

Introduction
Non-suicidal self-injury (NSSI) is defined as the deliberate destruction of one’s own body tissue without lethal intent (Nock, Reference Nock2010). It has been recognized as a serious public health problem across diverse populations, particularly among adolescents and individuals with mental disorders (Brown & Plener, Reference Brown and Plener2017; Denton & Álvarez, Reference Denton and Álvarez2024; Qu et al., Reference Qu, Wen, Liu, Zhang, He, Chen and Chen2023). In China, the lifetime prevalence of NSSI among youth reaches up to 24.7% (Qu et al., Reference Qu, Wen, Liu, Zhang, He, Chen and Chen2023). Within clinical populations, 6.8% of outpatients and 6.5% of inpatients meet the diagnostic criteria for NSSI disorder based on the proposed Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) criteria (Zhang et al., Reference Zhang, Ouyang, Liang, Wu, Bao, Yang and Wang2023). Due to the significant health and economic consequences associated with NSSI, there is an urgent need for effective interventions (Ribeiro et al., Reference Ribeiro, Franklin, Fox, Bentley, Kleiman, Chang and Nock2016; Wilkinson, Reference Wilkinson2013).
Previous research on NSSI has predominantly focused on behaviors, while the ideation of NSSI has received less attention. NSSI thoughts, which may occur independently of actual behaviors, have a prevalence equal to or higher than behaviors (Nock, Reference Nock2010; Robinson, Garisch, & Wilson, Reference Robinson, Garisch and Wilson2021). Among inpatient adolescents, lifetime rates reach 78% for NSSI thoughts and 72% for NSSI behaviors (Millon et al., Reference Millon, Alqueza, Kamath, Marsh, Pagliaccio, Blumberg and Auerbach2024). Notably, empirical findings indicated that approximately 9.6% of adolescents report NSSI thoughts in the absence of corresponding behaviors, and this subgroup demonstrated significantly higher risks of suicidal ideation and attempts compared to adolescents with no history of NSSI (Robinson et al., Reference Robinson, Garisch and Wilson2021). Given the distress caused by NSSI thoughts and their strong association with behaviors, the present study assessed both NSSI thoughts and behaviors to further understand the therapeutic effects of DBT-ST across these dimensions (Robinson et al., Reference Robinson, Garisch and Wilson2021; Voss et al., Reference Voss, Hoyer, Venz, Pieper and Beesdo‐Baum2020).
Psychotherapy is the primary treatment for NSSI, and dialectical behavior therapy (DBT) has substantial evidence supporting its effectiveness (Brown & Plener, Reference Brown and Plener2017; Hawton, Saunders, & O’Connor, Reference Hawton, Saunders and O’Connor2012). Standard DBT, which includes individual therapy, group skills training, between-session telephone coaching, and a therapist consultation team, has been proven effective in treating NSSI (Linehan et al., Reference Linehan, Korslund, Harned, Gallop, Lungu, Neacsiu and Murray-Gregory2015). However, due to its intensity and the shortage of trained clinicians, standard DBT can be difficult to access (McMain et al., Reference McMain, Guimond, Barnhart, Habinski and Streiner2017). As a stand-alone treatment, DBT skills training (DBT-ST) is currently being implemented in various settings, with its effectiveness garnering increasing interest (Neacsiu et al., Reference Neacsiu, Eberle, Kramer, Wiesmann and Linehan2014; Soler et al., Reference Soler, Pascual, Tiana, CebriA, Barrachina, Campins and PErez2009). Studies have revealed the effectiveness of DBT-ST in treating borderline symptoms (Heerebrand et al., Reference Heerebrand, Bray, Ulbrich, Roberts and Edwards2021), suicidal or NSSI episodes (McMain et al., Reference McMain, Guimond, Barnhart, Habinski and Streiner2017), and general psychiatric symptoms (Valentine et al., Reference Valentine, Bankoff, Poulin, Reidler and Pantalone2015), demonstrating its feasibility and effectiveness in clinical practice. However, as NSSI is a transdiagnostic risk factor, existing literature on DBT-ST for NSSI has mainly focused on samples with borderline personality disorder (BPD) (Heerebrand et al., Reference Heerebrand, Bray, Ulbrich, Roberts and Edwards2021; McMain et al., Reference McMain, Guimond, Barnhart, Habinski and Streiner2017; Soler et al., Reference Soler, Pascual, Tiana, CebriA, Barrachina, Campins and PErez2009), underscoring the need for more research across diverse mental disorders.
Theoretical models and empirical research indicate that emotion dysregulation is the core mechanism underlying NSSI, regardless of cultural context (Hasking, Whitlock, Voon, & Rose, Reference Hasking, Whitlock, Voon and Rose2017; He et al., Reference He, Chen, Fan, Sun, Yang, Liu and Wang2025; Wolff et al., Reference Wolff, Thompson, Thomas, Nesi, Bettis, Ransford and Liu2019; Yates, Reference Yates2004). Furthermore, the cultural tendency toward emotional restraint and suppression in China may increase the likelihood of individuals adopting concealed coping strategies like NSSI when facing distress (Song, Chan, & Ryan, Reference Song, Chan and Ryan2024). Based on the biosocial theory, DBT posits that various dysfunctional behaviors (e.g., suicide attempts, NSSI, substance use) stem from emotion dysregulation, and therefore focuses centrally on improving emotion regulation skills (Wilks, Korslund, Harned, & Linehan, Reference Wilks, Korslund, Harned and Linehan2016). Research further supports that emotion regulation is a key mechanism through which DBT achieves its therapeutic effects (Asarnow et al., Reference Asarnow, Berk, Bedics, Adrian, Gallop, Cohen and McCauley2021). This offers a theoretical rationale for the proposal that DBT-ST can improve emotion regulation and reduce dysfunctional behaviors in various cultural contexts. However, most studies on the effectiveness of DBT have been conducted in American and European contexts, leaving its applicability in Asian, particularly Chinese populations, underexplored (Loo et al., Reference Loo, Keng, Ramírez‐Espinosa, Nor Hadi, Ramírez‐Gutiérrez and Shoesmith2021). Emerging evidence supports the feasibility of implementing DBT across diverse cultural contexts. A pilot study conducted in Taiwan found that one year of DBT significantly reduced suicidal behaviors and overall symptoms in patients with BPD (Chang et al., Reference Chang, Liu, Korslund, Lin, Lin, Huang and Wu2022). Similarly, another study that integrated Zhong-Yong thinking (a Chinese form of dialectical thinking) into DBT for college students indicated that the culturally adapted intervention produced superior long-term improvements in outcomes such as anxiety and other symptoms compared to the control group (Yang et al., Reference Yang, Liu, Wang, Chen, Chen, Yang and Zhang2020). Moreover, the flexibility of DBT delivery has been extended to digital formats, as demonstrated by a four-week online group training that significantly alleviated depression and anxiety among medical students during the normalized phase of the COVID-19 pandemic control (Liang et al., Reference Liang, Feng, Zheng, Wu, Zhang and Li2021). In other Asian countries, such as Malaysia, a 14-week intervention study for Muslim patients with BPD confirmed that DBT-ST significantly alleviated core symptoms (Keng et al., Reference Keng, Mohd Salleh Sahimi, Chan, Woon, Eu, Sim and Wong2021). Despite this compelling theoretical rationale and existing adaptations, the implementation of DBT-ST in China remains at an early stage, and robust nationwide multi-center research evaluating its effectiveness for clinical populations with NSSI is still lacking.
The objective of this study was to examine the effectiveness of DBT-ST for NSSI in a nationwide multi-center Chinese clinical sample. Specifically, this study aimed to evaluate its impact on the frequency of NSSI thoughts and behaviors, clinical symptoms, and psychological functioning. We hypothesized that DBT-ST will be more effective than social support group therapy (SSGT) in reducing the frequency of NSSI thoughts and behaviors, alleviating clinical symptoms, and promoting psychological functioning.
Methods
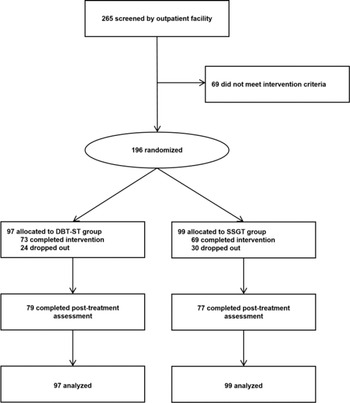
This single-blind, randomized clinical trial was conducted at 12 sites across China between September 2019 and January 2020 (see Supplementary Methods S1 and S2 for details). The trial was registered with ClinicalTrials.gov (NCT04094623). Written informed consent was obtained from all participants following a complete explanation of the study. For those participants who were younger than 18 years, the signature from a parent or guardian was also required on the informed consent. This study was approved by the Ethics Committees of The Affiliated Brain Hospital of Nanjing Medical University (2019-KY043-01). The participant flow is presented in Figure 1.
Participant flowchart.
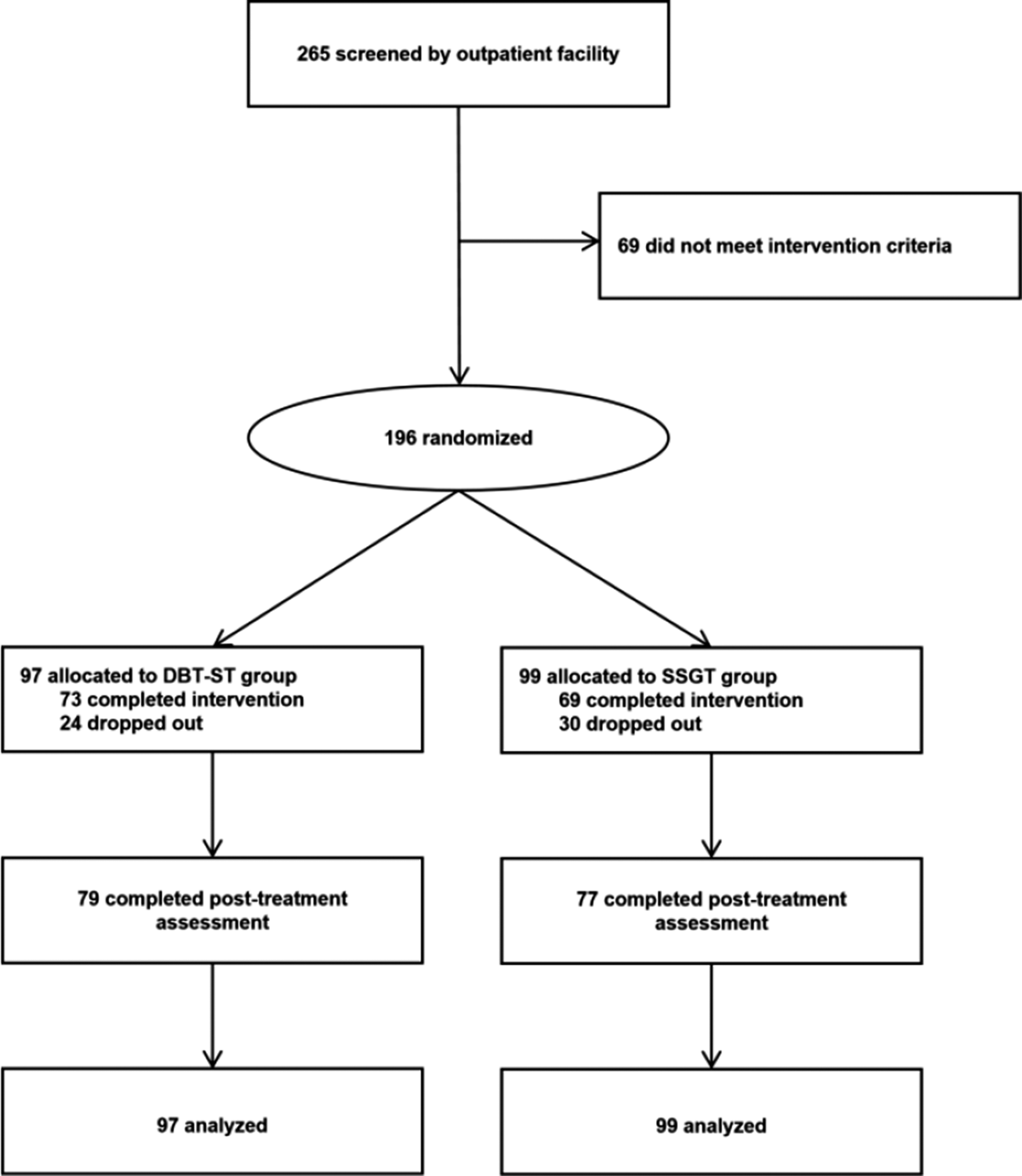
Figure 1. Long description
At the top, 265 screened by outpatient facility. An arrow leads right to 69 did not meet intervention criteria, and down to 196 randomized. This splits into two branches. Left branch: 97 allocated to D B T dash S T group, 73 completed intervention, 24 dropped out. Downward arrow to 79 completed post-treatment assessment, then to 97 analyzed. Right branch: 99 allocated to S S G T group, 69 completed intervention, 30 dropped out. Downward arrow to 77 completed post-treatment assessment, then to 99 analyzed. All boxes are connected by arrows indicating participant flow.
Participants enrolment and randomization
Participants were recruited via outpatient services. Psychiatrists and trained investigators evaluated these participants with inclusion and exclusion criteria for intervention. Inclusion criteria were as follows: (a) meeting the DSM-5 diagnostic criteria for one or more mental disorders; (b) meeting the DSM-5 diagnostic criteria for NSSI; (c) 10–59 years of age; (d) able to understand written and spoken Chinese. Exclusion criteria were as follows: (a) having a serious neurological disease; (b) having a serious physical disease; (c) pregnant or breast-feeding women; (d) life-threatening suicidal plans or attempts within one month, (e) severe aggressive behaviors, mania episode, substance dependence or abuse, (f) other severe psychopathology or physical illness requiring immediate inpatient treatment. Participants were randomly assigned to treatment groups using simple randomization, performed by an independent statistician with a computer-generated random number table in SPSS 22.0.
Treatment
Both interventions, DBT-ST and SSGT, comprised 13-week sessions, each lasting 120 minutes. Participants did not receive any other individual or group psychotherapy during the study. Dropout criteria were as follows: (a) missing four or more consecutive treatment sessions, (b) experiencing severe psychological crisis (e.g., suicide attempts, aggressive behavior toward others, or other acute risk incidents) that, following therapist assessment, were judged to necessitate interventions such as hospitalization; (c) voluntary withdrawal from the intervention (for adolescents, guardian consent was also required for withdrawal). Prior to the first group session, all participants attended an individual interview. During this interview, a psychotherapist reconfirmed the inclusion criteria, established an individual profile, cultivated motivation, and obtained the participant’s commitment to the treatment process. As part of this process, the participant was required to sign a Non-Suicidal Agreement as a safety commitment.
Dialectical behavior therapy skills training (DBT-ST)
The DBT-ST intervention was adapted from Marsha Linehan’s standard manual (Linehan, Reference Linehan1993), incorporating the operational procedures as adapted by Soler et al. (Reference Soler, Pascual, Tiana, CebriA, Barrachina, Campins and PErez2009). To ensure consistency across all research sites, a unified set of materials (including therapist manual, patient manual, and homework manual) was developed. The intervention covered four core skill modules: mindfulness, distress tolerance, emotion regulation, and interpersonal effectiveness. Each weekly session followed a structured format: a brief mindfulness exercise, review of the previous week’s homework, instruction in new skills, and assignment of homework for the coming week (see Methods S3 and S4 for details).
Social support group therapy (SSGT)
The SSGT group was designed to provide a relational experience, with the primary therapeutic technique being peer support. Therapists mainly served as facilitators in group interactions, enabling participants to discuss their difficulties.
Therapist training and quality control
At each center, both DBT-ST and SSGT were delivered by the same group leader and co-therapist. Throughout the intervention, weekly online group supervision was held. Both DBT-ST and SSGT supervision sessions followed an identical structure, each involving a review of prior challenges followed by a preview and demonstration of the upcoming protocol, in accordance with their respective manual. Furthermore, with consent from all participants, each therapy session at every center was audio-recorded. The leading research team conducted random checks of these recordings. Regular research quality control meetings were held in addition to clinical supervision. Further details regarding therapist training and supervision can be found in the Supplementary Materials (Methods S5).
Assessments
Assessments were conducted at baseline (before treatment) and post-treatment (13 weeks) by independent assessors who were blinded to group assignment.
The primary outcome was assessed by the Ottawa Self-Injury Inventory (OSI) (Nixon et al., Reference Nixon, Levesque, Preyde, Vanderkooy and Cloutier2015). This instrument has been culturally adapted and validated for use in China (Zhang, Cheng, Xiao, & Liu, Reference Zhang, Cheng, Xiao and Liu2015) and is frequently employed in intervention research (Cheng et al., Reference Cheng, Zhao, Song, Han, Liu, Chen and Han2024; Yin et al., Reference Yin, Zhang, Yu, Shi and Yu2025). The Chinese version of the OSI consists of 28 items and assesses multiple features of NSSI, including the frequency of NSSI thoughts and behaviors, functions, methods, locations, and addictive features. For the purpose of the current study, we used the items assessing the frequency of NSSI thoughts and the frequency of NSSI behaviors over the past month.
Secondary outcomes included suicidal ideation and attempts assessed by a self-designed questionnaire, depression assessed by the 24-item Hamilton Depression Rating Scale (HAMD) (Hamilton, Reference Hamilton1960), borderline symptoms assessed by Borderline Symptom List-23 (BSL-23) (Bohus et al., Reference Bohus, Kleindienst, Limberger, Stieglitz, Domsalla, Chapman and Wolf2009), emotion dysregulation assessed by the 36-item Difficulties in Emotion Regulation Scale (DERS-36) (Gratz & Roemer, Reference Gratz and Roemer2004), impulsivity assessed by the Barratt Impulsiveness Scale (BIS) (Patton, Stanford, & Barratt, Reference Patton, Stanford and Barratt1995), alexithymia assessed by the 26-item Toronto Alexithymia Scale (TAS-26) (Taylor, Ryan, & Bagby, Reference Taylor, Ryan and Bagby1985), mindfulness assessed by the Mindful Attention Awareness Scale (MAAS) (Brown & Ryan, Reference Brown and Ryan2003), psychological resilience assessed by the Connor-Davidson Resilience Scale (CD-RISC) (Connor & Davidson, Reference Connor and Davidson2003), and emotional intelligence assessed by the Wong and Law Emotional Intelligence Scale (WLEIS) (Wong & Law, Reference Wong and Law2002). A detailed description of the assessments for secondary outcomes can be found in the Supplementary Methods S6.
Statistical analysis
An a priori sample size calculation was performed using G*Power 3.1. For a mixed-design (within-between) interaction, with a significance level (α) of 0.05 and 80% power to detect a medium effect size (Cohen’s f = 0.25), a total of 128 participants completing the study were required. To account for anticipated attrition rates of 20–30% based on prior studies of DBT (Dixon & Linardon, Reference Dixon and Linardon2020; McMain et al., Reference McMain, Guimond, Barnhart, Habinski and Streiner2017; Soler et al., Reference Soler, Pascual, Tiana, CebriA, Barrachina, Campins and PErez2009), the initial recruitment target was set at 182 participants (91 per group).
Analyses were conducted on an intention-to-treat (ITT) basis. Baseline demographic and clinical characteristics were compared using the chi-square test or Fisher’s exact test for categorical variables, and independent samples t-tests for continuous variables. Attrition rates were compared between groups using the chi-square test, and reasons for attrition were summarized using descriptive statistics.
Independent-samples t tests were performed in secondary analyses to compare baseline outcome scores between the DBT-ST and SSGT groups. Treatment effects were analyzed using hierarchical linear modeling (HLM). The models specified time (baseline, post-treatment) as a within-subject variable, group (DBT-ST, SSGT) as a between-subjects variable, and their interaction (time × group), while controlling for baseline scores as covariates. Simple slope tests were conducted if a significant interaction effect was found, to further explore the trend of changes in both groups. Treatment condition was coded with SSGT = −0.5 and DBT-ST = 0.5. Effect sizes (Cohen’s d) were computed as a standardized measure of the treatment effect (Bergeron et al., Reference Bergeron, Vaillancourt-Morel, Corsini-Munt, Steben, Delisle, Mayrand and Rosen2021; Feingold, Reference Feingold2009). Then, we conducted a one-way analysis of variance (ANOVA) to explore differences in treatment outcomes across participants with different primary diagnoses following DBT-ST treatment. Due to the variety of diagnoses and the relatively small sample sizes in some diagnostic groups, we categorized the participants into four groups for the analysis: depression disorder, BPD, bipolar disorder, and other disorders (including missing diagnoses).
Missing data accounted for 1.2% of observations at baseline and 21.9% post-treatment. This was largely due to participant attrition, with a smaller proportion attributable to occasional item non-response on certain scales. Little’s MCAR test indicated that the data were missing completely at random. Therefore, multiple imputation was deemed an appropriate method for handling missing data. Multiple imputation based on averaging 50 iterative Markov-Chain Monte Carlo imputations was conducted to complete the missing data (Austin, White, Lee, & Van Buuren, Reference Austin, White, Lee and Van Buuren2021). A sensitivity analysis was performed using complete case analysis to assess the robustness of the findings (the results are available in Supplementary Tables S3–S5). Data analysis were carried out by R.
Results
Participants and treatment adherence
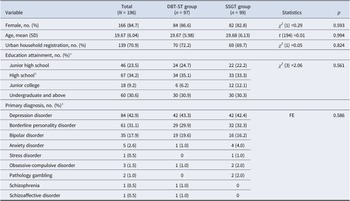
One hundred and ninety-six participants were recruited in the intervention, with 97 participants randomized to the DBT-ST group and 99 participants randomized to the SSGT group (Table 1). There were no significant differences between the two groups in terms of demographic and clinical characteristics at baseline. Overall, 54 of the 196 (27.6%) participants withdrew, with no significant difference between the DBT-ST and SSGT groups (DBT-ST: 24 [24.7%] of 97; SSGT: 30 [30.3%] of 99; p = 0.477). The reasons for dropout are as follows: missing four or more consecutive treatment sessions (DBT-ST: 3, 12.5%; SSGT: 7, 23.3%), hospitalization (DBT-ST: 1, 4.2%; SSGT: 0, 0.0%), feeling improved (DBT-ST: 2, 8.3%; SSGT: 1, 3.3%), work/school commitments (DBT-ST: 2, 8.3%; SSGT: 2, 6.7%), lack of time (DBT-ST: 5, 20.8%; SSGT: 5, 16.7%), distant location from hospital (DBT-ST: 2, 8.3%; SSGT: 5, 16.7%), and perceiving the treatment as unsuitable (DBT-ST: 9, 37.5%; SSGT: 10, 33.3%).
Demographics and clinical characteristics
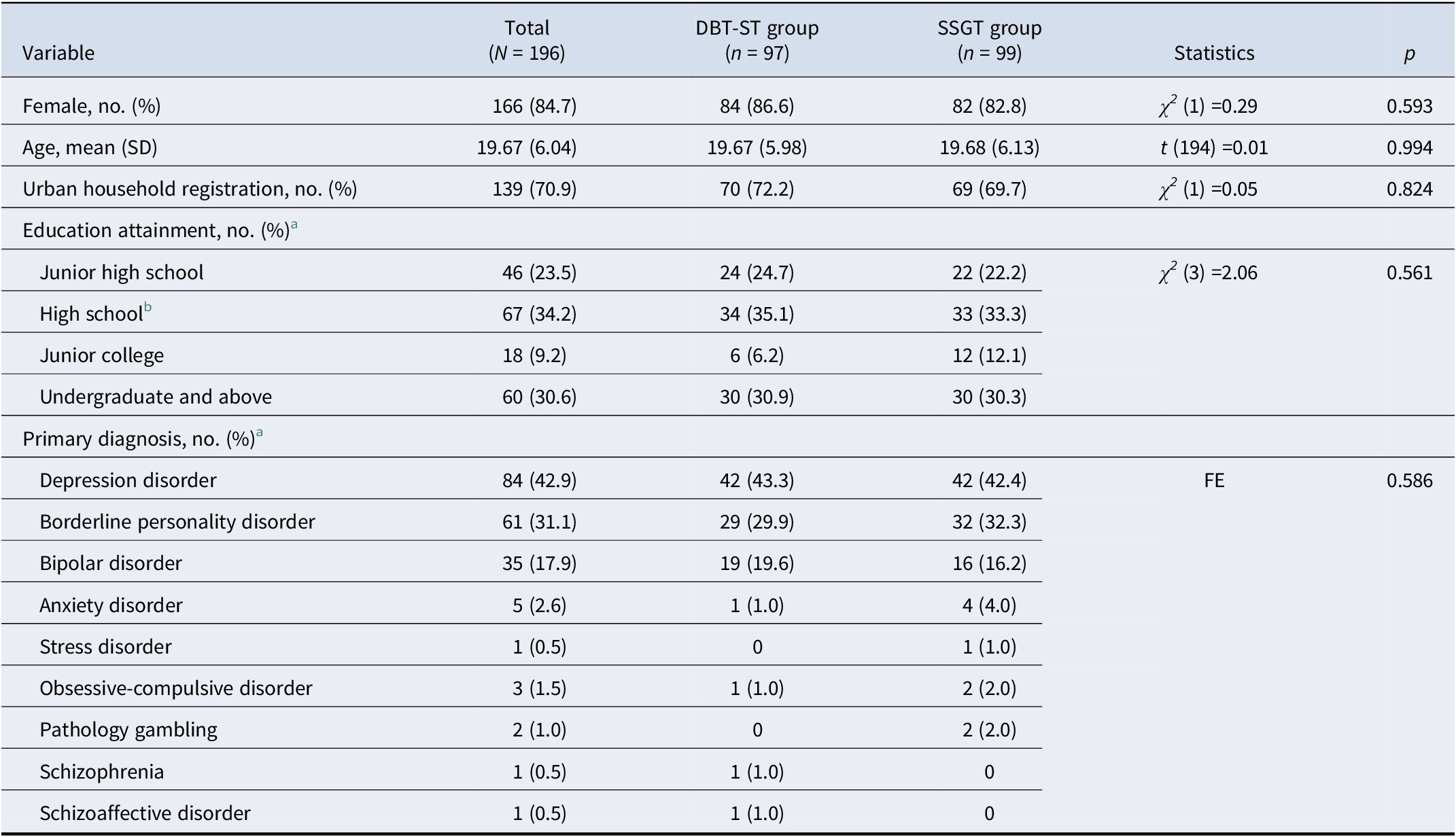
Table 1. Long description
Starting from the top, columns are Variable, Total (N equals 196), D B T dash S T group (n equals 97), S S G T group (n equals 99), Statistics, and p. For Female, number and percent: Total 166 (84.7), D B T dash S T 84 (86.6), S S G T 82 (82.8), chi-squared (1) equals 0.29, p equals 0.593. For Age, mean (S D): Total 19.67 (6.04), D B T dash S T 19.67 (5.98), S S G T 19.68 (6.13), t (194) equals 0.01, p equals 0.994. Urban household registration: Total 139 (70.9), D B T dash S T 70 (72.2), S S G T 69 (69.7), chi-squared (1) equals 0.05, p equals 0.824. Education attainment (data incomplete): Junior high school, Total 46 (23.5), D B T dash S T 24 (24.7), S S G T 22 (22.2); High school, Total 67 (34.2), D B T dash S T 34 (35.1), S S G T 33 (33.3); Junior college, Total 18 (9.2), D B T dash S T 6 (6.2), S S G T 12 (12.1); Undergraduate and above, Total 60 (30.6), D B T dash S T 30 (30.9), S S G T 30 (30.3); chi-squared (3) equals 2.06, p equals 0.561. Primary diagnosis (data incomplete): Depression disorder, Total 84 (42.9), D B T dash S T 42 (43.3), S S G T 42 (42.4); Borderline personality disorder, Total 61 (31.1), D B T dash S T 29 (29.9), S S G T 32 (32.3); Bipolar disorder, Total 35 (17.9), D B T dash S T 19 (19.6), S S G T 16 (16.2); Anxiety disorder, Total 5 (2.6), D B T dash S T 1 (1.0), S S G T 4 (4.0); Stress disorder, Total 1 (0.5), D B T dash S T 0, S S G T 1 (1.0); Obsessive-compulsive disorder, Total 3 (1.5), D B T dash S T 1 (1.0), S S G T 2 (2.0); Pathology gambling, Total 2 (1.0), D B T dash S T 0, S S G T 2 (2.0); Schizophrenia, Total 1 (0.5), D B T dash S T 1 (1.0), S S G T 0; Schizoaffective disorder, Total 1 (0.5), D B T dash S T 1 (1.0), S S G T 0. Statistics for diagnoses: F E, p equals 0.586. Footnotes: a, data incomplete for these categories; b, high school includes technical secondary school, senior high school, and higher vocational educational school.
a Data were incomplete for these categories.
b High school includes technical secondary school, senior high school and higher vocational educational school.
Outcome analyses
Descriptive statistics for outcomes at baseline and post-treatment are presented in Supplementary Table S1. At baseline, no significant differences were observed between the DBT-ST and SSGT groups across all outcomes. The results of the treatment effect analysis based on the complete case analysis are consistent with the findings that follow.
Primary outcomes
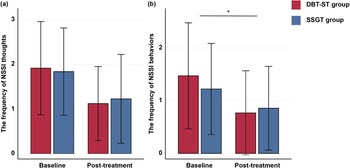
As shown in Figure 2 and Table 2, the frequency of NSSI thoughts decreased significantly in both the DBT-ST and SSGT groups from baseline to post-treatment (b = −0.70; 95% CI −0.89, −0.51; p < 0.001), with no significant main effect of group and no significant time × group interaction. There was a significant time × group interaction for the frequency of NSSI behaviors (b = −0.34; 95% CI -0.63, −0.05; p = 0.020). Simple slope tests showed that the DBT-ST group had a greater reduction in the frequency of NSSI behaviors from baseline to post-treatment compared to the SSGT group (Cohen’s d = 0.74 versus 0.38). There were no significant differences at post-treatment for the frequency of NSSI thoughts and behaviors (Supplementary Table S1).
Comparison between participants receiving DBT-ST and SSGT in (a) the frequency of NSSI thoughts and (b) the frequency of NSSI behaviors.
Note: Both groups demonstrated significant reductions in the frequency of NSSI thoughts and behaviors, with the DBT-ST group showing a greater reduction in NSSI behaviors compared to the SSGT group. Error bars represent standard deviation. * p < 0.05.
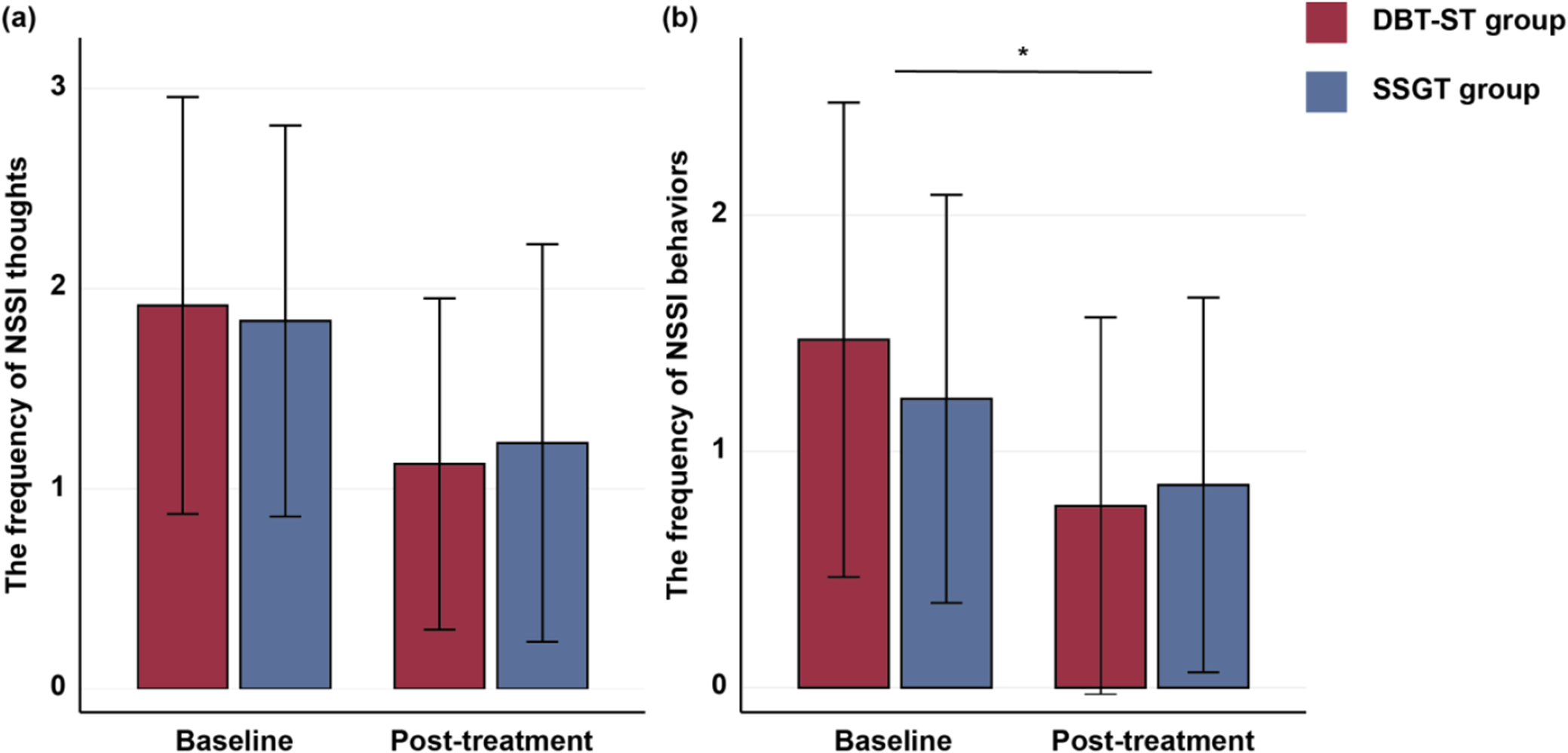
Figure 2. Long description
Top-left panel labeled a shows the frequency of N S S I thoughts on the y-axis and baseline versus post-treatment on the x-axis. Light gray bars represent D B T dash S T group and dark gray bars represent S S G T group. Both groups decrease from baseline to post-treatment. Top-right panel labeled b shows the frequency of N S S I behaviors with the same group colors and axes. Both groups decrease, but the reduction is greater for D B T dash S T. An asterisk and horizontal line above the bars indicate statistical significance. Bottom-left and bottom-right panels repeat the same data with D B T dash S T in red and S S G T in blue. Legends on the right clarify group colors. Error bars indicate variability. All panels show reductions from baseline to post-treatment, with the largest decrease in N S S I behaviors for D B T dash S T.
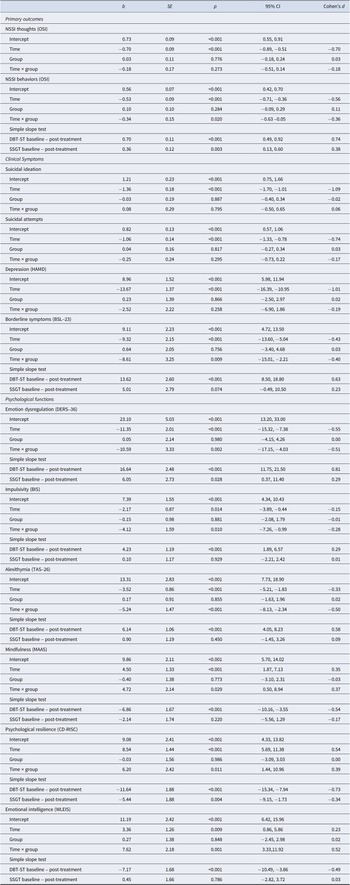
Results of the main effect of group and time, and the interaction effects for all outcomes
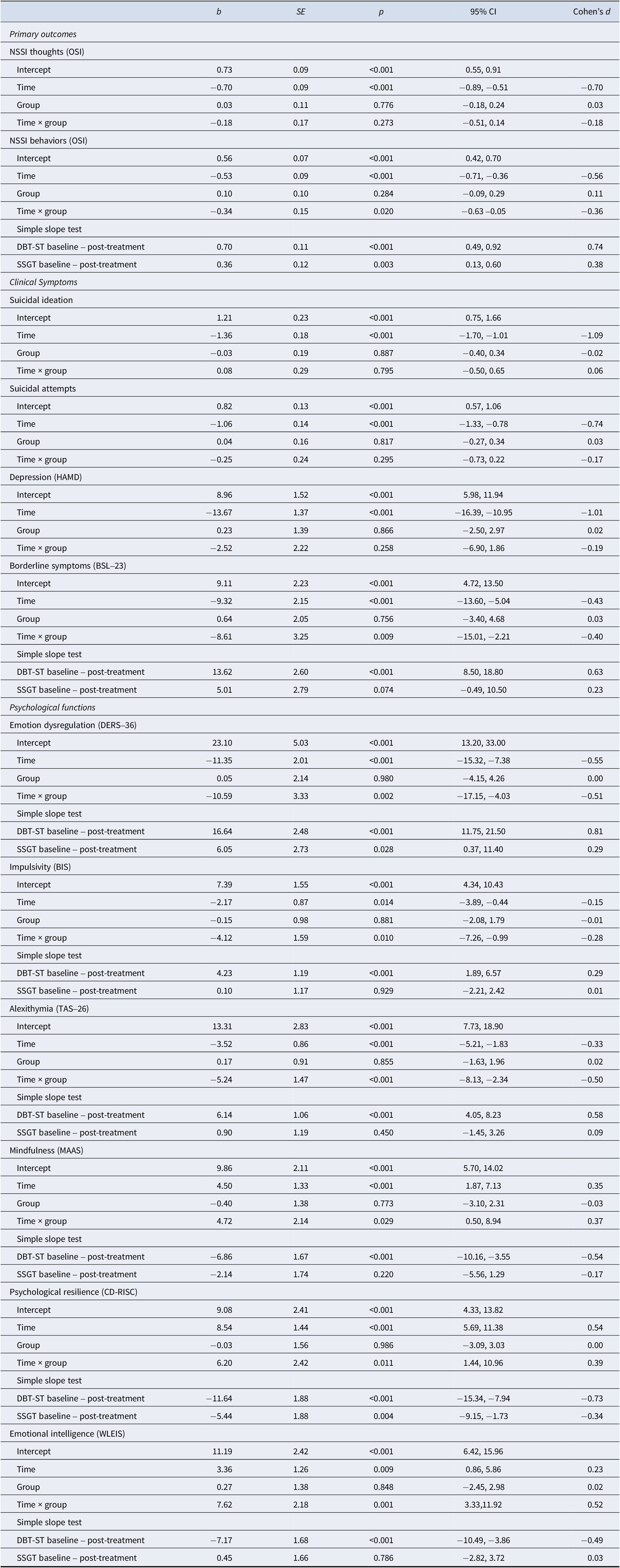
Table 2. Long description
From the top, the table is divided into three main sections: Primary outcomes, Clinical symptoms, and Psychological functions. Each section lists outcomes in bold, with rows for Intercept, Time, Group, and Time by Group effects. For each row, columns display b (coefficient), S E (standard error), p (p-value), 95 percent confidence interval, and Cohen's d (effect size). Significant negative time effects are observed for N S S I thoughts (b = minus 0.70, S E = 0.09, p less than 0.001, 95 percent C I minus 0.89 to minus 0.51, d = minus 0.70), N S S I behaviors (b = minus 0.53, S E = 0.09, p less than 0.001, 95 percent C I minus 0.71 to minus 0.36, d = minus 0.56), suicidal ideation (b = minus 1.36, S E = 0.18, p less than 0.001, 95 percent C I minus 1.70 to minus 1.01, d = minus 1.09), suicidal attempts (b = minus 1.06, S E = 0.14, p less than 0.001, 95 percent C I minus 1.33 to minus 0.78, d = minus 0.74), depression (b = minus 13.67, S E = 1.37, p less than 0.001, 95 percent C I minus 16.39 to minus 10.95, d = minus 1.01), borderline symptoms (b = minus 9.32, S E = 2.15, p less than 0.001, 95 percent C I minus 13.60 to minus 5.04, d = minus 0.43), emotion dysregulation (b = minus 11.35, S E = 2.01, p less than 0.001, 95 percent C I minus 15.32 to minus 7.38, d = minus 0.55), impulsivity (b = minus 2.17, S E = 0.87, p = 0.014, 95 percent C I minus 3.89 to minus 0.44, d = minus 0.15), and alexithymia (b = minus 3.52, S E = 0.86, p less than 0.001, 95 percent C I minus 5.21 to minus 1.83, d = minus 0.33). Mindfulness, resilience, and emotional intelligence show significant positive time effects. Group effects are non-significant throughout. Time by group interactions are significant for N S S I behaviors, borderline symptoms, emotion dysregulation, impulsivity, mindfulness, resilience, and emotional intelligence, with effect sizes ranging from d = 0.23 to d = 0.81. Simple slope tests compare D B T dash S T and S S G T from baseline to post-treatment, with D B T dash S T generally showing larger effect sizes. All abbreviations are defined in the table footnote.
Note: OSI, Ottawa Self-Injury Inventory; HAMD, Hamilton Depression Scale; BSL-23, Borderline Symptom List-23; DERS-36, 36-item Difficulties in Emotion Regulation Scale; BIS, Barratt Impulsiveness Scale; TAS-26, 26-item Toronto Alexithymia Scale; MAAS, Mindful Attention Awareness Scale; CD-RISC, Connor-Davidson Resilience Scale; WLEIS, Wong and Law Emotional Intelligence Scale.
Secondary outcomes
Clinical symptoms
Suicidal ideation (b = −1.36; 95% CI −1.70, −1.01; p < 0.001), suicidal attempts (b = −1.06; 95% CI -1.33, −0.78; p < 0.001), depression (b = −13.67; 95% CI -16.39, −10.95; p < 0.001) decreased significantly from baseline to post-treatment in both groups, while there were no main effect of group and no significant time × group interaction for these outcomes. There was a significant time × group interaction for borderline symptoms (b = −8.61; 95% CI -15.01, −2.21; p = 0.009). Simple slope tests showed that the DBT-ST group had a greater reduction in borderline symptoms from baseline to post-treatment compared to the SSGT group (Cohen’s d = 0.63 versus 0.23). There were no significant differences at post-treatment for suicidal ideation and attempts, depression, or borderline symptoms (Supplementary Table S1).
Psychological functioning
There was a significant time × group interaction for emotion dysregulation (b = −10.59; 95% CI -17.15, −4.03; p = 0.002, impulsivity (b = −4.12; 95% CI -7.26, −0.99; p = 0.010), alexithymia (b = −5.24; 95% CI -8.13, −2.34; p < 0.001), mindfulness (b = 4.72; 95% CI 0.50, 8.94; p = 0.029), psychological resilience (b = 6.20; 95% CI 1.44, 10.96; p = 0.011) and emotion intelligence (b = 7.62; 95% CI 3.33, 11.92; p < 0.001). Simple slope tests showed that the DBT-ST group had greater reductions in all of these outcomes compared to the SSGT group (see Table 2 for details). At post-treatment, the DBT-ST group showed lower scores than the SSGT group on emotion dysregulation (t = 3.01, Cohen’s d = 0.43, p = 0.003), impulsivity (t = 2.41, Cohen’s d = 0.34, p = 0.017), and alexithymia (t = 2.61, Cohen’s d = 0.38, p = 0.010), and higher scores on psychological resilience (t = −2.25, Cohen’s d = −0.32, p = 0.026), and emotional intelligence (t = −3.96, Cohen’s d = −0.56, p < 0.001) (Supplementary Table S1).
The one-way ANOVA revealed no significant differences in score changes across outcomes between patients with different primary diagnoses after receiving DBT-ST (Supplementary Table S2).
Discussion
This study examined the effectiveness of a 13-week DBT-ST intervention in a clinical sample of individuals with NSSI in China. To the best of our knowledge, this is the first nationwide multi-center clinical study of DBT-ST conducted in the Chinese context. Our findings revealed that the DBT-ST and SSGT groups had comparable dropout rates following the intervention. The DBT-ST group showed improvements across all outcomes, including the frequency of NSSI thoughts and behaviors, clinical symptoms and psychological functioning, with significant superiority over SSGT in the frequency of NSSI behaviors, borderline symptoms, emotion dysregulation, impulsivity, alexithymia, mindfulness, psychological resilience, and emotional intelligence. These findings highlight the effectiveness of DBT-ST as a stand-alone treatment for NSSI.
In our study, the attrition rate in the DBT-ST group was similar to rates reported in prior studies (e.g., 24%, Soler et al., Reference Soler, Pascual, Tiana, CebriA, Barrachina, Campins and PErez2009; 39%, Linehan et al., Reference Linehan, Korslund, Harned, Gallop, Lungu, Neacsiu and Murray-Gregory2015; 28%, McMain et al., Reference McMain, Guimond, Barnhart, Habinski and Streiner2017; 28%, Dixon & Linardon, Reference Dixon and Linardon2020), providing preliminary evidence for the cross-cultural implementation feasibility of this intervention. Nevertheless, the DBT-ST group did not demonstrate a significantly lower dropout rate compared to the SSGT group. The absence of a significant between-group difference may be explained by the use of an active control rather than a waitlist or treatment-as-usual condition, which likely enhanced retention in the control group. This finding aligns with evidence from other active-control studies, in which DBT-ST showed no statistically significant advantage in reducing dropout (Asarnow et al., Reference Asarnow, Berk, Bedics, Adrian, Gallop, Cohen and McCauley2021). Future research could explore specific factors influencing treatment adherence to support clinicians in matching patients with interventions they are more likely to sustain. Additionally, data on dropout reasons indicated that most dropouts were due to external factors, such as time constraints, academic/work requirements, and geographical distance, which is consistent with commonly reported barriers in DBT interventions (Dixon & Linardon, Reference Dixon and Linardon2020). This trend highlights the adherence challenges posed by the fast-paced lifestyle and contextual pressures in China. Some participants also reported the treatment as unsuitable, which may relate to the intervention content, the structured format, or a preference for individual therapy. Notably, a similar proportion of dropouts in the SSGT group reported this reason, suggesting that it is not unique to the DBT-ST intervention content. The attrition rate was comparable to that of similar studies and largely driven by external factors, implying the preliminary feasibility and acceptability of DBT-ST in China.
After a 13-week intervention, both the DBT-ST and SSGT groups showed significant reductions in the frequency of NSSI thoughts and behaviors, with the DBT-ST group reporting a significantly sharper decline in the frequency of NSSI behaviors compared to the SSGT group. This superior reduction in NSSI behaviors is consistent with prior research indicating that both standard DBT and DBT-ST yield better outcomes for NSSI episodes than control groups (McMain et al., Reference McMain, Guimond, Barnhart, Habinski and Streiner2017, Reference McMain, Links, Gnam, Guimond, Cardish, Korman and Streiner2009; Mehlum et al., Reference Mehlum, Tørmoen, Ramberg, Haga, Diep, Laberg and Grøholt2014). In contrast to our hypotheses, we did not observe DBT-ST to be superior to SSGT in reducing the frequency of NSSI thoughts. One explanation is that our assessment focused solely on frequency, while prior evidence suggests DBT may primarily reduce the intensity rather than the frequency of NSSI thoughts (Rizvi & Fitzpatrick, Reference Rizvi and Fitzpatrick2021). Additionally, NSSI thoughts are implicit and subjective. Along with potential recall bias or difficulties in identification among some patients, this may have affected the accuracy of the assessment.
The results showed that the DBT-ST group experienced a greater reduction in borderline symptoms compared to the SSGT group, while both groups had reductions in suicidal ideation, suicidal attempts, and depression. DBT was originally developed to treat BPD by helping patients regulate emotions and reduce problematic behaviors (Keefe et al., Reference Keefe, Kim, DeRubeis, Streiner, Links and McMain2021; Linehan et al., Reference Linehan, Korslund, Harned, Gallop, Lungu, Neacsiu and Murray-Gregory2015; Stiglmayr et al., Reference Stiglmayr, Stecher-Mohr, Wagner, Meiβner, Spretz, Steffens and Renneberg2014). Although participants in this study were not exclusively diagnosed with BPD, the results indicate that DBT-ST is still effective in reducing borderline symptoms within the Chinese context. This may be attributed to the fact that DBT skills target several core manifestations of borderline symptoms, including emotion dysregulation, impulsivity, and negative self-concept, which are also commonly observed in other mental disorders (Crowell, Beauchaine, & Linehan, Reference Crowell, Beauchaine and Linehan2009; Valentine et al., Reference Valentine, Bankoff, Poulin, Reidler and Pantalone2015). Therefore, these skills help participants improve in these domains, leading to a reduction in overall borderline symptoms. However, both groups showed a distinct decline in suicidal ideation, suicidal attempts, and depression, with no significant difference between the DBT-ST and SSGT groups. The failure to find superiority of DBT-ST in these outcomes may be due to the short-term format of the intervention, which provided inadequate time for the internalization and proficient application of skills required for greater improvement. Furthermore, both interventions incorporate common therapeutic elements, such as a supportive environment and opportunities for emotional expression. These nonspecific factors may help alleviate emotional distress in both intervention groups, thereby potentially contributing to improvement in suicidal ideation and attempts, as well as depressive symptoms.
Regarding psychological functioning, the findings indicated that DBT-ST was associated with greater reductions in emotion dysregulation, impulsivity, and alexithymia, as well as greater improvements in mindfulness, psychological resilience, and emotional intelligence compared to the SSGT group. These findings provide further supporting evidence that DBT-ST offers a broader range of psychological benefits, which are consistent with prior research demonstrating the effectiveness of standard DBT and DBT-ST in improving psychological well-being (Heath, Midkiff, Gerhart, & Turow, Reference Heath, Midkiff, Gerhart and Turow2021; Soler et al., Reference Soler, Pascual, Tiana, CebriA, Barrachina, Campins and PErez2009). DBT-ST cultivates a set of core skills that can be generalized and applied across diverse life situations, which in turn helps individuals improve multiple domains of psychological functioning (Feigenbaum, Reference Feigenbaum2010). The improvement in these psychological functions can also be understood through the lens of the Chinese cultural context. For instance, the dialectical approach central to DBT resonates with the Zhong–Yong concept in Confucianism, which may help participants more naturally integrate acceptance and change (Gao et al., Reference Gao, Huang, Yao, Liu, Zhou, Zhang and Mo2022). Furthermore, employing localized case examples aids participants in applying skills to daily life, thereby fostering change more effectively. Therefore, the skills taught in DBT-ST can help patients with heterogeneous mental disorders acquire relevant coping strategies and improve their psychological functioning across a wide range of dimensions.
No significant differences were found in the effectiveness of DBT-ST across patients with heterogeneous mental disorders in our study. DBT-ST is highly adaptable across diverse diagnostic settings and effective in treating transdiagnostic conditions (Heath et al., Reference Heath, Midkiff, Gerhart and Turow2021). Previous research suggests that transdiagnostic frameworks enhance recruitment and foster valuable learning and interaction among patients with different diagnoses (Durpoix, Lachaux, Weiner, & Weibel, Reference Durpoix, Lachaux, Weiner and Weibel2023). Our study offers corroborating evidence for the application of DBT-ST in treating NSSI among patients with heterogeneous mental disorders in clinical practice. It should be noted that due to the limited sample sizes in each subgroup, the results should be interpreted cautiously.
Several limitations of this study should be noted. First, our findings primarily relied on self-report measures, which are susceptible to response biases. Second, the assessment of NSSI focused on the frequency of thoughts and behaviors, without capturing other multidimensional characteristics such as intensity or duration, which may limit the generalizability of the findings. Third, the 13-week intervention and the two-assessment time-point design limit conclusions regarding the long-term maintenance of treatment effectiveness. Fourth, the finding of no significant differential effect of DBT-ST across disorders requires cautious interpretation, as it is preliminary and may be statistically underpowered. To address these limitations and deepen understanding of DBT-ST for NSSI, future research should incorporate multimethod assessments and measure the multifaceted features of NSSI thoughts and behaviors (e.g., intensity, duration). Furthermore, extending the follow‑up period and including multiple assessment time points would help assess long‑term effectiveness. Finally, a larger and more diverse sample is required to examine the effects of DBT‑ST across different diagnostic groups and to strengthen the conclusions.
Conclusions
Our study provides evidence that 13-week DBT-ST is a promising intervention for NSSI thoughts and behaviors, with positive effects on clinical symptoms and psychological functioning in patients with heterogeneous mental disorders. Further study is required before drawing definitive conclusions as to the long-term effectiveness of DBT-ST intervention.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/S0033291726104553.
Data availability statement
The data analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgements
We would like to thank Prof. Martin Bohus, Dr. Nikolaus Kleindienst and Dr. Ruben Vonderlin from Heidelberg University for reviewing the manuscript and providing valuable suggestions for its revision.
Author contribution
Data analysis was performed by F.M. and M.L., with C.W., P.Z. and D.Y. assisting in data collation. F.M., S.C. and M.L. drafted the original manuscript, while F.M. and S.C. were responsible for revising and refining it. M.R., J.G., Z.R. provided supervision for the clinical interventions. The interventions were conducted and data collected by C.Y., J.L., Y.L., Y.S., X.L., G.Y., X.M., X.L., H.L., Z.W., S.H. C.W. reviewed, edited and critically revised the paper. All authors approved the final paper.
Funding statement
The trial was funded by Jiangsu Provincial key research and development program (BE2019609), National Natural Science Foundation of China (82371556), Jiangsu Provincial Double-Innovation Doctor Program (JSSCBS20221917), and Science and Technology Development Foundation of Nanjing Medical University (NMUB20220126).
Competing interests
The authors declare none.



 Open access
Open access