability to account for the effects of genes that are common to parents and children, or to consider whether genetically influenced traits in children influence how they are parented and how parenting affects them. Parent-offspring adoption studies can help address these gaps. However, adoption studies that prospectively examine social environmental processes from early childhood through adolescence are rare. To date, the Early Growth and Development Study (EGDS) and the Colorado Adoption Project (Plomin & DeFries, Reference Plomin and DeFries1985) are the only such studies. In the parent-offspring adoption design, similarities between birth parents and the adopted child suggest genetic influences (attributed to shared genes and a lack of shared rearing environments) or prenatal influences (occurring in utero). Associations between adoptive parents’ and adopted children’s characteristics suggest postnatal environmental processes (based on shared rearing environments and the lack of shared genes), although evocative gene-environment correlation (rGE) effects may also cause adoptive parent-child associations. When data about the biological siblings (full siblings and half siblings) or genetically unrelated siblings who are reared in either the birth parent home or in the adoptive home are included, additional insights can be gained regarding the role of the postnatal rearing environment. This is achieved by examining sibling correlations as a function of shared or nonshared home environment, the degree of genetic relatedness of the sibling pair (0%, 25%, or 50% of shared genes, on average), and the degree of genetic relatedness between the child and rearing parent(s) (0%, 50%). We summarized the history of the adoption design and provided a synopsis of prior key EGDS findings in a recent monograph (Reiss et al., Reference Reiss, Ganiban, Leve, Neiderhiser, Shaw and Natsuaki2022), with primary findings indicating evidence for main effects of the rearing environment in the absence of passive gene-environment correlation, and evidence for both evocative gene-environment correlations and gene × environment interactions beginning in early childhood. Although main effects of parenting, marital functioning, and parent psychopathology are not new findings, EGDS has been able to show that associations between these family characteristics and child psychosocial adjustment are not attributable to passive gene-environment correlation, and that they can be detected across childhood and into adolescence.
Materials and Methods
Overview of the Early Growth and Development Study (EGDS) Cohorts
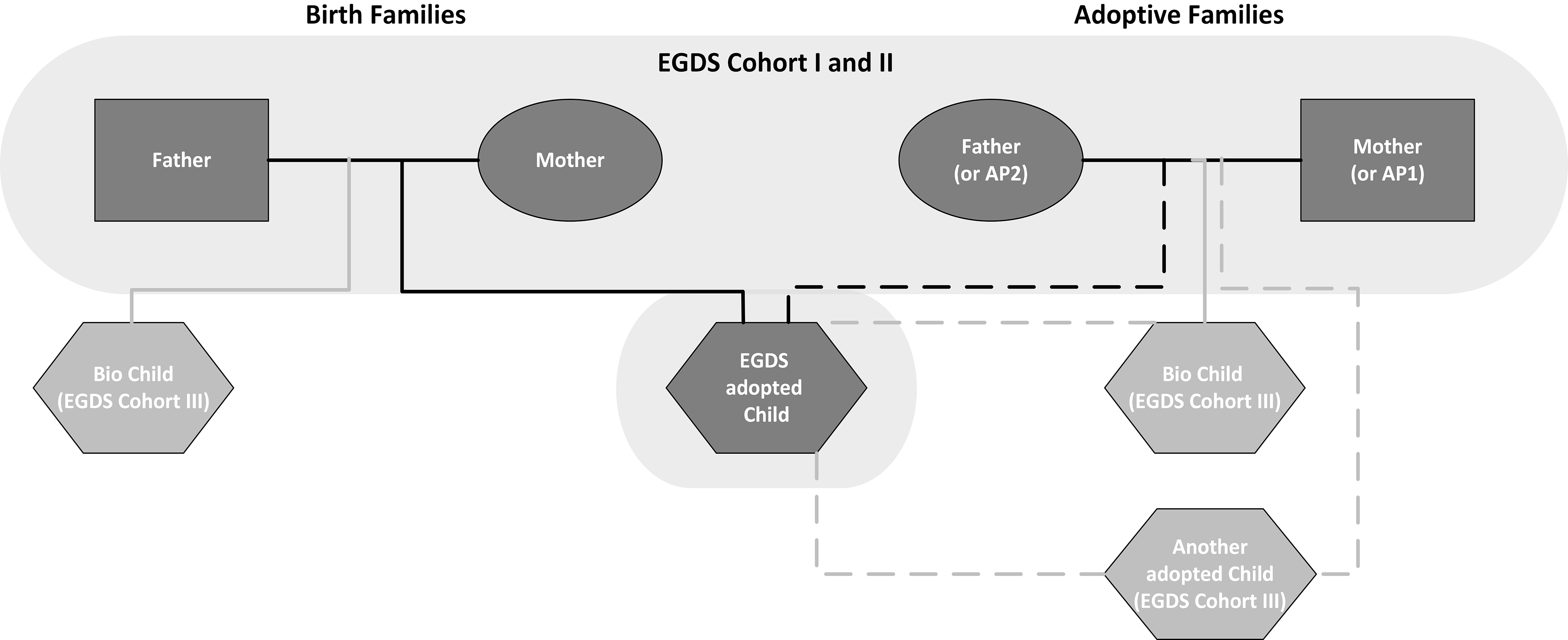
This article provides an update on the available data and cross-cohort findings from EGDS (see Leve et al., Reference Leve, Neiderhiser, Ganiban, Natsuaki, Shaw and Reiss2019; Leve et al., Reference Leve, Neiderhiser, Ge, Scaramella, Conger, Reid, Shaw and Reiss2007, Leve et al., Reference Leve, Neiderhiser, Shaw, Ganiban, Natsuaki and Reiss2013 for earlier reports), and highlights opportunities for harmonization and multicohort analyses with other genetically informed studies. The EGDS started in 2002 as a prospective adoption study designed to examine the influence of specific features of families and social contexts on child adjustment, and factors that may mediate the expression of genetic influences or that may be moderated by (or moderate) genetic influences. The original EGDS cohort (n = 361 children; Cohort I) was subsequently expanded to enlarge the sample, increase power to detect prenatal environment influences, and replicate findings across cohorts and/or across different family configurations (see Figure 1). The first expansion occurred in 2007, when a second cohort of adoptees and their birth and adoptive parents was recruited (n = 200 children; Cohort II). Next, beginning in 2013, the biological siblings of the Cohort I and II adoptees who were raised in the birth home were recruited when they turned age 7 (n = 217 children; Early Parenting of Children—EPoCh; Cohort III; Leve et al., Reference Leve, Neiderhiser, Harold, Natsuaki, Bohannan and Cresko2018). Finally, beginning in 2016, Cohort III was expanded to include all additional siblings between age 7−21 living in either the birth parent or adoptive parent home (n = 881 children; Environmental influences on Child Health Outcomes [ECHO]; Cohort III). With this final expansion, the EGDS study also added new behavioral and health outcomes and developmentally salient environmental exposures. Assessments continued longitudinally. With each cohort expansion, we included many of the same measures across the three EGDS cohorts, to promote cross-cohort analyses. We also prioritized including data elements (e.g., items and measures) that were available in other national registries and datasets to increase comparability with other studies. By focusing on longitudinal family processes from early childhood to age 21 and leveraging the three cohorts of EGDS participants, our study provides a unique opportunity to detect gene-environment interplay as it arises and unfolds across pivotal developmental periods from infancy to early adulthood.
EGDS Parent-Offspring Adoption and Sibling Study design.
Note: AP, adoptive parent; EGDS; Early Growth and Development Study; Bio Child; biological offspring of the parents listed above them.

Figure 2 illustrates the interrelation of the EGDS Cohorts and its substudies, and the developmental periods covered. EGDS-Cohort I (n = 361) and Cohort II both began in infancy, with Cohort I initially emphasizing toddler development (‘Toddlers’) and Cohort II focusing specifically on the role of prenatal influences (‘Prenatal’). These first two cohorts include adoptees and their adoptive and birth parents. The Cohort II expansion provided increased power to examine prenatal influences on development, which were underpowered with Cohort I alone. Over time, the study focus shifted to mirror key developmental and family process milestones. Substudies with the original EGDS Cohort I and II participants examined development during the transition to elementary school (‘School’), child mental health (‘NIMH’), child health (‘Health’), development during the transition to middle school (MSCH’), and adolescent health and behavior (‘ADOL’). For example, in the ‘School’ substudy, new data were collected on school readiness, academic achievement, and stress reactivity (measured by salivary cortisol collection); in the ‘NIMH’ substudy, new data on child and adoptive parent mental health symptoms and diagnoses were collected; in the ‘Health’ substudy, pathways to healthy weight and obesity through the assessment of children’s and parents’ health promotive behaviors (e.g., diet, physical activity, sleep) were examined; in ‘MSCH’ we focused on peer relations, parenting behaviors, and psychological adjustment during the transition to middle school; and in ‘ADOL’ we focused on adolescent risk and protective factors such as substance use, peer relations, and pubertal development and we collected hair samples to measure hormonal changes across adolescence.
Timeline for the EGDS Cohort I, II, and III Studies and Assessments.
Note: The EGDS substudies were supported by the following grants from the National Institutes of Health: Toddlers and School (R01 HD042608); Prenatal (R01 DA020585); NIMH (R01 MH092118); Health (R01 DK090264); MSCH (R56 HD042608); EPoCh (R01 DA035062); ADOL (R01 DA045108); ECHO (UG3/UH3 OD023389). aAssessments are currently ongoing; final n will be higher.

With the launch of the Early Parenting of Children (EPoCh) in 2014, we expanded EGDS to include siblings of the original adoptees. Cohort III EPoCh focused specifically on the original birth families in Cohort I or Cohort II who were parenting a 7-year-old sibling of an originally enrolled adoptee. Finally, ECHO further expanded Cohort III to include all additional siblings age 0−21 who were living in either the adoptive or birth home of a Cohort I or II family. Together with the EPoCh cohort, these siblings comprise the EGDS Cohort III sample. The addition of the Cohort III siblings provided new opportunities to examine within-household differences in child outcomes as a function of child genetics and their rearing environment, and new opportunities to examine differences in biological siblings reared apart as a function of their different rearing environments. Additionally, the ECHO study provided funding to collect longitudinal data on all original EGDS Cohort I, II, and III children, with two assessments between 2016−2023, followed by annual assessments for all enrolled children beginning in 2024. Except for ECHO, assessment activities for the studies shown in Figure 2 are complete.
Sample Description
The full EGDS sample of adoptees includes 561 children across Cohort I and II. Six additional participant types who are associated with the 561 adoptees have also been recruited into EGDS. This includes: (1) 443 additional children in the adoptive family home (Cohort III); (2) 438 additional children in the birth family home (Cohort III); (3) 554 Cohort I and II birth mothers; (4) 210 Cohort I and II birth fathers; (5) 553 adoptive fathers and 567 adoptive mothers from Cohort I and II (numbers do not sum to 561 mothers/fathers because the sample includes 41 same-sex parent families); and (6) 15 additional parents or caregivers in the adoptive family homes and 91 additional parents in the birth family home who began participating in EGDS after the Cohort I and II studies were launched, due to family composition transitions. About half of the children in the EGDS cohorts are male (54.1%), and 53.5% of the children are White, 16.6% are Black or African American, 15.7% are multiracial, 12.7% are Hispanic or Latine, <1% are Asian, <1% are Native Hawaiian or Pacific Islander, <1% are American Indian, and <1% are of unknown ethnicity/not reported. The median Cohort I and II child age at adoption placement was 2 days (M = 5.58, SD = 11.32; range = 0–91 days). Of the siblings recruited into EGDS for Cohort III, 13% (n = 145) are a full sibling to the adoptee, 44% (n = 487) are a half sibling to the adoptee, and 43% (n = 466) are unrelated to the adoptee. The median Cohort III child age at adoption placement for additional siblings in the adoptive family home (for those siblings who were adopted, n = 295) was 2 days (M = 114.62, SD = 424.31; range = 0 to 3870 days). For siblings who were adopted within the birth parent home (n = 5), the median placement date was 1225 days (M = 1507.2, SD = 1510.21; range = 61 to 3512 days). Cohort I and II adopted children’s birthdates range from January 2003 to May 2009, EPoCh Cohort III children’s birthdates range from December 2005 to May 2012, and the additional siblings recruited for ECHO Cohort III have birthdates ranging from August 1996 to July 2018.
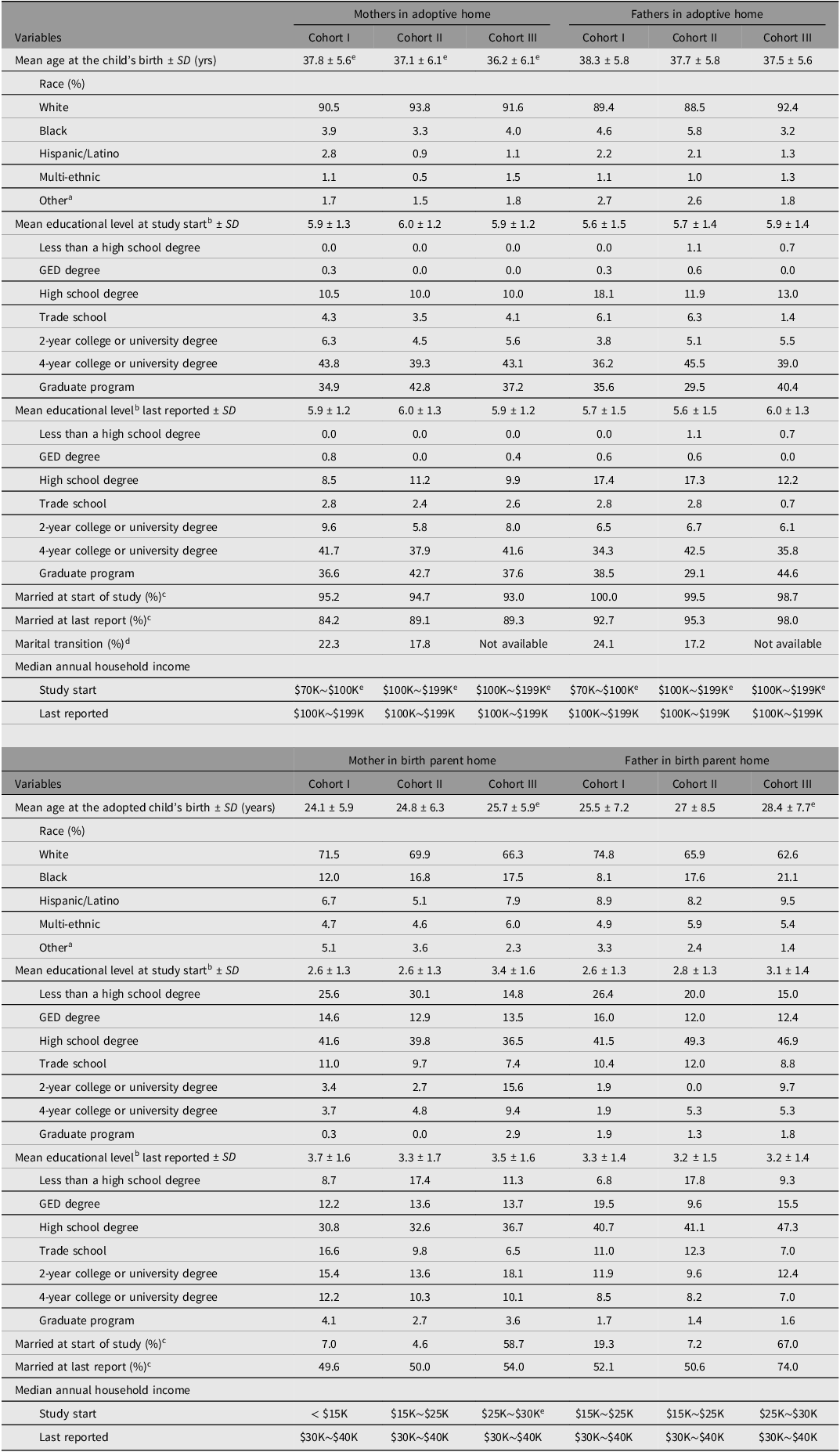
Demographic information regarding parent age, race, ethnicity, education, marital status, and income is provided in Table 1, by Cohorts I, II, and III. Cohort I and II differences in adoptive and birth family characteristics were examined for all demographic variables, and negligible differences were identified. As indicated by these demographic statistics and as noted in our prior publications (Natsuaki et al., Reference Natsuaki, Neiderhiser, Harold, Shaw, Reiss and Leve2019; Reiss et al., Reference Reiss, Ganiban, Leve, Neiderhiser, Shaw and Natsuaki2022), the birth and adoptive parents differed on many demographic characteristics, reflecting the typical pattern of sociodemographic characteristics often found in adoption studies, with adoptive parents having substantially more advantaged socioeconomic backgrounds than birth parents (DeFries et al., Reference DeFries, Plomin and Fulker1994). In addition, birth parents’ highest education level completed and household income levels have continued to rise since the start of the study, whereas the adoptive parents’ highest education and household income have been more stable over time, as was expected based on the parent participants’ ages at study entry.
Early Growth and Development Study (EGDS) sample demographics

a Includes Asian, Native Hawaiian/Pacific Islander, American Indian/Alaskan Native, and Unknown.
b Mean education level is calculated with a 7-point scale ranging from 1 (<high school degree), 2 (GED), 3 (high school degree), 4 (trade school), 5 (2-year college), 6 (4-year college), to 7 (graduate program).
c Includes marriage and living together in a committed marriage-like relationship.
d Includes divorced, separated, widowed/deceased, remarried.
e Statistically significant difference between cohorts at p < .01.
Recruitment Methods and Eligibility Criteria
Recruitment of Cohort I and II birth and adoptive families occurred between March 2003–January 2010, beginning with the recruitment of adoption agencies into the study (N = 45 agencies in 15 states). Recruitment staff were based in the Mid-Atlantic, the West/Southwest, the Midwest, and the Pacific Northwest regions of the U.S. EGDS participants currently reside in 45 U.S. states, the District of Columbia in the U.S., and in four other countries. The study eligibility criteria for Cohort I and II included: (a) the adoption placement was domestic, (b) placement occurred within 3 months postpartum, (c) the infant was placed with an adoptive family that was not biologically related to the child, (d) there were no known major medical conditions such as extreme prematurity or extensive medical surgeries, and (e) the birth and adoptive parents were able to understand English at the 8th-grade level.
All types of adoptive families were eligible for study enrollment (e.g., same-sex parents, single parents, and hearing-impaired parents) and were initially contacted by an adoption agency liaison via mail. Families were given the opportunity to opt out of future study contact by returning a self-addressed, stamped postcard. When adoptive families did not opt out of participating, adoption agency liaisons contacted the birth mothers linked to the adoptive families to describe the study and ask for permission for a study recruiter to contact them directly. When contact was granted, the EGDS birth parent recruiter proceeded with recruitment efforts. Next, the EGDS adoptive family recruiter attempted to recruit the adoptive family using the contact information provided by the adoption agency. Last, project staff attempted to recruit the birth father, either voluntarily through the birth mother or through contact information provided by the adoption agency. See Leve et al. (Reference Leve, Neiderhiser, Shaw, Ganiban, Natsuaki and Reiss2013) for additional recruitment details and a flow chart of the recruitment procedures for Cohort I and II families. Adoption agencies are considered community partners in the research, remaining actively engaged and receiving study newsletters.
For Cohort III EPoCh, the eligibility criteria included: (a) birth mother enrolled in EGDS between 2003 and 2009 following the birth of the EGDS adoptee, (b) birth mother was parenting a biological sibling of an EGDS Cohort I or II adoptee, (c) this biological sibling was born between 2005 and 2012. The EPoCh participants were recruited at biological sibling age 7 from an eligible pool of n = 287 children. Birth parents participating in EPoCh had similar demographic characteristics (race, ethnicity, income, education) as the full sample of EGDS birth parents, with the exception that they were significantly younger t(398) = 4.385, p < .001 than the full sample, likely due to the study inclusion criteria (parenting a 7-year old child at the time of recruitment).
For ECHO, eligibility criteria included: (a) EGDS Cohort I or II birth or adoptive parent participant, (b) family had not withdrawn from the study (n = 32 adoptive families and 13 birth families had withdrawn), (c) birth parent was not deceased (n = 16 birth parents were deceased), and (c) the original Cohort I adoptee, Cohort II adoptee, EPoCh sibling, or additional children aged 0−20.99 were living with either a Cohort I or II birth or adoptive parent participant. Recruitment of siblings in ECHO Cohort III included n = 190 EPoCh siblings, n = 433 additional children in the adoptive family home, and n = 419 additional children in the birth family home. Prior publications compared the demographic information between triads who participated in the EGDS Cohort I and II (N = 561 triads) with those of the eligible nonparticipants (N = 2,391 triads available for analysis) and found minimal systematic sampling biases, suggesting that the EGDS sample is generally representative of the population from which it was drawn (see Leve et al., Reference Leve, Neiderhiser, Shaw, Ganiban, Natsuaki and Reiss2013 for details). In addition, as described in prior reports (Leve et al., Reference Leve, Neiderhiser, Ganiban, Natsuaki, Shaw and Reiss2019), we have found minimal evidence of selective placement and significant variability in the level of contact between adoptive and birth families, but with minimal effects of contact on study predictors or child outcomes. These null findings suggest that statistical assumptions foundational to the adoption design have generally been upheld.
Ethical Considerations in an Adoption Study
A fundamental priority for our research team has been to ensure that EGDS does not actively or inadvertently transmit information between a birth family and an adoptive family. To ensure this firewall is upheld, EGDS has consistently employed separate birth parent and adoptive family recruiters and assessment staff for each family, to ensure that the research team does not transfer information across homes that are linked through adoption. This approach is maintained for assessments, with different staff members interviewing birth family participants versus adoptive family participants, both within a wave and longitudinally. We ask adoptive and birth parents whether children in their home are aware of the adoption, and in the few instances (<2% of families) where a child or partner is unaware, all questions about adoption are not included in the assessment battery. Our measures also refer to ‘parents’ and ‘children’ and not ‘adoptive parents’ or ‘adopted children’. If a participant spontaneously asks questions about the adoption or about their counterpart, study staff do not provide information but instead the participant is referred to their adoption agency. These protocols have been successful. In the 23 years since our recruitment efforts began, we have not had a breach of confidentiality of which we are aware.
Study Procedures and Constructs Assessed
Data collection instruments for EGDS have been selected to maximize harmonization with data from other registries and repositories to facilitate tests of replication and to increase power when cross-registry data are harmonized. For example, in early childhood, we selected temperament and behavior measures such as the Rothbart temperament assessment batteries to align with other twin and adoption studies that focused on early childhood (e.g., the Colorado Adoption Project; Plomin & DeFries, Reference Plomin and DeFries1985) and the Arizona Twin Project (Lemery-Chalfant et al., Reference Lemery-Chalfant, Oro, Rea-Sandin, Miadich, Lecarie, Clifford, Doane and Davis2019). Beginning in 2016, with our participation in a National Institutes of Health cooperative grant, Environmental Influences on Child Health Outcomes (ECHO; Blackwell et al., Reference Blackwell, Cella, Adair, Cordero, Das, Elliott, Hipwell, Jacobson, Neiderhiser, Stanford, Wright and Gershon2024; Knapp et al., Reference Knapp, Kress, Parker, Page, McArthur, Gachigi, Alshawabkeh, Aschner, Bastain, Breton, Bendixsen, Brennan, Bush, Buss, Camargo, Catellier, Cordero, Croen and Dabelea2023), we included measures of five child outcomes: pre-, peri-, and postnatal outcomes; obesity; airways health; neurodevelopment; and positive health. Data from these five child outcomes are harmonized within a consortium of 69 cohort sites across the U.S. and Puerto Rico. Since its onset, we have also selected measures that are widely used in child development research, and where possible, are freely available at no charge (e.g., Gershon et al., Reference Gershon, Wagster, Hendrie, Fox, Cook and Nowinski2013).
EGDS assessment methods have included self-reported surveys, in-person interviews, and standardized testing for birth parents, adoptive parents, and children, with more than 340 unique measures administered and more than 2300 individual measures when considered by respondent by study wave. At the psychological construct level, this includes questionnaire and diagnostic interview approaches for all participants, observational assessments and teacher questionnaires for adoptive and EPoCh families, and official arrest records for birth parents. For physical health constructs, adoptive families completed food and activity diaries, and medical records were collected for birth parents, adopted children, and birth children. Biomarker data has included DNA collection from all participants, diurnal cortisol measures from adopted children, EPoCh children, and birth parents, and puberty-related hormones assayed from hair samples from adopted children. After children were enrolled in ECHO, additional biospecimen collections included shed teeth, urine samples, hair samples, and spirometry. Assessments were generally conducted in person during early and middle childhood, and via remote and virtual visit approaches in adolescence. A full listing of study measures by child age is available at https://egds.la.psu.edu/measures/. De-identified longitudinal data collected as part of the ECHO consortium are available through NICHD’s Data and Specimen Hub (DASH), (https://dash.nichd.nih.gov/). In addition, as discussed in the next section, we routinely share EGDS de-identified data with external colleagues throughout the U.S. and Europe following receipt of a signed data security policy, data use agreement, and submission of a project abstract to facilitate cross-cohort analyses, partnering with more than 70 different external collaborators to date.
Leveraging Multiple Study Designs to Advance Knowledge About Genetic and Environmental Contributions to Child Development
There are many different types of genetically informed designs, each with unique strengths. The primary strengths of the prospective parent-offspring adoption design (Cohorts I and II) and our adoptee-sibling addition (Cohort III) are their ability to identify genetic influences at the whole genome aggregate level (not specific to particular alleles), the elimination of passive rGE, and the ability to detect G × E and evocative rGE. Specifically, because the adoptive parents are genetically unrelated to their adopted children, passive rGE is eliminated and associations between the birth parent(s) and adoptive parent(s) reflect a heritable effect transmitted from birth parent to the child, which then can evoke a predicted response from the rearing parent. In twin studies and other designs where the rearing parents and child are genetically related, it is more complex to disentangle the effects of the child’s genes from those of their parents when examining associations between parent and child phenotypes, as evocative rGE associations may be confounded by passive rGE effects. The inclusion of full and half siblings of the adoptee in the birth home provides additional leverage to isolate rearing environmental influences, by examining similarities and differences in child outcomes in genetically related sibling pairs who are reared apart and often living in quite different household environments. For example, if the full- and half-sibling pair correlations on depressive symptoms for siblings reared apart are about the same as those for the genetically unrelated sibling pairs living in the same home, we can infer environmental causes, and then test hypothesized environmental mechanisms (e.g., parenting behaviors, socioeconomic conditions). Inclusion of siblings in the adoptive home (either related to the adoptive parents, or unrelated) provides a further avenue to examine sibling pair similarities and differences among children reared in the same household, because shared genes and passive rGE may be present for one child-parent dyad but not for another child-parent dyad within the home. Because most other sibling studies include family members who are genetically related, and most twin studies include twins reared together, when EGDS data are harmonized with other sibling and twin datasets, novel insights can be made about the transmission of behavior across generations and the joint roles of genetic, prenatal, and postnatal environmental factors beyond what any single genetically informed study can do independently.
Results
Sampling of EGDS Manuscripts That Have Integrated Data Across Cohorts and Datasets
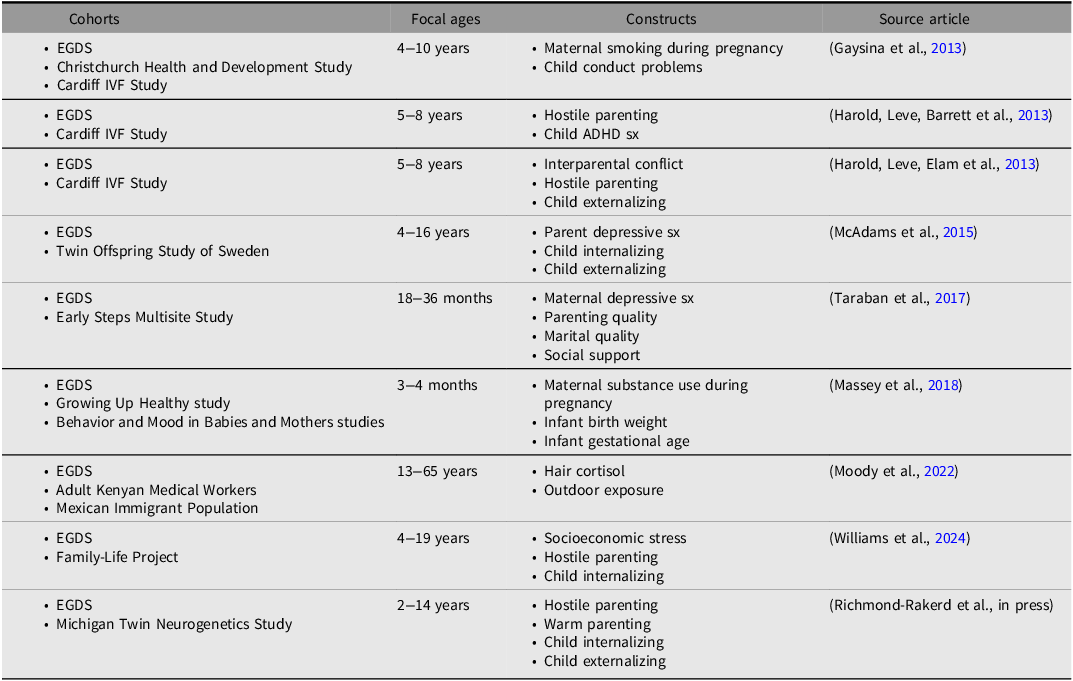
Our collaboration with national and international colleagues to aggregate EGDS data with data from other cohorts has led to replication and extension of findings related to the role of genetic and environmental influences and their interaction and/or correlation on children’s psychological development from early childhood to adolescence. Table 2 provides a sampling of published manuscripts that have harmonized data from one or more of the EGDS cohorts with data from another registry or cohort. In addition, EGDS data are included in dozens of manuscripts from the ECHO consortium that examine environmental influences on child development, for which public summaries can be located here: https://echochildren.org/research-summaries/. Further, most of our publications since 2015 aggregate data from Cohorts I and II and often include data from Cohort III.
Sampling of manuscripts using EGDS data alongside data from another cohort(s) to test hypotheses related to genetic, environmental, and/or prenatal influences on child development

As shown in Table 2, multicohort papers that include EGDS have aggregated data across multiple studies and design types, including: (1) studies that examined associations between maternal substance use during pregnancy and child outcomes in EGDS participants as compared to studies of children reared with one or both biological parents (e.g., Gaysina et al., Reference Gaysina, Fergusson, Leve, Horwood, Reiss, Shaw, Elam, Natsuaki, Neiderhiser and Harold2013; Massey et al., Reference Massey, Mroczek, Reiss, Miller, Jakubowski, Graham, Shisler, McCallum, Huestis, Ganiban, Shaw, Leve, Eiden, Stroud and Neiderhiser2018). This approach allows for examination of prenatal influences on development by comparing patterns of association in children who have different prenatal and postnatal parents relative to children who have the same prenatal and postnatal parents. Our findings have indicated that associations between prenatal maternal substance use and child psychological and health outcomes are identifiable even when the pregnant mother and the rearing parent are not the same person, adding robustness to the literature on the causal effects of prenatal substance use. (2) Studies that have confirmed the causal role of the rearing environment by examining the role of passive rGE through a comparison of associations between parenting behaviors and the marital relationship with child psychopathology between EGDS children (no genetic relationship to their rearing parents) with findings from the Cardiff IVF study where the children are either genetically related to one (egg or sperm donor), both (homologous IVF), or neither (embryo donation) rearing parent (e.g., Harold, Leve, Barrett et al., Reference Harold, Leve, Barrett, Elam, Neiderhiser, Natsuaki, Shaw, Reiss and Thapar2013; Harold, Leve, Elam et al., Reference Harold, Leve, Elam, Thapar, Neiderhiser, Natsuaki, Shaw and Reiss2013). (3) Studies that examine comparability of findings between EGDS and culturally and economically diverse populations, such as the Family-Life Project, Adult Kenyan Medical Workers, and Mexican Immigrant populations (e.g., Moody et al., Reference Moody, van Dammen, Wang, Greder, Neiderhiser, Afulani, Willette and Shirtcliff2022; Williams et al., Reference Williams, Oro, Blackwell, Liu, Miller, Ganiban, Neiderhiser, DeGarmo, Shaw, Chen, Natsuaki and Leve2024) to examine generalizability of EGDS findings to other cultures and contexts, identifying the importance of attending to culture when examining psychosocial outcomes. (4) Studies that compare findings between EGDS and other national twin registries, including the Michigan Twin Neurogenetics Study within the broader Michigan State University Twin Registry (Burt & Klump, Reference Burt and Klump2019) and the Twin and Offspring Study in Sweden (TOSS; Neiderhiser & Lichtenstein, Reference Neiderhiser and Lichtenstein2008), to replicate patterns of findings regarding the genetic and environmental underpinnings of associations between parent and child phenotypes using different intergenerational design approaches (e.g., McAdams et al., Reference McAdams, Rijsdijk, Neiderhiser, Narusyte, Shaw, Natsuaki, Spotts, Ganiban, Reiss, Leve, Lichtenstein and Eley2015; Richmond-Rakerd et al., in press). Finally, (5) studies that compare findings between EGDS and participants in randomized controlled trials such as the Early Steps Multisite Study (Dishion et al., Reference Dishion, Shaw, Connell, Gardner, Weaver and Wilson2008), replicating patterns of findings in associations between parental mental health symptoms and parenting where participants in one of the cohorts have undergone a parenting intervention (Taraban et al., Reference Taraban, Shaw, Leve, Wilson, Dishion, Natsuaki, Neiderhiser and Reiss2017). Through these multicohort strategies, we have both been able to showcase the unique design features of EGDS, while demonstrating replication and reproducibility of findings — an analytic strategy that we plan to continue going forward.
Discussion
Accessing EGDS Data
Current funding is ongoing until 2030 and includes data collection activities for EGDS families until participants turn age 21. EGDS data previously collected using common data elements from the ECHO study are available on the NICHD data and specimen hub (https://dash.nichd.nih.gov/) (DASH) by searching for ‘ECHO’ (Gillman, Reference Gillman2025). As of August 2025, this repository includes data collected through October 31, 2023 on a range of variables, including: sociodemographics, child and family health history, pregnancy-related variables, child health behaviors and lifestyle, child neurodevelopmental health and functioning, built physical environment, home social environment, caregiver psychosocial, child physical health and functioning, child social role performance and functioning, child sleep health, child well-being, and nonomics bioassay results. The repository includes the data collection instruments, a codebook, de-identification methodology, and a training manual, among other resources. Because ECHO is a national program that includes data from 69 pediatric cohorts, as of October 31, 2023, it includes data from 36,027 pregnancies (among 24,370 pregnant persons) and 35,353 children (the EGDS cohorts are included within these numbers). ECHO is currently focused on maintaining longitudinal data for participants previously enrolled in ECHO and recruiting and assessing parents during new pregnancies. For this reason, over time, there will be an increasing number of sibling pairs in ECHO that can be accessed for behavioral genetic sibling-based analyses. As of August 2025, there were 3489 sibling pairs (i.e., families with more than 1 child) from 43 different cohorts in ECHO, accessible via DASH. There is typically a 12-month lag from the time of data collection to deposit of the data in DASH, and a query of the nonpublic database indicated that there were 5376 families with more than 1 child in ECHO, suggesting that the DASH sample size will increase by approximately 2000 each year through 2030. All participant IDs in the ECHO DASH dataset are linked through their biological mother. Participant IDs with identical values in the first 7 characters of the child participant ID are linked siblings (through the biological mother), and can be selected for linked sibling analyses using these first 7 digits. When the first 7 digits differ across two participant IDs, this indicates that the children do not share a biological mother. In addition, the rearing parent type (adoptive) can be selected to identify children who are not being reared by their biological mother, to conduct parent-offspring adoption studies. ECHO protocols also required the collection of DNA samples for genomic analyses. Genotyping has been completed on 21,904 children, 12,685 biological mothers, and 791 biological fathers who participated in the first 7 years of ECHO. The genotyped data will be made available on dbGaP (https://dbgap.ncbi.nlm.nih.gov/home/) on a timeline determined by the National Institutes of Health.
The EGDS team is eager to continue our multicohort approach and engage in new collaborative efforts to share de-identified data from EGDS with a broad range of researchers. The EGDS is unique and can effectively address complex questions about the intersecting influences of genetics, prenatal exposures, and postnatal environmental experiences on child and adolescent development.
Data availability
De-identified data are publicly available through NICHD’s Data and Specimen Hub (DASH), (https://dash.nichd.nih.gov/) or by contacting the corresponding author.
Acknowledgments
We thank the birth and adoptive parents and all the youth who participated in this study, and the adoption agencies who helped recruit study participants. Special gratitude is given to David Reiss, who founded the original study and was instrumental in the study activities until his retirement in 2023; to current consultants and co-investigators, Chang Liu, Kristine Marceau, Misaki Natsuaki, Theda Rose, and Daniel Shaw; to Sally Guyer for data management; to study coordinators, recruiters, data teams, and assessors; and to our collaborators and co-authors who tested hypotheses using study data.
Financial support
This project was supported by R01 HD042608, NICHD, NIDA, and OBSSR, NIH, U.S. PHS (PI Years 1–5: David Reiss; PI Years 6–10: Leslie Leve), R01 DA020585 NIDA, NIMH, and OBSSR, NIH, U.S. PHS (PI: Jenae Neiderhiser), R01 MH092118, NIMH, NIH, U.S. PHS (PIs: Jenae Neiderhiser and Leslie Leve), R01 DK090264, NIDDK, NIH, U.S. PHS (PI: Jody Ganiban), R01 DA035062, NIDA, NIH, U.S. PHS (PI: Leslie Leve), R56 HD042608, NICHD, NIH, U.S. PHS (PI: Leslie Leve), R01 DA045108 (PI: Jenae Neiderhiser), and UG3/UH3 OD023389, Office of the Director, NIH, U.S. PHS (PIs: Leslie Leve, Jenae Neiderhiser, and Jody Ganiban). The content is solely the responsibility of the authors and does not necessarily represent the official views of the Eunice Kennedy Shriver National Institute of Child Health & Human Development, the Office of the Director, or the National Institutes of Health.
Competing interests
No authors have a conflict of interest.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.


 Open access
Open access