


Introduction
Depression affects approximately one in five adolescents in their lifetime (Shorey et al., Reference Shorey, Ng and Wong2022) and is associated with social isolation, lower academic attainment, physical health issues, and suicidality (Clayborne et al., Reference Clayborne, Varin and Colman2019; Fombonne et al., Reference Fombonne, Wostear, Cooper, Harrington and Rutter2001). Many adolescents with depression will never receive psychological support (Pile et al., Reference Pile, Shammas and Smith2020). To improve access, young people recommend delivering support in schools (Pile et al., Reference Pile, Herring, Bullard, Loades, Chan, Reynolds and Orchard2022) and national UK policy now promotes the delivery of low-intensity psychological interventions within schools (e.g. Mental Health Support Teams; Department of Health and Social Care and Department for Education, 2018). Mental Health Support Teams (MHSTs) offer low-intensity interventions for mild-to-moderate mental health issues delivered by Education Mental Health Practitioners (EMHPs), a complementary role to child and young people’s wellbeing practitioners (CWPs) who primarily work in community settings. However, evidence for the effectiveness of early interventions in educational settings is limited. A review of randomised controlled trials (RCTs) suggested that guided self-help for depression in children and young people was associated with moderate effects compared with control conditions, but yielded slightly poorer outcomes compared with face-to-face therapy (Bennett et al., Reference Bennett, Cuijpers, Ebert, McKenzie Smith, Coughtrey, Heyman, Manzotti and Shafran2019). Meta-analytic results for depression interventions in schools found small-to-medium effects compared with control conditions, but no clear advantage when compared with active comparators (Gee et al., Reference Gee, Reynolds, Carroll, Orchard, Clarke, Martin, Wilson and Pass2020). Combining co-development work with insights from cognitive science to suggest key intervention targets could enable the development of more accessible, effective and clearly defined (and so scalable) interventions. One example of this is an intervention called IMAGINE (Integrating Memories And Generating Images of New Experiences), which has been co-developed with young people, parents and practitioners. Whilst rigorous evaluation is ongoing, at this stage of developing IMAGINE and its training materials, it is also crucial to explore its compatibility with the intended workforce for successful future implementation.
IMAGINE is a brief, imagery-based psychological intervention targeting dysfunctional mental imagery and autobiographical memory processes. Individuals with depression commonly exhibit recurrent intrusive imagery of past distressing events, demonstrate impaired capacity to generate detailed representations of positive future experiences, and display a tendency towards over-general autobiographical memory retrieval (e.g. Dalgleish and Werner-Seidler, Reference Dalgleish and Werner-Seidler2014; Pile et al., Reference Pile, Smith, Leamy, Oliver, Bennett, Blackwell, Meiser-Stedman, Stringer, Dunn and Holmes2021a). These have been highlighted as worthwhile treatment targets for psychological intervention and are likely to be developmentally appropriate (Holmes et al., Reference Holmes, Blackwell, Burnett Heyes, Renner and Raes2016; Pile and Lau, Reference Pile, Lau and Cohen Kadosh2020). IMAGINE incorporates three key techniques: (1) imagery rescripting procedures to reduce distress associated with intrusive negative imagery (Pile et al., Reference Pile, Smith, Leamy, Oliver, Bennett, Blackwell, Meiser-Stedman, Stringer, Dunn and Holmes2021a for protocol and case example); (2) positive imagery generation to create vivid prospective images; and (3) memory specificity training to increase specificity and access to memories. IMAGINE was co-designed for young people aged 16–18, manualised and based on cognitive behavioural therapy (CBT) principles. Memory specificity training is facilitated through a mobile app that prompts young people to complete a daily autobiographical memory task. IMAGINE has been evaluated in a case series (Pile et al., Reference Pile, Smith, Leamy, Oliver, Bennett, Blackwell, Meiser-Stedman, Stringer, Dunn and Holmes2021a) and a feasibility RCT (n=56; Pile et al., Reference Pile, Smith, Leamy, Blackwell, Meiser-Stedman, Stringer, Ryan, Dunn, Holmes and Lau2018; Pile et al., Reference Pile, Smith, Leamy, Oliver, Bennett, Blackwell, Meiser-Stedman, Stringer, Dunn and Holmes2021b), both of which demonstrated high feasibility (e.g. 89% retention) and acceptability (4.26 out of 5) and no safety concerns. Intention-to-treat analysis found large effects in favour of IMAGINE (relative to an active treatment) at post-intervention in reducing depressive symptoms (d=−1.34, 95% CI [−1.87, −0.80]) and improving memory specificity (d=0.79 [0.35, 1.23]). The active ingredients and valued outcomes have been identified in a process evaluation (Pile et al., Reference Pile, Schlepper, Lau and Leamy2023). A phase IIB RCT is currently in progress (ISRCTN14015295; Pile et al., Reference Pile, Tinch-Taylor, Carter, Richardson, De Rijk, Leamy, Blackwell, Meiser-Stedman, Dunn, Byford, Holmes, Creswell and Smith2025) in which IMAGINE is delivered by low-intensity practitioners. The 16-to-18-year age range was selected as it represents both a period of heightened vulnerability to depression and a critical window for preventing maladaptive cognitive styles from becoming entrenched. This narrow age band was chosen to minimise developmental heterogeneity and ensure age-appropriate content. However, should IMAGINE demonstrate efficacy, co-designing adapted manuals with younger age groups would be warranted to maximise reach.
Given that IMAGINE is a brief, manualised, CBT-based intervention, low-intensity practitioners could be an appropriate workforce to offer it. However, without adequate consideration of compatibility, interventions are unlikely to be adopted or sustained (Proctor et al., Reference Proctor, Landsverk, Aarons, Chambers, Glisson and Mittman2009), and MRC guidance recommends evaluating both effectiveness and implementation processes for complex interventions (Skivington et al., Reference Skivington, Matthews, Simpson, Craig, Baird, Blazeby, Boyd, Craig, French and McIntosh2021). Implementation science, therefore, can support the development of novel interventions by helping understand how they can become embedded into routine practice (Eccles et al., Reference Eccles, Armstrong, Baker, Cleary, Davies, Davies, Glasziou, Ilott, Kinmonth, Leng, Logan, Marteau, Michie, Rogers, Rycroft-Malone and Sibbald2009). For example, pre-implementation work can characterise the nature of contexts to explore their ‘readiness’ and the extent to which they have capacity and capability to facilitate implementation. Implementation science theory, such as normalisation process theory (NPT), may help understand key barriers and enablers to successfully implement new interventions. NPT focuses on the work that people do individually and in groups to embed interventions into routine practice (Dalkin et al., Reference Dalkin, Hardwick, Haighton and Finch2021; May et al., Reference May, Finch, Mair, Ballini, Dowrick, Eccles, Gask, MacFarlane, Murray, Rapley, Rogers, Treweek, Wallace, Anderson, Burns and Heaven2007). NPT is organised into four constructs: coherence (how people understand and make sense of an intervention), cognitive participation (how people engage and participate with an intervention), collective action (how intervention work is spread across stakeholders and the resources required to support this), and reflexive monitoring (how people appraise the effects of an intervention) (McEvoy et al., Reference McEvoy, Ballini, Maltoni, O’Donnell, Mair and MacFarlane2014).
More generally, three recent reviews highlight that there is limited research investigating the implementation of mental health support in schools (Clarke et al., Reference Clarke, Sorgenfrei, Mulcahy, Davie, Friedrich and McBride2021; Gee et al., Reference Gee, Wilson, Clarke, Farthing, Carroll, Jackson, King, Murdoch, Fonagy and Notley2021; Roach et al., Reference Roach, Cullinan, Shafran, Heyman and Bennett2023) and provide initial insights. For example, Gee et al. (Reference Gee, Wilson, Clarke, Farthing, Carroll, Jackson, King, Murdoch, Fonagy and Notley2021) highlighted community factors (e.g. stigma), provider characteristics (e.g. staff competence), organisational capacity (e.g. leadership support), training and technical assistance and intervention characteristics. Meanwhile, barriers and facilitators identified by Roach et al. (Reference Roach, Cullinan, Shafran, Heyman and Bennett2023) were organisational demands (e.g. time, cost, space, capacity), the intervention and how it is explained (e.g. lack of flexibility to tailor materials, lack of user-friendly materials), training and communication, the implementation strategy, and mental health stigma. A mixed methods study evaluated implementing MHSTs in 25 trailblazer sites (Ellins et al., Reference Ellins, Hocking, Al-Haboubi, Newbould, Fenton, Daniel, Stockwell, Leach, Sidhu and Bousfield2023). Factors enabling the implementation were schools welcoming in-house mental health support and strong recruitment to the EMHP training programme. Barriers included that staff felt the mild-to-moderate scope was restrictive and did not match rising complexity in mental health issues encountered by staff, challenges defining the scope of MHSTs (e.g. whether they were to focus on direct psychological intervention versus systems change), and challenges retaining EMHPs, partly due to issues with career progression and the role being limited to offering low-intensity CBT interventions. Some groups were also perceived to be under-served by MHSTs; namely young people with neurodivergent conditions, young people from minoritised ethnic backgrounds, and those experiencing social adversity.
The aim of this study is to explore the views of practitioners about potential barriers and enablers to implementing novel interventions for adolescent depression in schools. To address this aim, we presented a description of IMAGINE as an example for practitioners to consider. NPT was considered a suitable theory to guide this study as it has been used in a range of study settings and has been proposed to be appropriate for the prospective investigation of implementation factors. This includes in early intervention development work where there is limited or no hands-on experience of delivery to consider issues of normalisation to support intervention refinement and implementation planning (May et al., Reference May, Rapley, Mair, Treweek, Murray, Ballini, Macfarlane, Girling and Finch2015; McEvoy et al., Reference McEvoy, Ballini, Maltoni, O’Donnell, Mair and MacFarlane2014). NPT also aligns with realist evaluation approaches that focus on how relationships between intervention contexts and mechanisms of action lead to intervention outcomes (Pawson and Tilley, Reference Pawson and Tilley2004) and thus may help consider how to optimise potential intervention effects. By drawing on implementation theory, our findings may also be generalised to other brief, school-based mental health interventions. We sought to answer the following research questions:
-
What implementation processes may act as barriers and enablers to implementing a novel intervention for depression (IMAGINE) and how might these work?
-
What contextual factors may act as barriers and enablers to implementing novel interventions for depression and how might these work?
Method
We conducted a phenomenological, qualitative interview study using reflexive thematic analysis (Braun and Clarke, Reference Braun and Clarke2022). We chose reflexive thematic analysis as it is a well-established, flexible approach. Using this approach meant we could balance inductively exploring participant views and being open to unexpected findings, while also deductively making sense of the data considering theory and the broader literature. The overarching theoretical framework of our study was critical realism. Critical realism posits that there is an objective, knowable world that exists independently of human observation (i.e. ontological realism) and that knowledge production is fallible, approximate, and influenced by our own standpoint (i.e. epistemological subjectivism) (Maxwell, Reference Maxwell2012). To ensure explicit and comprehensive reporting, we used the COnsolidated criteria for REporting Qualitative research (COREQ) (Tong et al., Reference Tong, Sainsbury and Craig2007) (see Appendix A, Supplementary material). We also considered proposed quality criteria for reflexive thematic analysis studies (Braun and Clarke, Reference Braun and Clarke2021a).
Reflexivity
Critical realism aligned with the reflexivity aspect of reflexive thematic analysis as it positions researchers as active agents in producing knowledge and highlights the importance of acknowledging our viewpoints and biases in the study conduct. Therefore, we provide a brief overview of our experiences and perspectives most relevant to this study. The first author (lead researcher and interviewer) is a White man, training to become a clinical psychologist in South London and with experience of low mood as an adolescent. They previously worked as a research assistant on an implementation science project and as an assistant psychologist in the NHS, and completed a training course in low-intensity cognitive behavioural interventions for common mental health problems in adults. The first and second authors were not involved in developing IMAGINE. The second author is a consultant clinical psychologist in a specialist CAMHS service and a Higher Education institution co-director for a Children and Young Person’s Psychological Trainings (CYP-PT) where CWPs, EMHPs and their supervisors are trained. The third author is a consultant clinical psychologist in a specialist CAMHS service and research lead for a university clinical psychology programme. The last author is a senior lecturer in clinical psychology who led the development of IMAGINE.
Sampling and recruitment
Participants were (1) qualified low-intensity practitioners (CWPs, EMHPs) with experience working in schools and (2) practitioners whose role is to clinically supervise these low-intensity roles. Only participants working in England were eligible. We aimed to recruit 10–15 low-intensity practitioners and 10–15 supervisors. We considered recommendations for determining sample size in qualitative studies (Braun and Clarke, Reference Braun and Clarke2021b; Sim et al., Reference Sim, Saunders, Waterfield and Kingstone2018) to arrive at this sample size estimate. We felt this reflected the expected depth of the data collected, given the topic was not overtly emotive or emphasising participants’ personal identities, and our aim to capture diversity in terms of the geographical area of work and associated factors (e.g. differences in local policies and training programmes, ethnic and socioeconomic demographics). This is consistent with similar studies (e.g. Connell et al., Reference Connell, McMahon, Harris, Watkins and Eng2014; Sanders et al., Reference Sanders, Foster and Ong2011).
Convenience sampling was used to recruit participants through dissemination of study advertisements via social media (i.e. Twitter, Facebook groups, LinkedIn) and professional networks (e.g. mailing lists). We employed snowball sampling by asking participants to inform other eligible staff. Finally, we used purposive sampling to recruit participants from different geographical areas and teams.
Procedure and data collection
Demographic information included the number of years practitioners were in role, the geographical area of their workplace, and type of organisation they work in (e.g. NHS, third sector, local authority). The interview topic guide (Appendix B, Supplementary material) was developed based on previous qualitative research that used NPT (McEvoy et al., Reference McEvoy, Ballini, Maltoni, O’Donnell, Mair and MacFarlane2014). Given the prospective nature of the study, we did not include questions related to reflexive monitoring that we deemed more relevant to later implementation stages. The topic guide was revised following consultation with young people and adults with lived experience as well as pilot interviews (n=2).
One-to-one interviews were conducted remotely on Microsoft Teams by the first author. No participants who had interviews scheduled dropped out or withdrew their participation. No interviews were repeated. Practitioners participated in interviews from private rooms. All interviews were videorecorded. Interviews began with questions about participants’ job role; their views on current psychological support for depression; and whether any novel, one-to-one, low-intensity interventions had been implemented in their team. Following these questions, the interviewer shared a link to a YouTube video describing IMAGINE. After watching this, participants were asked about their views on IMAGINE and what it might be like to implement it in their service. Throughout the data collection and analysis stages, the first author took notes to reflect on how interviews were progressing, their position as a researcher, and how this was influencing the research process and interpretation of findings.
Data analysis
Data analysis followed a six-step approach to reflexive thematic analysis (Braun and Clarke, Reference Braun and Clarke2022). These were:
-
(1) Transcription: the auto-transcription function in Microsoft Teams was used to generate initial versions of transcripts with the first author then listening to interview recordings to correct and amend them on a pragmatic basis (e.g. Evers, Reference Evers2011), with the aim of capturing a relatively close verbatim transcription of what participants said. Transcripts were not returned to participants for comment.
-
(2) Data familiarisation: through repeated reading of transcripts while taking reflexive notes to reflect on initial impressions.
-
(3) Coding: data were coded in NVivo. We planned to code interviews deductively using an NPT-based coding manual (May et al., Reference May, Albers, Bracher, Finch, Gilbert, Girling, Greenwood, MacFarlane, Mair, May, Murray, Potthoff and Rapley2022). However, on reflection, this deductive approach felt like a barrier to exploring the meaning of participant viewpoints, particularly as the code definitions were quite specific and technical in nature and so did not readily map onto the data. As such, we decided to code interviews inductively with the intent of foregrounding participant perspectives and remaining open to different readings of the data. The first two transcripts were coded by two team members.
-
(4) Initial theme development: similar codes were grouped in an iterative process based on shared meaning.
-
(5) Refining and defining themes: at this stage, it felt useful to consider NPT constructs as this supported the identification of areas of overlap and redundancy across a large number of varied candidate themes. For example, themes that appeared to relate to how participants made sense of IMAGINE [i.e. coherence] were grouped and considered in relation to one another. This approach also helped with developing a narrative to make sense of how themes connected, including the distinction of themes that foregrounded contextual factors rather than the implementation of IMAGINE. The process of theory refinement continued into step 6, the writing-up phase.
Steps were broadly sequential, although the process was recursive in revisiting steps at different points. The first author led the data analysis, with input from the research team at different stages. The intention of involving the wider team was not to arrive at a ‘true’ reading of the data, but to consider multiple perspectives and to provide a quality and rigour check. As the first author felt that the views of low-intensity practitioner group and supervisor group in interviews did not diverge markedly, all interviews were analysed together.
Methodological detail for IMAGINE: identification and inclusion criteria
The RCT methodology for identifying young people was co-designed with those with lived experience. They highlighted that we need to take a more active approach to identifying young people with depression and that diagnostic assessments could result in stigma. The RCT protocol is, therefore, to screen all young people aged 16–18 for depressive symptoms using the Mood and Feelings Questionnaire, invite those scoring above cut-off to take part in the first assessment, and then offer intervention to those that score above clinical cut-off again 2 weeks later. In current UK low-intensity services, young people are usually offered an intervention for ‘low mood’ following referral. In the Results section, we will reflect on the terminology used by the participants.
The inclusion and exclusion criteria in the RCTs are designed to maximise access whenever possible (with the exception of targeting a narrow age range). Young people are not excluded if they have co-morbid diagnoses such as anxiety, autism or attention deficit hyperactivity disorder (ADHD). Exclusion criteria include: a diagnosis of learning disability or significant head injury, neurological disorder or epilepsy; currently receiving another psychological intervention (including school counselling); levels of risk that would contraindicate imagery rescripting; and current diagnosis of bipolar disorder, post-traumatic stress disorder (PTSD) or psychosis.
Results
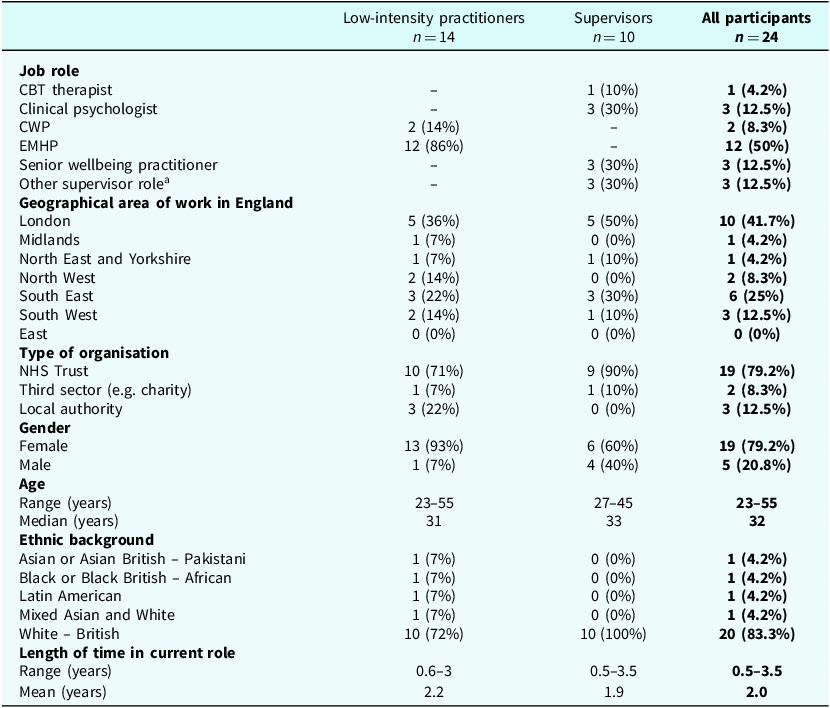
Twenty-four participants (14 low-intensity practitioners and 10 supervisors) were interviewed. Interviews lasted 30–78 minutes (mean = 44 minutes). Considering the overall sample (see Table 1), most participants were White British (83%), women (79%) and working in the NHS (79%). Participants reported that their team worked with a varying number of schools (range 1–70; median = 22). Supervisors had been working for varying lengths of time in roles supervising psychological practitioners (range 0.5–6 years; mean = 2.7 years).
Participant demographic information for low intensity practitioners and supervisors

a Three supervisors responded with more specific role titles in the demographic form, including: Mental Health Nurse & Supervising Practitioner; Mental Health Support Team Supervisor and Senior Practitioner, and Team Leader & CWP Supervisor.
Overview of themes
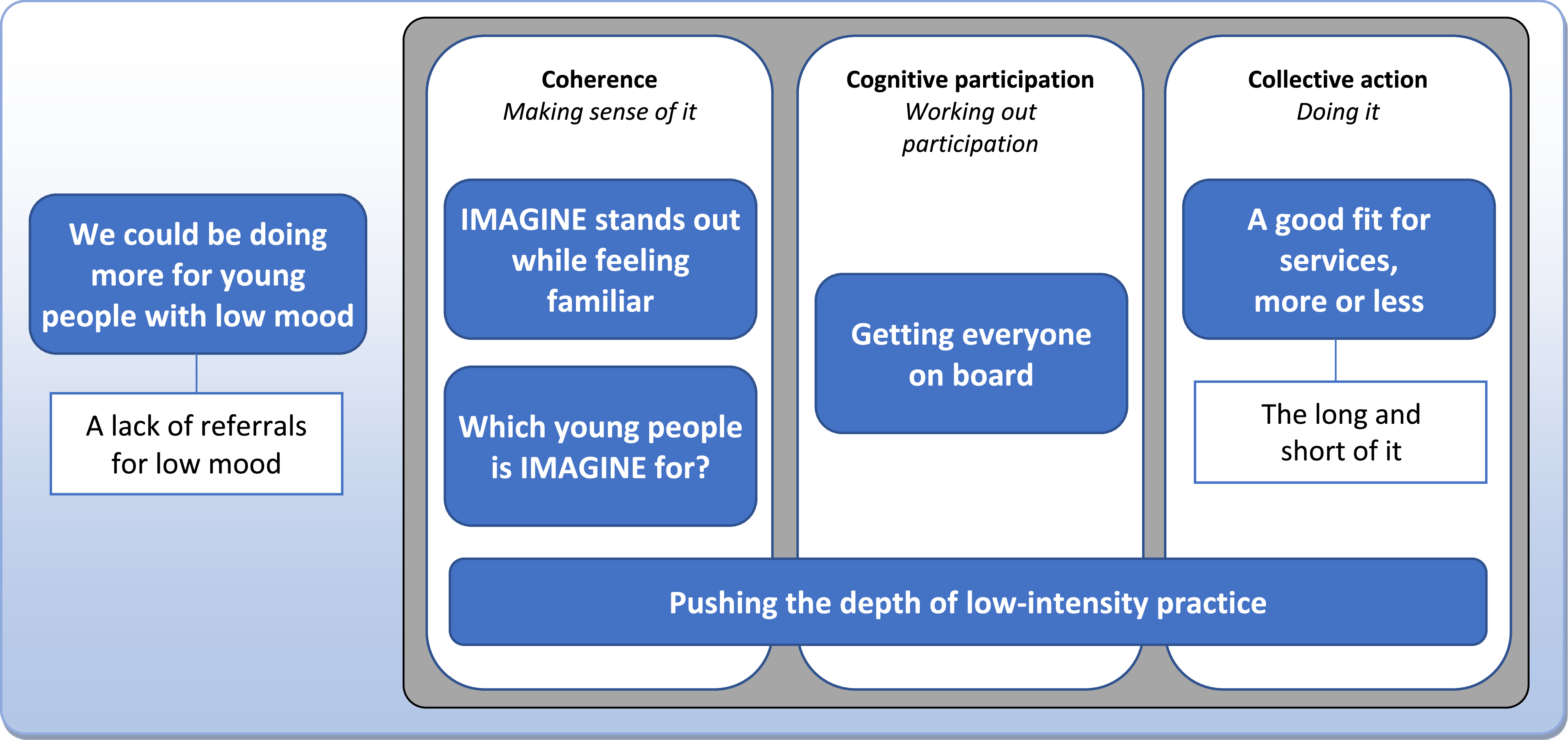
A thematic map is presented in Fig. 1. The thematic map is divided into context- and implementation-related themes, although these are considered to overlap and interact. A broad contextual factor was a sense among practitioners that services could be doing more to support young people with low mood and a desire to improve care, while also acknowledging a lack of appropriate referrals. Themes related to implementation were considered with reference to NPT. In relation to coherence (‘making sense of it’), practitioners differentiated IMAGINE from usual practice and responded positively to it, as well as trying to make sense of which young people it was for. In relation to cognitive participation (‘working out participation’), practitioners discussed the importance of getting buy-in from various stakeholders to support implementing IMAGINE. Regarding collective action (‘doing it’), practitioners described IMAGINE as a relatively good fit for practice, although they highlighted potential fit issues with the brief treatment course and longer session duration. One theme about IMAGINE seeming like a step-up for low-intensity practice, was conceptualised as cutting across NPT constructs.
Thematic map organised with reference to NPT constructs of coherence, cognitive participation, and collective action.

Contextual factors
-
1. We could be doing more for young people with low mood: ‘There’s a limit to the interventions that we currently offer’
Practitioners spoke about how their current interventions for low mood, primarily behavioural activation (BA) in a guided self-help format, are effective for many of the young people they see. Participants also noted its limitations, discussing who it may be less helpful for, including young people who are already engaging in activities but experiencing anhedonia. Obstacles to treating low mood were also noted, including motivational issues and a lack of support from young people’s systems (e.g. parents, carers). Participants also suggested low mood is harder to treat in young people compared with anxiety:
If there’s one part of that doesn’t buy into [BA], if school isn’t supportive or if home isn’t supportive, or if the young person doesn’t quite buy into it, then it’s not effective at all (low-intensity practitioner 11, North West, NHS)
[BA] hasn’t been as successful as the anxiety intervention, there are more drop-outs from low mood (low-intensity practitioner 9, West London, third sector)
Practitioners discussed how low mood can vary considerably in its presentation (e.g. anhedonia, reduced activity), precipitating factors (e.g. exam pressure, bullying), and co-occurring issues (e.g. anxiety, trauma), suggesting that this heterogeneity may warrant different approaches to treatment. Challenges supporting young people with low mood were also situated in a broader mental health context:
The term depression, low mood can be quite an umbrella term, particularly for adolescents, and there are a huge number of particularly kind of life experience and adjustments and transitional changes that can drastically contribute to mood […] young people might have really difficult home experiences or family mental health issues or y’know difficulties in terms of adverse experiences, trauma (supervisor 2, Southwest London, NHS)
We all know how difficult it is currently to be seen by CAMHS because they’re sort of oversubscribed (supervisor 3, South East, NHS)
Many participants spoke about how their services are always evolving to meet the needs of young people, including using existing materials with some adaptations for specific presentations (e.g. guided self-help for anger). Supervisors, in particular, highlighted their service’s involvement in research projects to keep up with new evidence. Almost all practitioners spoke about the need for alternative interventions for young people and highlighted the limited choice of interventions offered. Practitioners spoke about how increasing intervention choice could help services better meet the needs of young people:
[The leadership team] are keen to, you know, branch out, to kind of look at new interventions to make sure we’re staying up to date with the evidence base (supervisor 7, South East, NHS).
The more choice that we can give them, in terms of types of intervention, then the better […] there isn’t a lot of choice for them really, with low mood and depression at that age (low-intensity practitioner 14, South West, NHS)
1.1 A lack of referrals for low mood: ‘I’ve never had a low mood case’
While highlighting a gap in service provision for young people with low mood, practitioners almost universally highlighted that there were much fewer referrals for low mood, compared with anxiety:
We don’t have a huge amount of referrals for low mood (low-intensity practitioner 10, South East, Local authority)
The lack of referrals for low mood was not necessarily attributed to a lack of need. Participants spoke about how young people with low mood may be missed as they might not reach out for help or recognise that they may benefit from support. Some practitioners spoke about how school staff may not identify low mood due to the way it presents and the age of onset of low mood occurring when young people are more independent. Some participants discussed how more could be done to identify young people with low mood:
Something that needs to be worked on and improved is that obviously improving access and getting the young people in it who really need it. People who might be under the radar or they’re not speaking up (supervisor 9, Southeast London, NHS)
Coherence (making sense of it)
-
2. IMAGINE stands out while feeling familiar: ‘IMAGINE covers that base that behavioural activation doesn’t’
When presented with IMAGINE, most participants described it making a good first impression and being distinctive, but complementary, to usual practice. Participants described IMAGINE as exciting and innovative. The CBT-based, manualised approach to IMAGINE was recognisable to participants:
There is definitely something to this IMAGINE intervention and it feels it feels like it’s sort of tapping into the zeitgeist in terms of everything I know about where CBT is going (supervisor 3, South East, NHS)
I like that there’s a workbook that gives a description of every session because that’s very used to- how we work and then that makes it very clear for practitioners (low-intensity practitioner 4, West London, NHS)
While familiar in structure, IMAGINE was seen by many as quite different. Participants highlighted its focus on mental imagery and self-compassion. Practitioners spoke about the value of IMAGINE in including components to help update negative memories, develop positive images of the future, and cultivate self-compassion. Some participants described how IMAGINE may address gaps in service provision for young people with low mood:
In my clinical experience […] imagery can be really powerful (supervisor 2, Southwest London, NHS)
There is a part of me that kind of thinks ohh is there anything else [for treating depression]? That’s why when I saw this, my goodness, this looks amazing (low intensity practitioner 6, North West, local authority)
-
3. Which young people is IMAGINE for?: ‘It’s about finding young people it works for’
After watching the video describing IMAGINE, many participants asked specific questions about its eligibility criteria. In these moments, the first author identifies becoming aware of their outsider status in relation to not being involved in developing IMAGINE and welcomed their views on this based on their own experience. Practitioners said it would be important to consider young people’s trauma history as this could mean IMAGINE is not appropriate. Practitioners described mixed feelings on the 16- to 18-year-old age range. Some said this age range seemed appropriate, while others thought this may be too narrow as this age group are seen less in services, and it could be helpful for younger people. There was scepticism among some practitioners about whether there was sufficient demand for IMAGINE, given the relative lack of referrals for low mood and the 16–18 age group:
Inclusion, exclusion kind of indicators I think that would have to be quite clear, especially depending on levels of trauma (low-intensity practitioner 9, West London, third sector)
I don’t know if [the 16- to 18-year-old age range] would, maybe, you know, close it off to a lot of young people that could potentially benefit from it (low-intensity practitioner 8, South East, local authority)
Participants speculated about particular groups IMAGINE may benefit, with some suggesting it could be helpful for young people who have been bullied and those who struggle with negative thoughts or memories. Some participants discussed how IMAGINE may be particularly suitable for young people from different marginalised or disadvantaged backgrounds (e.g. looked after children, young people who have offended):
[A client] had some quite traumatic bullying experiences and is just really struggling to move on from that. And she’s the one where the thought challenging didn’t help at all and, you know, behavioural activation isn’t really right for her either … I think, yeah, for someone like her, [IMAGINE] could be really helpful (supervisor 7, South East, NHS)
[IMAGINE could be useful for] the kids not in education, employment or training or kind of the ones that maybe are kind of at more of the I would say exclusion front to kind of help them work towards a future plan (supervisor 5, Southeast London, third sector)
Participants questioned how appropriate IMAGINE would be for young people with neurodevelopmental difficulties. For example, they wondered whether young people with autism might struggle to use imagery or young people with ADHD might have issues with attention. Practitioners suggested that the suitability of IMAGINE for young people may be considered on a case-by-case basis and queried potential adaptations for these groups:
One of the difficulties with autism is being able to kind of use your imagination (low-intensity practitioner 5, Midlands, NHS)
Theme across NPT constructs
-
4. Pushing the depth of low-intensity practice: ‘This is asking [low-intensity practitioners] to access something a bit deeper, isn’t it?’
This theme cuts across different NPT constructs as it relates to specific ways participants differentiated IMAGINE from usual low-intensity practice and the potential implications of this for organising and allocating work to staff. Participants highlighted aspects of IMAGINE that suggested it felt like a step up from usual practice for practitioners. These differences included IMAGINE being more experiential, focusing more on cognition and the past, being more likely to bring up difficult emotions, and an increased potential for risk and trauma disclosures in discussing negative memories. The first author’s impression that these differences felt somewhat outside the remit of low intensity practice was informed by his experience of this type of work in an adult setting:
We’re very behavioural-based and this feels more cognitive-based (low-intensity practitioner 8, South East, local authority)
It could potentially lead to trauma disclosures and things that we don’t necessarily work with (low-intensity practitioner 9, West London, third sector)
While practitioners mostly said the skills required to deliver IMAGINE were similar to usual practice interventions (e.g. empathy, curiosity), practitioners thought it may require more creativity, ability to contain emotions, responsiveness in session, and skills in managing risk. Related to this, some felt IMAGINE sat somewhere between low-intensity and high-intensity work. One practitioner mentioned the senior wellbeing practitioner role potentially being well suited to delivering IMAGINE:
If someone brings up like a traumatic memory […] that would need to be really like thought about carefully and sensitively (supervisor 8, Southwest London, NHS)
It’s something yeah, almost that you would do if you were in the Band 6 kind of that middle position (supervisor 6, South East, NHS)
Although many participants suggested IMAGINE could be delivered by low-intensity practitioners, some reservations about this were raised, particularly among supervisors. Concerns included that delivering IMAGINE could be anxiety-provoking for practitioners and that senior leadership may think IMAGINE falls outside the scope of low-intensity work:
I went to something recently about low-intensity, and everyone was talking about how […] we want to develop the breadth of low-intensity work at the CYP level, not the depth […] based on you know what I’m looking at, [IMAGINE] feels more like depth (supervisor 3, South East, NHS)
Cognitive participation (working out participation)
-
5. Getting everyone on board: ‘This is the dream, isn’t it? That everyone’s on board’
Many participants spoke about being open to being involved in implementing IMAGINE. Participants spoke about the different people and groups that would be important to get involved in implementation initially, including practitioners, managers, and schools. Practitioners described a broadly top-down process where new interventions would filter down based on decisions made by senior leadership. Schools were seen as more involved in supporting referrals, rather than in making decisions about what interventions were taken up:
A lot of the other practitioners […] would love to be able to use something like this (low-intensity practitioner 8, South East, local authority)
The Band 7s and then our Band 8s as well who kind of oversee that would probably be in the actual deciding of whether it would be passed down to us (low-intensity practitioner 12, South West, NHS)
Practitioners spoke about how clear information about IMAGINE and evidence for its effectiveness, particularly in comparison with usual practice, would be important for services. Good-quality materials were also seen as important for buy-in. This includes having physical workbooks, and promotional materials for young people, parents, carers, and schools. The app used for homework was widely praised as practitioners felt it would increase accessibility and help overcome barriers to home practice tasks (e.g. paper being forgotten, lack of suitable mobile apps):
Something to really spark the service leads’ attention, “OK, this is something that we really need in our service” […] maybe some data for like the interventions we’re doing already and how maybe they’re not hitting (low-intensity practitioner 1, Southeast London, NHS)
Teenagers are on their phone 24/7, so let’s use that to our advantage? You know, go on your phone, but do your [therapy] homework please (low-intensity practitioner 7, South East, NHS)
Collective action (doing it)
-
6. A good fit for services, more or less: ‘It would be quite easy to … slot into the way that we work already’
In terms of the operational work related to training, resources, and intervention delivery, participants suggested IMAGINE would not differ too much from implementing other usual practice interventions. Participants broadly felt like IMAGINE was feasible and workable as part of their team’s offering and their role:
I think it would embed in quite well. I don’t think there would be any issues with it (supervisor 4, South West, NHS)
Participants spoke about how the format of training for IMAGINE could be similar to usual practice interventions. Supervisors discussed how it can be useful to have their own separate training and cases to use IMAGINE. Peer learning and supervision were highlighted as familiar ways practitioners get to grips with interventions that would support delivering IMAGINE:
I think the same training that you would do for the current manuals would be okay (low-intensity practitioner 3, Southwest London, NHS)
Whilst IMAGINE appeared to mostly be a good fit for services, many participants also suggested potential adaptations to reflect usual practice more closely. Participants queried whether IMAGINE could be merged into usual practice (e.g. first delivering BA and then IMAGINE), seemingly due to fears about not covering more behaviour-focused intervention components (e.g. emphasis on increasing meaningful activity) and potential resistance to change:
Would it be appropriate as a standalone intervention? Maybe feeling like it’s missing kind of the B (behaviour) and that maybe feels kind of important (supervisor 10, North East, NHS)
If there are practitioners that are so used to using BA, for example, having a new intervention probably might be a bit tricky to get used to (supervisor 4, South West, NHS).
6.1. The long and short of it: ‘It’s quite brief although it’s longer sessions’
A key fit issue raised by participants was the length of sessions and brief course of treatment. Many felt like the session length (up to 90 minutes) was too long for a school setting as this would require young people to miss two lessons and some raised that it may be difficult to find a confidential, physical space for that length of time. Participants suggested IMAGINE could be delivered over summer period or scheduled at the end of the day to minimise these issues:
We’d need to talk to schools by, you know, we’re gonna need a space. It’s gonna be for 90 minutes […] would that work in a school environment? (low-intensity practitioner 5, Midlands, NHS)
Practitioners also wondered whether the duration of treatment was sufficient to build a sufficient therapeutic alliance and address young people’s problems. Some suggested extending the treatment course to address these concerns and more closely reflect current practice:
It’s only a month, so … and you know, is that long enough to bring about change? (supervisor 1, Southeast London, NHS)
If it could be broken down into short- 45-minute sessions somehow that might be helpful (low-intensity practitioner 13, North East, NHS)
Discussion
This paper reports a pre-implementation study investigating psychological practitioners’ views about implementing IMAGINE in schools. Six themes were identified based on interviews that highlight a range of potential contextual and implementation barriers and enablers.
An overarching contextual theme related to a sense among practitioners that more could be done to support young people with low mood. This theme touched on many aspects of the mental health context for young people that have been highlighted in the literature, including: the heterogeneity of depression, routine practice interventions not being effective for everyone, long waiting lists for CAMHS and the pressure this puts on early intervention services, and the importance of offering young people more choice of interventions (Cliffe et al., Reference Cliffe, Peck, Shafique, Hards and Loades2023; Ellins et al., Reference Ellins, Hocking, Al-Haboubi, Newbould, Fenton, Daniel, Stockwell, Leach, Sidhu and Bousfield2023; Pile et al., Reference Pile, Herring, Bullard, Loades, Chan, Reynolds and Orchard2022). This suggests the importance of intervention innovation to offer more tailored support and more intervention choice. By contrast, a key barrier to implementing IMAGINE was the lack of referrals for low mood, particularly for the 16–18 age group. Given the evidence that depression is common and impairing for this age group, this is likely to be an issue with access and identification rather than lack of need. Many CAMHS services also do not accept referrals for those age 18 and the provision of services during this time is poor (Appleton et al., Reference Appleton, Elahi, Tuomainen, Canaway and Singh2021). More generally, a systematic review highlighted a range of barriers to children and young people seeking mental health support, including limited knowledge about where to access mental health support, a preference for not relying on others, and social stigma and embarrassment (Radez et al., Reference Radez, Reardon, Creswell, Lawrence, Evdoka-Burton and Waite2021).
The remaining themes were organised with reference to NPT and focus on implementation processes. Given that participants did not have hands-on experience of IMAGINE, it follows that many themes aligned with the ‘coherence’ construct (which relates to how staff make sense of innovations) as this has been conceived as a precursor to other NPT constructs that may be more relevant to later implementation stages (May et al., Reference May, Cummings, Girling, Bracher, Mair, May, Murray, Myall, Rapley and Finch2018). Factors related to this sense-making work included that it appeared to make a positive first impression, it shared qualities of low-intensity interventions that were familiar (e.g. brief, manualised, CBT-informed), and it was seen to have distinguishing features that practitioners saw as appealing or effective (i.e. imagery rescripting, cultivating self-compassion). Practitioners also highlighted how aspects of IMAGINE may make it more suitable for young people from marginalised groups as they may struggle with difficult memories and could benefit from work aimed at instilling hope for the future. Evidence suggests that marginalised groups (e.g. minoritised ethnic groups, LGBTQ + people) are more likely to develop depression and less likely to access support, thus it is important to consider how to improve access to interventions for these groups (Ahmad et al., Reference Ahmad, McManus, Cooper, Hatch and Das-Munshi2022; Moagi et al., Reference Moagi, van Der Wath, Jiyane and Rikhotso2021). In contrast, a potential barrier to implementing IMAGINE was the uncertainty practitioners had about IMAGINE being suited to young people with autism or ADHD. Interestingly, to our knowledge, there is no evidence to support these concerns. For example, Ozsivadjian et al. (Reference Ozsivadjian, Hollocks, Southcott, Absoud and Holmes2017) found no significant differences in the use of imagery in daily life between children with and without autism. Trauma was also highlighted as being outside the scope of low-intensity work. However, many young people experience trauma (e.g. estimate of 62% of US adolescents; McLaughlin et al., Reference McLaughlin, Koenen, Hill, Petukhova, Sampson, Zaslavsky and Kessler2013; Lawrence-Sidebottom et al., Reference Lawrence-Sidebottom, Huffman, Beam, Guerra, Parikh, Roots and Huberty2024) and will develop depression without meeting criteria for PTSD. Limited research exists examining whether traumatic experiences predict differential treatment outcomes in this population. One study comparing three treatments for adolescent depression (Waldron et al., Reference Waldron, Howard and Reinecke2019) found that all groups improved significantly regardless of trauma history, with no differences at long-term follow-up between those who had and had not experienced trauma (although those without trauma histories showed more rapid improvement in psychotherapy conditions). Whilst this suggests that trauma should not serve as an exclusion criterion for accessing support, more research is needed in low-intensity populations. This finding relates to the broader theme of needing clarity regarding the target population for novel interventions within this practitioner group. Enhanced workforce training, supervision, and clinical guidance would be beneficial to address concerns surrounding, including those with experiences of trauma and those with neurodivergent conditions.
The remit of low-intensity work is an area of debate, and this was highlighted in the results. For example, the extent to which IMAGINE may be considered a low-intensity intervention was highlighted. Whilst IMAGINE is brief, manualised, and CBT-informed; other aspects diverged from low-intensity interventions including its experiential nature, greater focus on cognition, and the potential that young people may disclose traumatic experiences. This uncertainty perhaps aligns with recognised challenges in retaining low-intensity practitioners in MHSTs linked to the role being characterised by high volume of work and frustration with the role being limited to delivering a limited range of interventions (Ellins et al., Reference Ellins, Hocking, Al-Haboubi, Newbould, Fenton, Daniel, Stockwell, Leach, Sidhu and Bousfield2023). Based on our findings, there appeared to be some discrepancy between the range of interventions low-intensity practitioner roles can offer, and the competing desires for clear specification and for this staff group to develop their clinical skills and broaden their skillset. Further research will be helpful to understand how best to resolve this discrepancy. There is also no reason to assume that IMAGINE is restricted to low-intensity delivery and so, if it demonstrated evidence of efficacy, further co-design and evaluation processes could helpfully evaluate its delivery in other contexts, by other practitioners and in different populations.
In terms of how people become engaged with an intervention (i.e. cognitive participation), practitioners indicated that an important process was getting everyone on board; including young people, parents, practitioners, and those deciding what interventions services offer. There was a sense that choosing interventions was largely a top-down process with minimal involvement from schools, young people, and carers. This appeared to reflect evaluation findings from the roll-out of MHSTs that reported limited involvement of these groups in the design and delivery of MHSTs (Ellins et al., Reference Ellins, Hocking, Al-Haboubi, Newbould, Fenton, Daniel, Stockwell, Leach, Sidhu and Bousfield2023).
The collective action construct in NPT highlights how, for novel interventions to be taken up by services, it is important that they are ‘workable’ and that resources (e.g. training, staffing) are allocated appropriately. Related to the workability of IMAGINE, a factor that may act as a barrier or enabler is the extent to which services may be able to adapt it to meet local needs. Intervention adaptability has been highlighted in past research as being a desirable quality in interventions (Roach et al., Reference Roach, Cullinan, Shafran, Heyman and Bennett2023); however, this may threaten intervention fidelity (i.e. the extent to which interventions are implemented as intended). Given that practitioners suggested changes to how IMAGINE may be delivered may indicate a resistance to change among practitioners. Reservations were also expressed about the effectiveness of IMAGINE given its brevity and its lack of focus on mechanisms targeted by usual practice interventions (i.e. meaningful activity). Our findings may indicate that practitioners’ reservations about the effectiveness of brief interventions may be an obstacle to these interventions being implemented. Finally, although much has been made of the potential for schools to enhance access to mental health support, our study highlights barriers that have been identified in previous research related to having sufficient time and space to deliver interventions in educational settings (Roach et al., Reference Roach, Cullinan, Shafran, Heyman and Bennett2023).
Strengths and weaknesses of the study
A potential strength of this study was that the lead researcher was not involved in developing IMAGINE; this positionality will have shaped the analytic process in that the lead researcher approached data collection and analysis without prior investment in IMAGINE and was less oriented toward presenting IMAGINE in a favourable light. Our recruitment strategy was a potential strength of this study, as we recruited a relatively diverse group of participants with regard to areas of England included. Although we do not claim that our results are generalisable, our findings may have captured some of the diversity of mental health provision across localities. Notably, all supervisors who were recruited were White British. Although this reflects unequal representation of minoritised ethnic groups in more senior positions in mental health services (Health and Social Care Information Centre, 2013), this may have influenced our results in not including supervisors who may have had their own experience of inequitable care regarding their ethnicity that may have informed their perspectives.
A potential weakness of our study was the focus on recruiting low-intensity practitioners. Interviewing other stakeholders (e.g. adolescents, parents, school staff, senior leadership) may also have broadened our analysis and highlighted factors that were not discussed by practitioners. However, we chose to focus on psychological practitioners given that these groups could be considered a ‘mid-point’ between intervention recipients (i.e. adolescents) and those deciding what interventions are offered. Another weakness is that we did not return the transcripts to participants for comment, and we did not ask participants to provide feedback on the findings. This would have been valuable to inform our analysis and would be of benefit to include in future research.
A further limitation is our use of the terms ‘low mood’ and ‘depression’ interchangeably. Whilst IMAGINE is an indicated intervention for elevated depressive symptoms (i.e. scoring above a clinical cut-off at two time points), the term ‘low mood’ is consistently used in the low-intensity approach and practitioners frequently use both terms synonymously. We therefore used both to align with current NHS low-intensity practice and reflect participant language. However, as highlighted by the above quotations, depression in this age group is highly heterogeneous and network analyses suggest various central symptoms (e.g. self-hatred, loneliness, sadness and pessimism; Mullarkey et al., Reference Mullarkey, Marchetti and Beevers2019). Whilst IMAGINE is likely to be transdiagnostic (i.e. it demonstrates clinical promise for reducing anxiety; Pile et al., Reference Pile, Smith, Leamy, Oliver, Bennett, Blackwell, Meiser-Stedman, Stringer, Dunn and Holmes2021), a service-level challenge emerges in identifying young people who present with depressive symptoms but may not experience or recognise ‘low mood’ as their primary concern. This is compounded by the fact that, due to stigma and time constraints, formal diagnostic assessments are often not appropriate.
Another limitation of our study was that practitioners were recruited without hands-on experience of delivering IMAGINE, as it was not feasible to recruit clinicians with direct delivery experience at this stage of intervention development. Hands-on experience of delivery would have supported consideration of specific barriers and enablers to implementation. We also recognise that recruiting participants who had not yet delivered IMAGINE in a real-world setting limited the extent to which NPT could be used to support data interpretation. Participants’ accounts were necessarily more speculative and less experience-based, which meant we focused on higher-level constructs to support interpretation, rather than considering more fine-grained NPT sub-constructs. However, there were also advantages to this approach. For example, our recruitment strategy did not require therapists to be involved in a trial evaluating IMAGINE. This meant that we could recruit participants from a more diverse range of contexts (e.g. varied geographical location, service size and type, including third sector and charities). Furthermore, given the stage of intervention evaluation, there are only a small number of therapists who have delivered IMAGINE, and so consistent with the purpose of the current study, were hoping to understand what future therapists might see as implementation barriers. Future work to evaluate IMAGINE in a phase IIB RCT (Pile et al., Reference Pile, Tinch-Taylor, Carter, Richardson, De Rijk, Leamy, Blackwell, Meiser-Stedman, Dunn, Byford, Holmes, Creswell and Smith2025) will include semi-structured interviews with trial therapists in a process evaluation.
Clinical and research implications, and future research
The relatively few referrals for low mood suggest that it is important to consider implementation strategies that target potential barriers to help-seeking (e.g. stigma) in advance. Novel interventions may also be enabled through having clear information about their suitability or adaptability for signs of neurodevelopmental conditions (e.g. difficulties with attention or imaginative thinking) and trauma. Multi-stakeholder involvement research has highlighted that removing professional terminology may increase intervention accessibility (Pile et al., Reference Pile, Herring, Bullard, Loades, Chan, Reynolds and Orchard2022). Given that practitioners were querying potential adaptations to IMAGINE may indicate that adapting interventions is commonplace in practice, although this presents challenges for ensuring interventions are delivered with fidelity. Recommendations in a review of intervention fidelity in trials have advised specifying core intervention components and acceptable adaptations in early stages of intervention development (Toomey et al., Reference Toomey, Hardeman, Hankonen, Byrne, McSharry, Matvienko-Sikar and Lorencatto2020). This may ensure that core, theoretically important intervention components remain intact while more peripheral components may be adapted by services to promote fit in their local contexts.
For IMAGINE, this research has resulted in several key modifications, primarily to the training protocol and future research directions. It emphasised elements requiring explicit attention in practitioner training (e.g. inclusion criteria, trauma, neurodiversity) and underscored the importance of system-level endorsement and the evidence needed to secure it. More broadly, it highlighted the mismatch between our methodology for identifying young people with depression (i.e. co-designed screening process that identifies significant need) and current service models that rely on self-referral with low rates. This finding has significant implications for policy development and advocacy efforts.
Conclusion
This study qualitatively explored practitioners’ and supervisors’ views about barriers and enablers to implementing a brief, novel, imagery-based intervention for adolescent depression in schools. Our findings highlight generally positive views among practitioners about IMAGINE and a sense that it could fit into usual practice. Potential obstacles raised were considerations about what young people may benefit from IMAGINE and uncertainty about where IMAGINE may sit in a stepped care model. The views of practitioners working in these settings can provide valuable insights into understanding the extent to which new, evidence-based interventions are likely to be translated into practice. Given the increased focus in the UK on increasing access to mental health support to adolescents in schools, this paper provides insights into key implementation and contextual factors that may influence the uptake of current and future interventions.
Key practice points
-
(1) At early stages of evaluating novel interventions, practitioners without hands-on experience of intervention delivery can provide valuable insights, based on their experience of providing psychological support, that can be used to prospectively consider how to overcome potential barriers and capitalise on potential enablers prior to later evaluation and implementation stages.
-
(2) Practitioners highlighted factors that may enable the implementation of a novel intervention for adolescent depression (IMAGINE) including that it: appeared to stand out positively (e.g. in targeting imagery processes), includes materials that may help with getting stakeholders onboard (e.g. a homework mobile application), and could be implemented in schools in a similar manner to usual practice interventions.
-
(3) Potential barriers to implementing IMAGINE included: practitioners’ sense that young people with neurodivergent conditions may struggle with imagery-based interventions (although this is not necessarily supported in the literature), a potential lack of fit in a school context due to the length of sessions, and uncertainty about whether IMAGINE could be delivered by low-intensity practitioners or if it fell outside their remit.
-
(4) In the context of psychological support for adolescent depression in schools in England, practitioners acknowledged that while current provision is limited, they also observed a lack of referrals for young people experiencing low mood.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1754470X26100609
Data availability statement
The authors confirm that the data that is available is included within the article. The full data transcripts are not available to ensure participants cannot be identified. This is consistent with our ethical procedures.
Acknowledgements
None.
Author contributions
Stephen A. McIntyre: Conceptualization (equal), Data curation (lead), Formal analysis (lead), Investigation (equal), Methodology (equal), Project administration (lead), Writing - original draft (lead), Writing - review & editing (equal); Jessica Richardson: Conceptualization (supporting), Data curation (supporting), Formal analysis (supporting), Investigation (equal), Methodology (supporting), Project administration (equal), Supervision (equal), Writing - review & editing (supporting); Patrick Smith: Conceptualization (supporting), Formal analysis (supporting), Investigation (supporting), Methodology (supporting), Project administration (supporting), Supervision (equal), Writing - review & editing (supporting); Victoria Pile: Conceptualization (equal), Formal analysis (supporting), Investigation (equal), Methodology (equal), Project administration (supporting), Supervision (lead), Writing - review & editing (lead).
Financial support
Dr Victoria Pile (Advanced Fellowship, NIHR301312) is funded by the NIHR for this research project. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR, NHS or the UK Department of Health and Social Care.
Competing interests
The authors declare no competing interests.
Ethical standards
Ethical approval for this study was granted by King’s College London’s Research Ethics Office (reference number: MRSP-21/22-26419). All participants provided written informed consent to participate in the study and for the results to be published. Ethical Principles of Psychologists and Code of Conduct, as set out by the BABCP and BPS, were adhered to. Participants were given £20 for their participation.



 Open access
Open access
Comments
No Comments have been published for this article.