


Introduction
Pain and depression occur commonly in older adults with multimorbidity (OAMM; Scherer et al., Reference Scherer, Hansen, Gensichen, Mergenthal, Riedel-Heller, Weyerer, Maier, Fuchs, Bickel, Schön, Wiese, König, Van Den Bussche and Schäfer2016; Mcqueenie et al., Reference Mcqueenie, Jani, Siebert, Mcloone, Mccowan, Macdonald, Mair and Nicholl2021; Ronaldson et al., Reference Ronaldson, Arias De La Torre, Prina, Armstrong, Das-Munshi, Hatch, Stewart, Hotopf and Dregan2021). In primary care, screening for and managing these conditions among affected individuals typically consists of assessing patients’ symptoms at the time of scheduled visits, which occur several times a year for this expanding population. These episodic assessments often rely on retrospective, unstructured symptom inquiry or validated questionnaires (Mindlis et al., Reference Mindlis, Kiosses and Reid2025). Retrospective assessments (unstructured or structured) are subject to recall bias (Henry et al., Reference Henry, Moffitt, Caspi, Langley and Silva1994; Urban et al., Reference Urban, Charles, Levine and Almeida2018; Horwitz et al., Reference Horwitz, Zhao and Sen2023) and can produce poor quality data (Horwitz et al., Reference Horwitz, Zhao and Sen2023) as the most intense and proximal aspects of an experience can influence memory for depressive symptoms (Horwitz et al., Reference Horwitz, Zhao and Sen2023). Thus, patients’ reports during primary care visits may not accurately reflect actual depression or pain trajectories – leading to risk of over-and undertreatment such as medication titration and clinical inertia.
Recent studies have examined recall bias in retrospective symptom assessment through ecological momentary assessment (EMA). For example, in a study of recall bias of knee osteoarthritis symptoms, higher pain was reported at follow-up compared to prospective daily assessments (Previtali et al., Reference Previtali, Boffa, Di Martino, Deabate, Delcogliano and Filardo2022). Similarly, retrospective overreporting was found for gastrointestinal symptoms in patients with functional bowel disorders, when comparing prospective and retrospective assessments (Jones et al., Reference Jones, Yun, Wass, Rixon, Shah, Walker, Koloski, Holtmann, Talley and Beath2022). However, recall bias in depressive and pain symptoms has not, to the authors’ knowledge, been examined previously in OAMM.
Therefore, we analysed data generated in a pilot trial evaluating the feasibility and acceptability of EMA among OAMM, with the goal of ascertaining the extent of discrepancies between recalled (retrospective) and daily (prospective) symptom reports. We also explored sociodemographic and clinical characteristics associated with greater symptom recall discrepancies between retrospective and prospective assessments.
Methods
Participants were recruited through the geriatric primary care practice of Weill Cornell Medicine (3/2024–9/2024) if they were ≥60 years, had a depression diagnosis (chart documented or self-reported), ≥ two chronic illnesses, a smartphone, and were English-speaking. We excluded patients with dementia, bipolar disorder, and severe mental illness based on chart review and self-report. Full details of the study have been described elsewhere (Mindlis et al., Reference Mindlis, Rodebaugh, Kiosses and Reid2026). Briefly, following informed consent, participants completed baseline validated questionnaires, followed by EMA surveys three times daily for two weeks. Within one week of completing all EMA surveys, participants completed a follow-up interview.
Measures
Depressive symptoms
Participants completed the Patient Health Questionnaire (PHQ-8) at baseline and follow-up. Scoring is identical to the PHQ-9 (Kroenke et al., Reference Kroenke, Spitzer and Williams2001).
Pain intensity
The PROMIS Pain Intensity 3a (Cella et al., Reference Cella, Riley, Stone, Rothrock, Reeve, Yount, Amtmann, Bode, Buysse, Choi, Cook, Devellis, Dewalt, Fries, Gershon, Hahn, Lai, Pilkonis, Revicki, Rose, Weinfurt and Hays2010) scale assessed pain intensity over the past week at baseline and follow-up. Participants rated their pain at its worst, on average, and currently on a 5-point scale ranging from ‘had no pain’ to ‘very severe’.
Sociodemographic characteristics
We assessed age, gender, race, ethnicity, education, income, and relationship status.
EMA measures
For this analysis, we focused on EMA items assessing symptoms of depression and pain intensity in participants who completed all interviews.
Depressive symptoms
The EMA survey included selected items from the PHQ-9 that might fluctuate in a two–three hour period and items assessing sleep and appetite (assessed once a day in the morning and evening surveys, respectively). One item assessing suicidal thoughts was excluded to maximize survey acceptability. Thus, participants rated PHQ-9 items for depressed mood, anhedonia, negative self-thoughts, fatigue, and trouble concentrating using wording adapted for brevity in previous EMA studies (Schleider, Reference Schleider2021), and given a time frame of ‘since my last survey’. The EMA survey also included a pain intensity item (‘What is your level of pain right now?’) (Cella et al., Reference Cella, Riley, Stone, Rothrock, Reeve, Yount, Amtmann, Bode, Buysse, Choi, Cook, Devellis, Dewalt, Fries, Gershon, Hahn, Lai, Pilkonis, Revicki, Rose, Weinfurt and Hays2010). Response options for all items ranged from 0 (Terrible) to 100 (Excellent) for sleep and appetite items, and from 0 (Not at all) to 100 (Extreme) for all other symptoms.
Statistical analysis
Analysis was carried out using SPSS V 29. Average scores for EMA items were calculated. Given the discrepancy between the EMA items range (0–100) and the follow-up questionnaires (0–3 for PHQ items; 1–5 for pain intensity), the mean scores on EMA items were transformed to a 0–3 scale for depression symptoms, and a 1–5 scale for pain intensity. Specifically, pain intensity scores were partitioned into five categories: 0–20 (1), 21–40 (2), 41–60 (3), 61–80 (4), 81–100 (5); whereas depression symptom scores were partitioned into four categories: 0–25 (0), 26–50 (1), 51–75 (2), 76–100 (3). Trouble sleeping and appetite items were reverse coded so that higher scores indicated more difficulty sleeping and worse appetite. Discrepancy scores were calculated as the recall (score on the retrospective follow-up interview) minus the average EMA-measured prospective scores for the two weeks for all depressive symptoms, and for the past week for pain intensity. Associations between discrepancy scores and baseline characteristics were evaluated through correlations. Following previous approaches to recall bias (Jones et al., Reference Jones, Yun, Wass, Rixon, Shah, Walker, Koloski, Holtmann, Talley and Beath2022), we explored recency effects by correlating day 14 EMA scores with discrepancy recall scores.
Results
Participants (N = 18) had an average age of 80.3 (SD = 7.8, range 67–95), were mostly female (89%) and non-Hispanic/Latino White (83%). Participants had significant depressive symptoms (mean PHQ-8 score of 8.7, SD = 5.8), including 39% who scored in the moderate-to-severe depression range. Over half (61%) reported moderate-to-severe pain intensity (i.e., score of 3 or greater on 1–5 scale of the PROMIS Pain Intensity 3a scale) at baseline.
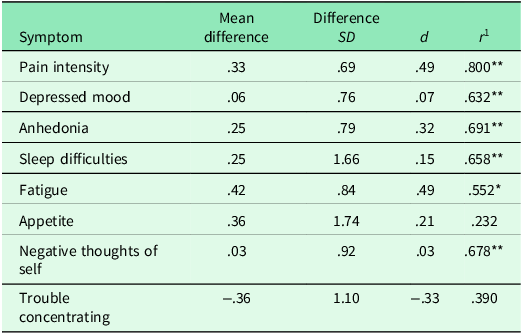
Recall of depressive symptoms and pain intensity during the two-week study period was overall higher than the average EMA scores (See Table 1). The difference was small overall (average d = .18), ranging from the smallest for negative self-thoughts (d = .03) to the largest for pain intensity (See Figure 1) and fatigue (d = .49). EMA reports and recalled scores at follow-up correlated for all domains except appetite and trouble concentrating.
Discrepancy between EMA-measured and recalled symptoms of depression and pain intensity during the two-week study period

Note: **p <.01, *p <.05. 1Represents the correlation between EMA-measured and recalled symptoms. Scores range from 1–5 for pain intensity, and 0–3 for PHQ-9 items.
Representation of differences between daily and averaged prospectively measured pain intensity compared to recalled scores over one week.

We examined the associations between baseline characteristics and discrepancy scores. Greater pain intensity at baseline was associated with greater recall discrepancy (i.e., between retrospective and prospective assessments) for trouble sleeping (r = .60), but lower discrepancy for anhedonia (r = −.56). Older participants had more discrepancy in anhedonia recall (r = .48). Higher income was associated with improved recall of negative self-thoughts (r = −.64) and trouble sleeping (r = −.59) and higher education was associated with better recall of negative self-thoughts (r = −.60).
Day 14 pain intensity was associated with discrepancies in recalled pain (r = −.52, p =.029) and appetite (r = −.480, p =.044). Further, discrepancies in trouble concentrating recall were associated with depressed mood and negative self-thoughts on day 14 (r = −.67, p =.002 and p = −.72, p <.001, respectively). No significant associations were found for day 14 anhedonia, trouble sleeping, fatigue, appetite, and trouble concentrating with recall discrepancy.
Discussion
We found preliminary evidence of recall bias in symptom reporting for pain intensity and depressive symptoms in OAMM. While small on average, some of the discrepancies had medium effect sizes, such as for pain intensity – with a difference equivalent to 3.3 points on the 0–10 pain intensity visual analogue scale. This level of discrepancy has real-world implications. Using the World Health Organization analgesic ladder as a guide, a patient who reports a pain score of 7 (severe pain) in the office could well receive a prescription for an opioid medication. In contrast, if the same patient reported a pain intensity score of 4 (moderate pain) via EMA symptom monitoring, they would likely be prescribed a non-opioid medication to mitigate pain.
Our findings support a small but expanding literature on recall bias for pain and depressive symptoms – albeit with younger populations – including overreporting at recall in knee osteoarthritis (Previtali et al., Reference Previtali, Boffa, Di Martino, Deabate, Delcogliano and Filardo2022) and functional bowel syndromes (Jones et al., Reference Jones, Yun, Wass, Rixon, Shah, Walker, Koloski, Holtmann, Talley and Beath2022). While we found that some baseline characteristics such as pain intensity were associated with greater discrepancies, no clear patterns emerged in line with prior research (Jones et al., Reference Jones, Yun, Wass, Rixon, Shah, Walker, Koloski, Holtmann, Talley and Beath2022). Similar to our findings of recency effects, a study on a non-clinical sample of younger adults found evidence of peak end bias, with more recent symptoms being more highly correlated than average scores over a two-week period for the PHQ-9 (Horwitz et al., Reference Horwitz, Zhao and Sen2023). Further research into recall bias in OAMM is needed, including identifying predictors of recall discrepancy.
To our knowledge, this is the first study of recall bias for pain and depression symptoms in OAMM, with additional strengths being the use of EMA to prospectively measure daily symptoms, and the wide age range of our sample (67–95). However, several limitations should be noted, with the main limitation being the discrepancy between the EMA items range and the follow-up questionnaires, which we handled via transformations. While these findings should be considered preliminary due to this discrepancy and there is a need for additional studies using consistent ranges, two items should be highlighted despite the transformations. First, if the cut-offs we used for EMA item ranges were incorrect, we would expect consistent bias across all variables; yet while some symptoms were overreported (e.g., pain and depressed mood), other symptoms had almost no difference (e.g., negative thoughts of self), and we found no correlations between others (e.g., prospective and retrospective reports of appetite and trouble concentrating). Further, while transformations can affect some analyses, correlations are not as impacted by scoring, and even with a different transformation we would expect the correlation patterns to be the same. Thus, although interpretation would be simpler if transformations were not necessary, our current results cannot be explained by the need for transformations. Finally, we did not assess baseline cognitive function beyond excluding participants with chart-documented or self-reported dementia diagnoses and, relatedly, depressive symptoms may have impacted memory (Singh-Manoux et al., Reference Singh-Manoux, Akbaraly, Marmot, Melchior, Ankri, Sabia and Ferrie2010; Nafilyan et al., Reference Nafilyan, De Coulon and Avendano2025). Considering mild cognitive impairment may be as high as 50–60% in primary care settings (Kulshreshtha et al., Reference Kulshreshtha, Parker, Fowler, Summanwar, Ben Miled, Owora, Galvin and Boustani2024; Summanwar et al., Reference Summanwar, Owora, Ben Miled, Dexter, Kulshreshtha, Strunk, Jiang, Coppedge, Disla, Galvin, Boustani and Fowler2025) where it often goes unrecognized (Liu et al., Reference Liu, Jun, Becker, Wallick and Mattke2024), additional studies are needed that can determine differential rates of recall bias based on cognitive function. Given our sample composition, it is also possible that OAMM without depressive symptoms would display less recall bias in pain symptoms. However, given the high co-occurrence of chronic pain and depressive symptoms in older adults (Bair et al., Reference Bair, Robinson, Katon and Kroenke2003; Mcqueenie et al., Reference Mcqueenie, Jani, Siebert, Mcloone, Mccowan, Macdonald, Mair and Nicholl2021), these findings are still relevant to this population.
Recall bias is a significant issue for clinical research, and an even bigger one for primary care providers. Chronic pain and depression care are typically delivered in primary care, where there is limited time and competing priorities when caring for OAMM. Even when structured assessments are used, the most common questionnaires for both pain (e.g., Brief Pain Inventory, Cleeland and Ryan, Reference Cleeland and Ryan1994, PEG Scale Assessing Pain Intensity and Interference, Krebs et al., Reference Krebs, Lorenz, Bair, Damush, Wu, Sutherland, Asch and Kroenke2009, PROMIS Pain intensity Scale, Cella et al., Reference Cella, Riley, Stone, Rothrock, Reeve, Yount, Amtmann, Bode, Buysse, Choi, Cook, Devellis, Dewalt, Fries, Gershon, Hahn, Lai, Pilkonis, Revicki, Rose, Weinfurt and Hays2010), and depression (PHQ-9, Kroenke et al., Reference Kroenke, Spitzer and Williams2001, Geriatric Depression Scale, Sheikh and Yesavage, Reference Sheikh and Yesavage1986) rely on retrospective assessments covering periods between one and two weeks. Notably, while we found evidence of recall bias in a two-week period, primary care visits may happen months apart, and OAMM are asked to recall long periods. Better quality data on pain intensity and depression symptoms are needed for OAMM. EMA-based approaches to remote symptom assessment in the inter-visit period, such as automated tools or daily dairies, may offer patients and providers better quality data to aid decision making.
Conclusions
Our sample size precludes us from generalizing these findings, and the use of a different response scale for EMA and recall items limits some of our findings. However, even with correlations which are not affected by scoring transformation, we saw notable patterns. Given the reliance on retrospective assessment in primary care settings for OAMM, these provocative data need to be confirmed in larger studies to establish the magnitude of symptom recall discrepancies in larger samples of OAMM, as well as mitigating strategies to better care for this population in primary care.
Data availability statement
The study data set cannot be publicly shared as consent was not sought from participants to allow for the publication of deidentified data sets. Analytic code is available upon request.
Acknowledgements
None.
Author contributions
IM: Study concept and design, statistical analysis, interpretation of data, drafting of the manuscript, final approval of the version to be published. MCR: Study concept and design, critical revision of the article, and final approval of the version to be published. TLR: Study concept and design, interpretation of data, critical revision of the article, and final approval of the version to be published.
Funding statement
None in the design, methods, subject recruitment, data collections, analysis, and preparation of this paper. This work was supported by the National Institute on Aging [Mindlis: T32 AG049666; Reid: K24AG053462, P30AG022845]. Research reported in this publication was additionally supported by the National Center For Advancing Translational Sciences of the National Institutes of Health under Award Number [UL1TR002384] (REDCap).
Competing interests
The authors have no conflicts.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. Written informed consent was obtained from all subjects.


 Open access
Open access