


Attention deficit/hyperactivity disorder (ADHD) is a heritable neurodevelopmental condition, characterized by inattention, hyperactivity and impulsivity, which first manifests in childhood, and in most persists into adulthood whether at full clinical or subthreshold level (Posner et al., Reference Posner, Polanczyk and Sonuga-Barke2020; Faraone et al., Reference Faraone, Bellgrove, Brikell, Cortese, Hartman, Hollis, Newcorn, Philipsen, Polanczyk, Rubia, Sibley and Buitelaar2024). This disorder affects around 2.5% of adults worldwide (Faraone et al., Reference Faraone, Bellgrove, Brikell, Cortese, Hartman, Hollis, Newcorn, Philipsen, Polanczyk, Rubia, Sibley and Buitelaar2024). ADHD commonly co-occurs with other psychiatric disorders and somatic diseases, including metabolic and cardiovascular diseases (CVDs) (Rietz et al., Reference Rietz, Brikell, Butwicka, Leone, Chang, Cortese, D’Onofrio, Hartman, Lichtenstein, Faraone, Kuja-Halkola and Larsson2021; Li et al., Reference Li, Chang, Sun, Garcia-Argibay, Du Rietz, Dobrosavljevic, Brikell, Jernberg, Solmi, Cortese and Larsson2022; Libutzki et al., Reference Libutzki, Neukirch, Reif and Hartman2024).
Observational studies have shown ADHD was associated with more than 1.5-fold increased risk of heart failure (HF) and coronary artery disease (CAD) (Li et al., Reference Li, Chang, Sun, Garcia-Argibay, Du Rietz, Dobrosavljevic, Brikell, Jernberg, Solmi, Cortese and Larsson2022). However, these associations may be inflated due to shared familial liability, as recent studies using national multi-generational data have noted familial co-aggregation and small-to-moderate genetic correlations between ADHD and CVDs (Li et al., Reference Li, Zhou, Vos, Bos, Steen, Wray, Hartman and Snieder2025; Rietz et al., Reference Rietz, Brikell, Butwicka, Leone, Chang, Cortese, D’Onofrio, Hartman, Lichtenstein, Faraone, Kuja-Halkola and Larsson2021). Although such positive genetic correlations may reflect genetic confounding (horizontal pleiotropy), they may also indicate a causal pathway (vertical pleiotropy), or a combination thereof (van Rheenen et al., Reference van Rheenen, Peyrot, Schork, Lee and Wray2019).
Two previous Mendelian randomization (MR) studies, employing genetic variants as instrumental variables (IVs), suggested a causal link between ADHD and both HF and CAD (Leppert et al., Reference Leppert, Riglin, Wootton, Dardani, Thapar, Staley, Tilling, Davey Smith, Thapar and Stergiakouli2021; Zheng and Cai, Reference Zheng and Cai2025). These studies relied on the genome-wide association study (GWAS) of ADHD in 2019 (ADHD2019), which identified 12 significant loci (Leppert et al., Reference Leppert, Riglin, Wootton, Dardani, Thapar, Staley, Tilling, Davey Smith, Thapar and Stergiakouli2021; Zheng and Cai, Reference Zheng and Cai2025). The most recent ADHD GWAS meta-analysis (ADHD2023) (Demontis et al., Reference Demontis, Walters, Athanasiadis, Walters, Therrien, Nielsen, Farajzadeh, Voloudakis, Bendl, Zeng, Zhang, Grove, Als, Duan, Satterstrom, Bybjerg-Grauholm, Bækved-Hansen, Gudmundsson, Magnusson and Børglum2023), incorporating expanded cohorts (included nearly twice the number of cases compared to ADHD2019), identified 27 significant loci and provided more precise genetic effect estimates. Additionally, six of the previously identified loci were not significant in ADHD2023. Thus, a re-evaluation of the potential causal effects of ADHD on CAD and HF using these updated and more powerful genetic data is warranted (Demontis et al., Reference Demontis, Walters, Athanasiadis, Walters, Therrien, Nielsen, Farajzadeh, Voloudakis, Bendl, Zeng, Zhang, Grove, Als, Duan, Satterstrom, Bybjerg-Grauholm, Bækved-Hansen, Gudmundsson, Magnusson and Børglum2023).
Furthermore, if the causal relationship exists, identifying potential modifiable mediators linking the association of ADHD with CAD and HF can provide potential intervention targets for preventing or delaying the incidence of CAD and HF in individuals with ADHD. One of the two MR studies (Zheng & Cai, Reference Zheng and Cai2025) identified some mediators, including educational attainment (EA), smoking, obesity, opioid use, and triglycerides. However, it did not investigate some important potential candidates, such as cardiometabolic (e.g., type 2 diabetes (T2D) and hypertension), psychiatric (e.g., depression), and lifestyle risk factors (e.g., alcohol drinking, sedentary behavior), all of which have been shown to be linked with ADHD (Li et al., Reference Li, Chang, Sun, Garcia-Argibay, Du Rietz, Dobrosavljevic, Brikell, Jernberg, Solmi, Cortese and Larsson2022; Cortese et al., Reference Cortese, Moreira-Maia, St Fleur, Morcillo-Peñalver, Rohde and Faraone2016; Glass and Flory, Reference Glass and Flory2010; Fleming et al., Reference Fleming, Fitton, Steiner, McLay, Clark, King, Mackay and Pell2017; Garcia-Argibay et al., Reference Garcia-Argibay, Li, Du Rietz, Zhang, Yao, Jendle, Ramos-Quiroga, Ribasés, Chang, Brikell, Cortese and Larsson2023; Cook et al., Reference Cook, Li and Heinrich2015), and are known to affect cardiovascular health. However, their specific role within the causal pathway from ADHD to CVD remains unclear, necessitating mediation analysis. Additionally, the previous identified mediators need to be replicated using the latest and larger GWASs.
MR provides a framework for causal inference by using genetic variants as IVs, mitigating bias from confounding and reverse causation under specific assumptions. Multivariable MR (MVMR) and two-step MR (also known as network MR) extend this approach to estimate direct and indirect effects via mediators (Carter et al., Reference Carter, Sanderson, Hammerton, Richmond, Davey Smith, Heron, Taylor, Davies and Howe2021). Our study had two objectives. First, we aimed to strengthen the evidence for a causal effect of ADHD on CAD and HF using the most recent GWAS data on ADHD (Demontis et al., Reference Demontis, Walters, Athanasiadis, Walters, Therrien, Nielsen, Farajzadeh, Voloudakis, Bendl, Zeng, Zhang, Grove, Als, Duan, Satterstrom, Bybjerg-Grauholm, Bækved-Hansen, Gudmundsson, Magnusson and Børglum2023), CAD (Aragam et al., Reference Aragam, Jiang, Goel, Kanoni, Wolford, Atri, Weeks, Wang, Hindy, Zhou, Grace, Roselli, Marston, Kamanu, Surakka, Venegas, Sherliker, Koyama and Ishigaki2022), and HF (Shah et al., Reference Shah, Henry, Roselli, Lin, Sveinbjörnsson, Fatemifar, Hedman, Wilk, Morley, Chaffin, Helgadottir, Verweij, Dehghan, Almgren, Andersson, Aragam, Ärnlöv, Backman, Biggs and Smith2020). Second, we aimed to identify and quantify the mediating roles of cardiometabolic risk factors, inflammation factors, lifestyle behaviors, psychiatric disorders, and socioeconomic factors.
METHODS
Study design
First, we used two-sample MR to investigate if effects of ADHD on the risk of CAD and HF are causal. Next, we used a two-step MR method leveraging GWAS summary statistics to quantify the extent to which selected cardiometabolic and inflammatory risk factors, lifestyle behaviors, psychiatric disorders, and socioeconomic factors mediate the identified causal relationships (Figure S1).
MR assumptions
MR yields causal estimates of the association between exposure and outcome via IVs, under three key MR assumptions. (1) the relevance assumption requires that the IVs selected are strongly associated with the exposure, a condition fulfilled by selecting SNPs with robust genome-wide significance (p < 5 × 10−8). (2) The independence assumption requires that the IV-outcome association is unconfounded. This is plausible due to Mendel’s laws of random segregation and independent assortment. (3) The exclusion restriction criterion assumes that IVs only affect the outcome via the exposure. This criterion is violated in case of horizontal pleiotropy. We tested the robustness of our findings to potential violation of the exclusion restriction with a number of sensitivity analyses detailed below.
The two-sample setting introduces two additional assumptions. (4) The two samples represent the same underlying population, characterized by comparable demographic profiles, shared environmental exposures, and a consistent genetic ancestry within their European descent. The samples were drawn from different databases of common European descent, ADHD GWAS includes iPSYCH, 23andMe, Psychiatric Genomics Consortium (PGC), and deCODE genetics; CAD GWAS includes UK Biobank and CARDIoGRAMplusC4D; HF GWAS includes UK Biobank. (5) Sample overlap is minimal. The potential impact of sample overlap on study conclusions was assessed by re-analyzing with individual SNPs or subsets of SNPs excluded and by comparing multiple MR estimation methods (e.g., IVW, MR-Egger, weighted median).
GWAS data sources and variable definitions
Table S1 shows the details on the selected GWASs for exposure, outcomes and mediators. The IVs for ADHD were obtained from the most comprehensive GWAS of ADHD to date (Demontis et al., Reference Demontis, Walters, Athanasiadis, Walters, Therrien, Nielsen, Farajzadeh, Voloudakis, Bendl, Zeng, Zhang, Grove, Als, Duan, Satterstrom, Bybjerg-Grauholm, Bækved-Hansen, Gudmundsson, Magnusson and Børglum2023), in 38,691 cases and 186,843 controls. ADHD cases were identified based on diagnoses made by psychiatrists (ICD-10, F90.0, F90.1, F98.8) and prescriptions for medication specific to ADHD (ATC-NA06BA, mostly methylphenidate). This GWAS identified 27 independent (LD r 2 < 0.1 within 500 kb), genome-wide significant (P < 5 × 10−8) SNPs.
Our outcomes included CAD and HF. The CAD GWAS was conducted among 1,165,690 participants (including 181,522 cases) of predominantly European ancestry (Aragam et al., Reference Aragam, Jiang, Goel, Kanoni, Wolford, Atri, Weeks, Wang, Hindy, Zhou, Grace, Roselli, Marston, Kamanu, Surakka, Venegas, Sherliker, Koyama and Ishigaki2022). In this GWAS, CAD cases were individuals with a myocardial infarction, chronic ischemic heart disease, or angina (using ICD-9 or ICD-10 codes), determined either by self-report or by linkage with morbidity or hospital registries. HF (47,309 cases) in the GWAS was defined as a clinical diagnosis of HF of any etiology, and controls (n=930,014) were participants without HF (Shah et al., Reference Shah, Henry, Roselli, Lin, Sveinbjörnsson, Fatemifar, Hedman, Wilk, Morley, Chaffin, Helgadottir, Verweij, Dehghan, Almgren, Andersson, Aragam, Ärnlöv, Backman, Biggs and Smith2020).
Five general categories of mediators were explored: (1) cardiometabolic risk factors (systolic blood pressure, SBP; diastolic blood pressure, DBP; T2D; body mass index, BMI), (2) inflammatory factors (C-reactive protein, CRP), (3) lifestyle behaviors (smoking initiation, SI; alcohol consumption; physical activity, PA; leisure screen time, LST), (4) psychiatric disorders (depression; anxiety; autism spectrum disorders (ASD); conduct disorder; personality disorder), and (5) a socioeconomic factor (EA). SBP and DBP values were the mean of two automated or two manual blood pressure measurements (Keaton et al., Reference Keaton, Kamali, Xie, Vaez, Williams, Goleva, Ani, Evangelou, Hellwege, Yengo, Young, Traylor, Giri, Zheng, Zeng, Chasman, Morris, Caulfield, Hwang and Kolcic2024). T2D was defined by a combination of diagnostic fasting glucose, casual glucose, 2h plasma glucose, HbA1c levels, and use of glucose-lowering medication, from either self-report and electronic medical records, depending on availability of data in the contributing cohort (Mahajan et al., Reference Mahajan, Spracklen, Zhang, Ng, Petty, Kitajima, Yu, Rüeger, Speidel, Kim, Horikoshi, Mercader, Taliun, Moon, Kwak, Robertson, Rayner, Loh, Kim and Chen2022). BMI was calculated by dividing weight (kg) by height squared (m2) (Yengo et al., Reference Yengo, Sidorenko, Kemper, Zheng, Wood, Weedon, Frayling, Hirschhorn, Yang, Visscher and GIANT2018). CRP levels (mg/l) were measured by immunoturbidimetry—a high sensitivity method on a Beckman Coulter AU5800 and were transformed according to the natural logarithm (Ligthart et al., Reference Ligthart, Vaez, Võsa, Stathopoulou, de Vries, Prins, Van der Most, Tanaka, Naderi, Rose, Wu, Karlsson, Barbalic, Lin, Pool, Zhu, Macé, Sidore, Trompet and Alizadeh2018). SI was defined as a binary phenotype (ever vs never smokers) obtained from self-report questionnaires (Liu et al., Reference Liu, Jiang, Wedow, Li, Brazel, Chen, Datta, Davila-Velderrain, McGuire, Tian, Zhan, Choquet, Docherty, Faul, Foerster, Fritsche, Gabrielsen and Vrieze2019). Alcohol consumption was defined as the average number of drinks a participant reported drinking each week, aggregated across all types of alcoholic beverages (Liu et al., Reference Liu, Jiang, Wedow, Li, Brazel, Chen, Datta, Davila-Velderrain, McGuire, Tian, Zhan, Choquet, Docherty, Faul, Foerster, Fritsche, Gabrielsen and Vrieze2019). PA and LST were based on self-report questionnaires (Wang et al., Reference Wang, Emmerich, Pillon, Moore, Hemerich, Cornelis, Mazzaferro, Broos, Ahluwalia, Bartz, Bentley, Bielak, Chong, Chu, Berry, Dorajoo, Dueker, Kasbohm, Feenstra and den Hoed2022). PA was defined as a binary phenotype (physically active vs inactive) defined as those with moderate-to-vigorous intensity physical activity (MVPA) during leisure time in contrast to those without. LST was defined as a continuous variable, measured by self-report questionnaires. Depression in the original GWAS was assessed by either self-report or the primary or secondary diagnosis of a depressive mood disorder from linked hospital admission records (Howard et al., Reference Howard, Adams, Clarke, Hafferty, Gibson, Shirali, Coleman, Hagenaars, Ward, Wigmore, Alloza, Shen, Barbu, Xu, Whalley, Marioni, Porteous, Davies, Deary and McIntosh2019). Diagnosis of personality disorders was according to DSM-IV criteria on the basis of structured clinical interviews (Witt et al., Reference Witt, Streit, Jungkunz, Frank, Awasthi, Reinbold, Treutlein, Degenhardt, Forstner, Heilmann-Heimbach, Dietl, Schwarze, Schendel, Strohmaier, Abdellaoui, Adolfsson, Air, Akil, Alda and McIntosh2017). Other psychiatric disorders were determined by a psychiatrist or from linked hospital admission records according to ICD-8, ICD-9, or ICD-10 codes (Meier et al., Reference Meier, Trontti, Purves, Als, Grove, Laine, Pedersen, Bybjerg-Grauholm, Bækved-Hansen, Sokolowska, Mortensen, Hougaard, Werge, Nordentoft, Breen, Børglum, Eley, Hovatta, Mattheisen and Mors2019; Grove et al., Reference Grove, Ripke, Als, Mattheisen, Walters, Won, Pallesen, Agerbo, Andreassen, Anney, Awashti, Belliveau, Bettella, Buxbaum, Bybjerg-Grauholm, Bækvad-Hansen, Cerrato, Chambert, Christensen and Børglum2019; Demontis et al., Reference Demontis, Walters, Rajagopal, Waldman, Grove, Als, Dalsgaard, Ribasés, Bybjerg-Grauholm, Bækvad-Hansen, Werge, Nordentoft, Mors, Mortensen, Cormand, Hougaard, Neale, Franke, Faraone and Børglum2021). EA was determined by mapping the highest level of education that a respondent achieved to an International Standard Classification of Education (ISCED) category and then assigning a years-of-education equivalent for each ISCED category; one standard deviation (SD) represents 3.4 years of schooling (Okbay et al., Reference Okbay, Wu, Wang, Jayashankar, Bennett, Nehzati, Sidorenko, Kweon, Goldman, Gjorgjieva, Jiang, Hicks, Tian, Hinds, Ahlskog, Magnusson, Oskarsson, Hayward, Campbell and Young2022).
Instrument selection
Table S1 shows the details on the selected GWASs for exposure, outcomes and mediators. The GWAS reported 27 independent genome-wide significant loci (r²< 0.1 within 500 kb, P < 5 × 10−8). For MR instrument construction we applied more stringent clumping (r²< 0.001 within 10 Mb) and harmonization filters. SNP alleles were oriented towards positive effects on the exposure. Then, we harmonized SNP alleles from the outcome GWAS to the exposure alleles. In case of palindromic SNPs, we inferred the correct strand based on allele frequency, and removed SNPs in case of ambiguity (i.e., allele frequency between 0.42–0.58). This resulted in 25 SNPs for ADHD. For multivariable MR, we first identified instruments for individual exposure or mediator variables in their respective GWASs. This resulted in a list of in total 6,518 SNPs. We extracted effect estimates of all of these SNPs from each GWAS. After clumping and allele harmonization, 4,055 SNPs remained.
Statistical analysis
Univariable MR: total effects of ADHD on CAD and HF
We estimated the associations of genetically instrumented ADHD on CAD and HF using univariable two-sample MR (2SMR). We calculated Wald ratios for each individual SNP (SNP-outcome effect divided by SNP-exposure effect), with standard errors derived by the delta method. These Wald ratios were pooled using random effects inverse-variance weighted (IVW) meta-analysis; the pooled estimate was then interpreted as a causal effect of exposure (here, a log odds higher genetic liability of ADHD) on outcome under the assumption that all SNPs are valid IVs (Hemani et al., Reference Hemani, Zheng, Elsworth, Wade, Haberland, Baird, Laurin, Burgess, Bowden, Langdon, Tan, Yarmolinsky, Shihab, Timpson, Evans, Relton, Martin, Davey Smith, Gaunt and Haycock2018).
Mediation analyses: the product-of-coefficients method
To estimate mediation by a single mediator, the product-of-coefficients method was used, which consisted of two main steps (i.e., two-step MR). The first step was to estimate the association of genetically instrumented ADHD with each intermediate trait using univariable MR. The second step was to estimate the association of the genetically instrumented mediator with the CVDs using instruments for the mediator as well as for ADHD using the inverse variance weighted multivariable MR (MVMR-IVW) method, with weights based on SNP-variance in the outcome. This allows for assessment of the direct effect of each mediator on CVDs, adjusting for ADHD. After these two steps, we estimated the indirect effect (i.e. the effect of ADHD on CVDs via each mediator) by multiplying the coefficients obtained in each step. Then, the proportion mediated by each mediator was estimated through dividing the indirect effect by the total effect (the univariable MR estimate of ADHD to CVD). We used bootstrapping to estimate the standard errors and 95% confidence interval (CI) for the indirect effect and the proportion mediated. If the bias-corrected 95%CI for indirect effect and the proportion mediated did not include zero, the indirect effect and the proportion mediated were considered to be statistically significant (Preacher and Hayes, Reference Preacher and Hayes2004).
For the intermediate traits, we only carried out the second step if the coefficients in the first step were significant. If subsequently the coefficients in the second step were also significant, the intermediate trait was considered as a mediator.
Sensitivity analyses
As a sensitivity analysis to our main product-of-coefficients mediation analysis, we used the difference-in-regression-coefficients method to corroborate estimates. The difference method consisted of the following steps. First, the direct effect of ADHD on CVD, adjusted for the mediator, was estimated with MVMR, using instruments for both mediator and ADHD. Second, the direct effect was subtracted from the total effect of ADHD on CVD (from univariable MR) to estimate the indirect, mediating effect of the mediator. The proportion mediated was then calculated by dividing the indirect effect by the total effect.
We estimated proportion mediated for all combinations of mediators. To this end, using MVMR, we modelled multiple mediators simultaneously together with ADHD using instruments for each variable in the model. Then, using the difference-in-regression-coefficients, we calculated indirect effects and proportions mediated through each combination of mediators.
Several sensitivity MR analyses were carried out to assess the robustness of our results. First, we assessed heterogeneity in Wald ratio estimates from individual SNPs with Cochran’s Q statistic; significance was interpreted as suggestive of horizontal pleiotropy. Second, we calculated MR-Egger intercepts to assess whether horizontal pleiotropy may have resulted in directional bias; we interpreted a significant non-zero Egger intercept as suggestive of directional, unbalanced horizontal pleiotropy. Third, we performed MR-Egger and weighted median MR methods that are robust to varying degrees of horizontal pleiotropy (Bowden et al., Reference Bowden, Davey Smith and Burgess2015). There are notable differences in the assumptions underlying the Weighted Median and MR-Egger methods compared to IVW MR. The Weighted Median method offers robust causal inference by calculating the weighted median, eliminating the need to assume all SNPs are valid or free from horizontal pleiotropy. In contrast, the MR-Egger method allows for and tests horizontal pleiotropy among SNPs, assessing this through a regression model that includes an intercept term. Fourth, we performed reverse MR analysis by genetically instrumenting mediators and CVDs using trait-specific genetic instruments.
All MR analyses were conducted using R (version 4.2.2) and the TwoSampleMR R package version 0.5.6. We adhered to the STROBE-MR guidelines in the execution and reporting of this study (Skrivankova et al., Reference Skrivankova, Richmond, Woolf, Davies, Swanson, VanderWeele, Timpson, Higgins, Dimou, Langenberg, Loder, Golub, Egger, Davey Smith and Richards2021).
RESULTS
Univariable MR: total effects of ADHD on CAD and HF
Figure 1 shows the 2SMR results using the IVW approach. Genetically instrumented ADHD was significantly associated with higher odds of CAD (OR 1.13, 95% CI [1.07, 1.19], p < .001) and HF (OR 1.11, 95% CI [1.05, 1.19], p < .001) respectively.
Genetically predicted effect of ADHD on CAD or HF using the two-sample MR method. Abbreviation: MR, Mendelian randomization; IVW indicates the inverse-variance weighted method; CAD, coronary artery disease; HF, heart failure.

Univariable MR: effects of ADHD on intermediate traits
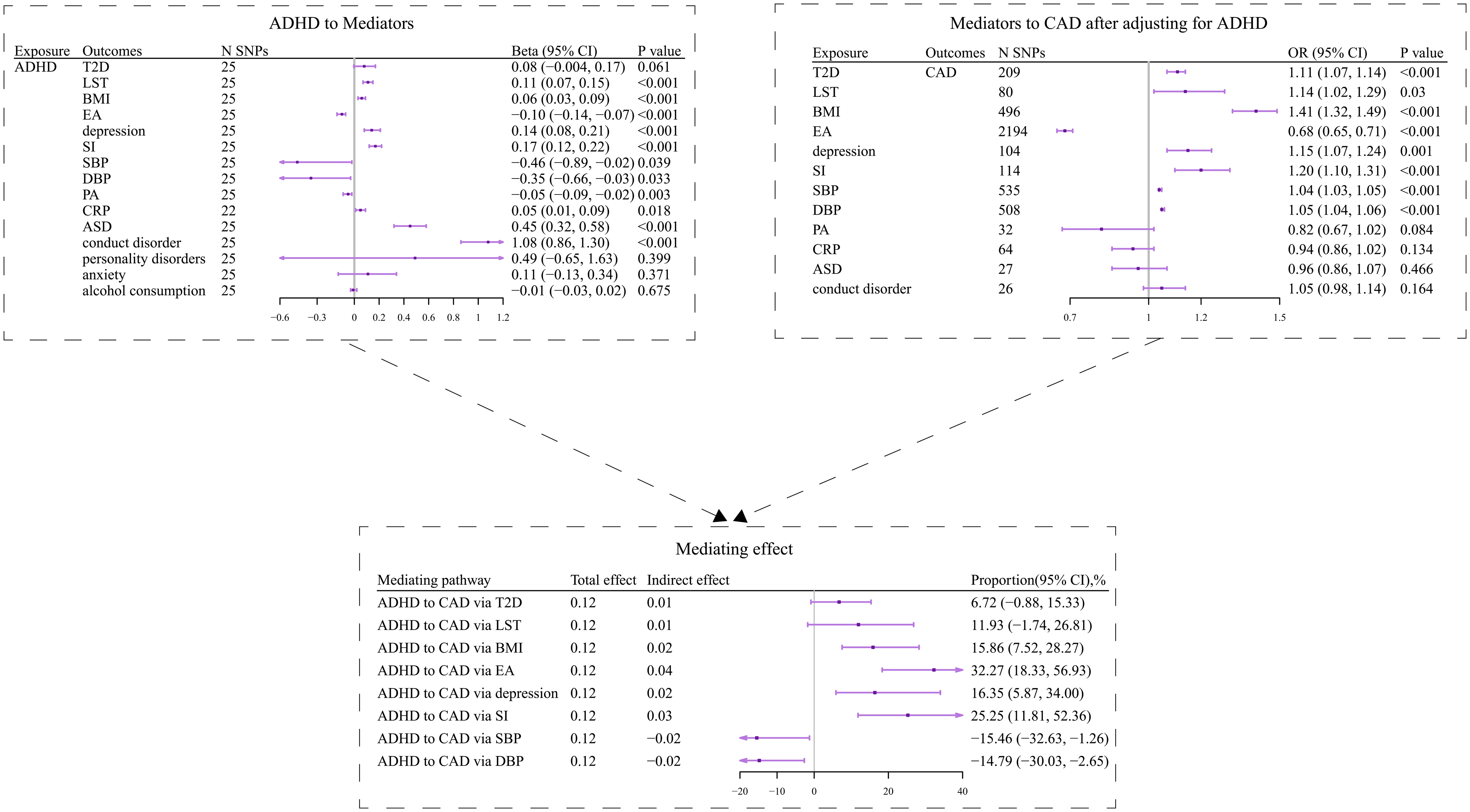
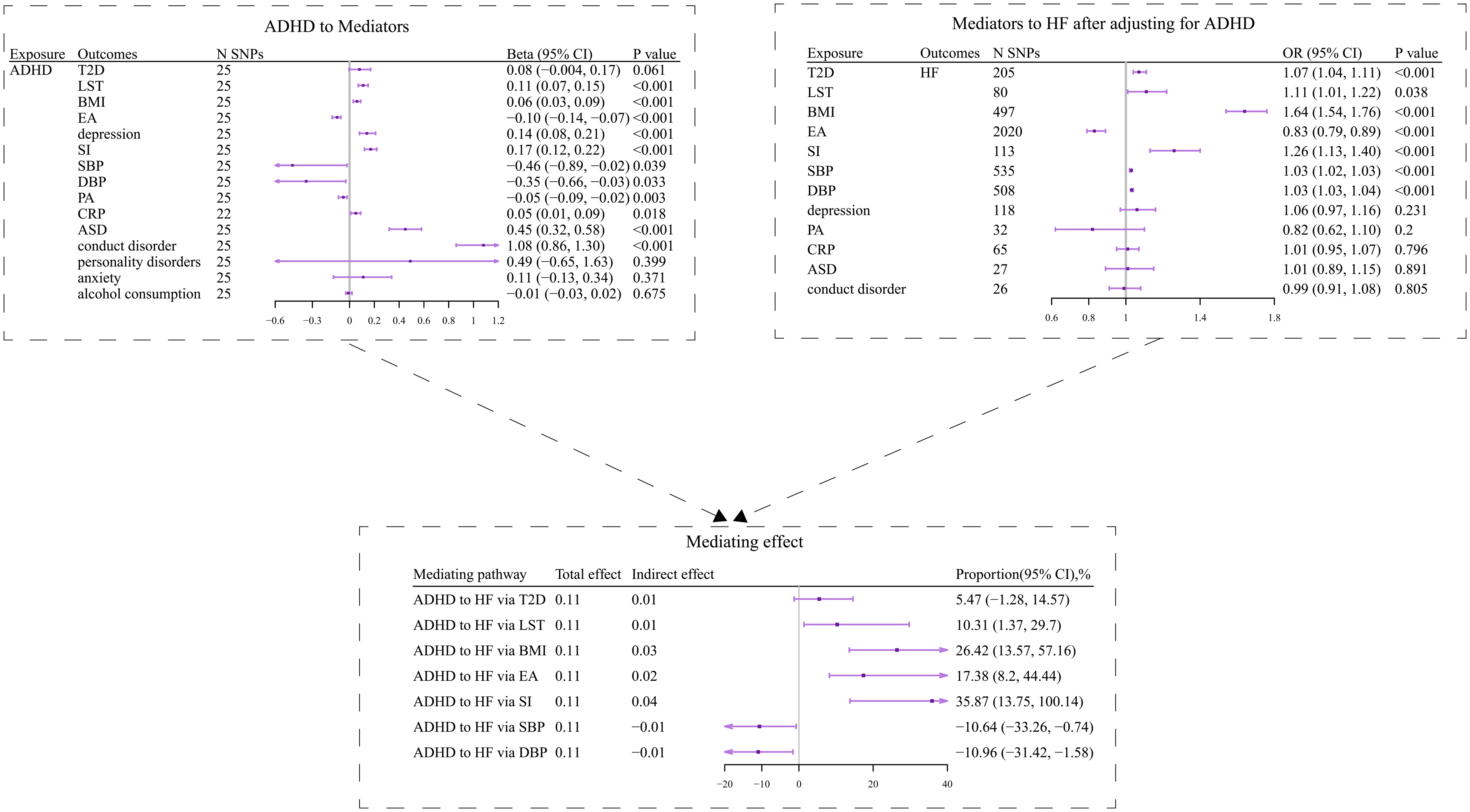
MR analyses between ADHD and each intermediate trait were performed using the main IVW approach. Genetically instrumented ADHD was borderline significantly associated with higher T2D odds (OR 1.09, 95% CI [1.00, 1.18]); higher risks of psychiatric disorders (ASD, OR 1.57, 95% CI [1.37, 1.78]; conduct disorder, OR 2.95, 95% CI [2.37, 3.66]; depression, OR 1.15, 95% CI [1.08, 1.23]); higher risk of SI (OR 1.18, 95% CI [1.13, 1.24]); higher LST (β 0.11 SD, 95% CI [0.07, 0.15]); higher BMI (β 0.06 kg/m2, 95% CI [0.03, 0.09]); higher CRP levels (β 0.05 ln(mg/L), 95% CI [0.01, 0.09]); lower EA (β −0.10 SD (3.4 years of schooling), 95% CI [−0.14, −0.07]); lower risk of PA (OR 0.95, 95% CI [0.91, 0.98]); lower DBP (β −0.35 mmHg, 95% CI [−0.66, −0.03]); and lower SBP (β −0.46 mmHg, 95% CI [−0.89, −0.02]). Genetically instrumented ADHD was not significantly associated with other risk factors (Table S2, Figure 2).
MR estimates and proportion for each individual mediator in the ADHD-CAD association using the product of coefficients method with bootstrap method-estimated 95% CIs.
Abbreviation: OR, odds ratio; CI, confidence interval; ADHD, Attention deficit hyperactivity disorder; CAD, coronary artery disease; T2D, type 2 diabetes; BMI, body mass index; LST, leisure screen time; EA, educational attainment; SI, smoking initiation; SBP, systolic blood pressure; DBP, diastolic blood pressure; PA, physical activity; CRP, C-reactive protein; ASD, autism spectrum disorder.
Multivariable MR: effects of intermediate traits on CVDs adjusting for ADHD
For risk factors significantly associated with ADHD in the first step, their causal effects on CVDs adjusting for ADHD were estimated. Adjusted for ADHD, one log-odds higher genetically instrumented T2D associated with 11% higher odds of CAD (OR 1.11, 95% CI 1.07 to 1.14). Genetically instrumented depression was significantly associated with 15% higher odds of CAD (OR 1.15, 95% CI 1.07 to 1.24). Genetically instrumented SI was associated with 20% higher odds of CAD (OR 1.20, 95% CI 1.10 to 1.31). One SD longer genetically instrumented LST was associated with 14% higher odds of CAD (OR 1.14, 95% CI 1.02 to 1.29). A 1-kg/m2 higher genetically instrumented BMI was associated with 41% higher odds of CAD (OR 1.41, 95% CI 1.32 to 1.49). One SD (3.4 years of schooling) longer genetically instrumented EA was associated with 31% decreased odds of CAD (OR 0.68, 95% CI 0.65 to 0.71). A 1-mmHg higher genetically instrumented DBP was associated with 5% higher odds of CAD (OR 1.05, 95% CI 1.04 to 1.06). One mmHg higher genetically instrumented SBP was associated with 4% higher odds of CAD (OR 1.04, 95%CI 1.03 to 1.05) (Table S3, Figure 2).
In addition, there was evidence of a causal effect of the following mediators on HF after adjustment for ADHD. Adjusted for ADHD, one log-odds higher genetically instrumented T2D associated with 7% higher odds of HF (OR 1.07, 95% CI 1.04 to 1.11). One log-odds higher genetically instrumented SI associated with 26% higher odds of HF (OR 1.26, 95% CI 1.13 to 1.40). Each SD longer genetically instrumented LST was associated with a 11 % (OR 1.11, 95% CI 1.01 to 1.22) higher odds of HF. A 1-kg/m2 higher genetically instrumented BMI was associated with 64% higher odds of HF (OR 1.64, 95% CI 1.54 to 1.76). One SD (3.4 years of schooling) longer genetically instrumented EA was associated with 17% lower odds of HF (OR 0.83, 95% CI: 0.79 to 0.89). A 1-mmHg higher genetically instrumented DBP was associated with 3% higher odds of HF (OR 1.03, 95% CI 1.03 to 1.04). A 1-mmHg higher genetically instrumented SBP was associated with 3% higher odds of HF (OR 1.03, 95% CI 1.02 to 1.03) (Table S4, Figure 3).
MR estimates and proportion for each individual mediator in the ADHD-HF association using the product of coefficients method with bootstrap method-estimated 95% CIs.
Abbreviation: OR, odds ratio; CI, confidence interval; ADHD, Attention deficit hyperactivity disorder; HF, heart failure; T2D, type 2 diabetes; BMI, body mass index; LST, leisure screen time; EA, educational attainment; SI, smoking initiation; SBP, systolic blood pressure; DBP, diastolic blood pressure; PA, physical activity; CRP, C-reactive protein; ASD, autism spectrum disorder.
Mediation estimation
Figure 2 shows the mediating effect produced by the product-of-coefficients method in the ADHD-CAD association. In the mediation analyses using the product of coefficients method, SI, depression, BMI, EA, DBP, and SBP, respectively, mediated 25.25% (95% CI 11.81% to 52.36%), 16.35% (95% CI 5.87% to 34.00%), 15.86% (95% CI: 7.52% to 28.27%), 32.27% (95% CI 18.33% to 56.93%), −14.79% (95% CI −30.03% to −2.65%), and −15.46% (95% CI −32.63% to −1.26%) of the association between ADHD and CAD. LST and T2D potentially mediated 11.93% (95% CI −1.74% to 26.81%) and 6.72% (95% CI −0.88% to 15.33%), respectively.
Figure 3 shows the mediating effects derived from the product-of-coefficients method in the ADHD-HF association. LST, SI, BMI, EA, DBP, and SBP explained 10.31% (95% CI 1.37% to 29.7%), 35.87% (95% CI 13.75% to 100.14%), 26.42% (95% CI 13.57% to 57.16%), 17.38% (95% CI 8.2% to 44.44%), −10.96% (95% CI −31.42% to −1.58%), and −10.64% (95% CI −33.26% to −0.74%) of the total effect of ADHD on HF, respectively. T2D mediated 5.47% (95% CI −1.28% to 14.57%).
Combined proportion mediated
Among the 2-mediator combinations, “EA+depression” explained the largest proportion 37.41% (95% CI 3.79% to 71.99%) of the effect of ADHD on CAD. Adding T2D and SI sequentially increased the proportion mediated (“EA+depression+T2D”: 71.32%, 95% CI 47.04% to 89.95%; “EA+depression+T2D+SI”: 81.23%, 95% CI 59.89% to 101.31%), which explained the highest proportion among all 3- and 4-mediator combinations. Adding BMI (“EA+depression+T2D+SI+BMI”) increased the proportion explained (83.59%, 95% CI 63.95% to 101.49%). Sequentially adding LST, DBP, and SBP did not increase the combined mediated proportion (“EA+depression+T2D+SI+BMI+LST”: 82.90%, 95% CI 62.15% to 100.47%; “EA+depression+T2D+SI +BMI+LST+DBP”: 78.25%, 95% CI 55.87% to 96.16%; “EA+depression+T2D+SI+BMI+LST+DBP+SBP”: 74.41% 95% CI 49.85% to 91.47%) (Figure 4).
The combinations with the largest proportion mediated per category in the ADHD-CAD association.
Abbreviation: TE, total effect; DE, direct effect; IDE, indirect effect; CI, confidence interval; CAD, coronary artery disease; T2D, type 2 diabetes; BMI, body mass index; LST, leisure screen time; EA, educational attainment; SI, smoking initiation; SBP, systolic blood pressure; DBP, diastolic blood pressure.

Among the combinations of 2 mediators, “T2D+SI” explained 76.48% (95% CI 34.85% to 148.32%) of ADHD on HF. This increased to 82.39% (95% CI 45.90% to 131.60%) after adding BMI (“BMI+T2D+SI”). Subsequently adding DBP, SBP, LST, and EA did not increase the combined mediated proportion (“BMI+T2D+SI+DBP”: 79.03%, 95% CI 43.79% to 116.75%; “BMI+T2D+SI+DBP+SBP”: 78.44%, 95%CI 42.66% to 110.56%; “BMI+T2D+SI+DBP+SBP+LST”: 71.12%, 95% CI 32.03% to 101.01%; “BMI+T2D+SI+DBP+SBP+LST+EA”: 60.64%, 95% CI 12.03% to 81.33%) (Figure 5).
The combinations with the largest proportion mediated per category in the ADHD-HF association.
Abbreviation: TE, total effect; DE, direct effect; IDE, indirect effect; CI, confidence interval; HF, heart failure; T2D, type 2 diabetes; BMI, body mass index; LST, leisure screen time; EA, educational attainment; SI, smoking initiation; SBP, systolic blood pressure; DBP, diastolic blood pressure.

Sensitivity analyses
Heterogeneity Q statistics were significant (P < 0.05) from genetic instruments for ADHD to the outcomes and mediators, suggesting widespread potential horizontal pleiotropy (Table S2). The MR-Egger intercepts, however, generally were not significantly different from zero, suggesting that any horizontal pleiotropy was balanced and thus did not bias our main results. Only in the ADHD on CAD analysis, the Egger intercept was significantly different from 0 (P = 0.032). In the MVMR-IVW analyses, there was reasonable instrument strength (F > 10) of SNPs for SBP, DBP, depression, SI, T2D, LST, and BMI in all MVMR analyses, although conditional instrument strength for ADHD and EA was low.
To corroborate the individual mediation results from the product-of-coefficients method, we used the difference-in-regression-coefficients method, in which we estimated the indirect effect of ADHD through each mediator by subtracting the direct effect of ADHD from the total effect. Among these mediators, only the indirect effect through SI was significant, SI mediated 24.68% (95% CI 11.18% to 65.69%) of the purported relation between ADHD and CAD (Figure S2), and 55.15% (95% CI 13.07% to 127%) between ADHD and HF (Figure S3).
In reverse MR analyses, EA was significantly associated with lower ADHD risk, while BMI, LST, T2D, SI, and depression were associated with higher ADHD risk (Table S5).
Discussion
This two-step MVMR study provides updated evidence supporting a causal effect of genetically predicted ADHD on increased risks of both CAD and HF, utilizing the largest available GWAS data for ADHD. We identified several modifiable risk factors, notably BMI, T2D, EA, SI, and depression for ADHD-CAD association, and BMI, T2D, and SI for ADHD-HF association, that jointly mediated a substantial proportion (over 80%) of these associations. These findings provide potential intervention targets for mitigating cardiovascular risk in individuals with ADHD.
Our study both confirmed and extended prior MR evidence linking ADHD to CAD and HF (Leppert et al., Reference Leppert, Riglin, Wootton, Dardani, Thapar, Staley, Tilling, Davey Smith, Thapar and Stergiakouli2021; Zheng and Cai, Reference Zheng and Cai2025) by leveraging the larger and more precise ADHD2023 GWAS. In contrast to an earlier study (Zheng & Cai, Reference Zheng and Cai2025), which examined smoking, obesity, and education but did not assess psychiatric disorders, T2D, hypertension, or alcohol drinking, PA, LST, and inflammatory factors as potential mediators, we identified previously unexamined mediators — notably depression, LST, and T2D — that significantly mediated the causal relationship between ADHD and CAD/HF. Unlike the prior MR study (Zheng and Cai, Reference Zheng and Cai2025) only using one-by-one mediation analyses, we also examined the role of combined psychiatric, metabolic, lifestyle, and socioeconomic factors in a unified model. The combined mediation proportions (> 80%) provide new insights into the way ADHD confers cardiovascular risk through multi-domain pathways.
We identified smoking behaviors, measured by SI, as a mediator for both CAD and HF. This aligns with previous studies demonstrating the association between ADHD on smoking (Zheng and Cai, Reference Zheng and Cai2025; Garcia-Argibay et al., Reference Garcia-Argibay, du Rietz, Lu, Martin, Haan, Lehto, Bergen, Lichtenstein, Larsson and Brikell2022; Soler Artigas et al., Reference Soler Artigas, Sánchez-Mora, Rovira, Vilar-Ribó, Ramos-Quiroga and Ribasés2023), including earlier smoking initiation, heavy smokers and increased difficulty with smoking cessation (Treur et al., Reference Treur, Demontis, Smith, Sallis, Richardson, Wiers, Børglum, Verweij and Munafò2021), and previous research reporting a clear dose-response relationship between smoking and CVD risk (Cho et al., Reference Cho, Shin, Kim, Kim, Byeon, Jung, Kang, Lee, Kim and Lip2024). The potential physiological mechanisms between smoking and CVD risk include oxidative stress, endothelial dysfunction, inflammation, and lipid modification (Chen et al., Reference Chen, Li, Zheng, Wang, Xie, Xu, Dai, Gu, Xia, Zhao, Liu and Xu2019). This indicates the importance of smoking prevention and cessation efforts in the ADHD population for cardiovascular health.
BMI also emerged as a main mediator in the pathway from ADHD to both CAD and HF. This is consistent with prior MR and cohort studies linking ADHD to higher BMI and obesity (Martins-Silva et al., Reference Martins-Silva, Vaz, Hutz, Salatino-Oliveira, Genro, Hartwig, Moreira-Maia, Rohde, Borges and Tovo-Rodrigues2019; Liu et al., Reference Liu, Schoeler, Davies, Peyre, Lim, Barker, Llewellyn, Dudbridge and Pingault2021). ADHD features, such as impulsivity and difficulties with planning, may contribute to unhealthy eating behaviors (e.g., overeating) and subsequent weight gain (Cortese and Castellanos, Reference Cortese and Castellanos2014), although this needs to be determined through research still. Given that obesity and elevated BMI are an important risk factor of CVD, the indirect pathway from ADHD to higher BMI to CVD suggests that managing BMI represents another intervention point.
Lower EA was identified as the single largest mediator for the ADHD-CAD association and also mediated the ADHD-HF association. This resonates with observations of poorer academic and occupational outcomes in individuals with ADHD (Soler Artigas et al., Reference Soler Artigas, Sánchez-Mora, Rovira, Vilar-Ribó, Ramos-Quiroga and Ribasés2023) and the established link between lower socioeconomic status and increased CVD burden (Schultz et al., Reference Schultz, Kelli, Lisko, Varghese, Shen, Sandesara, Quyyumi, Taylor, Gulati, Harold, Mieres, Ferdinand, Mensah and Sperling2018). Additionally, we found depression mediated part of the ADHD effect on CAD. The psychosocial challenges associated with ADHD can impact self-esteem and emotional regulation, potentially increasing vulnerability to depression (Garcia-Argibay et al., Reference Garcia-Argibay, Brikell, Thapar, Lichtenstein, Lundström, Demontis and Larsson2024). Depression, in turn, is a risk factor for CAD, possibly acting through metabolic dysregulation, stress-related coagulation abnormalities, and neurohormonal imbalances (Honigberg et al., Reference Aragam, Jiang, Goel, Kanoni, Wolford, Atri, Weeks, Wang, Hindy, Zhou, Grace, Roselli, Marston, Kamanu, Surakka, Venegas, Sherliker, Koyama and Ishigaki2022; Kwapong et al., Reference Kwapong, Boakye, Khan, Honigberg, Martin, Oyeka, Hays, Natarajan, Mamas, Blumenthal, Blaha and Sharma2023). This suggests that addressing depressive symptoms in individuals with ADHD could confer cardiovascular benefits.
While individual mediators were identified, these factors are often interrelated (Zhang et al., Reference Zhang, Chen, Pärna, van Zon, Snieder and Thio2022). The substantial joint mediation observed (over 80% for both CAD and HF by specific combinations) suggests that effective CVD risk reduction in ADHD likely requires a multifaceted approach. Strategies targeting obesity (e.g., diet, exercise), smoking cessation, educational support, and the prevention and treatment of T2D and depression are particularly relevant (Zhang et al., Reference Zhang, Chen, Triatin, Snieder, Thio and Hartman2024). Interventions promoting healthy lifestyles may offer dual benefits by potentially improving ADHD symptoms and mitigating cardiovascular risk factors (Choi et al., Reference Choi, Han, Kang, Jung and Renshaw2015). Similarly, effective ADHD treatment might improve academic or occupational functioning, indirectly influencing mediators like EA and depression (Jangmo et al., Reference Jangmo, Stålhandske, Chang, Chen, Almqvist, Feldman, Bulik, Lichtenstein, D’Onofrio, Kuja-Halkola and Larsson2019).
Strengths of this study include the use of the largest, comprehensive GWAS data on ADHD, predefined potential mediators, and CVD outcomes, improving instrument strength and analytical power. There are also limitations. First, this study assumes no interaction between the exposure (ADHD) and mediators, which currently cannot be modelled in the two-step MR. Second, although we obtain stronger instruments for ADHD compared to previous study based on GWAS ADHD2019 (Zheng and Cai, Reference Zheng and Cai2025), conditional instrument strength for ADHD in MVMR was still low (F < 10). Future GWAS may provide stronger instruments to corroborate these findings. Third, results using MR approach can be biased due to horizontal pleiotropy, an untestable violation of the exclusion restriction criterion. This might especially be true for our use of binary exposures, in which SNPs affect outcome through the underlying genetic liability rather than the binary state itself (Burgess and Labrecque, Reference Burgess and Labrecque2018). We therefore conducted sensitivity analyses, including MR-Egger and weighted median approaches, thought to be robust against varying degrees of pleiotropy. In general, these sensitivity analyses yielded consistent results, but we still need to interpret the main findings with some caution.
CONCLUSIONS
Our findings, based on the latest GWAS with a larger sample size, corroborate previous evidence suggesting a positive causal relationship between ADHD and CAD or HF, with substantial mediation by SI, EA, and BMI. This study also identified additional mediators, depression, and LST, and the substantial joint mediation patterns. Combined intervention on these factors may have beneficial effects on reducing risk of CAD and HF in individuals with ADHD.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/thg.2025.10037.
Data availability
GWAS data are available through the MRC IEU Open GWAS database (https://gwas.mrcieu.ac.uk/) and GWAS catalog (https://www.ebi.ac.uk/gwas/)
Funding
This research is supported by the European Union Horizon 2020 Research and Innovation Programme (grant 965381, TIMESPAN). This research reflects only the authors’ view, and the European Commission is not responsible for any use that may be made of the information it contains. This study was supported by National Natural Science Foundation of China (no.72342017; 72304207), Tianjin Natural Science Foundation Youth Project (no.25JCQNJC00010), and Chronic Disease Management Research Project of National Health Commission Capacity Building and Continuing Education Center (no.GWJJMB202510021044). Open access funding provided by University Medical Center Groningen. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Contribution statement
JL, YLZ, TX, CHLT, HS, and CAH were responsible for study conception and design. JL mainly performed the data analysis. JZ and CHLT performed the data analysis check. JL, YLZ, TX, ZKC, ZC, CHLT, HS and CAH performed the data interpretation. JL and YLZ drafted the manuscript. JL, YLZ, TX, ZKC, ZC, YGW, CHLT, HS, and CAH critically reviewed the manuscript. All authors approved the final version of this manuscript to be published. CAH, HS and CHLT are the guarantors of this work.
Competing interests
There are no potential conflicts of interest among all authors.








 Open access
Open access