


Introduction
Cone Beam CT (CBCT) is an advancement in radiotherapy, ensuring accurate patient setup and treatment verification. Using CBCT delivers additional radiation dose, which must be kept As Low As Reasonably Practicable (ALARP) in compliance with the Ionising Radiation (Medical Exposure) Regulations (IR(ME)R). 1
This study investigated an issue that occurred in previous work conducted in Singleton Hospital, which identified imaging dose uncertainties caused by excess CBCT frames in Elekta X-Ray Volume Imaging (XVI) systems, analysing log files to reveal variations in imaging protocols and equipment performance. Reference Smakovs, Jenkins, Williams, Edwards and Lewis2 The results showed that some patients received additional imaging dose due to the delivery of excessive imaging frames above the nominal value, which can increase the risk of potential harm to healthy tissue and side effects for radiotherapy patients. Also, it showed that ‘fast’ protocols (with a gantry rotation speed of 360 degrees per minute) were most affected.
This study will further develop previous work by focusing specifically on breast imaging protocols, which were found to have the highest number of incidences of excess frames. Reference Smakovs, Jenkins, Williams, Edwards and Lewis2 By analysing the XVI log files and protocols, the objectives were to identify potential causes of excess frames, implement protocol adjustments to reduce unnecessary exposure, and verify that image quality remains clinically acceptable.
Methods
Radiographers at various UK centres first identified the issue of higher-than-expected frame counts during CBCT exposures. Instances were flagged where delivered frames exceeded the expected number by more than Elekta’s 10% tolerance threshold, potentially increasing patient imaging doses. To investigate further, log files from the Elekta XVI system were analysed, capturing occurrences where frame counts surpassed Elekta’s 10% threshold. 3
The individual files were investigated in detail to determine potential reasons for the excess frames. Log files from the Elekta XVI system were retrospectively analysed to identify instances where the delivered frame count exceeded the tolerance threshold of 10%. For the department breast protocols, the planned frames are 181; this would result in a warning message to appear at 199 frames (10%).
Figure 1 shows an example from the Left Breast Fast protocol configured to start gantry movement and image acquisition at 90 degrees and rotate counterclockwise (start angle deviation of 1 degree tolerance). ‘Inline reconstruct’ entries in the log files correspond to the individual acquisition frames. The protocol is configured to have a planned number of 181 frames with a 10% tolerance of 199 frames. This example received 200 frames, which triggered a warning message. Upon review, 6 frames (Inline reconstruct 0002–0006) were delivered with no significant gantry movement, indicating static imaging. Similar behaviour occurred with interrupted acquisitions due to the breath-hold technique in patients due to patient motion. The interrupted image procedure was excluded from analysis.
Left breast fast protocol static imaging occurrence.

The optimised XVI allows the gantry start angle to begin before the image acquisition start angle by applying a 5-degree offset, which will aim to reduce the static imaging frames at the beginning of the scan. As the stop angle cannot be adjusted the same way, excess frames are still seen as the gantry decreases rotation speed.
Table 1 compares the post (Clinical) protocol used and shows the configuration for an optimised version. By adding 5 degrees to the start angle and allowing the XVI to start acquisitions while the gantry has accelerated.
Left breast fast pre and post protocol setup

Effective dose was estimated using PC Program for X-ray Monte Carlo (PCXMC) simulation software 4 , with acquisition geometry matched to the CBCT breast protocols and dose being scaled using the delivered mAs and acquisition frame counts taken from the XVI files.
XVI scans were repeated 4 times for each protocol version (pre and post optimisation) using the Catphan 503 phantom. 5 The purpose of using the phantom was to assess image quality using the XVI mean pixel value for the density of polystyrene and LDPE material inserts to calculate contrast, and to use a uniformity Catphan insert to calculate uniformity, while ensuring no image artefacts were introduced by the optimised protocols. CBCT dosimetry was validated using a Radcal electrometer and a pencil ionisation chamber, measuring CTDI in air, which was measured pre- and post-optimised protocols to ensure agreement pre- and post-optimisation protocols with PCXMC and commissioning procedures.
Results
Left and right breast fast protocol
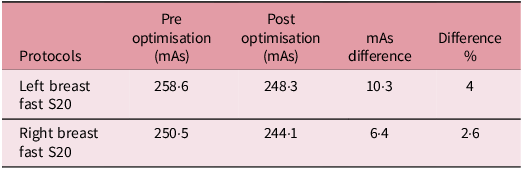
Table 2 summarises the mean delivered mAs values across 4 scans for each protocol. The percentage difference represents the relative change between the average pre- and post-optimisation values.
Left and right breast mAs comparison

Table 2 illustrates a reduction in mAs following the optimisation technique with a decrease of 4% and 2·6% for the Left and Right breast protocols, respectively. This reduction shows an improved consistency in frame delivery and a measurable decrease in imaging dose through the XVI system.
Table 3 shows the average number of delivered acquisition frames across 4 repeated scans for each protocol, showing reductions of 8 frames for the Left Breast protocol and 5 frames for the Right Breast protocol. This represents that the optimisation technique has an average reduction of 7 frames across these protocols, indicating improved system efficiency and reduction in imaging dose.
Left breast frames comparison

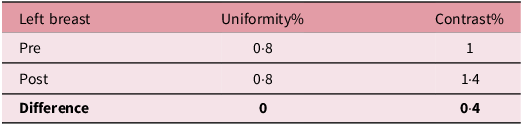
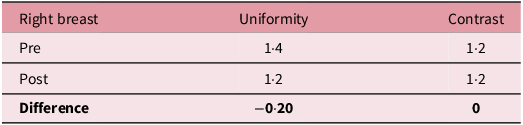
Tables 4 and 5 below summarises the pre- and post-optimisation protocols’ uniformity and contrast through the Catphan phantom to determine any clinical difference in image quality.
Left breast uniformity and contrast comparison

Right breast uniformity and contrast comparison

Tables 4 and 5 show that uniformity and contrast values remain within clinical tolerance following optimisation with minimal variation between pre- and post-optimisation protocols, which indicate that image quality remained comparable while reducing mAs and acquisition frame delivery, as shown in Tables 2 and 3.
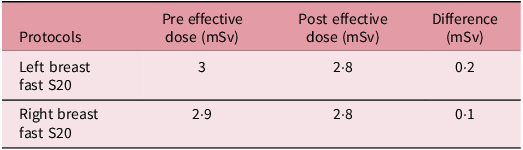
The pre- and post-optimisation effective dose estimates were scaled with PCXMC through recorded mAs and frames delivered from XVI files shown in Table 6.
Left and Right breast protocol effective dose measurements comparison

Table 6 shows effective dose estimates calculated using PCXMC with dose scaled using the delivered mAs and frame count obtained from XVI, and is supported by CTDI measurements. Effective dose decreased by 0·2 mSv for the Left Breast protocol and 0·1 mSv for the Right Breast protocol. These correspond to reductions equivalent to 14 and 7 chest X-rays, respectively. 6 This supports the ALARP principle and strengthens compliance with Ionising Radiation (Medical Exposure) Regulations (IR(ME)R) by minimising unnecessary patient exposure without compromising image quality.
Clinical results of the amount of higher expected frames comparison
Figure 2 shows the occurrence histogram, where the number of XVI occurrences goes above Elekta 10% tolerance. The date range used for the results is (Pre optimisation = 01/02/2025–31/03/2025 & Post optimisation = 07/04/2025–02/06/2025). This is approximately a 2-month review for pre-optimisation protocol and the 2-month post-protocol. Post optimisation (red) shows a lower median deviation (1·51%) compared to pre optimisation (blue, 2·51%), with fewer high-percentage outliers. The maximum deviations above tolerance reduced substantially with a drop from 16·1% to 8·5% for the Left Breast Fast S20 protocol and from 18·6% to 12·1% for the Right Breast Fast S20 protocol. The distribution shifts towards lower excess values, indicating improved protocol consistency and reduced unnecessary imaging dose.
Pre- post-optimisation comparison histogram.

The results demonstrate that this optimisation technique is transferable to other standard and fast CBCT protocols, which show similar static imaging trends.
Conclusion
This study demonstrates that optimising the Elekta XVI for Breast imaging protocols can reduce excess CBCT frame acquisitions while maintaining clinical image quality. Introducing modifications to gantry start angles prior to image acquisition, the number of static frames was reduced, which resulted in lower delivered mAs and effective dose. Catphan 503 phantom analysis supported the evidence that contrast and uniformity remained similar with minimal change, indicating the optimisation did not affect image quality. The optimised protocols configuration is applicable to other fast and standard CBCT protocols where similar behaviour in static imaging is recorded; this approach can be used across other protocols to reduce imaging dose.
The clinical occurrence of frames exceeding Elekta’s 10% tolerance threshold decreased, with maximum deviations reduced from 16·1% to 8·5% for Left Breast Fast S20 and from 18·6% to 12·1% for Right Breast Fast S20 Protocols. The effective dose was reduced with the breast protocols, 0·2 mSv for the Left and 0·1 mSv for the Right breast, which is equivalent to 14 and 7 chest X-rays, respectively, showing adherence to ALARP principles.
Although excess frame contributions to patient dose were small, their reduction improves overall system efficiency, consistency and confidence in imaging accuracy. Ongoing auditing of XVI performance is recommended to ensure compliance with Ionising Radiation (Medical Exposure) Regulations IR(ME)R and to support continuous quality improvement in image-guided radiotherapy. Through the clinical audit and commissioning work included in this report, the optimised protocol is being used clinically.
Competing interests
The authors declare no conflict of interest.





 Open access
Open access