


Key learning aims
-
(1) To consider what characterises and defines a complex case.
-
(2) To consider the role of client, therapist, healthcare and contextual factors in complex cases.
-
(3) To consider how services and therapists can respond to clinical complexity.
Introduction
This article introduces a model to formulate complex cases in CBT and a case example is used to illustrate its practical applications. Although the topic of clinical complexity is well-established in CBT, there is no consensus, definition or empirically tested model of it (Murray and El-Leithy, Reference Murray and El-Leithy2022; Tarrier et al., Reference Tarrier, Wells and Haddock2000). This article is intended to be a step towards that. It proposes a definition of clinical complexity with respect to therapeutic processes, with hypotheses about how these can be formulated and used to guide clinical practice. Subsequent empirical tests are needed to find out if the hypotheses are correct and evaluate the effectiveness of the guidance.
To date, the absence of a complexity model has resulted in a lot of subjectivity in the judgements of therapists and service providers. Because complexity is currently undefined, the field has low specificity and low sensitivity: it is ascribed in situations where it is not present, and overlooked in situations where it is present (Barton et al., Reference Barton, Armstrong, Wicks, Freeman and Meyer2017). A straightforward case for one therapist is viewed as a complex case by another. The goal of this article is to increase consensus about how to define complexity and formulate it, describing how client, therapist, healthcare and contextual factors all contribute.
There is every reason to be optimistic about working in complex cases. CBT can be highly effective working with complexity, depending on how it is formulated and approached (see the Cognitive Behavioural Therapist, 2017; vol. 10). There is no need for therapists to be avoidant or pessimistic, not least because this is likely to increase complexity rather than reduce it. However, to date, the therapeutic strategies needed to work in complex cases have been shared mainly through folklore: experienced therapists provide tips in supervision and training. Received wisdom is inevitably a blend of true and false claims – hopefully more of the former – but until it is codified and tested, it remains folklore waiting for scientific investigation. This article is a proposed codification and it explores the factors that contribute to clinical complexity and how a client, therapist and service can mitigate them and overcome them. A case example is used to illustrate the key points.
Case illustration
The client in this case example, David, is described in detail in a published case study (Barton et al., Reference Barton, Armstrong, Meares, Bromley and Whitton2024). He is a co-author of this article and has consented for his case to be described. At the time of his treatment, David was a 67-year-old man with a 14-year history of recurrent depression, generalised anxiety, panic and post-traumatic stress disorder (PTSD) symptoms. Three of his four adult children had serious mental health problems. The background context was a highly conflictual relationship with his father who had died three years previously. In the three years since his father died, David had suffered fluctuating symptoms with periods of relative stability interspersed with depression, suicidal thoughts, increased anxiety, nightmares and a sense of personal inadequacy. His mood was highly reactive depending on his family situation and/or intrusive memories about his father. David had received a broad range of biomedical and psychological therapies over the preceding 14 years, some of which had provided temporary benefit, but none had produced lasting change. Two previous courses of CBT had emphasised coping with depression rather than recovering from it, and had a short-lasting effect.
One way to describe and reflect on a client’s problems is to develop a biopsychosocial problem map – see Fig. 1. Mapping is a recognised way of making sense of complex dynamic systems in social and healthcare settings (e.g. Gillani et al., Reference Gillani, Prince, Ray-Novak, Feerasta, Jones, Mintz and Moore2024; Khan and Ali, Reference Khan and Ali2024; Stansfield et al., Reference Stansfield, Cavill, Marshall, Robson and Rutter2021). The problem map is a matrix with biomedical, psychological and social rows partitioned into past and current columns. Once the client’s main difficulties have been mapped, hypotheses can be generated about how their problems interact. Dotted lines are used to represent tentative links, continuous lines depict stronger hypotheses, and arrow heads are used to represent causal links. The visuo-spatial format encourages therapists to notice interactions between problems, something that can go undetected when knowledge about a client is limited to declarative information. On a practical level, it can take several sessions to develop an accurate problem map: how the client’s problems interact takes time to hypothesise, test and understand. Across a course of treatment, the map usually develops from tentative to stronger hypotheses when new information comes to light.
Client biopsychosocial problem map.

CBT therapists will already be familiar with the value of graphic formulations, but unlike disorder-specific formulations, which explain how a particular problem is maintained, the problem map has a macro reflective function, to overview the main problems affecting a client and notice inter-relationships between them. It is not a micro formulation of a particular disorder; rather, it broadens attention across multiple difficulties, the majority of which will not be targeted in a course of therapy. It is primarily a reflective tool for therapists and it augments the disorder-specific formulation rather than replacing it. It can help to find order in an otherwise confusing clinical picture.
Reflecting on David’s problems, what criteria might be applied to determine whether his case is complex? Because the field only has implicit criteria, therapists are likely to bring attention to different factors. For some, psychological co-morbidity and risk will be salient. For others, the presence of family and social factors will be key. For others, the history of relational trauma or unsuccessful prior treatment will be the main issue. It is plausible that any of these factors could present challenges in David’s treatment; however, it is unclear whether clinical complexity should be defined with respect to client characteristics or complications that occur within treatment (possible or actual). In either scenario, liberal or conservative criteria can be applied. For example, if co-morbidity is deemed sufficient for complexity, most cases would be complex. In our view, this is over-inclusive to the point of undermining complexity as a construct. In contrast, if complexity is grounded in treatment complications, a smaller proportion of cases would reach threshold for complexity.
The current model proposes the latter approach, that complexity is defined with respect to treatment complications. When clients are identified as complex prior to treatment, this is based on implicit appraisals of the challenges that are expected to occur in treatment, and these may or may not be accurate predictions. There are three elements in this type of appraisal: (1) the client complexity factor; (2) the predicted treatment challenge; (3) the actual treatment process. The current model encourages therapists to make these appraisals explicit and, most importantly, to differentiate client characteristics from expected and actual therapeutic events.
When these are not considered separately, there is a significant risk that client factors are assumed to result in treatment difficulties, rather than attempting to mitigate them and find out what happens in practice. There is also a risk that attention narrows around complexity and this distracts from facilitative factors, therapist and service variables. In the worst-case scenario, clients are rejected from services and told they are “too complex” without an explanation of: (a) which complexity factors are present, (b) what treatment complications are expected, and (c) why these cannot be overcome. Clients are not the sole determinants of what occurs during treatment: in any course of therapy, client, therapist, healthcare and contextual factors interact to facilitate or complicate the therapeutic process, and the influence of each participant needs to be taken into consideration.
Complexity and facilitative factors across the whole case
Client factors
Rather than identifying clients as complex, its more helpful to specify their complexity factors and describe the challenges that these could provoke within treatment. This needs to be balanced with reflection on facilitative factors and how these can be harnessed and supported. In spite of having long-term difficulties, David was very determined to overcome his problems and he was assertive in his approach to therapy. He was keen to form a trusting relationship with a therapist and appeared to have good alliance potential. Nevertheless, at the outset of therapy his problems appeared to be complicated and challenging to treat.
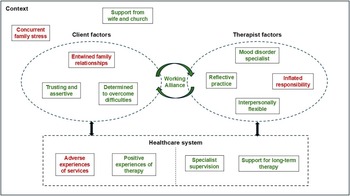
When considering whether a client has complicated problems, there is a risk of conflating this with related constructs such as severe, persistent, etc. The etymology of ‘complicated’ suggests a particular definition: multiple factors that are entwined or inter-woven. Problems that interact in a known, predictable way are unlikely to be complicated, whereas entwined problems are likely to be unpredictable, ambiguous or unstable. A number of David’s problems interacted with each other; for example, co-morbid depression and anxiety, but they did not interact in an entwined or unstable way – see Fig. 1. When he felt depressed he also felt more anxious and these states were mutually maintaining (Sharp and Harvey, Reference Sharp and Harvey2001). In contrast, David was perplexed by the difficulties he had experienced, over several decades, in his family relationships. Different members of the family held conflicting narratives about David’s father and the way he related to others. David’s beliefs about his father, and himself, were often confused, and several years of reflection had not produced a settled understanding of what had occurred in their relationship. Entwined family relationships had a deep and distressing effect on David over an extended period. David’s main complexity and facilitative factors are summarised in the case map depicted in Fig. 2.
Complexity and facilitative factors (complexity in red, facilitative in green).

Therapist factors
The therapist in David’s case was the first author. He had worked for 17 years in a specialist CBT service in the North East of England, with a particular interest in mood disorders. His continuing professional development included self-practice/self-reflection (Chaddock et al., Reference Chaddock, Thwaites, Bennett-Levy and Freeston2014) and training workshops on interpersonal processes. Prior to treatment, he appeared to be a good match to David’s needs in terms of CBT knowledge, skills, reflective capacity and interpersonal range. His weaknesses were a tendency to be overly theoretical and take too much responsibility for change. He and his supervisor were aware of these tendencies and they did not manifest with all clients. Nevertheless, they had the potential to influence David’s treatment in an unhelpful way – see Fig. 2.
Healthcare factors
Healthcare factors need to be considered from both client and therapist perspectives. From the therapist’s point of view, the healthcare system was in a state of flux during the COVID-19 pandemic, but arrangements were in place for David’s treatment to be provided remotely. With respect to meeting David’s needs, there were two key facilitative factors. Firstly, the therapist received specialist supervision from the second author who had 26 years of experience supervising complex cases. The therapist and supervisor had a strong supervisory alliance and shared an interest in mood disorders. Secondly, the tertiary service in which they were based was able to offer long-term treatment when clients needed it. Given that David’s previous CBT had been brief and its effects not lasting, the option of longer-term treatment was facilitative and supportive.
From the client’s point of view, David had strong alliances with some NHS staff which could have a facilitative effect in this treatment (Cooper et al., Reference Cooper, Gillmore and Hogg2016). However, he also had a number of adverse experiences in mental health services. He had requested trauma-focused therapy over a number of years and was repeatedly told it would be de-stabilising and he would not be strong enough to tolerate it. Five years previously, a locum member of staff in a Community Treatment Team (CTT) discharged him from the Trust, possibly to meet service targets, at a time when David’s depression was severe and his risk of suicide was moderately high. The locum staff member had no knowledge of the therapy service that David was subsequently referred to. Being discharged during a vulnerable period had a very negative impact on David which, unfortunately, re-activated trauma memories and worsened his mental health for several months. It took two years of repeated requests for him to be re-referred into services. Memories of these experiences were salient for David and had the potential to trigger a lot of distress – see Fig. 2.
Contextual factors
Contextual factors also need to be considered from both client and therapist perspectives. From the therapist’s point of view, he was settled and supported in his professional and personal life, with no significant issues adversely affecting his work. From the client’s point of view, David had limited sources of social support but the sources he had were highly engaged, consistent and committed to his treatment, particularly his wife and members of his church. However, David’s broader family situation was very fluid and stressful, with three of his four adult children having significant mental health problems (Gantt-Howrey et al., Reference Gantt-Howrey, Brookover and Robins2025). David and his wife were providing a high level of support to them and responding to unpredictable events and crises on a regular basis. This had the potential to disrupt the flow and focus of treatment – see Fig. 2.
Clinical cases have a combination of complexity and facilitative factors and how they interact dynamically over time influences the therapeutic process. One way of formulating this is with respect to the therapeutic relationship. If a sufficiently strong working alliance can form, there is potential for the client to benefit from therapy even if they have complicated problems. Conversely, if client, therapist, healthcare and contextual factors create barriers within the working alliance, the therapeutic process will be prone to friction, obstruction or rupture, and this will significantly limit therapeutic gains (Doukani et al., Reference Doukani, Free, Araya, Michelson, Cerga-Pashoja and Kakuma2022). This situation describes and defines clinical complexity: in the current model, treatment is complicated to the degree that there are barriers within the working alliance. Client, therapist, healthcare and contextual factors contribute to different degrees in different cases, but it is the presence of alliance barriers that constitutes clinical complexity.
The working alliance and clinical complexity
In CBT, strong working alliances are necessary, but not always sufficient, for good clinical outcomes (Castonguay et al., Reference Castonguay, Constantino, McAleavey and Goldfried2010; Impala et al., Reference Impala, Dobson and Kazantzis2022; Cameron et al., Reference Cameron, Rodgers and Dagnan2018). Alliance building is an early-phase treatment task along with socialising the client to CBT, developing an initial formulation, agreeing treatment goals, prioritising a target problem, etc. When collaboration grows in the early sessions, this provides the foundation to deliver an evidence-based protocol. The alliance has to be maintained across treatment and it needs explicit attention in the event of a misunderstanding, disagreement or rupture. However, when clients are benefiting from treatment, the alliance tends to strengthen naturally without needing much explicit attention (Wester et al., Reference Wester, Koch, Münch, Driver, Lutz and Rubel2025). In straightforward cases, the working alliance forms naturally from the start of treatment and the therapeutic process is smooth and uncomplicated. In complex cases, there are barriers to forming and/or maintaining a working alliance and the therapeutic process is prone to friction (Ekeblad et al., Reference Ekeblad, Dahlman, Pio, Malmquist and Falkenström2022).
Straightforward cases can create the mis-impression that interpersonal factors precede the tasks of therapy and are not a constituent part of them (Lorenzo-Luaces and DeRubeis, Reference Lorenzo-Luaces and DeRubeis2018). In fact, it is more accurate to view the tasks of therapy as a constituent part of the working alliance, as reflected in Bordin’s (Reference Bordin1979) original model of the alliance having bond, goal and task-related elements. From this perspective, the whole therapeutic process is contained in the working alliance, including the evidence-based protocol. Different aspects of the therapeutic relationship can be distinguished, such as bond, goal and task, but they cannot be separated.
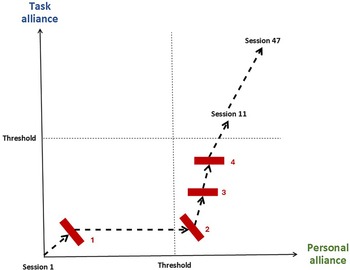
The complexity model distinguishes personal alliance, reflected in the interpersonal bond, and task alliance, reflected in goal-directed therapeutic tasks. These are not separate treatment phases, rather, they are different aspects of the same therapeutic relationship. They need to be balanced across a course of therapy and both dimensions need to be strong enough for the alliance to work effectively. Personal alliance (represented by the x-axis in Fig. 3) is the degree of mutual trust in the bond between the client and the therapist. This develops through the therapist offering support, empathy and compassion in a way that is responsive to the client’s needs, and this is reciprocated through the client disclosing personal information, allowing themselves to feel emotions and receive the therapist’s help and support. These are the setting conditions for a trusting bond to develop. How the personal alliance grows depends a lot on the interpersonal styles of the client and therapist, but these are the essential elements.
Alliance vectors and barriers (barriers depicted in red).

Task alliance (represented by the y-axis in Fig. 3) is the degree to which the dyad is aligned and engaged in a change process. This aspect depends on sufficient agreement about the goals and tasks of therapy, including the formulation and rationale for change. In a course of CBT, various therapist and client actions are needed for goals and tasks to be agreed and facilitate a change process. The therapist needs to be reflective, curious and communicate hope about the client overcoming their difficulties. The client also needs to be sufficiently reflective, goal-directed and open to new learning.
When working with clients with complicated problems, it is cost-effective to take the time needed to build a strong working alliance, even when session limits are in place (Falkenström et al., Reference Falkenström, Ekeblad and Holmqvist2016). If the personal alliance reaches threshold, but the task alliance does not, the interpersonal bond can facilitate a supportive therapy but new learning is unlikely to occur. Conversely, if the task alliance reaches threshold, but the personal alliance does not, new learning may occur but it is unlikely to have a lasting emotional impact. When neither the personal nor task alliance reach threshold, the client cannot benefit from treatment and it is essential to prioritise alliance building in this situation (Binnie, Reference Binnie2012; Hayes and Andrews, Reference Hayes and Andrews2020).
In David’s case there were four significant barriers in forming and maintaining a working alliance and it took 11 sessions for both personal and task alliance to reach threshold. Figure 3 represents the process that David and his therapist navigated during different treatment phases (Schiepek et al., Reference Schiepek, Gelo, Viol, Kratzer, Orsucci, de Felice and Schöller2020).
Barrier 1 – The client’s past experiences of services
Because David had been declined trauma-focused therapy in the past, and been discharged from services inappropriately, he was anxious to find out how the therapist would respond to his request to explore the causes of his depression, not just manage symptoms. David did not meet all the criteria for PTSD and he had not been placed on a trauma pathway. His main presenting problem was recurrent depression and the request to explore causes raised the therapist’s concern that this could lead to depressive rumination. However, in the initial sessions, it would have been a significant barrier to engagement if the therapist had taken attention away from the causes of David’s depression. Rather than commence with a standard course of cognitive therapy (Beck et al., Reference Beck, Rush, Shaw, Emery, DeRubeis and Hollon2024) or behavioural activation (Martell et al., Reference Martell, Dimidjian and Herman-Dunn2021), which David had received in the past, the therapist encouraged him to share information about his relationship with his father. He also encouraged him to talk about his experiences in mental health services, both positive and negative. This initial response to David’s request helped to build a lot of personal alliance which formed rapidly over the first three sessions. David felt supported, taken seriously and hopeful. A potential barrier to engagement was overcome, because empathy and compassion were prioritised in response to David’s concerns. However, personal alliance needed to be balanced with task alliance and there were three inter-related barriers to achieving this.
Barrier 2 – The client’s multiple interacting problems
As indicated in Fig. 1, David was not only living with distressing memories of his father. On a regular basis, he was managing depressed mood, elevated anxiety, a chronic pain condition and a turbulent family situation. The therapist was concerned that treatment could become diffuse or ‘pinball’ if too many of David’s problems were tackled simultaneously. This was discussed explicitly and David agreed that therapy needed a consistent focus. He had a clear preference to limit attention to his relationship with his father, and this became the agreed target problem. Limiting attention to an agreed target helped David prepare for trauma-focused work. His family problems affected him intermittently in the following months, but they did not interfere with the therapy or obstruct it. Having an agreed target strengthened the task alliance; however, after approximately six sessions there was no agreed plan how to treat the relational trauma.
Barrier 3 – The therapist’s inflated responsibility
The therapist was conscious that previous courses of therapy had supported David and given him tools to manage distress, but they had not helped him to heal from trauma or reduce his risk of depression. The therapist realised that a strong personal alliance was forming, but he felt uncertain about the optimal treatment plan and started to feel overly responsible for initiating a change process. This was partly because David’s case did not fit neatly into a depression or PTSD protocol. The therapist was conscious of avoiding further failed treatment, and he started to put pressure on himself to find a rationale for change. This strained the collaboration at key points; for example, the therapist assumed that David felt anger towards his father, rather than asking him. He proposed a piece of compassion-focused work to develop David’s self-soothing skills, but this was confusing and frustrating for David because he had already let the therapist know that a previous course of compassion focused therapy (Leaviss and Uttley, Reference Leaviss and Uttley2015) – while helpful at the time – had not addressed the relational trauma. Fortunately, David was open about this at the next session and it was discussed explicitly. In subsequent supervision, the therapist realised that he had fallen into the trap of taking too much responsibility and he had acted unilaterally in guiding the therapy. The personal alliance was strong enough to contain this and David tolerated the associated frustration. Rather than it rupturing the therapeutic relationship, it had a clarifying effect on next steps.
Barrier 4 – Uncertainty about a bespoke treatment plan
As described in Barton et al. (Reference Barton, Armstrong, Meares, Bromley and Whitton2024), a specific therapy plan was agreed after 11 sessions. Although David did not meet all the criteria for PTSD, the formulation of intrusive memories and disturbances in self-organisation had the potential to benefit from memory processing from trauma-focused CBT (Ehlers, Reference Ehlers2013; Ehlers and Clark, Reference Ehlers and Clark2000). Although David’s main presenting problem was recurrent depression, a treatment component from a PTSD protocol was a better fit to the emerging formulation, and explicit conversations in supervision were essential to clarify this and target the therapy appropriately. The 11 sessions spent building the working alliance gave David the opportunity he needed to prepare for trauma-focused therapy, and when he commenced memory processing he was ready and well-supported to do so. Across the remainder of treatment, the working alliance continued to strengthen across a total of 47 sessions. At each step, the interpersonal bond was strong enough to support and contain the tasks of therapy. David’s therapeutic gains helped to deepen mutual trust and shared engagement in the change process, ultimately leading to a very positive clinical outcome.
In each of the alliance barriers in David’s case, they were overcome through an iterative process of: (a) noticing the barriers, with attention brought to them; (b) reflecting on the barriers, seeking to formulate and understand them; and (c) discussing the barriers explicitly, in supervision and therapy. Problems in the therapeutic relationship can sometimes be addressed implicitly, for example, through non-verbal communication, but more significant barriers need explicit conversations in supervision and therapy (Safran et al., Reference Safran, Muran and Eubanks-Carter2011).
Overcoming alliance barriers
Clinical complexity is present whenever there are barriers within the working alliance and this can occur in any service, not just specialist services. When faced with treatment complications, clients and therapists need to navigate a path that balances personal and task alliance, sometimes bringing attention to mutual trust and sometimes to the change process. The aim is to increase collaboration with stronger mutual trust and greater alignment on change.
Personal alliance barriers usually have an interpersonal focus; for example, the therapist taking too much responsibility, the client being reminded of a previously unhelpful therapist, the client’s family telling him he should be able to manage without help, the service manager expressing caution that the client has made complaints in the past, etc. Any factor, or perceived factor, that increases wariness between client and therapist will limit disclosure, emotional expression and reduce openness and receptivity to the other person. A more business-like, superficial or tense relationship is likely to result.
Task alliance barriers usually have a technical focus in the sense that there is a discrepancy in the priorities, shared understanding or goals of the client and the therapist. The lack of alignment is not based on personal mistrust or wariness, rather the tasks of therapy have not yet been agreed, or the client and therapist are holding incompatible versions of them. As a general rule, the more entwined a client’s problems, the more challenging it is to establish a task alliance and higher intensity treatment is needed to achieve this. When problems are entwined, it usually takes time to understand and formulate them. It is analogous to a dense knot tied with multiple threads: therapy is understanding the knot, simplifying it and untying it. Without this understanding, pulling on random threads just tightens the knot. The threads are configured in such a way that a particular sequence of actions is needed, and this reflects the pathway to change when clients have complicated problems. When problems are simple, pulling on any thread unties the knot. When problems are complicated, a particular sequence of steps has to be discovered.
Treatment should always be simple at the point of delivery, but in complex cases it is not always obvious which simple step to take (Driscoll et al., Reference Driscoll, Cukrowicz, Reardon, Joiner and Joiner2014; Guthrie, Reference Guthrie2000; Newman, Reference Newman2020). The majority of evidence-based treatments in CBT are disorder-specific; that is, a primary diagnosis or target problem is identified and a protocol for that problem is provided. This is also the recommended strategy when clients have multiple problems, and a problem map is a helpful way of identifying the optimal target. However, when problems are entwined, non-targeted difficulties can interact with the target problem and obstruct the treatment process. In extreme cases, this can lead to ‘pinballing’ between multiple problems without a consistent focus.
The art of working with complicated problems is bringing the evidence base to the client; finding a path through multiple difficulties by treating at least one problem thoroughly (Barton and Armstrong, Reference Barton and Armstrong2019). In finding a path to change, it is sometimes necessary to change focus and pivot to a different target, but this needs to be done reflectively and collaboratively, rather than reactively and unilaterally. A related strategy is to target a transdiagnostic process that spans multiple problems (Cowles and Nightingale, Reference Cowles and Nightingale2015; McEvoy et al., Reference McEvoy, Nathan and Norton2009) or use a class of intervention that can be applied to multiple difficulties simultaneously (Hayes and Hofmann, Reference Hayes and Hofmann2018).
One of the challenges in providing a case illustration is it can only represent a small subset of the complications that might occur in clinical practice. David’s case is a good example of a client with complicated problems and alliance barriers that were overcome during therapy. In David’s case, this was sufficient to produce a good clinical outcome (see Barton et al., Reference Barton, Armstrong, Meares, Bromley and Whitton2024), but this is not true in all cases. When cases are more complex, for example, clients who repeatedly use therapy interfering behaviours, the same reflective process is encouraged: bring attention to the alliance barrier; reflect on the various factors that could be influencing it, including non-client factors; communicate about the barrier explicitly, in supervision and in therapy. The same process is used when a therapist or service has therapy interfering behaviours.
Further research and development is needed to apply the model to a broader range of cases. In particular, complexity factors associated with therapists, healthcare systems and socio-political contexts need further specification. The model also needs prospective tests of its main predictions:
-
Entwined client problems present a challenge for the task alliance and need higher intensity treatment.
-
Complexity factors across multiple participants interact to create alliance barriers, not just client factors.
-
When facilitative factors are harnessed, alliance barriers are more likely to be noticed, reflected on and discussed explicitly in supervision and therapy.
The benefits of incorporating this model into clinical practice also need to be tested empirically, e.g. testing the accuracy of predicted treatment complications; measuring therapy process and outcomes when therapists and supervisors are trained in this model.
Summary
-
(a) Clients can have complexity factors that have the potential to challenge the working alliance; for example, entwined problems, difficulties trusting other people, negative experiences of services, etc.
-
(b) Clients can also have facilitative factors that have the potential to support the working alliance; for example, resilience factors, determination to improve, positive experiences of past therapy, etc.
-
(c) Therapist, healthcare and contextual factors also have the potential to facilitate and challenge working alliances, and their influence needs to be considered within complex cases.
-
(d) Prior to embarking on a course of treatment, complexity and facilitative factors need to be considered across the whole case, to inform the optimal clinical pathway and treatment plan.
-
(e) The presence of complexity factors does not inevitably lead to barriers within the working alliance: rather, attempts should be made to mitigate and overcome potential complications.
-
(f) Mitigation includes discussing issues with clients that could become obstacles in treatment, so they have clear expectations of therapy and are ready and prepared when it commences. It also includes addressing therapist and service factors that have the potential to obstruct collaboration; for example, through supervision and clinical leadership.
-
(g) When therapy is underway, therapists need to invite clients to feedback about their experience of the therapeutic relationship as candidly as possible. Services and therapists need to measure the working alliance regularly and elicit session feedback across treatment.
-
(h) When alliance barriers are present, attention needs to be brought to them with time for reflection, formulation and explicit conversations in supervision and therapy. Mapping client problems (Fig. 1), complexity and facilitative factors (Fig. 2) and alliance vectors (Fig. 3) are helpful ways of reflecting on the whole case.
-
(i) When the personal alliance is barriered, there is insufficient mutual trust in the interpersonal bond and this is what needs to be discussed. When the task alliance is barriered, there is insufficient alignment on the goals and tasks of therapy and this is what needs to be discussed.
-
(j) Some alliance barriers can be influenced implicitly, for example through non-verbal communication, but the more significant the barrier, the greater the need for explicit communication.
-
(k) Explicit communication does not guarantee the resolution of clinical complications, but it is the best available strategy to overcome alliance barriers and increase the opportunity for the client to benefit from treatment.
Key practice points
-
(1) When clients have complicated problems, it is helpful for therapists to map out how their difficulties interact to identify an optimal target for change.
-
(2) Treatment is complicated to the degree that there are barriers in the working alliance and these significantly limit the benefits a client can gain from treatment.
-
(3) Overcoming alliance barriers relies on bringing attention to them, reflecting on them and communicating explicitly about them in supervision and therapy.
Data availability statement
All data relating to the clinical case are available from the first author.
Acknowledgements
The authors would like to express their gratitude to Mark Freeston and members of the Centre for Specialist Psychological Therapies in CNTW NHS Foundation Trust who supported the early development of this work. We would also like to thank Beth Bromley and two anonymous reviewers for helpful suggestions.
Author contribution
Stephen Barton: Conceptualization (lead), Validation (lead), Writing - original draft (lead), Writing - review & editing (lead); Peter Armstrong: Conceptualization (lead), Validation (supporting), Writing - review & editing (supporting); Stephen Holland: Conceptualization (supporting), Validation (supporting), Writing - review & editing (supporting); Leanne Langley: Conceptualization (supporting), Validation (supporting), Writing - review & editing (supporting); Layla Mofrad: Conceptualization (supporting), Validation (supporting), Writing - review & editing (supporting); Matt Stalker: Conceptualization (supporting), Validation (supporting), Writing - review & editing (supporting); Hayley Tyson-Adams: Conceptualization (supporting), Validation (supporting), Writing - review & editing (supporting); David Whitton: Conceptualization (supporting), Validation (supporting), Writing - review & editing (supporting).
Financial support
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing interests
The authors have no competing interests.
Ethical standard
The authors have abided by the ethical principles and code of conduct set out by the British Association of Behavioural and Cognitive Psychotherapies and British Psychological Society. The reported study is practice-based evidence and did not receive ethical approval in advance. In lieu of this, oversight was sought from CNTW Foundation Trust management which supported service-user involvement in collecting practice-based evidence. The service user was an active participant in the research process and is a co-author of the article.


 Open access
Open access
Comments
No Comments have been published for this article.