


Individuals with severe mental illness (SMI) – such as schizophrenia and bipolar disorder – face a life expectancy 15–20 years lower than that of the general population.Reference Hjorthøj, Stürup, McGrath and Nordentoft1,Reference Miller and Bauer2 Although many factors contribute to this considerable mortality gap, a significant driver is preventable cardiovascular disease.Reference Nielsen, Banner and Jensen3 In 2014, the National Institute for Health and Care Excellence (NICE) recommended that mental health services carry out an annual physical health check on each patient with SMI, involving assessing lifestyle behaviours (such as smoking and substance misuse), measuring health parameters (such as blood pressure and body mass index, BMI) and taking blood tests to measure lipids and glycated haemoglobin (HbA1c).4 Audits assessing adherence to the guidelines, however, revealed low completion rates of physical health checks by early intervention in psychosis (EIP) teams. In 2017 – the year before our pilot study – only 38% of EIP patients in the South of England had received a full physical health check.5 The tests with lowest completion rates were the two blood tests (lipid panel and HbA1c). The National Health Service (NHS) Long Term Plan aims for EIP teams to provide full physical health checks for 390 000 patients with SMI by the 2023–2024 year,6 but blood tests are a formidable barrier to reaching this target.
There could be a number of reasons why blood test completion rates are particularly low: a lack of venepuncture-trained clinicians, patient refusal of venepuncture and logistical challenges in arranging for patients to attend a general practice (GP) surgery for blood tests.Reference Butler, de Cassan, Turner, Lennox, Hayward and Glogowska7 One potential way of addressing many of these problems is the use of point-of-care testing (POCT) designed for use with capillary whole blood samples. These ‘finger-prick’ tests are less invasive than venepuncture, produce results within minutes and some POCT devices are also portable. In a pilot study between 2018 and 2019, our team found that a POCT device was acceptable to clinicians and patients and increased the rate of physical health check completion in one EIP team.Reference Butler, de Cassan, Glogowska, Fanshawe, Turner and Walton8 We therefore aimed to scale up this study and introduce POCT to EIP teams across South East England, to assess whether these benefits would be seen at a larger scale.
Method
Quantitative evaluation
Study design
We conducted a real-world evaluation of the introduction of POCT technology to enable the delivery of NICE-recommended physical health screening for cardiovascular comorbidities in patients with SMI, as part of routine clinical care. The evaluation was a non-randomised controlled intervention study: POCT devices were provided to EIP teams across South East England, with teams in South West England acting as a comparator. The South West was chosen as a pragmatic comparator, being geographically close, having relatively similar demographic baseline data compared with other English regions and possessing a similar EIP caseload. POCT devices were introduced to three clusters of trusts in the South East in three waves: March, April and May 2021. The devices were Afinion™ 2 analysers with Afinion™ 2 HbA1c and Lipid Panel cartridges (Abbott Rapid Diagnostics Limited): 40 devices were provided to 30 teams across all 8 mental health trusts in South East England, with a total caseload of 2286. Caseloads within teams and trusts varied, and devices were allocated proportionately.
POCT training and use
Across eight NHS mental health trusts in the South East of England 75 clinicians from 30 EIP teams were trained to use the POCT devices. Training consisted of 1 h of clinical teaching on how to interpret HbA1c and lipid panel results, communicating these results to patients and helping clinicians know where to access lifestyle intervention advice or medical advice from doctors within their specific team. This was followed by 1 h of practical teaching on how to use the machine and an opportunity for clinicians to try out the POCT on each other. All teaching sessions were carried out with small groups of clinicians with the machine present and trainers working remotely on Microsoft Teams. Standard operating procedure sheets were provided to staff following the teaching, and verbal consent to being contacted to complete an optional questionnaire was obtained. Quality control and external quality assurance (QC/EQA) was carried out by staff on a monthly basis and managed by an external quality assurance company (Weqas: www.weqas.com).
Data collection
Anonymised, individual-level patient data were extracted from each trust. Eight of these were in the South East region (labelled 1–8 for anonymity) and four in the South West region (labelled A–D). For each of these trusts, data collection was made in reference to three 6-month time windows, with the end dates termed ‘census dates’. In the South East, the first two of these windows represented the pre-intervention period and the final time window was the 6-month period after POCT became available.
Four trusts (one in the South East region, three in the South West region) were excluded as data of sufficient quality could not be obtained. For one trust in the South East region (trust 7), data were available from only two 6-month periods (one when POCT was unavailable and one when POCT was available).
The two primary outcomes were the proportion of EIP patients within a trust receiving an HbA1c test in the preceding 6 months and the proportion of EIP patients within a trust receiving a lipid panel test in the preceding 6 months.
The secondary outcome was the proportion of EIP patients within a trust having a complete physical health check recorded in the preceding 6 months. This consists of recorded information for: HbA1c test, lipid panel test, smoking status, alcohol intake, body mass index (BMI), blood pressure and substance misuse.
For each census date, data consisted of the number of individuals for whom a health check for the given outcome was conducted within the preceding 6 months, together with the total number of individuals registered in the service for the entire duration of that period.
For trust A in the South West region, no BMI testing was routinely recorded. For this trust, data for the ‘all components’ outcome was based on the number of individuals who received tests for all health check components except BMI.
To triangulate our findings, we used comparator data from the National Clinical Audit of Psychosis (NCAP), which provides publicly available audit data from EIP services across England. We extracted NCAP results for the percentage of caseload receiving all of the required physical health checks over a 3-year period, and compared South East England (intervention) with the South West (comparator). The audits from 2019–2020 and 2020–2021 were considered pre-intervention and the 2021–2022 audit was considered post-intervention.
Statistical analysis
A power calculation was based on an assumed rate of 38% of individuals attending an annual screening.9 A sample size of 75 individuals per group has approximately 80% power to detect a difference in proportions of 19% versus 40% between groups within 6 months.
The age and gender breakdowns of eligible participants per trust were summarised in tables as means and standard deviation or percentages, as appropriate. For each of the primary and secondary outcomes, the proportion of participants tested within each of the specified 6-month periods was calculated separately for each trust for which data were available.
For each individual-level data outcome, a generalised linear mixed model for binomial data was fitted, treating the time points from each trust in the South East region as replicate observations. An estimate of change in the proportion of participants tested in the post-intervention period compared with the average of the proportions tested in the pre-intervention periods was obtained by modifying the contrasts of the fixed effect terms. As census dates of the data collection time windows varied only slightly between trusts, they were treated as directly comparable for the purpose of analysis. Within-trust correlation was modelled by including both a random intercept term for trust (capturing correlation between the repeated measurements for each trust) and a random coefficient for trust (allowing variation between trusts in the change from pre-intervention to post-intervention periods). Model comparison using the Akaike information criterion (AIC) suggested improvement of fit of these models compared with similar models that omitted the random effects terms.
To compare the average change in the South East trusts with the corresponding change in the single South West trust for which data were available, data from the South West trust were added to the model and an additional fixed effect term was added. Contrasts were again adjusted so that this additional parameter represented the difference in change from pre- to post-intervention periods for South East compared with South West trusts. The model comparison was made by AIC, comparing with a model without this additional parameter.
Statistical analysis was performed using R for Windows version 4.2.1 and the lme4 package.Reference Bates, Mächler, Bolker and Walker10
Clinician questionnaires
The clinician questionnaire was developed from a previous qualitative study by our team, which explored the barriers and drivers for engagement in POCT in community mental health teams.Reference Butler, de Cassan, Turner, Lennox, Hayward and Glogowska7 The questionnaire comprised a mix of multiple-choice questions and open-ended questions (for details see Supplementary Appendix 1, available at ). Its themes cover training, the practicalities of using the device, how it affects the clinician–patient interaction, clinician workload, quality control/external quality assurance and the impact of the technology. It was hosted on an online survey tool (JISC Online Surveys) and emailed to staff members who had completed the device training at two time points: 2 months and 8 months into using the device. This was designed to capture the experience of getting used to the device, as well as the experience of having used it for many months. Questionnaires were anonymous. Simple frequencies were obtained for each of the questions, with free-text responses analysed for content using thematic analysis.Reference Braun and Clarke11 A summary of the results is reported in Results section; these are ordered under ‘thematic area’ headings, which include quantitative data and themes qualitatively analysed from free-text questions.
The study, characterised as a service evaluation conducted at the service level and utilising anonymous patient data, was determined not to fall within the parameters requiring ethical review. The project was commissioned by NHS England and structured under a memorandum of understanding between NHS England, Oxford Clinical Commissioning Group and Oxford Health NHS Foundation Trust.
Results
Quantitative evaluation results
Summary information
For the intervention group (South East England), the mean age of participants was 31.3 years (s.d. = 11.6) in pre-intervention period 1 (∼March 2020 to September 2020), 32.8 years (s.d. = 12.0) in pre-intervention period 2 (∼September 2020 to March 2021) and 33.9 years (s.d. = 12.3) in the intervention period (∼March 2021 to September 2021). The percentages of male participants were 64% (714/1122) and 60% (732/1230) in the two pre-intervention periods and 60% (730/1218) in the intervention period. For the control group (South West England), the mean age of participants was 28.4 years (s.d. = 9.3) and 31.2 years (s.d. = 10.0) in the pre-intervention periods and 33.0 years (s.d. = 10.7) in the intervention period. The percentages of male participants were 80% (47/59) and 71% (48/68) in the pre-intervention periods and 73% (53/73) in the intervention period.
Health check data
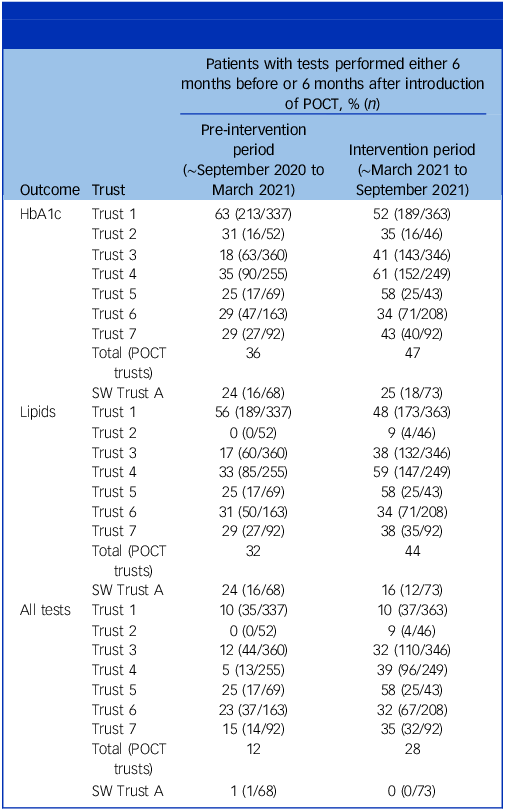
For most trusts there was an increase in testing after introduction of POCT, although there was variation between trusts both in the amount of testing performed and in the scale of any change (Table 1, Figs 1 and 2). For each outcome assessed there was evidence of an increase in testing rates during the post-intervention period (for the post-intervention period relative to the average of the pre-intervention periods: odds ratio 2.02, 95% CI 1.17–3.49 for HbA1c testing; odds ratio 2.38, 95% CI 1.43–3.97 for lipid testing; odds ratio 3.61, 95% CI 1.94–7.94 for all health check components). During the 6-month post-intervention period across trusts in the South East region, 47% of registered participants received an HbA1c test, 44% a lipid test and 28% all health check components. The comparable data collected from the trust in the South West region, where POCT was not introduced, showed no significant change in testing rates.
Number and percentage of eligible patients receiving physical health checks before and after introduction of POCT

POCT, point-of-care testing; SW, South West England.
Proportion of patients in each trust receiving testing for HbA1c (left), lipids (middle) and all tests (right), pre- and post-intervention.

Odds ratios (with 95% CIs) of the South East region, comparing the proportion of patients receiving HbA1c (left), lipids (middle) and all tests (right), in the 6-month post-intervention period compared to the average of the two 6-month pre-intervention periods. The x-axis is plotted on a lotharithmic scale.

NCAP data
In the 2 years before the intervention, both the South East and South West regions reported completed physical health checks in just under 60% of their caseloads in the NCAP audits (2019–2020: South East 59.04% (650/1101), South West 56.9% (474/833); 2020–2021: South East 58.30% (609/1044), South West 59.30% (401/676)). In the post-intervention period (2021–2022) completion rates in both regions increased: in the South East (intervention group) the rate rose to 83.6% (936/1120) and in the South West it increased to 66.6% (502/754). The intervention group had a relative increase of 43.4%, compared with the comparator group’s increase of 12.31% (Fig. 3).
Proportion of a region’s patient caseload with a complete set of physical health checks recorded on the National Clinical Audit of Psychosis audit. Time-point 1 (2019–2020 audit) and time-point 2 (2020–2021) are considered pre-intervention, and time-point 3 (2021–2022) represents the post-intervention period.

Clinician questionnaire results
Of the 75 EIP clinicians trained on the devices, 64 reported that they planned to use the devices during the study period. The other 11 reported that they were relying on another member of staff to take the lead on using the devices. Clinicians’ job descriptions and backgrounds varied considerably, and included both physical and mental health nurses, occupational therapists, psychological therapists and healthcare assistants.
All clinicians were sent the questionnaire 2 months and 8 months after the start of the study period; 55 (86%) responded to the 2-month questionnaire and 31 (48%) to the 8-month questionnaire.
Thematic area 1: Training
Overall, the online training was well received by the EIP clinicians: 35 respondents (64%) found it ‘very helpful’, 20 (36%) found it ‘quite helpful’ and no one found it ‘slightly helpful’ or ‘not helpful’.
Thematic area 2: Using the device
After 2 months of using the device, only 30 (54%) respondents reported feeling confident using the devices. However, after 8 months the proportion increased to 86.2% (27 respondents).
Within the first 2 months of using the device 17 (31%) respondents experienced problems. These were mainly due to the difficulty of carrying out the lipid test (which required more blood than the HbA1c test), the device shutting down during environmental temperature extremes and technique-related issues.
Thematic area 3: Patient interaction
Responses suggested that the POCT increased the opportunity for clinicians to discuss physical health with patients, and these interactions were often very rich. It was reported to be particularly useful for patients who were anxious or paranoid about venepuncture:
‘For patients who don’t like blood tests, this is ideal’ (P023)
‘Several service users have repeatedly refused venepuncture but have accepted POC testing, which has been really helpful’ (P018).
Another benefit seen by clinicians was that patients were able to receive all of the physical health results immediately:
‘Service users found it very helpful to get feedback straight away and advice re. healthy lifestyles based on “visible” results. They were also positive about us writing to their GPs for additional support/tests’ (P035)
‘It is good to complete the whole PHC [physical health check] and relevant blood tests together – as these can give results at the same time making the PHC more meaningful, as a plan of action can be implemented straight away’ (P034)
‘Don’t have to chase clients to get blood tests at GP’ (P036).
Between the 2-month and 8-month questionnaires, there was a 24% absolute increase in clinicians feeling confident in explaining brief lifestyle interventions to patients. They also reported that most patients (60%) responded positively to the device after 2 months, and this increased by 15% over the following 6 months.
Incorporating POCT into their clinical practice made 77% of clinicians responding to the 8-month questionnaire feel more empowered to help with a patient’s physical health:
‘Helped to build rapport with clients, they see you as having more skills and assessing all of them instead of just the mental illness’ (P056).
Thematic area 4: Quality control
Clinicians overwhelmingly found that having to carry out monthly combined QC/EQA had a negative impact on their practice, with 62% of respondents reporting that they found carrying out the monthly quality control checks difficult:
‘The quality control has been time consuming compared to the number of times we use the machine, especially as we were getting lots of error messages with the quality control samples and were not always sure why this was happening’ (P013).
After 2 months, 43% of respondents reported that the POCT had made their workload easier. However, at the 8-month questionnaire, this had dropped to 16%.
Thematic area 5: Impact of the technology
Multiple clinicians across different teams found POCT beneficial in a number of ways: (a) less invasive and better accepted by patients than venepuncture, (b) instant results, (c) no chasing up results from the GP and (d) an enriched clinician–patient interaction:
‘Loved by patients. Easy to use. Instant results’ (P022).
Interestingly, many respondents reported seeing improved uptake by patients who refused venepuncture, and also reported improvements in the number of patients with completed PHCs:
‘Our percentage of clients who have had a physical health review has more than doubled since they were first introduced into the service’ (P020)
‘We have seen a significantly improved compliance rate of PH checks’ (PO35).
Consistent negative feedback was related to technical issues with the device (set-up taking time, the device being temperamental in extremes of temperature, difficulty collecting enough blood for the lipid panel test, and also the monthly QC/EQA testing increasing clinician workload).
Perhaps the most representative comment about POCT was from clinician P021:
‘It is an excellent addition to the completion of physical health checks – but only if the POC machine works as expected’.
Discussion
This real-world implementation study suggests that POCT can increase the uptake of physical health checks by community EIP teams and lead to staff feeling empowered to address patients’ physical health problems.
The individual-level data revealed that the introduction of POCT was associated with a significant increase in the number of physical health checks: the percentage of patients who had a fully completed physical health check within a 6-month period increased from 10% before the introduction of the devices to 28% afterwards. There were also noticeable increases in the proportions who had HbA1c testing and lipid testing. This was not observed in the South West region, where POCT was not available, although the strength of this conclusion was limited by individual-level data being available from only one South West trust. We therefore used NCAP audit data to make additional comparisons against the region where POCT was not available.
The NCAP audit data reveal that in the 2 years before the intervention, both the South East and South West regions reported completed physical health checks in just under 60% of their caseloads annually. However, in the post-intervention period, in the South East (intervention group) this had increased from 58.3 to 83.6%, a much larger increase than the South West’s improvement from 59.3 to 66.6%. Only the South East met the NHS Mental Health Implementation Plan’s target for the 2021–2022 year of 70% of the caseload to have a completed physical health check.12 It is clear that causality cannot be determined from these findings – the fact that the audit dates do not align with the intervention period is a key limitation – but these data do support the findings of the individual-level data. It is important to note that these percentages are much higher than the individual-level data; this is likely due to the fact that these data were collected over a year, compared with 6 months, as well as discrepancies between the sampling methods used for NCAP audit and the individual data we extracted at the trust level.
Our finding that patients reported to clinicians that they preferred POCT is supported by a recent survey of 106 individuals with schizophrenia, 85% of whom preferred POCT to venepuncture.Reference Atkins, Taylor, Harland, Brewer, Williams, Chesney and et al13 The introduction of POCT resulted in most clinicians feeling more empowered to talk to their patients about physical health and it increased general rapport with patients. Immediate results, removing the complexities of patients having to await blood tests, were also commonly reported by staff as beneficial aspects of POCT.
As regards training clinicians on how to use POCT devices, most clinicians found it helpful and confidence in using the devices improved over time. It is notable that one-third of staff members reported technical or technique-related issues with the devices, particularly in the first questionnaire. In the future, top-up training may improve engagement with the devices.
Negative feedback from clinicians centred on technical and practical issues with using the POCT machine, as well as QC/EQA processes. Advances in device technology and ergonomics should therefore focus on reducing the size of the device, improving its resilience to atmospheric temperature extremes, improving the ease of QC/EQA testing and reducing the amount of blood required for lipid panel finger-prick testing. There were also requests for future POCT devices to carry out more blood tests relevant to patients with SMI, particularly prolactin, thyroid function and liver function tests. It is important for future studies to assess whether the introduction of POCT affects the frequency of venepuncture for tests not covered by POCT. We found that the use of POCT increased the workload for some members of staff. One solution developed by teams was for designated staff in the team to take responsibility for managing upkeep and governance of the devices in order to reduce the burden on front-line staff. This also highlights a limitation to the questionnaire data collected: the results of the second questionnaire are likely to be affected by a selection bias, and we may not have fully collected the views of those who gave up using the devices or did not find them helpful.
Further limitations
There are further limitations to this real-world implementation study. It was non-randomised and the presentation of training and questionnaires to the intervention group alone may have introduced observer bias. Our results may be affected by unadjusted confounding. There may be unmeasured, systemic differences between populations in the South East and South West regions, and it is important to note that the South East outperforms the rest of the UK on many economic, education and health metrics, potentially limiting the generalisability of the findings.14 We do not have a measure for what proportion of all physical health checks used POCT or whether some clinicians were using it more than others, and assessing whether the introduction of POCT changed physical health interventions or outcomes was outside the scope of the study. The study period straddled COVID-19 lockdowns, where physical health checks were deprioritised by many clinical teams.
Future research
Future research should explore the long-term sustainability of POCT, as well as assess the generalisability of these findings to diverse mental healthcare settings. One next step would be to longitudinally assess the impact of POCT on cardiometabolic health outcomes and mortality in indidivuals with SMI. There is now reasonably strong evidence to link POCT HbA1c testing and improved glycaemic control and disease management in diabetes populations.Reference Schnell, Crocker and Weng15 Whether this translates to individuals with SMI is yet to be discovered.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjp.2025.28
Data availability
The data that support the findings of this study are available on request from the corresponding author. National Clinical Audit of Psychosis audit data are available at: https://www.rcpsych.ac.uk/improving-care/ccqi/national-clinical-audits/national-clinical-audit-of-psychosis.
Author contributions
G.H., B.L. and M.L were responsible for conceptualising the research questions. S.A., P.J.T., T.R.F., M.G., I.S., G.H., B.L. and M.L were responsible for designing the study. J.B., J.B.F. and M.L. were responsible for data collection. T.R.F., B.L., G.H., M.G. and M.L. were responsible for analysis and interpretation of the data. M.L. was responsible for drafting the paper and all authors were involved in subsequent revisions and agree to be accountable for all aspects of the work.
Funding
The study was funded by National Health Service (NHS) England and structured under a memorandum of understanding between NHS England, Oxford Clinical Commissioning Group and Oxford Health NHS Foundation Trust. G.H., M.G., P.J.T. and T.R.F. were funded by the National Institute for Health and Care Research (NIHR) Community Healthcare MedTech and In Vitro Diagnostics Cooperative at Oxford Health NHS Foundation Trust (MIC-2016-018). T.R.F. receives funding from the NIHR Applied Research Collaboration Oxford and Thames Valley at Oxford Health NHS Foundation Trust. I.S. was employed by Oxford University Hospitals NHS Foundation Trust during the study. M.L., J.B.F. and J.B. were funded by NIHR Academic Clinical Fellowships. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Declaration of interest
None.






 Open access
Open access
eLetters
No eLetters have been published for this article.