


Introduction
The National Institute for Occupational Safety and Health (NIOSH) convened a consortium of 15 federal agencies and departments to develop the Emergency Responder Health Monitoring and Surveillance (ERHMS) system in 2012. This established a framework for the pre-deployment, deployment, and post-deployment phases during disaster response. Pre-deployment medical screening of responders as well as health monitoring and surveillance during the deployment were noted. 1 –Reference Funk and Horney 4
In 2017, NIOSH released a software platform, ERHMS Info Manager, for tracking and analyzing the data collected. 5 However, the ERHMS Info Manager software was retired on March 15, 2024. Therefore, agencies need to develop their own web-based reporting tools that work within their operational environment.
Urban Search and Rescue (US&R) is a branch of the United States Federal Emergency Management Agency (FEMA). It is composed of three Incident Support Teams (IST) and 28 state task forces. Unique to the US&R system is that physician Medical Officers (MOFR) are deployed with the IST, as well as physician Medical Team Managers (MTM) and paramedic medical specialists with each task force.
This study describes the design and field evaluation of web-based medical screening and reporting dashboard that improved workflow and provided daily health monitoring and surveillance of US&R responders.
Methods
In the Fall of 2024, an individual with a computer science background was engaged to gain an understanding of the MOFR’s and task force medical providers’ concept of operations and workflow to identify opportunities and provide solutions which were approved in March 2025.
Medical Screening Tool
The established practice was that the IST members’ medical screening examinations were performed in-person upon arrival at the base camp, as a Health Insurance Portability and Accountability Act (HIPAA) compliant method to provide medical information prior to arrival was not available.
The medical screen included a review of symptoms, past medical and surgical history, medications, allergies, and emergency contact information, followed by an in-person physical examination. This was a time-intensive process for the IST MOFRs and their members.
The Microsoft Forms tool (Microsoft Corporation, Redmond, Washington, USA) was identified as the optimal solution, as questions were customizable and information could be obtained prior to arrival. Individual responses and a summary compilation of all members were provided in a graphic table and spreadsheet format.
From an ethics and data security perspective, Protected Health Information (PHI) was handled in compliance with HIPAA. Submission access was limited to the MOFRs who received training on privacy and data security policies. A Business Associate Agreement (BAA) was established between Microsoft and US&R’s platform for hosting, transmission, and data storage, strengthening HIPAA compliance. The tool was distributed through Microsoft Teams IST Travel Chat (Microsoft) upon activation.
Web-Based Dashboard
A web-based dashboard was programmed that provided task force access to commonly used FEMA Incident Command System (ICS) forms (e.g., Medical Plan, Injury and Illness Log). The forms are also provided in a downloadable fillable PDF format. The dashboard provides the MOFRs password-protected access to the information outlined in Figure 1. This functionality allowed IST and task force medical providers one web-based location for their most common needs.
Password-protected MOFR access only information.

Injury and Illness Log
Tracking the submission and associated hand tabulation of task force daily Injury and Illness Logs was another identified opportunity for improved workflow using a web-based solution. This required a programming effort to allow the log, completed by a task force medical provider, to be submitted directly from the dashboard to the IST MOFR with PHI (e.g., patient name) removed and therefore not viewable by the MOFRs or the programmer. From an ethics and data security perspective, the form could be saved by the task force according to its HIPAA-compliant practices. A predetermined most common injury and illness list was provided (e.g., ankle sprain, cellulitis, diarrhea, fever, nausea, upper respiratory infection, and vomiting) with an open text box available for other conditions. The daily submissions and an automated tally of all task forces’ logs were available only to the IST MOFR to identify daily trends within and between task forces.
Medical Plan and MAPS Tool
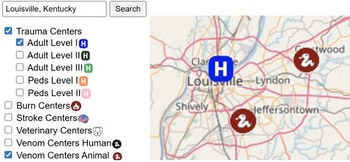
A MAPS tool, shown in Figure 2, provided resources from publicly available databases to aid medical providers in compiling a medical plan. For example, a hospital helipad’s latitude and longitude were determined by cross-referencing the 20,301 Federal Aviation Administration coordinates from an ArcGIS Hub database. A distance measurement tool was included that measures the distance between locations, e.g., from the task force’s base camp or search area to the nearest hospital.
Louisville, KY., Level 1 Hospital and Animal Venom Center Map.

An unexpected test of the various tools occurred within 2 weeks of approval and prior to a pilot test or training being performed. The US&R IST and 6 task forces involving 245 responders were deployed during the Severe Weather/Flooding—Central/Eastern US activation from April 2, 2025, to April 10, 2025.
The developer/programmer who was involved in the design, planning, and implementation of the various tools was also available during the deployment to troubleshoot any issues. A post-deployment survey was distributed via email within 2 weeks of task force demobilization, utilizing a Microsoft Forms tool (Microsoft) with the survey being closed after 2 weeks. This study was deemed by the UNMC Office of Regulatory Affairs as not human subject research (NHSR); therefore, no formal IRB review and approval was required.
Results
Medical Screening Tool
Despite no advance training or instructions on its use, 100% (35/35) of the IST members completed the pre-deployment medical screen. The average time to completion was 3 minutes and 38 seconds. The MOFR’s time commitment to perform an in-person medical screen was decreased with the medical history already available. A post-deployment survey response rate was 66% (23/35). Of those responding, 100% (23/23) opined that the medical screening form tool was intuitive, and the new process saved them time over the prior in-person medical screen.
Web-Based Dashboard
Even without advanced training or instructions on the use of the dashboard, 100% (16/16) of the respondents either agreed or strongly agreed that the dashboard was intuitive to use and saved them time over the prior workflow. Compiling all forms, reports, and tools on a single dashboard also improved the MTM, medical specialist, and MOFR workflow efficiencies.
Injury and Illness Log
Compliance among the 6 task forces to complete the Injury and Illness Log daily was 84% (67-100%). One task force was identified to have 8 cases of upper respiratory symptoms over a 6-day period. With the daily reports and automated summary compilation, the MOFRs were able to confirm that no other task forces were having similar illnesses which assisted in confirming operational readiness. One open text entry of a tick bite exposure validated one component of the post mission medical guidance. Medical providers identified the need for an abbreviated Injury and Illness Log when no cases were encountered. Having the programmer available to add this feature the same day as the request facilitated provider acceptance and satisfaction.
The post-deployment survey was completed by 89% (16/18) of the MTMs and medical specialists. Of those who were familiar with the prior injury and illness reporting workflow, 100% (9/9) opined that it did save time.
Medical Plan and MAPS Tool
Only 13% (2/16) of the respondents used the MAPS tool, although both noted it saved them time in preparing their medical plan. However, 56% (9/16) were not aware it was available, which emphasizes the need for advanced training in the use of the dashboard tools.
Limitations
The successful utilization of the daily-reporting Injury and Illness Log was dependent upon having physicians or paramedics embedded within the task forces. Responding agencies without medical providers would not be able to adopt this component.
Web-based tools were able to be utilized by US&R task forces using standard cellular connectivity. However, if cellular access became unavailable, as occurs during natural disasters, they also have enhanced internet connectivity with both satellite dishes and Starlink (SpaceX, Starbase, Texas, USA) capabilities. More austere conditions due to geography and weather may limit connectivity and use of the tools in real-time. Offline functionality is not available and would require the production of a mobile application. While many State US&R (SUSAR) agencies have enhanced internet access capabilities, those deployed without such capabilities would not be able to utilize this web-based platform when cellular access is unavailable.
With approval of the tools in March 2025 by the IST MOFRs and their use in the unexpected April 2025 deployment, a pilot test had not been completed, nor had there been any training of MTMs and medical specialists. This did not allow for all programming issues and workflow enhancements to be identified in advance. Any identified issues were mitigated by having the developer/programmer available to often provide same- or next-day solutions during the deployment.
The MAPS tool information is not continuously updated and serves only as a resource in the development of the medical plan. Facility operational readiness and capabilities are always dynamic during a natural disaster and must be verified.
While an in-person medical screen is performed at the time of demobilization, a post-deployment web-based medical screen was not; post-deployment health monitoring is also key to operational readiness and could be accomplished using the Microsoft Forms tool (Microsoft).
Finally, US&R embraced the ERHMS system guidelines but never adopted the ERHMS Info Manager software. With the software being retired, it was not possible to compare the functionality of the 2 platforms. Notably, once web-based tools that could be specifically customized to the workflow of IST MOFRs and task force medical providers were identified, they were readily adopted.
Discussion
A mission’s success is dependent upon ensuring operational readiness which was demonstrated in both the pre-deployment and deployment phases of this study. The Microsoft Forms tool (Microsoft) can be customized to meet most agency specific needs. However, this cannot be done in isolation and must include policies, procedures, and training in data management and privacy along with a BAA to strengthen HIPAA compliance.
A unique capability of the US&R system is that both the IST and task forces deploy with physicians, with task forces also including medical specialists, enabling daily medical and mental health monitoring. This influenced the design of the IST medical screening tool and supported each task force’s submission of a daily Injury and Illness Log. The Georgia Department of Health R-STaR program successfully utilized a different methodology using daily emails from responders during Hurricanes Matthew and Irma to monitor their health and safety which were reviewed by 3 epidemiologists.Reference Grippo, Edison and Soetebier 6 , Reference Turner, Edison and Soetebier 7 This emphasizes the need for any web-based platform to align with an agency’s staffing and workflow.
A mental health screen was preferred to be addressed during the in-person screen by the MOFR and was not included in the IST medical screening tool.
Months of extensive preplanning, design, and testing limited the troubleshooting and changes during the deployment. While there was no specific training on the use of the dashboard, task force providers were familiar with the forms utilized as they were electronic renditions of the approved US&R ICS forms. It is recommended that a web-based training environment be provided so that task forces can familiarize themselves with the dashboard functionality during scheduled training.
K-9s are deployed with every task force. During Hurricane Helene, the IST veterinarians oversaw the care of 80 dogs. A K-9 medical check-in tool and a K-9 injury and illness reporting tool are also under development. Both tools are extremely important as up to 67-84% of dogs on a deployment will have an injury and/or illness.Reference Gordon 8 , Reference Gordon and Ho 9
Other Search and Rescue (SAR) agencies (local, state, regional, national, or international) will be able to adopt this model by customizing web-based applications that align with their policies, procedures, staffing, and workflows using standard cellular internet access. Future research should determine whether this is possible with agencies having a different operational structure.
Conclusion
This study demonstrated that well-designed web-based tools can be successfully implemented during a US&R deployment. The system achieved complete pre-deployment screening compliance, high daily reporting adherence, and improved workflow efficiency without prior user training. Real-time developer support during the activation facilitated rapid optimization and user acceptance. These findings indicate that customizable, HIPAA-compliant web-based solutions can enhance responder health monitoring and operational readiness within disaster response operations.
Author contribution
Kael Michael Mlinek has met all the following authorship criteria:
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work;
Drafting the work or reviewing it critically for important intellectual content;
Final approval of the version to be published; and
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Eric Ernest, MD, has met all the following authorship criteria:
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work;
Drafting the work or reviewing it critically for important intellectual content;
Final approval of the version to be published; and
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Shaila Coffey, MD, in addition to being a deployed Medical Team Manager who used the dashboard tools in the field, has met all of the following authorship criteria:
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work;
Drafting the work or reviewing it critically for important intellectual content;
Final approval of the version to be published; and
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Arron Barksdale, MD, has met all the following authorship criteria:
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work;
Drafting the work or reviewing it critically for important intellectual content;
Final approval of the version to be published; and
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests
The authors declare none.
The conclusions, findings, and opinions expressed by authors in this article do not reflect the official position of the US Department of Homeland Security, the Federal Emergency Management Agency, Urban Search and Rescue Branch, or the authors’ affiliated institutions. Use of trade names is for identification only and does not imply endorsement.
Use of AI technology
Artificial Intelligence (AI) tools were not used for constructing any part of the manuscript.
Institutional or ethics review board
The University of Nebraska Medical Center (UNMC) Office of Regulatory Affairs (ORA) has determined that this project does not constitute human subject research as defined at 45CFR46.102. Therefore, it is not subject to the federal regulations, and formal IRB review and approval are not required.
Other acknowledgments
-
a. Microsoft—Microsoft Corporation, Redmond, Washington, USA
-
b. Starlink—SpaceX, Starbase, Texas, USA
-
c. Special recognition and thanks to Derek Parker (CATF-7) and Embret Fossum (UTTF-1) for their foundational support and assistance in operationalizing the various tools and to IST medical officers, Jared Strote MD (WATF-1) and Joshua Bobko (CATF-5), for their role in facilitating the successful implementation of the tools in the field.


 Open access
Open access