

Introduction
To shape meaningful and inclusive clinical research, it is essential to understand how patients, patient advocates, and researchers collaboratively navigate the complexities of co-designing clinical trial protocols, especially for conditions with widespread impact such as Long COVID. Also known as post-acute sequelae of SARS-CoV-2 infection, Long COVID is a chronic condition that occurs after a SARS-CoV-2 infection and persists for at least 3 months. It can manifest as a continuous, relapsing, remitting, or progressive disease state affecting one or more organ systems [1].
Diagnosis of Long COVID is currently symptom-based, with more than 200 symptoms reported through various studies [Reference Davis, Assaf and McCorkell2]. People living with Long COVID have challenged scientific narratives and advocated for recognition and support for this condition through firsthand accounts and collective efforts. The lived experiences of patients have not only provided crucial evidence for the existence and impact of Long COVID but also highlighted the need for patient-centered approaches in research and healthcare, ensuring that the voices of those directly affected are heard and valued in the scientific and medical communities [Reference Callard and Perego3].
Engagement of patients and patient advocates in research design has been associated with more patient-centered outcome measures, more meaningful results, increased adherence to study intervention and procedures, and improved dissemination and uptake of results [Reference Concannon, Fuster and Saunders4,Reference Domecq, Prutsky and Elraiyah5]. As a result, funding agencies such as the Patient-Centered Outcomes Research Institute (PCORI) have made patient engagement a central requirement for the pragmatic clinical trials it funds. Increasingly, the National Institutes of Health (NIH) has also recognized the value of patient and community engagement and has required dedicated personnel and milestones for its research programs. In many of these situations, researchers and patients have had time to build trusting and collaborative relationships, with many engaged research projects taking years to establish their community partner relationships. PCORI offers guidance on best practices in conducting research with teams of multiple stakeholders, and their recommendations include creating a shared vision, defining roles and responsibilities, and establishing team norms [6].
When the NIH formed the Researching COVID to Enhance Recovery (RECOVER) Initiative in February 2021 to support research focused on understanding and treating Long COVID, it created a robust structure that included patients, caregivers, and community representatives (Representatives). The goal of involving Representatives was to ensure that RECOVER would meet the needs of people affected by Long COVID. The RECOVER engagement strategy incorporates grounding principles to guide the inclusion of Representatives in all steps of the research process [7].
Inclusion of Representatives began with the RECOVER Observational Cohort Studies led by NYU Langone Health. The first group of Representatives was nominated by researchers from RECOVER study sites and through input from other researchers working on different initiatives across NIH, such as the Community Engagement Alliance, a research network designed to work with communities and community-based organizations [8]. This led to the formation of the RECOVER National Community Engagement Group (NCEG), which includes Representatives from a variety of backgrounds to advise RECOVER research. The NCEG recommended that all committees in RECOVER include Representatives so that voices with lived experience could be heard at every level and the work could be meaningful to those impacted by Long COVID.
In July 2022, the NIH launched a simultaneous effort within RECOVER that focused on identifying potential treatments for Long COVID and announced the Duke Clinical Research Institute (DCRI) as the RECOVER Clinical Trials Data Coordinating Center (CT-DCC). DCRI, under the direction of the NIH, was tasked with quickly and simultaneously launching five Long COVID clinical trial platforms. CT-DCC tasks for each platform protocol included facilitating NIH-directed working groups to develop protocols, identifying and contracting sites, and launching trials in less than a year. The five Protocol Working Groups (PWGs) were centered around the following mechanisms and symptoms of Long COVID: (1) viral persistence and dysregulated immune systems, (2) exercise intolerance, (3) sleep disturbances, (4) autonomic dysfunction, and (5) neurologic dysfunction.
Individuals who have lived experience with Long COVID often become experts beyond their patient journey and are knowledgeable about the current science around post-viral syndromes. The World Health Organization has developed guidelines for good participatory practice for trials of emerging and re-emerging pathogens. These guidelines are designed to effectively engage stakeholders in the design, conduct, and dissemination of prevention and treatment trials for pathogens for which few or no medical countermeasures exist. The guidelines emphasize the importance of authentically engaging stakeholders throughout the trial life cycle to enhance both the quality and outcomes of research [9].
While national and international initiatives have provided valuable guidance on patient and public involvement across the research continuum [10–12], there remains limited evidence for initiating systems that support the complementary expertise of patients, patient advocates, scientists, and trialists within a network tasked with the rapid design and implementation of clinical trial protocols. In this paper, we describe the protocol development efforts of the RECOVER clinical trial PWGs with an emphasis on patient and patient advocate voices, and key lessons learned that could serve as a roadmap for future clinical trial network endeavors.
Methods
Overview of PWGs
One of the overarching goals of developing the RECOVER clinical trial protocols was to have a broad range of expertise coming together from across the country to identify potential treatments for Long COVID. Thus, the NIH invited scientific experts pertinent to Long COVID mechanisms or specific signs or symptoms to participate in a PWG for each identified platform symptom area. In addition, investigators who submitted interventions prioritized by NIH leadership for study in clinical trials joined the relevant PWGs, as well as an expert in clinical trials, statistician, and project leader from DCRI. Guiding principles for the PWGs included development of a master protocol structure that could support testing multiple interventions with common inclusion/exclusion criteria and endpoints; alignment with longitudinal cohorts and across the five platform protocols; assurance that the various protocols enabled diverse and inclusive trials and could be developed and implemented rapidly; and inclusion of individuals affected by Long COVID (Representatives) as key members of the PWGs.
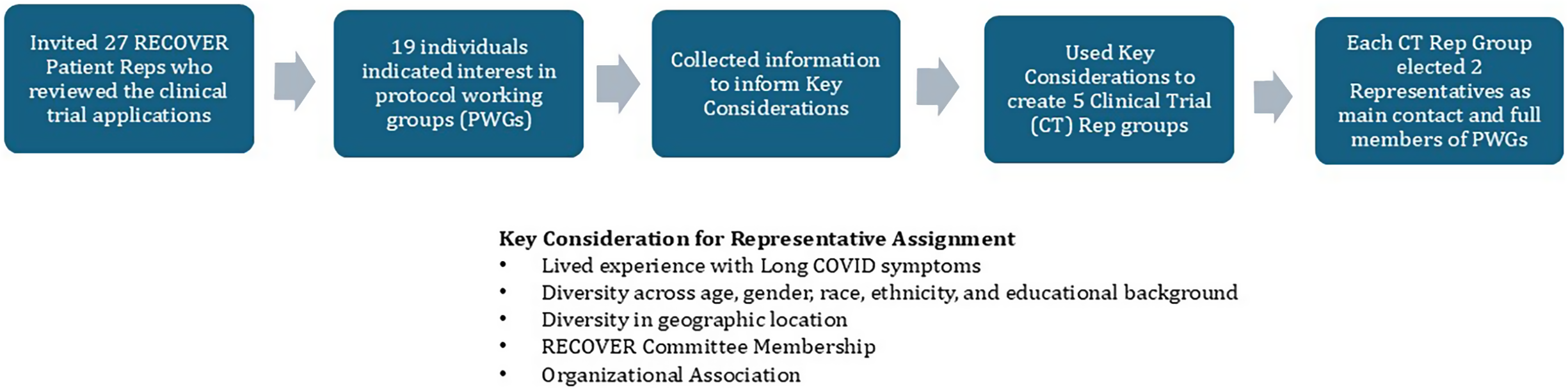
Representatives who had participated in prior RECOVER observational activities or reviewed the intervention and study proposals submitted by investigators to the NIH for the clinical trials were invited to be part of the protocol development process. The RECOVER CT Engagement Team surveyed the Representatives to determine their experience with a particular Long COVID symptom, such as lived experience or advocacy, as well as their demographics (with the goal of balancing the groups based on race, gender, and geography). The Engagement Team then assigned Representatives into groups for each platform protocol. At the first group meeting, Representatives were asked to nominate two people from the group to serve on the PWG. As an exception, to facilitate the rapid development of the first planned clinical trial, two Representatives from the RECOVER Clinical Trial Steering Committee were selected to serve on that PWG. Figure 1 illustrates the RECOVER PWG Representative selection process.
RECOVER protocol working group patient representative (Reps) selection process.

Representative roles and responsibilities
The two Representatives in each PWG attended and contributed to meeting discussions, reviewed draft documents, offered feedback during the development process, and shared their insights back to their Representative group for additional feedback. Representatives involved with the PWG, along with all members of the PWGs, were asked to review and provide feedback on the study design and informed consent form, with a focus from the patient’s perspective on inclusion/exclusion criteria, endpoints of interest, number of clinic visits, and participant compensation; the Representatives were also asked to focus on access for participants, burden of participation, and balancing the impact to participants against the importance of information and data collected. All final decisions related to protocols were made by PWG Study Co-chairs and NIH after collecting feedback from the PWG members. PWG members were expected to dedicate up to 20 hours of time before the protocol’s initial submission to the central Institutional Review Board. Compensation was provided to all PWG members for their time, including Representatives.
Support for Representatives
During the process of protocol development, the RECOVER CT Engagement Team followed the Clinical Trials Transformation Initiative elements for successful collaboration between patient groups and sponsors of clinical trials. These elements highlight the importance of establishing meaningful partnerships, demonstrating mutual benefits, and collaborating as partners from the planning stage forward [Reference Bloom, Beetsch and Harker13]. The Engagement Team aimed to provide ongoing support for Representatives to ensure their lived experience knowledge was integrated. A member of the Engagement Team attended each PWG meeting with Representatives and met with them separately to help identify questions and provide any clarification needed on the protocols or other scientific documents. The Engagement Team documented Representative feedback in the PWG and other meetings and shared the information with the leadership of the PWG, DCRI leadership, and NIH leadership overseeing the protocol development process. Later in the protocol process, weekly emails were sent to Representatives to update them on developments, such as Data and Safety Monitoring Board review. Additionally, smaller meetings occurred with Representatives, the Engagement Team, PWG Study Co-chairs, and NIH to amplify Representatives’ insights, answer their questions, and foster a co-learning environment. Nevertheless, some Representatives expressed concerns that their expertise was not being meaningfully incorporated into the study design. This prompted the idea of gaining structured feedback from PWGs to better understand and inform best practices for engagement in future clinical trial development efforts.
Evaluation
To assess the experience of PWG participants and particularly Representatives’ perception about how their feedback was incorporated, the DCRI Engagement Team and RECOVER Clinical Trials leadership team developed an online survey that would be administered via Qualtrics (Provo, UT). The full survey is provided in the Supplementary Material. This questionnaire was designed using an iterative process, with initial questions largely based on the PCORI Engagement Assessment Tool, which is designed to assess inclusion, equitable partnership, accountability and actionability [14]. Input was obtained from Engagement Team Leads from the larger RECOVER effort, co-chairs of the RECOVER NCEG, two Representatives on the PWGs, and NIH.
The survey inquired about the general PWG role of the respondent (i.e., Representative, PWG Co-Chair, subject matter expert, or operational project leader) and whether the role seemed clearly defined, met expectations, was personally or professionally beneficial, and felt valued. The survey also explored participants’ previous experiences and knowledge of research and the research process, as well as their experience working with and engaging patients, patient advocates, and caregivers. It assessed individuals’ perceptions of the value they brought to the development of the trial protocol and the level of inclusion of patients, patient advocates, and community members as equal participants on the team. Additionally, the survey offered space for respondents to provide free-text responses, express concerns, and make recommendations.
The survey was distributed via email on February 27, 2024, to all members of the five PWGs, including all four Representatives connected to each platform protocol, operational project leaders, Co-chairs of the PWGs, and subject matter experts. On March 14, 2024, a reminder email and second invitation to share their experience was sent to all participants, and the survey was closed on April 28, 2024. The survey findings were reviewed during a series of meetings involving the full authorship team, which included a Representative.
Results
The survey was distributed to 69 members of the five PWGs. To provide confidentiality, the survey did not request the name of the person completing the survey or the name of the protocol that they helped develop. Twenty-eight members participated in the engagement survey, which included just 41% of Representatives. Among them, nine identified as Representatives, eight were PWG Co-Chairs or co-investigators, eight were clinical subject matter experts invited to RECOVER for their scientific expertise, and three were operational project leaders. Of the nine Representatives, seven (78%) identified as patient advocates, and eight (89%) identified as individuals with Long COVID; respondents were able to select more than one category. In addition, the race, ethnicity, socioeconomic status, and research experience of the Representatives were quite homogenous, with the vast majority of those participants being non-Hispanic White and having research experience.
Twenty (71%) respondents answered positively regarding meaningful contribution to the trial protocol and feeling that their contribution was valued. Twenty-three (82%) respondents had a high or moderate level of understanding about the research process prior to joining the RECOVER PWG, and 21 (75%) respondents had a moderate (14) or high (7) level of prior experience regarding patient, caregiver, and community engagement in health research prior to joining the RECOVER PWG. However, 13 (46%) survey respondents either were neutral, disagreed, or strongly disagreed with the statement that their roles were clearly defined as members of the PWG.
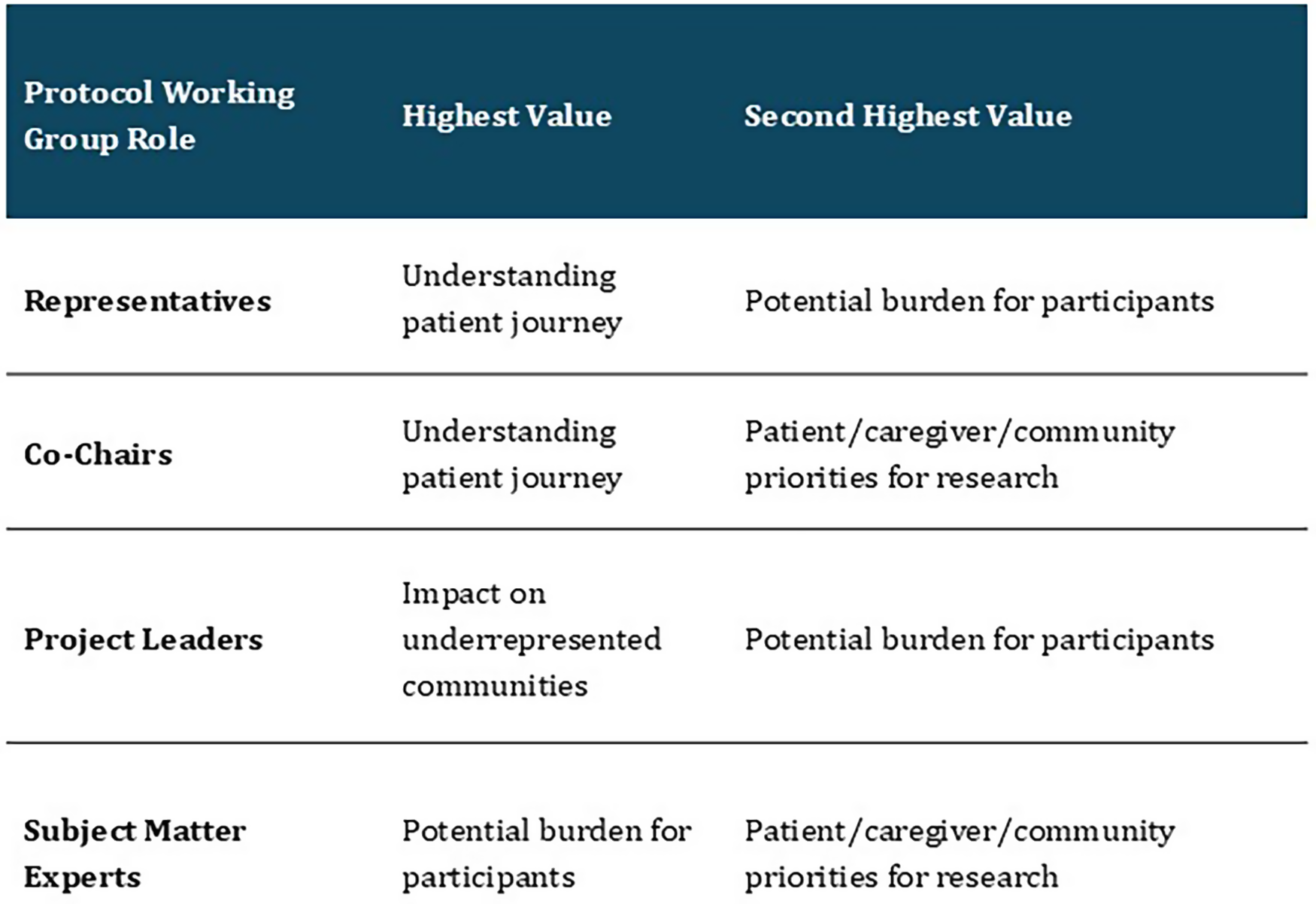
Twenty-three (82%) respondents noted that Representatives were somewhat valued, valued, or highly valued by the PWG team. In response to the question “What value has patient, caregiver, and community inclusion brought to the project of developing the clinical trial protocol?,” perceptions varied across respondent roles. These role-specific perspectives on the value of inclusion are presented in Figure 2.
Perceived value of patient, caregiver, and community inclusion in clinical trial protocol development across working group roles.

Based on results from another question, opinions were variable as to how well Representatives were included as equal members of the protocol development team; on a Likert scale of 0 to 4, with 0 equating to “not at all” and 4 equating to “completely,” six (21%) respondents recorded a 0 or 1, and 13 (46%) recorded a 3 or 4. Six (21%) respondents recorded a 1 or 2 in regard to clinical subject matter experts being included as equal members of the PWG. Opinions regarding equal inclusion of other groups, including operational project leaders, PWG Co-chairs or co-investigators, or clinical subject matter experts, were more heavily weighted toward an answer of 3 or 4.
When respondents were asked “What went well?,” responses were also highly variable, ranging from “nothing” to “I think people were working in good faith, but the process got in the way of success” to “We had a nice group of people. There was a mutual respect for reps though the group did not always have the authority/ability to address rep concerns.” Notably, those who identified as Representatives also had highly variable responses regarding what had gone well, including the following:
-
• “Nothing truly. The chosen treatments were extremely low quality and the team was unable to justify them. During the protocol development it became clear that all members, including heads, were unfamiliar with the patient population, including basic symptoms like PEM.”
-
• “Listening to the feedback and coming together to find a solution in the middle.”
-
• “The collaboration led to instrumental changes in the protocol design.”
-
• “The protocol changed and another protocol was developed that fit the needs of the [Long COVID] community and caused less harm to participants…”
-
• “As a representative I felt my voice was listened to and valued.”
When respondents were asked “What did not go well?,” responses were also highly variable, ranging from “nothing went well” to “I thought the investigators were oversold on their pet therapeutic approaches” to “There was no transparency in why the treatments were selected.” Several respondents expressed concerns that WG experts were not knowledgeable.
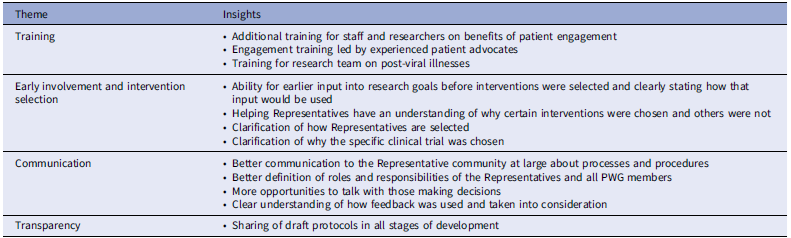
The dominant themes and responses to a survey question about additional resources that could have better supported Representatives’ involvement in the protocol development are captured in Table 1.
Survey results regarding what additional resources could have better supported Representatives

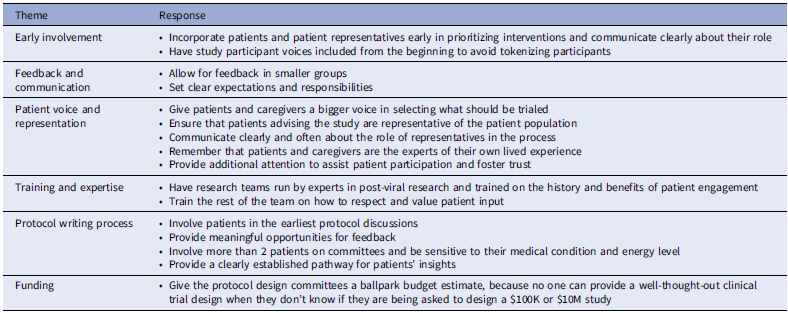
Table 2 shows the themes and responses when participants were asked what advice they would give to individuals who run clinical trial research and future funders about how to best incorporate the participant voice. Direct quotes from the participants are presented below, organized by role to emphasize the unique priorities each group brought to the process. The quotes highlight actionable recommendations for improving protocol development.
Survey results regarding advice that respondents would give to individuals who run clinical trial research and future funders about how to best incorporate the participant voice

Participant perspectives by role
-
• Patient, caregiver, or community representative
-
○ “Ensure that the team is familiar with the patient population and their specific needs, including symptoms like [post-exertional malaise]. Improve the quality of chosen treatments and justify them clearly.”
-
-
• Operational project leader/associate project lead
-
○ “Maintain open communication and collaboration among team members to ensure all perspectives are considered and integrated effectively.”
-
-
• PWG co-chair or co-investigator/appendix principal investigator
-
○ “Engage all team members fully to enhance the overall progress and quality of the protocol.”
-
-
• PWG team member – clinical subject matter expert
-
○ “Improve communication and coordination among team members to avoid misunderstandings and inefficiencies.”
-
The survey findings highlight the variability of experiences for individuals with different roles, expertise, and expectations in collaborating to develop clinical trial protocols for Long COVID, as well as challenges and tension that can arise.
Discussion
The goal of the multi-stakeholder collaborative PWG was to meld complementary expertise to create clinical trials that could further the body of knowledge for the treatment and management of Long COVID. This goal was particularly challenging because Long COVID is a new condition, and critical knowledge around Long COVID was evolving as the PWGs were developing the protocols. This was an opportunity to learn together and build from individual expertise about aspects of the condition but also led to a steep learning curve and potential differences in perspectives related to what to prioritize.
Notably, the RECOVER Clinical Trial Initiative was structured in a way that is unfamiliar to most NIH researchers; NIH program officers or designees were involved in many procedural processes, including the formation of the PWGs. All scientific decisions required approval from NIH leadership, and the process for obtaining approvals as well as the timeline and decision-making roles at NIH were sometimes not clearly defined.
Most respondents felt that Representatives were valuable and valued throughout the protocol development process and offered both understanding to the patient journey and impact on protocol design. Notably, not all Representatives perceived themselves and their perspectives as valued throughout the process. Providing meaningful opportunities for both feedback and influence is a critical aspect of engagement, and although RECOVER CT PWG Representative feedback was captured in a centralized tracking document and shared as part of the PWG involvement, we learned through the survey that not everyone was informed adequately about how their insights were incorporated within the protocol.
The discrepancy between how some PWG members perceived Representatives were treated and how the Representatives themselves felt about their participation is significant. The development of a RECOVER protocol required the rapid formation of an interdisciplinary working group, adherence to compressed timelines, and sustained commitment from team members to this high-impact project – conditions that can intensify group stress and strain communication [Reference Stivers and Tate15,Reference Liu and Liu16]. Moreover, patient engagement can take a variety of formats, ranging from giving input in a focus group to active participation in the design and execution of clinical trials (including roles such as co-designing study protocols and providing direct feedback on the research process) to partnering in decision-making on trial operations [17,Reference Lauzon-Schnittka, Audette-Chapdelaine, Boutin, Wilhelmy, Auger and Brodeur18]. Clear alignment on the role of patient representatives by all members of a collective team such as the PWGs is critical, as divergent opinions may otherwise emerge regarding how the representatives are valued. Difference in engagement experiences across groups highlights persistent challenges in achieving equitable participation with the protocol development phase. This finding highlights the need to better establish roles and responsibilities and communication channels for both patient representatives and research teams to avoid misalignment in future research.
Several considerations are important when interpreting these findings. These respondents do not reflect all patients with Long COVID or most patient populations for other disease processes. Both the limited response rate and the homogenous nature of Representatives may limit generalizability of Representative opinions on the process of engagement in study design and conduct. While these findings suggest early progress in patient engagement efforts, interpretation is limited by both the small sample size and the use of a survey-based approach. The heterogeneity observed across participant subgroups indicates that engagement experiences are likely context-dependent and may not be fully captured through structured survey instruments alone. Future assessments of patient engagement within networks would benefit from complementary qualitative or mixed-methods approaches to more fully characterize engagement processes and perceived value. Nonetheless, lessons learned from the overall process of protocol development are likely generalizable to other networks seeking to include the voices of patients/patient advocates/community members, subject matter experts, and operational experts.
Based on our findings, we recommend the following:
-
• Include individuals with lived experience as part of the study leadership team [Reference Maurer, Mangrum and Hilliard-Boone19].
-
• Invest in relationship building through dedicating adequate time to foster trust building among scientists, patients/patient advocates, and community members to support a shared purpose and collaborative protocol development [17,Reference Nielssen, Santana and Pokharel20,Reference Brockman, Balls-Berry and West21].
-
• Clarify roles and expertise levels, and have transparent pathways for decision-making, to reduce confusion and misalignment [17].
-
• Develop respectful meeting norms that value the complementary expertise of all members and ensure representatives’ perspectives are prioritized through responsive participation such as dedicated agenda time and focused small-group or one-on-one meetings [Reference Carman, Dardess and Maurer22].
-
• Ensure that researchers are educated on the complex and variable symptoms, especially for conditions that may be subjective and lack validated markers [Reference Li, Zhou and Ma23].
-
• Provide structured co-training opportunities that bring researchers together with patient and community partners to establish a shared foundational understanding of the research process. Training should support researchers in inclusive engagement practices and provide patient and community members with training on study protocol development and research literacy [Reference Bell, Vat and McGavin24].
-
• Implement clear co-design standards and reporting frameworks that set transparent expectations, specify how representatives’ feedback is collected and used, and define resolution pathways when perspectives differ [Reference Vargas, Zorbas and Longworth25].
Conclusion
The RECOVER PWG experience demonstrates that meaningful engagement of patients and community representatives in clinical trial design is both feasible and valuable, but not without challenges. Clear role definitions, transparent decision-making, and intentional communication are essential to avoid misalignment and ensure that lived experience informs protocol development. Future efforts should prioritize early and sustained engagement, training for all members, and mechanisms to incorporate diverse perspectives. These practices are critical to advancing inclusive, patient-centered research and improving outcomes for those affected by Long COVID and other complex conditions.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/cts.2026.10702.
Acknowledgments
Peter Hoffmann of the DCRI provided editorial support. The authors are entirely responsible for the scientific content of the paper. The paper adheres to the journal’s authorship policy.
Author contributions
Renee Leverty: Conceptualization, Methodology, Writing-original draft, Writing-review & editing; Sonya Sutton: Conceptualization, Methodology, Writing-review & editing; Charnesia Jackson: Conceptualization, Methodology, Writing-review & editing; Marta Cerda: Methodology, Writing-review & editing; Alain Chang: Methodology, Writing-review & editing; Kanecia Zimmerman: Conceptualization, Methodology, Writing-original draft, Writing-review & editing.
Funding statement
This research was funded internally as well as by the National Institutes of Health Agreement OT2HL156812 through the RECOVER program. The views and conclusions in this document are those of the authors and should not be interpreted as representing the official policies, either expressed or implied, of the NIH.
Competing interests
The authors declare that they have no competing interests.
Ethical standard
This research project, article, and the survey described herein are overseen by Duke University Campus Institutional Review Board Office, Pro00115193.



 Open access
Open access