


Introduction
The prevalence of chronic diseases has risen steadily in recent decades, posing a significant challenge to global healthcare systems, as highlighted by the substantial burden of conditions such as cardiovascular diseases, diabetes and chronic respiratory diseases (Wagner et al., Reference Wagner, Austin, Davis, Hindmarsh, Schaefer and Bonomi2001; World Health Organization, 2023). Particularly, the increase in multimorbidity, where people have two or more chronic conditions simultaneously, further worsens disease burden and complicates healthcare management (Adan et al., Reference Adan, Gillies, Tyrer and Khunti2020; Van Oostrom et al., Reference Van Oostrom, Picavet, De Bruin, Stirbu, Korevaar, Schellevis and Baan2014).
Implementing effective strategies for managing chronic diseases, especially in case of multimorbidity, presents considerable challenges (Wallace et al., Reference Wallace, Salisbury, Guthrie, Lewis, Fahey and Smith2015; McPhail, Reference McPhail2016). This is particularly relevant in primary care, where the majority of chronic disease care takes place (Rijken et al., Reference Rijken, de Bruin, Snoeijs, van Bijnen, Jansen and Schellevis2014; Van der Horst et al., Reference Van der Horst and de Wit2019). Given the absence of a cure for chronic conditions, the primary focus should be on improving the overall quality of life (QoL) through symptom management and lifestyle modifications (Lawn et al., Reference Lawn and Schoo2010). This requires proactive management strategies aligned with the principles of the Chronic Care Model (CCM), emphasising person-centred approaches to optimise health outcomes and minimise disease burden (Wagner, Reference Wagner1998; Aramrat et al., Reference Aramrat, Choksomngam, Jiaporncharoen, Wiwatkunupakarn, Pinyopornpanish, Mallinson, Kinra and Angkurawaranon2022). Central to this are self-management and shared decision-making, for which patients should receive tailored support, comprehensive knowledge and appropriate tools that align with their unique needs and circumstances (Grady et al., Reference Grady and Gough2014; Friesen-Storms et al., Reference Friesen-Storms, Bours, van der Weijden and Beurskens2015).
The Assessment of Burden of Chronic Conditions (ABCC) tool has been developed to comprehensively assess and visualise the burden experienced by patients with one or more chronic conditions, including chronic obstructive pulmonary disease (COPD), asthma, type 2 diabetes mellitus (T2DM) and chronic heart failure (CHF) (Boudewijns et al., Reference Boudewijns, Claessens, Van Schayck, Keijsers, Salomé, In’t Veen, Bilo and Gidding-Slok2020a). Unlike conventional patient-reported outcome measures (PROMs), the ABCC tool encompasses both general and disease-specific health, providing a nuanced view of patient well-being (Dawson et al., Reference Dawson, Doll, Fitzpatrick, Jenkinson and Carr2010). This helps healthcare providers to gain insight into the patient’s perspective on their overall health status, thereby facilitating providing personalised care (Claessens et al., Reference Claessens, Vervloet, Boudewijns, Keijsers, Gidding-Slok, Van Schayck and van Dijk2023b). Outcomes are visualised through a balloon chart, with each balloon representing a specific domain of disease burden. Variations in colour and height of the balloons correspond to the patient’s score on that domain (Figure 1). This tool not only provides a holistic overview of the perceived burden, but by directing the conversation between patients and healthcare providers towards the main areas of concern, it also serves as a supportive guide during consultations (Boudewijns et al., Reference Boudewijns, Claessens, Van Schayck, Keijsers, Salomé, In’t Veen, Bilo and Gidding-Slok2020a).
Visualisation of the ABCC tool for COPD.
The perceived burden by patients is visualised in a balloon chart. A red balloon indicates a high experienced burden, an orange balloon signifies a moderate burden and a green balloon represents a low burden. Grey balloons visualise domain scores from previous visits, enabling monitoring and visualisation of changes over time.

Prior research has established the validity and reliability of the ABCC tool (Claessens et al., Reference Claessens, Boudewijns, Keijsers, Gidding-Slok, Winkens and van Schayck2023a). Additionally, studies have been conducted on healthcare providers’ experiences (Claessens et al., Reference Claessens, Vervloet, Boudewijns, Keijsers, Gidding-Slok, Van Schayck and van Dijk2023b, Claessens et al., Reference Claessens, Vervloet, Boudewijns, Keijsers, Gidding-Slok, Van Schayck, Winkens and Van Dijk2024, Claessens et al., Reference Claessens, Boudewijns, Vervloet, Keijsers, Gidding-Slok, Van Schayck and Van Dijk2025), as well as on effectiveness and cost-effectiveness (Boudewijns et al., Reference Boudewijns, Claessens, Joore, Keijsers, Van Schayck, Winkens and Gidding-Slok2020b, Boudewijns et al., Reference Boudewijns, Claessens, van Schayck, Twellaar, Winkens, Joore, Keijsers, Krol, Urlings and Gidding-Slok2024). However, understanding patients’ perceptions on the use of the ABCC tool is essential for a comprehensive evaluation of its efficacy in promoting person-centred care, self-management and shared decision-making. Therefore, this study aims to assess the perspectives of patients with chronic conditions on the use of the ABCC tool during consultations with their healthcare providers (i.e. general practitioners (GPs) or practice nurses) in primary care.
Methods
Study design
This study had a qualitative phenomenological research design from an interpretivist point of view (Starks et al., Reference Starks and Trinidad2007). The consolidated criteria for reporting qualitative research (COREQ) guidelines were used to report this study (Tong et al., Reference Tong, Sainsbury and Craig2007).
Study population and recruitment
The current study builds upon data collected in a previously performed quasi-experimental study, which was aimed at evaluating the effectiveness of the ABCC tool (Boudewijns et al., Reference Boudewijns, Claessens, van Schayck, Twellaar, Winkens, Joore, Keijsers, Krol, Urlings and Gidding-Slok2024). Details regarding the recruitment and assignment of healthcare providers from various Dutch general practices to either the intervention or control group, as well as their subsequent recruitment of patients with chronic conditions (i.e., COPD, asthma, T2DM and CHF), and specific inclusion and exclusion criteria, are provided elsewhere (Boudewijns et al., Reference Boudewijns, Claessens, Joore, Keijsers, Van Schayck, Winkens and Gidding-Slok2020b).
All patients from the intervention group were eligible to participate in this qualitative study. Therefore 150 individuals were invited to participate in this study via an addendum to the final questionnaire of the previously conducted quasi-experimental study. Those willing to participate could respond via e-mail or phone. In case of no response, a follow-up reminder was sent by e-mail after one week, followed by a reminder by phone.
Respondents were provided with detailed information about the study and received an informed consent form via e-mail or post, according to their preference. Upon receipt of a signed informed consent form, participants were scheduled for an interview. Based on previous research, it was expected that 10 to 15 interviews would be sufficient to reach data saturation (Slok et al., Reference Slok, Twellaar, Jutbo, Kotz, Chavannes, Holverda, Salomé, Dekhuijzen, Rutten-van Mölken, Schuiten, In’t Veen and van Schayck2016; Vasileiou et al., Reference Vasileiou, Barnett, Thorpe and Young2018; Hennink et al., Reference Hennink and Kaiser2022).
The ABCC tool
All participants used the ABCC tool, which involved a series of procedural steps. Before the consultation, the patient completed a questionnaire to assess their experienced burden, after which the results were displayed in a balloon chart (Figure 1). During the consultation this balloon chart was discussed by the healthcare provider and patient. One or multiple domains could be selected to elaborate on. Clicking on a balloon revealed a general treatment advice (based on GP or specialist guidelines), after which a specific personalised goal and plan could be formulated. Prior to the next consultation, the patient completed the same questionnaire again. The balloon graph then included grey balloons, representing those from the previous consultation, as well as coloured balloons, indicating the current status. Progression or deterioration could then be discussed, leading to a new or adjusted care plan (Boudewijns et al., Reference Boudewijns, Claessens, Joore, Keijsers, Van Schayck, Winkens and Gidding-Slok2020b; Claessens et al., Reference Claessens, Vervloet, Boudewijns, Keijsers, Gidding-Slok, Van Schayck and van Dijk2023b).
Data collection
To prevent the data collection of this study from influencing the results of the previously conducted quasi-experimental study, it was postponed until the completion of the previous study, which ran from November 2019 until November 2022. As a result, there was a significant time gap between participants’ use of the ABCC tool and the interviews in some cases.
Data collection of the current study took place between March 2022 and January 2023, by conducting semi-structured interviews, primarily consisting of open-ended questions guided by a predefined topic list (Appendix 1). This list was collaboratively developed through consensus among the members of the research team. All interviews were performed by one researcher (LK), either in person or via video calls, and audio recorded for further analysis. LK had experience in conducting patient interviews for research purposes. Additionally, she underwent training in qualitative research methodologies to enhance her proficiency in this area. To ensure the interviewer’s independence from the interviewees, it is important to note that LK had no prior relationship with any of the participants.
Data analysis
The interviews were transcribed verbatim, followed by analysis using ATLAS.ti 24 software. The methods used included a combination of conventional content analysis and directed content analysis, incorporating both inductive and deductive coding approaches. First, the data were thoroughly reviewed to identify key themes and patterns. Initial codes were created via inductive coding. This was complemented by deductive coding, guided by pre-established themes from the interview guide. Similar codes were then grouped into broader categories, and higher-level themes were synthesised to provide a comprehensive understanding of the participants’ experiences and perspectives (Hsieh et al., Reference Hsieh and Shannon2005). The transcription was performed by one researcher (LK), while the coding of the transcripts was carried out by two different researchers. Initially, the first author (LP) and last author (AGS) independently coded three transcripts, followed by comparing codes and discussing inconsistencies. Subsequently, both authors coded four additional transcripts, again followed by discussing the codes. After reaching consensus, the first author (LP) continued with the remaining steps of data analysis.
Results
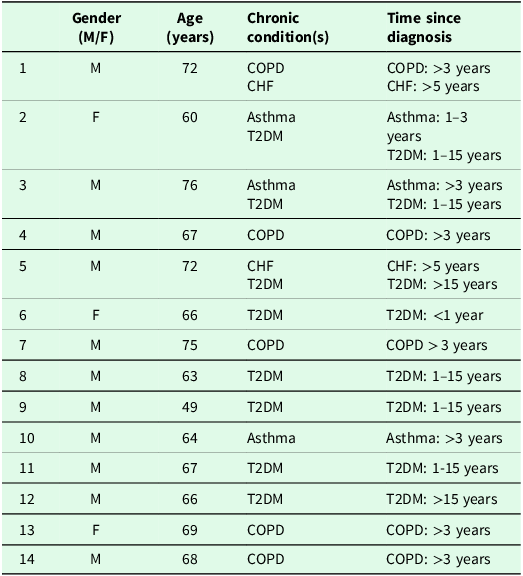
A total of 14 interviews were conducted with individual patients, including one interview in which the patient’s partner was present as well. On average, there was a time gap of 1.41 years (±0.31) between the participants’ last use of the ABCC tool and the interviews. The duration of the interviews ranged from 16 to 45 minutes. Characteristics of the participants are displayed in Table 1. It is noteworthy that certain conditions were underrepresented in our sample. For instance, patients with CHF were fewer compared to those with T2DM, who constituted most of the participants. Moreover, the sample exhibited a gender imbalance, with a higher proportion of male participants compared to female participants. As anticipated, data saturation was observed after 10 interviews.
Characteristics of the participants

Analysis revealed several recurring themes that were consistently observed throughout the interviews.
Overall
Regarding the frequency of the use of the ABCC tool, patients report varying use, ranging from one to several times.
“I believe I have filled it in a total of three or four times. With large intervals in between.” – Respondent 4
“I’ve already had to fill it out twice. I think (…) Uh, I think the last time was the second time or third time” – Respondent 6
When asked about their most recent use, the majority of the patients reported that it had been quite some time ago, leading to uncertainty or confusion regarding the exact timing.
“Yes, yes, hmm, more than six months ago for sure. A year ago maybe? Hmm, no, that’s a long time. I don’t remember.” – Respondent 6
Questionnaire
The moment of completion of the questionnaire varied among participants, with most completing it before the consultation from home, while one individual did so during the appointment with the healthcare provider.
“So, I did that, I did that at home, yes, yes.” – Respondent 1
“Yes, we just filled it in together at that moment indeed. (…) No, no. I filled it in together with the healthcare provider ” – Respondent 2
Overall, participants expressed satisfaction and appreciation for the questionnaire used in the ABCC tool. Most patients indicated that they found the questionnaire comprehensive and thorough, with all questions considered relevant.
“Uh… no, actually, I find all the questions important! The ones you ask (…) Quite comprehensive” – Respondent 6
The holistic approach of the questionnaire, which covered different aspects of daily life rather than focusing solely on disease-specific aspects, was highly appreciated by the majority of patients.
“You ask more questions, you know, and different questions too. (…) There are more questions about daily life. (…) I actually like that, yes. (…) And some questions about whether I was worried. I found that good too” – Respondent 6
“But more for the general aspect, I find that important. That’s often what it’s about for me.” – Respondent 13
Feedback from participants emphasised the user-friendly nature of the questionnaire, focusing on its ease of completion and accessibility.
“I actually found it easy to answer and understand. And to read.” – Respondent 6
Moreover, participants appreciated the balanced length of the questionnaire.
“Yeah, maybe also that it wasn’t too long to fill out. Not too many questions. And I think that’s nice.” – Respondent 12
Patients also expressed appreciation for the wide range of answer options in the questionnaire, recognising that it allowed them to give more detailed and nuanced answers compared to other surveys that offered fewer choices.
“I actually liked that there were so many answer options. Sometimes you only see two or three options, and I don’t think that works. You need to have choices, you know. I remember that I thought that was good.” – Respondent 9
Visual representation
Participants largely appreciated the visual representation of the data using balloons, finding it clear, insightful and easy to understand. They valued its ability to convey complex information simply, making it accessible even to those less proficient in reading.
“Yes, it was clear to see. Those balloon images are just very clear.” – Respondent 6
A few participants described the difficulty of matching the domains to the corresponding balloons. To address this challenge, it was suggested to use strings to visually connect them for clarity.
“Yeah, I had to figure out which name matched which balloon, you know. That was a bit… uh… yeah, a bit like guessing. So, I counted the balloons and also counted the names, so I knew, okay, this name goes with that balloon. That took a moment (…) Maybe you should tie a string to each so I can see which balloon goes with which name.” – Respondent 6
Communication
Most patients reported that the balloon graph was discussed during the consultation with the healthcare provider. Here the emphasis was often mainly on the red balloons.
“Everything that’s green (…) we don’t need to talk about that. It’s the things that are less… the red and the orange…” – Respondent 13
Participants in the study highlighted the ABCC tool as a valuable guide during the conversations with their healthcare providers. They appreciated its structured approach, which ensured that important topics were systematically addressed.
“Well, you don’t forget anything, all the points come up—smoking, alcohol, exercise, whatever you want, it’s all here, so you have a very structured conversation.” – Respondent 11
The tool not only facilitates structured conversations, but also helps patients to effectively express their problems to healthcare providers. Moreover, it benefits healthcare providers by enabling them to address reported issues.
“Yes, not just the patients, but especially the healthcare provider. They can respond to the problems that people indicate and thus find a solution. For those who experience difficulties, sometimes they have questions during the week, but at the moment of the consultation, they might forget. Then it’s filled in on the ABCC tool.” – Respondent 9
Participants also highlighted a shift towards more personal and in-depth conversations. They appreciated the opportunity to discuss topics such as concerns about the future, sexuality and intimacy, which previously had not been addressed during healthcare appointments. This shift allowed for a more comprehensive exploration of their health concerns and personal well-being.
“What struck me is that, for the first time, we talked about concerns about the future. And sexuality and intimacy. The healthcare provider herself also brought it up, like “yes, we’ve never really talked about that, have we’.” – Respondent 8
Personalising
All patients indicated that they had not clicked on the balloons. They were unaware that this option was available.
“No. Uh… clicked, you say? …Oh! That’s new to me. We haven’t done that.” – Respondent 14
The majority stated that they had not set any specific goals using the ABCC tool. Some mentioned not feeling the need to set goals due to experiencing minimal disease burden or already having clarity on what needed improvement.
“Again, for me, the problem was clear. And the treatment plan was clear, I just needed to lose a few kilos. The lifestyle had to be adjusted, so the treatment plan and the goal were clear… No, no, I’ve known that for a long time. I don’t need a tool for that.” – Respondent 9
Monitoring
Most patients indicated that they found the distinction between current (coloured) and previous (grey) balloons helpful for monitoring changes over time. Some participants initially needed explanations about the meaning of the grey balloons, but they subsequently appreciated the ability to visually compare their progress. Additionally, several patients noted that this system worked as a motivator, encouraging them to convert red balloons to green and maintain green ones.
“I find it to be a positive encouragement, really. Also, to see what you had last time and what you have now, whether there’s something that improves each time. It’s good to know the declines too. But if they stay the same, then it’s good as well. As long as it doesn’t get worse. So, that’s also a motivation to fill it out.” – Respondent 6
Memory
It is worth noting that initially the majority of the participants either vaguely remembered or did not recall the ABCC tool at all. However, when shown the balloon graph, participants who initially could not recall the tool, began to recognize it, although some could not recall specific components or features. For those who still could not recall all aspects of the instrument in detail, the conversation shifted partly to hypothetical discussions, exploring their perceptions and interpretations of the use of the ABCC tool rather than their actual experiences.
Discussion
This study aimed to assess patients’ experiences and perceptions of using the ABCC tool during consultations with their healthcare providers in primary care settings. Through in-depth interviews, participants provided valuable insights into their experiences and perceptions of using the ABCC tool in clinical settings, highlighting both strengths and areas for improvement.
Participants expressed overall satisfaction with the use of the ABCC tool. The questionnaire was considered comprehensive and relevant, as it covered various aspects of daily life rather than focusing solely on disease-specific issues. This holistic approach promotes a shift towards person-centred care, which is essential for improving the quality of care for people with chronic conditions, as recommended by the CCM and demonstrated by a previous effectiveness study (Wagner et al., Reference Wagner, Austin, Davis, Hindmarsh, Schaefer and Bonomi2001; Boudewijns et al., Reference Boudewijns, Claessens, van Schayck, Twellaar, Winkens, Joore, Keijsers, Krol, Urlings and Gidding-Slok2024). By doing so, the ABCC tool effectively addresses a recognised gap that emerged in previous research, where traditional healthcare models often overlooked broader, non-disease-specific factors that are critical to patient well-being (Wagner et al., Reference Wagner, Austin, Davis, Hindmarsh, Schaefer and Bonomi2001).
Moreover, the questionnaire was praised for its user-friendly design, making it easy to complete and accessible to all participants, regardless of their background. Its balanced length and wide range of answer options allowed for detailed and nuanced responses, which were highly appreciated as well. These are important aspects PROMs should adhere to in order to minimise respondent burden and thus maximise usability (van de Glind et al., Reference Van de Glind, Bakker-Jacobs, Triemstra, de Boer and van der Wees2018).
The clear visual representation of data using the balloon graph proved to be an accessible way to convey information, useful for all people regardless of their literacy level or language comprehension. This visual aid was found to be valuable during consultations with healthcare providers, as it effectively guided conversations towards the main areas of concern, thus facilitating more personal and in-depth discussions. However, some participants reported that it was difficult to figure out which domains belonged to which balloons. To enhance clarity, it was suggested to add strings to the balloons, clearly linking each domain to its corresponding balloon. This can help patients and healthcare providers interpret the data more easily, further simplifying the tool’s utility in clinical practice.
Moreover, initial confusion regarding the meaning of grey balloons was noted among some of the participants. This observation highlights the importance of clear communication and explanation by healthcare providers when introducing the tool and its balloon graph to patients to maximise its usefulness in practice. Despite requiring clarification of the meaning, these grey balloons were appreciated for their role in providing clear insights into changes over time. Several patients also stressed that this system worked as a motivator, which is consistent with the principles of motivational interviewing (Rollnick et al., Reference Rollnick, Miller, Butler and Aloia2008).
Despite the recognised benefits of the ABCC tool, patients were unaware of certain features, such as the ability to click on balloons for treatment advice and goal setting. This lack of awareness points to potential gaps in the use of the tool and highlights opportunities for improved healthcare provider training and patient instruction to optimise its effectiveness in practice.
Although the tool’s ability to facilitate goal setting and personalisation was appreciated, most patients expressed no need for specific goals. This was often attributed to the fact that they reported experiencing little burden, describing their situation as stable, or stated that they had adapted to it. Others indicated that the areas that needed attention were already well-known and long-standing issues. This suggests that they may have accepted these challenges as a part of life, rather than actively seeking to address them. If provided with targeted support through individualised care plans, outcomes could potentially improve.
Overall, the positive results regarding the completeness and relevance of the questionnaire, the clarity and accessibility of the visual display, the supportive role of the tool in conversations between patients and healthcare providers and the value of the monitoring function indicate that the ABCC tool is well received by patients and that its use in clinical settings should be supported.
The results of the current study are consistent with a previously published article that evaluated the experiences of patients and healthcare providers with the use of a precursor of the ABCC tool, known as the Assessment of Burden of COPD (ABC) tool (Slok et al., Reference Slok, Twellaar, Jutbo, Kotz, Chavannes, Holverda, Salomé, Dekhuijzen, Rutten-van Mölken, Schuiten, In’t Veen and van Schayck2016). Similar levels of patient satisfaction were observed in both studies. This consistency indicates that, even though improvements can be made to enhance usability, the integration of tools such as ABCC continues to gain positive traction in chronic condition management.
Strengths and limitations
This study possesses several strengths. First, the qualitative approach allowed for in-depth research and a nuanced understanding of patients’ perspectives and experiences (Carr, Reference Carr1994; Renjith et al., Reference Renjith, Yesodharan, Noronha, Ladd and George2021). This in-depth knowledge is crucial to advance the application of the tool in enhancing care delivery and improving patient outcomes. Second, the combination of inductive and deductive research contributed significantly to the credibility and robustness of the results (Fereday et al., Reference Fereday and Muir-Cochrane2006). The inductive coding approach helped reduce confirmation bias by allowing themes and patterns to emerge directly from the data rather than being predetermined. Hence, this method ensured that the analysis remained grounded in participants’ actual experiences and perspectives, thereby increasing the reliability of the findings (Nickerson, Reference Nickerson1998; Hsieh et al., Reference Hsieh and Shannon2005). By validating emergent themes against pre-established ones, the deductive approach minimised the risk of researcher bias (Hsieh et al., Reference Hsieh and Shannon2005; Fereday et al., Reference Fereday and Muir-Cochrane2006).
However, this study also faced some limitations. The long interval between the last use of the tool and the conduct of interviews may have resulted in recall bias (Khare et al., Reference Khare and Vedel2019; Boudewijns et al., Reference Boudewijns, Claessens, Joore, Keijsers, Van Schayck, Winkens and Gidding-Slok2020b; Dehghani Tafti et al., Reference Dehghani Tafti, Fatehpanah, Salmani, Bahrami, Tavangar, Fallahzadeh, Tehrani, Bahariniya and Tehrani2023). Therefore, participants’ responses may have reflected hypothetical scenarios rather than concrete memories. One issue that played part in this was the COVID-19 pandemic, when healthcare facilities faced disruptions that affected continuity of care, ultimately influencing patient engagement with tools such as ABCC (Dehghani Tafti et al., Reference Dehghani Tafti, Fatehpanah, Salmani, Bahrami, Tavangar, Fallahzadeh, Tehrani, Bahariniya and Tehrani2023). Moreover, given that this study builds upon a previously conducted quasi-experimental study, data collection of the current study had to wait until the completion of the previous study to avoid influencing its results (Boudewijns et al., Reference Boudewijns, Claessens, Joore, Keijsers, Van Schayck, Winkens and Gidding-Slok2020b). However, it is noteworthy that despite the above-mentioned limitation, participants were very positive about the tool, which implicates the potential of the instrument. Second, the study may have been prone to selection bias, stemming from the previous quasi-experimental study, in which blinding was not possible due to the nature of the intervention. Participants were selected and recruited directly by healthcare providers (Flannelly et al., Reference Flannelly, Flannelly and Jankowski2018; Boudewijns et al., Reference Boudewijns, Claessens, Joore, Keijsers, Van Schayck, Winkens and Gidding-Slok2020b). This may have resulted in a sample that mainly included patients with relatively stable conditions, as healthcare providers might have been reluctant to introduce a new tool to those with unstable health situations.
Recommendations for future research and practice
Future studies should focus on expanding the scope of the research beyond general practice by exploring the utility of the ABCC tool in different healthcare contexts, including paramedic fields. Therefore, an explorative study is being conducted into the views of physiotherapists in primary care on the (potential) use of the ABCC tool in practice. Furthermore, more research should be conducted on optimising the use of the tool in goal setting and creating personalised care plans.
Conclusion
In conclusion, this study provides valuable insights into patients’ experiences with the ABCC tool during consultations with their healthcare providers. Despite some challenges such as recall bias and limited awareness of certain features, participants generally expressed satisfaction with using the tool. Based on these findings, the tool can be further improved and its use should be further supported. However, the ABCC tool shows promise as a valuable instrument for improving consultations in clinical practice.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1463423626101091
Data availability statement
Data are available from the corresponding author on reasonable request.
Acknowledgements
We would like to thank all patients who participated in the interventions for their time and commitment. Additionally, we want to thank Valerie Debie, Silvia Bours and Mascha Twellaar for their assistance in transcribing the interviews.
Author contributions
LP: formal analysis, writing – original draft; LK: investigation, writing – review & editing; OvS: conceptualization, writing – review & editing, supervision, funding acquisition; JM: writing – review & editing; MV: conceptualization, writing – review & editing, funding acquisition; AGS: conceptualization, formal analysis, writing – review & editing, supervision, funding acquisition.
Funding statement
This study was funded by the Netherlands Organization for Health Research and Development (104006001).
Competing interests
None.
Ethical standards
This study was approved by the Medical Ethics Committee (METC) of Zuyderland Medical Centre, Heerlen, the Netherlands (METCZ20180131) on November 21, 2018. All participants provided written informed consent prior to participation.




 Open access
Open access