



Impact Statements
This QES consolidates evidence on barriers and facilitators of school-based mental health help-seeking among adolescents in SSA, where a high burden of MHPs has been reported. Although schools are positioned as cost-effective entry points for support, the findings indicate that service presence alone does not translate into utilisation. Adolescents interpret help-seeking through the relational, cultural and institutional conditions within which services are embedded. The synthesis identifies the interconnected structural and individual factors that shape poor help-seeking. Adolescents’ concerns centre on mistrust, weak rapport and prior negative experiences with providers. Social and contextual influences included perceived stigma, gender norms, low mental health literacy, limited accessibility to care, parental/familial authority and expectations, peer influence and reliance on informal or spiritual support systems. Across studies, adolescents assess disclosure risks, including fear of judgement, confidentiality breaches and social consequences, before engaging with formal services. Help-seeking is socially constructed and largely dependent on experienced and perceived relational safety rather than individual unwillingness to seek help. Interventions that prioritise awareness without addressing trust, confidentiality and institutional credibility are unlikely to improve uptake. School systems should operate as context-sensitive platforms that incorporate confidentiality protocols, trust-building strategies, clearly defined roles within school systems and active family and community involvement at each stage of support, aligned with cultural contexts. For policymakers, the QES supports a shift from service provision metrics to standards that assess relational safety, cultural context and accountability within school-based systems. For researchers, this review highlights the limited qualitative evidence and underrepresentation of adolescents’ perspectives, requiring context-sensitive research that centres lived experiences to inform intervention design.
Introduction
Mental health problems (MHPs), such as depression and anxiety, account for a sizeable proportion of the global disease burden among adolescents, with up to 14% of 10- to 19-year-olds affected worldwide (Jessiman et al., Reference Jessiman, Kidger, Spencer, Geijer-Simpson, Kaluzeviciute, Burn, Leonard and Limmer2022; Amone-P’Olak et al., Reference Amone-P’Olak, Kakinda, Kibedi and Omech2023; Akın and Sarrar, Reference Akın and Sarrar2024; Cosma et al., Reference Cosma, Black, Vuckovic, Pavic, Fonseca and Lazzerini2025). Despite this high prevalence, many adolescents do not access either professional help or informal support. This is particularly pronounced in Sub-Saharan Africa (SSA), where health systems are under-resourced, MH services are sparse and stigma remains widespread (Babatunde et al., Reference Babatunde, van Rensburg, Bhana and Petersen2021; Al Omari et al., Reference Al Omari, Khalaf, Al Sabei, Al Hashmi, Al Qadire, Joseph and Damra2022; Barrow and Thomas, Reference Barrow and Thomas2022).
While adolescence is a critical period for the emergence of MHPs, it also represents an important window for early intervention and the commencement of long-term MH promotion (Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021; Al Omari et al., Reference Al Omari, Khalaf, Al Sabei, Al Hashmi, Al Qadire, Joseph and Damra2022; Birrell et al., Reference Birrell, Grummitt, Smout, Maulik, Teesson and Newton2025). Most school-going adolescents in SSA cannot access formal MH care (Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021; Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023). This disconnect has been highlighted (Al Omari et al., Reference Al Omari, Khalaf, Al Sabei, Al Hashmi, Al Qadire, Joseph and Damra2022; O’Neill et al., Reference O’Neill, Stapley, Rehman and Humphrey2023), prompting concerns among researchers and practitioners regarding untreated MHPs (Mutahi et al., Reference Mutahi, Larsen, Cuijpers, Peterson, Unutzer, McKay, John-Stewart, Jewell, Kinuthia, Gohar, Lai, Wamalwa, Gachuno and Kumar2022; Hayes et al., Reference Hayes, Mansfield, Mason, Santos, Moore, Boehnke, Ashworth, Moltrecht, Humphrey, Stallard, Patalay and Deighton2024; Nguyen et al., Reference Nguyen, Conway, Murphy, Brady and Hennessy2025). Adolescents who do not receive prompt support for emerging MHPs are more likely to face academic disruption, social exclusion, early parenthood, exposure to violence and enduring psychiatric conditions in adulthood (Abdulsalam et al., Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023; Al-Shannaq and Aldalaykeh, Reference Al-Shannaq and Aldalaykeh2023). The implications of low help-seeking therefore extend beyond immediate emotional or behavioural problems to include long-term psychological disorders, impaired social and academic functioning and increased public health burdens (Seedaket et al., Reference Seedaket, Turnbull, Phajan and Wanchai2020; Lu et al., Reference Lu, Todhunter-Reid, Mitsdarffer, Muñoz-Laboy, Yoon and Xu2021; Radez et al., Reference Radez, Reardon, Creswell, Lawrence, Evdoka-Burton and Waite2021).
Help-seeking for MHPs refers to the adaptive coping process through which individuals recognise the need for support and engage with formal or informal sources of help (Rickwood et al., Reference Rickwood, Deane, Wilson and Ciarrochi2005). Barriers to help-seeking processes are multifaceted, including intrapersonal factors such as self-stigma and low mental health literacy (MHL), including limited knowledge, misconceptions and awareness of available support (Aguirre Velasco et al., Reference Aguirre Velasco, Cruz, Billings, Jimenez and Rowe2020; Barrow and Thomas, Reference Barrow and Thomas2022), interpersonal constraints such as poor social support or negative family attitudes and structural barriers such as cost, distance and lack of accessible services (Gulliver et al., Reference Gulliver, Griffiths and Christensen2010; Eigenhuis et al., Reference Eigenhuis, Waumans, Muntingh, Westerman, van Meijel, Batelaan and van Balkom2021). In contrast, facilitators of help-seeking may include the presence of trusted adults, integration of MHL programmes into the school curriculum, prior positive experiences with help-seeking and culturally appropriate MH messages (Aguirre Velasco et al., Reference Aguirre Velasco, Cruz, Billings, Jimenez and Rowe2020; Bach et al., Reference Bach, Bich and Anh2023). Although several systematic reviews have explored these themes, most have synthesised data from mixed populations of adolescents or focused exclusively on those with diagnosed conditions rather than considering school-going adolescents as a discrete subgroup (Aguirre Velasco et al., Reference Aguirre Velasco, Cruz, Billings, Jimenez and Rowe2020; Radez et al., Reference Radez, Reardon, Creswell, Lawrence, Evdoka-Burton and Waite2021; Barrow and Thomas, Reference Barrow and Thomas2022).
Recognising these long-term consequences, the World Mental Health Report (2022) (Freeman, Reference Freeman2022) and the Mental Health Action Plan (2013–2030) (Singh, Reference Singh2021) have highlighted school-based interventions as potentially cost-effective entry points for introducing support for MH (Singh, Reference Singh2021; Freeman, Reference Freeman2022; World Health Organization, 2022). In many high-income countries, schools and institutions have become central to early intervention efforts (Duong et al., Reference Duong, Bruns, Lee, Cox, Coifman, Mayworm and Lyon2021; Ma et al., Reference Ma, A-M and Anderson2023; McPhail et al., Reference McPhail, Thornicroft and Gronholm2024). A recent systematic review by Hayes et al. (Reference Hayes, Mansfield, Mason, Santos, Moore, Boehnke, Ashworth, Moltrecht, Humphrey, Stallard, Patalay and Deighton2024) evaluated universal school-based interventions and found tentative yet promising impacts on adolescents’ help-seeking attitudes and intentions, especially through intrapersonal pathways, such as MHL and stigma reduction. However, the review also pointed to numerous limitations, including methodological variations, limited long-term follow-up and a lack of contextual tailoring for most interventions (Hayes et al., Reference Hayes, Mansfield, Mason, Santos, Moore, Boehnke, Ashworth, Moltrecht, Humphrey, Stallard, Patalay and Deighton2024).
These limitations are especially pronounced in SSA, where schools often lack key foundational elements, such as embedded MH infrastructure and trained professionals (Jörns-Presentati et al., Reference Jörns-Presentati, Napp, Dessauvagie, Stein, Jonker, Breet, Charles, Swart, Lahti, Suliman, Jansen, van den, Seedat and Groen2021; Mabrouk et al., Reference Mabrouk, Mbithi, Chongwo, Too, Sarki, Namuguzi, Atukwatse, Ssewanyana and Abubakar2022). In addition, understanding help-seeking among adolescents in school settings remains limited (Meza et al., Reference Meza, Kiche, Soi, Khairuzzaman, Nales, Whetten, Wasonga, Amanya and Dorsey2020; Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023). These limitations underscore the need for contextually grounded research that explores how help-seeking within school environments is described and discussed in SSA. To date, existing research has predominantly addressed systemic health system limitations, but insufficient attention has been paid to the cultural, individual, institutional or context-specific factors that shape adolescents’ help-seeking behaviours (Meza et al., Reference Meza, Kiche, Soi, Khairuzzaman, Nales, Whetten, Wasonga, Amanya and Dorsey2020; Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021; Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021).
In SSA, where increasing attention is being paid to adolescents’ MH needs, less is known about school-going adolescents’ perspectives on MH experiences and their help-seeking negotiations within the school and sociocultural contexts. Existing research has largely focused on adolescent help-seeking pathways and constraints within health systems, often overlooking school-going adolescents’ perspectives regarding formal and informal support systems within SSA. To address this gap, the present qualitative evidence synthesis (QES) aimed to review and integrate findings from existing studies examining barriers and facilitators associated with MH help-seeking behaviours among school-going adolescents in SSA. In this review, MH help-seeking included formal sources such as school-based counselling and clinical services, as well as informal support systems, including family, peers and community networks. The review was guided by the following question: What barriers and facilitators influence MH help-seeking behaviours among school-going adolescents in SSA?
Methods
Review design
Our review of the barriers and facilitators of MH help-seeking behaviours among school-going adolescents in SSA adopted a QES approach. We opted to restrict the review to qualitative studies to provide a rich context for lived experiences, beliefs and attitudes, particularly concerning sensitive topics such as MH help-seeking behaviours (Flemming and Noyes, Reference Flemming and Noyes2021; Carmona et al., Reference Carmona, Baxter and Carroll2022). This enabled the review to explore societal and cultural factors and personal experiences or interactions that shape relevant behaviours in this setting (Long et al., Reference Long, French and Brooks2020; Flemming and Noyes, Reference Flemming and Noyes2021).
This review followed the Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) guidelines (Tong et al., Reference Tong, Flemming, McInnes, Oliver and Craig2012; Batten and Brackett, Reference Batten and Brackett2022) (see Supplementary Appendix A). The GRADE-CERQual approach (Lewin et al., Reference Lewin, Glenton, Munthe-Kaas, Carlsen, Colvin, Gülmezoglu, Noyes, Booth, Garside and Rashidian2015, Reference Lewin, Booth, Glenton, Munthe-Kaas, Rashidian, Wainwright, Bohren, Tunçalp, Colvin, Garside, Carlsen, Langlois and Noyes2018) was also used to determine the confidence level of each finding (see Supplementary Appendix D). A PRISMA flow diagram (Page et al., Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann, Mulrow, Shamseer, Tetzlaff, Akl, Brennan, Chou, Glanville, Grimshaw, Hróbjartsson, Lalu, Li, Loder, Mayo-Wilson, McDonald, McGuinness, Stewart, Thomas, Tricco, Welch, Whiting and Moher2021; Haddaway et al., Reference Haddaway, Page, Pritchard and McGuinness2022) is included to provide transparency in the reporting of the search and scrutiny processes (Carmona et al., Reference Carmona, Baxter and Carroll2022; Akl et al., Reference Akl, Khabsa, Iannizzi, Piechotta, Kahale, Barker, McKenzie, Page and Skoetz2024).
Framing the question (SPIDER framework)
To specify the review question, we used the SPIDER tool (sample, phenomenon of interest, design, evaluation and research type) (Cooke et al., Reference Cooke, Smith and Booth2012) to develop a list of search terms (Table 1).
Application of the SPIDER tool to the review questions

Table 1. Long description
The table consists of two columns: Element and Details.
* Sample S: School-going adolescents aged 10 to 19 years residing in Sub-Saharan Africa.
* Phenomenon of interest P I: Perceived barriers and facilitators influencing formal and informal mental health help-seeking behaviours among school-going adolescents in S S A.
* Design D: Qualitative studies including focus groups, in-depth interviews, group discussions, and paired interviews; mixed-method studies to extract qualitative data.
* Evaluation E: Perceived barriers, facilitators, views, experiences, attitudes, challenges, hindrances, access and referral processes.
* Research type R: Peer-reviewed qualitative studies focusing on mental health help-seeking behaviours in S S A.
* Keywords: A comprehensive list of search terms including Help-seeking behaviour, Mental health help-seeking, Utilization of mental health services, Attitude towards seeking help, Access to mental health services, Help-seeking intention, Attitude towards counselling, Attitude towards psychotherapy, Africa or African help-seeking behaviour, Sub-Saharan or Sub-Sahara or Africa south of the Sahara help-seeking behaviour, Africa or African mental health, Sub-Saharan or Sub-Sahara or Africa south of the Sahara help-seeking attitude, Africa or African help-seeking attitude, Africa or African help-seeking intention, Sub-Saharan or Sub-Sahara or Africa south of the Sahara help-seeking intention, Barrier, Challenge, Obstacle, Impediment, Hindrance, Obstruction, Hurdle, Delay, Access, and Refer.
Search strategy and information sources
We searched the PubMed, PsycINFO, Scopus, CINAHL, Google Scholar and ERIC databases. The search combined target variables with the following Medical Subject Headings (MeSH) terms: (1) barriers and facilitators, (2) school-going adolescents, (3) MH, (4) help-seeking and access behaviours, (5) SSA and (6) qualitative studies. The search strategy was developed and adjusted according to the PRISMA guidelines (Aromataris and Riitano, Reference Aromataris and Riitano2014; Bramer et al., Reference Bramer, de Jonge, Rethlefsen, Mast and Kleijnen2018; Page et al., Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann, Mulrow, Shamseer, Tetzlaff, Akl, Brennan, Chou, Glanville, Grimshaw, Hróbjartsson, Lalu, Li, Loder, Mayo-Wilson, McDonald, McGuinness, Stewart, Thomas, Tricco, Welch, Whiting and Moher2021). See the Supplementary Material (Supplementary Appendix G) for the search strings for each database and the procedures used. The first search was conducted in March 2024, with updates in July 2024, June 2025 and September 2025. Staged search updates were undertaken to capture newly published qualitative studies prior to final synthesis and submission, ensuring that the review reflects the most current and comprehensive evidence available at the time of reporting.
Search process and methods
The reference lists of the included articles were screened, and reference management and duplicate removal were conducted using EndNote (Bramer et al., Reference Bramer, Rethlefsen, Kleijnen and Franco2017), while study selection was supported using Rayyan (Ouzzani et al., Reference Ouzzani, Hammady, Fedorowicz and Elmagarmid2016). In addition to database and software-assisted screening procedures (EndNote and Rayyan), manual backward and forward citation searching was conducted to identify relevant qualitative studies that may not have been consistently indexed across databases. Finally, we wrote to the corresponding authors of eligible articles [3] to obtain full-text versions; two full texts were successfully obtained, while one remained unavailable and was thus excluded.
Eligibility criteria
Studies were included if they met the following criteria: (1) the sample described was clearly school-going adolescents aged 10–19 years (Singh et al., Reference Singh, Siddiqi, Parameshwar and Chandra-Mouli2019; World Health Organization, 2018), (2) the population sampled was identified as being at some risk for MHPs and (3) the content examined formal and informal help-seeking behaviours using one or more qualitative methods, such as interviews, focus group discussions, ethnography and so on, to explore subjective experiences, motivations and sociocultural contexts in MH help-seeking. The QES included peer-reviewed studies available in English from 1990 onwards.
Studies outside SSA, those that did not target the specified age group or were not focused on MH help-seeking, along with quantitative studies, were excluded from the synthesis. Articles had to be peer-reviewed, complete and meet qualitative methodology criteria for inclusion. The detailed inclusion and exclusion criteria are presented in Table 2.
Inclusion and exclusion criteria for the included articles

Table 2. Long description
The table consists of three columns titled Criteria, Inclusion, and Exclusion, with six rows of data.
* Geographic scope. Inclusion: Studies conducted in Sub-Saharan Africa. Exclusion: Studies conducted outside Sub-Saharan Africa.
* Phenomenon of interest. Inclusion: Studies focusing on perceived barriers and facilitators to formal and informal mental health help-seeking behaviours. Exclusion: Studies not examining perceived barriers or facilitators to mental health help-seeking.
* Population. Inclusion: school-going adolescents aged 10 to 19 years. Exclusion: Studies not involving school-going adolescents aged 10 to 19.
* Study design. Inclusion: Studies utilise qualitative research methods such as interviews, focus groups, qualitative content analysis or ethnographic observations. Exclusion: Quantitative-only studies, studies that did not employ qualitative methods.
* Publication type. Inclusion: Peer-reviewed full-text articles published in English. Exclusion: Grey literature, non-peer-reviewed sources, non-English publications.
* Time frame. Inclusion: Published from 1990 onwards. Exclusion: Published prior to 1990.
Study selection and screening process
We initially imported the search results into EndNote 20 (Bramer and Bain, Reference Bramer and Bain2017; Fulbright and Evans, Reference Fulbright and Evans2024), whose duplication function was used to identify and eliminate duplicate records.
Four expert reviewers, including the lead author and three academic researchers with MH expertise (AIK, TC, RP and KAP), independently screened the identified articles. Each reviewer assessed the relevance of the articles to the review aim. We enhanced this method by manually searching the reference lists and recording missing citations for important papers in addition to the database search. After the initial title screening, two reviewers (AIK and RP) independently screened the abstracts of the selected studies. Articles approved by at least one reviewer proceeded to full-text evaluation.
Endnote supported the import of all retrieved records and the removal of duplicates at the beginning of the screening process (Ivey and Crum, Reference Ivey and Crum2018). The deduplicated library was then transferred to Rayyan to support blinded screening, manage reviewer decisions and record conflicts during title, abstract and full-text assessments (Ouzzani et al., Reference Ouzzani, Hammady, Fedorowicz and Elmagarmid2016). A custom-made pro forma in the form of an Excel spreadsheet (Gibbs et al., Reference Gibbs, Loveless and Crane2022) captured the final screening outcomes, documented exclusion reasons and organised the dataset required for PRISMA flow reporting.
Search results
A comprehensive initial search across six databases, including CINAHL (n = 125), PubMed (n = 1,054), ERIC (n = 105), PsycINFO (n = 112), SCOPUS (n = 509) and Google Scholar (n = 51), yielded 1,905 citations. After importing into EndNote, 298 duplicates were identified and removed. The remaining 1,607 records were screened using a combination of Rayyan (Ouzzani et al., Reference Ouzzani, Hammady, Fedorowicz and Elmagarmid2016) and EndNote relevance filters. These flagged 267 records as ineligible based on the predefined exclusion criteria (e.g., off-topic titles and lack of relevance to the review question). Another 31 records were removed for various reasons, such as the article format being an opinion piece, full text not accessible despite email correspondence to the author or non-English language. This left 1,309 records for the title and abstract screening.
Through manual screening, 1,197 records were excluded for not meeting the review’s core criteria, such as population mismatch, irrelevant outcomes and ineligible study designs. Subsequently, 112 full-text articles were retrieved for a detailed eligibility assessment. Of these, 90 articles were excluded for the following reasons: not conducted in SSA (n = 29), not involving school-going adolescents aged 10–19 (n = 19), not addressing perceived barriers or facilitators to MH help-seeking (n = 13), use of a quantitative methodology (n = 17), full texts inaccessible despite retrieval efforts (n = 01) and not peer-reviewed (n = 11). Twelve articles satisfied the requirements and were included in the final analysis. The PRISMA flowchart (Figure 1) visually represents the study selection process (Table 3).
PRISMA diagram for study selection.

Figure 1. Long description
The flowchart is divided into three vertical phases: Identification, Screening, and Included.
1. Identification Phase:
- Top-left box: Records identified from Databases n equals 1,905. Breakdown includes Cinahl n equals 125, PubMed n equals 1,054, E R I C n equals 105, Psyc I N F O n equals 112, S C O P U S n equals 509, and Google Scholar n equals 51.
- Top-right box: Records removed before screening. Duplicate records removed n equals 298, records marked as ineligible by automation tools n equals 267, and records removed for other reasons n equals 31.
2. Screening Phase:
- Second box down on left: Records screened n equals 1,309. An arrow points right to Records excluded during title and abstract screening n equals 1,197.
- Third box down on left: Reports sought for retrieval n equals 112. An arrow points right to Reports not retrieved n equals 10.
- Fourth box down on left: Reports assessed for eligibility n equals 102. An arrow points right to a detailed list of Reports excluded totaling 90. Reasons include: Not conducted in Sub-Saharan Africa n equals 29, Population not school-going adolescents 10 to 19 years n equals 19, Quantitative design studies n equals 17, Full text not accessible n equals 01, No focus on perceived barriers or facilitators to mental health help-seeking n equals 13, and Not peer-reviewed n equals 11.
3. Included Phase:
- Bottom-left box: Final studies included in review n equals 12.
Characteristics of included studies and their contribution to the review question (12)

Table 3. Long description
The table consists of 8 columns: Title, References, Country/study setting, Participants n; Type, Study design, Data collection, Data analysis, and Contribution to review question.
Key entries include:
* Mfidi Reference Mfidi2017: South Africa, 15 participants (teachers and nurses). Highlights institutional barriers like limited training and unclear referral pathways.
* Abdulsalam et al. 2023: Nigeria, 24 students. Identifies stigma and gendered expectations as barriers; peer support as a facilitator.
* van de Water et al. 2018: South Africa, 10 adolescents. Focuses on how stigma regarding P T S D interventions discourages engagement.
* Coetzee et al. 2022: South Africa, 66 stakeholders. Discusses confidentiality and parental involvement in psychoeducational programs.
* Meza et al. 2020: Kenya, 36 participants. Notes logistical constraints and the benefits of task-shifting.
* Carlson et al. 2021: Uganda, 59 participants. Emphasizes trust and institutional readiness.
* Khombo et al. 2023: Zimbabwe, 15 students. Links mental health literacy to service uptake.
* Addy et al. 2021: Ghana, 53 participants. Shows reliance on informal support systems like family and peers.
* Panford-Quainoo et al. 2024: Ghana, 15 counsellors. Highlights systemic challenges like role conflict and resource deficits.
* Mukuna Reference Mukuna2025 and Nkosi Reference Nkosi2025: South Africa, 8 learners each. Both focus on rural high school settings, literacy, and peer influence.
* Mushonga et al. 2025: Zimbabwe and Ghana, various stakeholders. Examines how parental engagement facilitates or constrains access to services.
Data extraction and study characteristics
The researchers conducted a systematic data extraction procedure after the 12 studies were selected for the QES. The research data extraction template included study characteristics (author name, publication year and country/setting) and methodological features (design approach, sampling method, data collection and analysis approach). Participant details and relevant first- and second-order constructs (direct participant statements and researcher interpretations) that matched the research question were also included.
Across the 12 included studies, qualitative interview-based designs predominated, with thematic analysis being the most employed analytic approach. The studies spanned Southern, West and East Africa, including South Africa, Ghana, Kenya, Nigeria, Uganda and Zimbabwe. Earlier studies primarily centred on adolescent perspectives, whereas more recent work incorporated multi-stakeholder and implementation lenses, reflecting a shift towards systems-level analysis. Across contexts, the findings consistently converged on institutional capacity constraints, confidentiality practices, stigma and family engagement as central determinants of formal and informal help-seeking within school settings.
The authors RP and AIK assessed all 12 studies. The dual review process entailed a comparison of the extracted data fields with the original study texts to verify their completeness and precision while maintaining consistent interpretation. The reviewers resolved differences in participant categorisation and thematic content interpretation through consensus discussions. The minor revisions involved improving the wording of the extracted themes to more accurately represent the participants’ meanings and correcting methodological descriptor inconsistencies.
Quality and risk of bias assessment process
AIK and RP evaluated the reporting quality of the 12 papers included in the review. We employed the Critical Appraisal Skills Programme (CASP) checklist (Long et al., Reference Long, French and Brooks2020; Haile, Reference Haile2022; Maeda et al., Reference Maeda, Caskurlu, Kozan and Kenney2023), a widely used instrument specifically developed to assess the reporting quality of qualitative research. The inter-rater agreement between the two reviewers (AIK and RP) was assessed using Cohen’s kappa (Kilpatrick et al., Reference Kilpatrick, Savard, Audet, Costanzo, Khan, Atallah, Jabbour, Zhou, Wheeler, Ladd, Gray, Henderson, Spies, McGrath and Rogers2024) based on independent ratings of the 12 included studies using the CASP checklist. The observed agreement was 87.5%, and the expected agreement by chance was 56.3%, resulting in a Cohen’s kappa of .714, which indicates substantial agreement.
The CASP checklist consists of 10 essential enquiries, each designed to evaluate distinct aspects of the research. These include a well-defined research purpose, methodological rigour, study design rationale, participant recruitment strategy, data collection methods employed (including explicit consideration of the researcher–participant relationship), ethical concerns and detailed processes undertaken for analysis to ensure analytical validity, transparency and clarity in the findings reported. Consequently, the synthesis included 12 studies with a total of 10 parameters (Table 2). Khombo et al. (Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023) did not meet the “clarity of the aims of the research” criterion. However, their study did not fall short on any of the other nine parameters used in this study. As the remaining criteria were satisfied, this study was included in the review. See Supplementary Appendix B for the study evaluation table based on the CASP.
Thematic analysis, coding and synthesis
We employed an inductive thematic analysis to establish the codes. This method allowed for the emergence of themes from the data rather than being pre-defined (Braun and Clarke, Reference Braun and Clarke2023). In NVivo, we sorted and coded the data according to various patterns and themes. This was done by reading and re-reading the primary source data (i.e. quotes by adolescents, MH experts and various stakeholders in the selected papers).
Confidence in the evidence
The review authors, AIK and RP, used the GRADE-CERQual approach to evaluate the confidence levels for each finding in their review. The GRADE-CERQual approach evaluates confidence in the evidence based on four main components: methodological limitations of the included studies, coherence of the review findings, adequacy of the data supporting the review findings and relevance of the included 12 studies to the review question (Lewin et al., Reference Lewin, Booth, Glenton, Munthe-Kaas, Rashidian, Wainwright, Bohren, Tunçalp, Colvin, Garside, Carlsen, Langlois and Noyes2018). The assessment of each component enabled us to reach a collective decision regarding the overall confidence level for each review finding, which we classified as high, moderate, low or very low. We began by assuming high confidence in all findings, which we reduced to lower levels when substantial concerns emerged in any of the four CERQual components. Both review authors reached an agreement during the final assessment (See Supplementary Appendix D, Table 5).
Results
Influence of barriers on mental health help-seeking behaviours
Across the reviewed research, the findings revealed that perceived stigma was the most frequently encountered barrier to accessing MH services (Mfidi Reference Mfidi2017; Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021; Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023). Other common barriers included low MHL (Meza et al., Reference Meza, Kiche, Soi, Khairuzzaman, Nales, Whetten, Wasonga, Amanya and Dorsey2020), cost (Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021), inaccessibility of services (Meza et al., Reference Meza, Kiche, Soi, Khairuzzaman, Nales, Whetten, Wasonga, Amanya and Dorsey2020; Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021), issues related to confidentiality (Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021) and negative past experiences with the provider (Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023). Parents’ attitudes (Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023) and academic pressure (Meza et al., Reference Meza, Kiche, Soi, Khairuzzaman, Nales, Whetten, Wasonga, Amanya and Dorsey2020) further inhibited adolescents from seeking help for MHPs. Table 4 summarises these barriers.
Barriers to mental health help-seeking

Table 4. Long description
The table consists of four columns and six numbered rows.
Row 1. Barrier Theme: Perceived stigma. Subthemes: Social or public stigma and cultural stigma. Number of Studies: 12.
Row 2. Barrier Theme: Gender norms as a barrier to help-seeking. Subthemes: Masculinity norms and stigma around emotional expression; gendered socialisation and structural constraints on help-seeking. Number of Studies: 9.
Row 3. Barrier Theme: Mental health literacy (Knowledge, misconceptions and awareness gaps). Subthemes: Poor recognition of M H P s; limited knowledge and misbeliefs about self-help and professional support options; negative attitudes hindering M H P recognition and help-seeking; limited knowledge of how to access mental health information. Number of Studies: 11.
Row 4. Barrier Theme: Privacy, trust and confidentiality concerns with M H professionals. Subthemes: Fear of confidentiality breaches; inadequate counselling environments and lack of privacy; distrust in mental health professionals. Number of Studies: 7.
Row 5. Barrier Theme: Lack of accessibility and availability of M H services. Subthemes: Distance to services; lack of mental health professionals; inadequate resources. Number of Studies: 9.
Row 6. Barrier Theme: Family and parental attitudes, peer influence and alternative support. Subthemes: Family control and restriction of help-seeking; preference for informal and relational support networks; cultural and normative beliefs shaping help-seeking. Number of Studies: 7.
Theme 1: Perceived stigma
All studies reviewed indicated perceived stigma as the most frequently cited barrier to MH help-seeking behaviours among school-going adolescents. Stigma was conceptualised across four interrelated dimensions: social/public stigma (negative reactions from others), anticipated stigma (fear of being judged if one seeks help), self-stigma (internalised shame and self-blame) and cultural stigma (beliefs linking mental distress to moral, spiritual or supernatural explanations). Adolescents who encounter stigma related to MH are less likely to acknowledge their potential MHPs and seek formal or informal help for their MH. This collectively creates an environment in which seeking help for MHPs is met with shame, fear and reluctance to seek help.
The pervasiveness of stigma and cultural standards has contributed to an atmosphere in which confronting problems related to MH elicits feelings of dread and shame. For example, in some schools and communities, adolescents who express emotional distress or seek MH support risk being labelled as weak or disobedient, especially where strength and emotional control are linked to respectability and maturity.
The stigma surrounding MH topics is often reinforced socially by peer groups, either explicitly or implicitly. Adolescents often face severe social/public stigma from their families, peers and communities in SSA (Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021; Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023). This stigma usually stems from negative opinions and false beliefs about MHPs themselves, such that the fear of being ostracised or labelled as “weak” or “crazy” prevents adolescents from acknowledging their MHPs and seeking help. Evidence from one included study indicates that adolescents encounter overtly negative peer reactions to MH difficulties, as reflected in the following account: “Their response is unkind, and their behaviours can be shameful. They show emotions of fear and hate…” (Nkosi, Reference Nkosi2025, p. 27), demonstrating a deep-rooted fear of judgement.
Similarly, another study reported that female adolescents avoid disclosure due to fear of being labelled or judged: “When you let people know what you are going through, they will think you are mad. I just keep to myself” (Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021, p. 12). This demonstrates that adolescents, in their bid for acceptance, are sensitive to how their peer group may react, thus inhibiting them from seeking help (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018). For example, one study reported that peers often respond with ridicule or exclusion: “People would ‘[not] talk to them. They make fun of them,’ say, ‘you are crazy’ and ignore them, or ‘judge them.” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p. 1091).
Adolescents are often worried about the disclosure of their MHPs, as it can lead to rumours and stigma among the public. For example, one study reported the following: “…I heard people in the community whispering my name about something I had said in the session, and it broke my trust…” (Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023, p. 5).
A participant in another study reported a similar stigmatising experience: “I heard students saying they were making fun of themselves, and they said, ‘you, you have a mental problem, go and talk to the counsellor, go and see the counsellor’.” (Panford-Quainoo et al., Reference Panford-Quainoo, Oppong Asante and Osei-Tutu2024, p. 190). Overall, social and public stigma cumulatively contribute to an inhospitable atmosphere for adolescents, in turn discouraging them from seeking MH services. The widespread presence of these stigmas intensifies the lack of communication with others about one’s MHPs, further exacerbating isolation and the potential for more severe MHPs.
In addition to social and public stigma, SSA communities are confronted with cultural stigma that affects adolescent help-seeking (Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023). Cultural stigma refers to the beliefs and views that connect MHPs with weakness or failure embedded within a cultural context (Codjoe et al., Reference Codjoe, Barber, Ahuja, Thornicroft, Henderson, Lempp and N’Danga-Koroma2021; Ojagbemi and Gureje, Reference Ojagbemi and Gureje2021). In many SSA cultures, MHPs are often seen as having a lack of will or a spiritual problem that causes families and communities great shame and humiliation. One secondary school student in a study from Ghana stated, “When you start hearing voices, it’s only the spiritualist like fetish priests who can help you” (Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021, p. 12). Additionally, another secondary school student perspective reflects this noting that“…these psychotic mental illnesses are said to be caused by evil spirits or to be a kind of retribution from supernatural spirits or beings” (Nkosi, Reference Nkosi2025, p. 28). A participant in another study reported, “My family… were like, ‘Counselling? Really?’… ‘Counselling is for White people only.’” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p. 1092). As Brouwers (Reference Brouwers2020) propose, culture can also breed silence among MHPs.
Theme 2: Gender norms as a barrier to help-seeking
Gender norms play a significant role in adolescents’ decisions to seek MH help (Campbell et al., Reference Campbell, Bann and Patalay2021; Jörns-Presentati et al., Reference Jörns-Presentati, Napp, Dessauvagie, Stein, Jonker, Breet, Charles, Swart, Lahti, Suliman, Jansen, van den, Seedat and Groen2021). Studies have indicated that female students are generally more willing to seek professional help than their male counterparts (Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023). This difference stems from societal norms that label emotional expression as a weakness, especially among boys (Meza et al., Reference Meza, Kiche, Soi, Khairuzzaman, Nales, Whetten, Wasonga, Amanya and Dorsey2020; Coetzee et al., Reference Coetzee, Gericke, Human, Stallard and Loades2022). In many cultures, boys are expected to be stoic, making it difficult for them to acknowledge psychological distress or to seek help (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018; Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021; Abdulsalam et al., Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023).
In contrast, girls are socialised to be more open about their feelings and encouraged to seek support when needed (Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023). Evidence from one included study illustrates how prior exposure to counselling can reinforce help-seeking among female students:“…female participants use more emotion-focused strategies, such as seeking emotional support from others than male participants” (Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023, p. 3).
However, male students often avoid MH services due to fear of losing their dignity. For example, one study reported: “Seeking counselling is for women; men bottle their issues lest they lose their dignity.” Similarly, a participant from another study reported, “As a male, this thing of going to see someone to cry and talk to is taboo; it takes away my masculinity” (Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023, p. 5). Similarly, another study reported a participant who stated, “I think the girls and boys experience things that they wouldn’t necessarily want to say in front of the other, or the boys are going to be too cool to say in front of the girls…” (Coetzee et al., Reference Coetzee, Gericke, Human, Stallard and Loades2022, p. 196). Societal pressure to conform to masculine ideals makes it harder for boys to seek help.
To further illustrate the impact of gender norms as a barrier to help-seeking, Abdulsalam et al. (Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023) found that both gender and age play a role in whether adolescents in Northeastern Nigeria seek help for MHPs. These patterns are further influenced by the interaction between cultural or religious norms and the student’s gender. For example, one study reported a participant who stated feeling uncomfortable when a young man was selected as a counsellor: “I don’t feel like going for counselling there. Our counsellor is a young male counsellor. In Islam, an unmarried girl should not sit alone with a man not from her family because something bad may happen between them.” (Abdulsalam et al., Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023, p.12). Male counsellors also face difficulties due to religious beliefs. One counsellor noted, “There are insinuations and allegations if you are a young, unmarried chap as a counsellor. Because you sit with students, especially females, people suspect you, not that you are doing your counselling work” (Abdulsalam et al., Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023, p.12). Identifying and managing gender dynamics is necessary to improve adolescents’ MH help-seeking behaviours.
Theme 3: Mental health literacy (knowledge, misconceptions and awareness gaps)
Due to low MHL, defined as “knowledge and beliefs about MHPs which aid their recognition, management or prevention” (Jorm et al., Reference Jorm, Korten, Jacomb, Christensen, Rodgers and Pollitt1997, p.182), adolescents do not always seek help for MHPs (Amone-P’Olak et al., Reference Amone-P’Olak, Kakinda, Kibedi and Omech2023; Ma et al., Reference Ma, A-M and Anderson2023; Clough et al., Reference Clough, Nazareth, Day and Casey2024). Four main components affect adolescents’ knowledge and behaviour regarding MH, including: poor recognition of MHPs; limited knowledge and misbeliefs about self-help and professional support; negative attitudes hindering MHP recognition and help-seeking; limited knowledge regarding how to access MH information.
Often, adolescents misunderstand or mislabel their MHPs due to, for example, parents mislabelling an adolescent’s MHPs as mere obstinacy or wilfulness. Many believe that their distress is temporary or normal and do not believe that it is a mental illness. One study reported a participant who highlighted, “Some of [the guardians] would not come… they did not understand the value of psychological treatment (PT).” (Meza et al., Reference Meza, Kiche, Soi, Khairuzzaman, Nales, Whetten, Wasonga, Amanya and Dorsey2020, p. 6). Another study reported a participant who revealed, “Parents wouldn’t know what their children are going through. They are not even aware. They will just say it’s stress. They just take it for granted. So, they should attend those meetings” (Mushonga et al., Reference Mushonga, Jopling, Glozah, Kamvura, Dodd, Gudyanga, Maramba, Dambayi, Ayuure, Bere, Achana, Owusu, Chibanda, Abas, Weobong and Kumwenda2025, p. 7). This barrier was also found in teachers, as one student stated, “My teacher thinks I am lying about it [attending counselling]. Because I am too naughty, I don’t go to school” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p. 1092).
Some adolescents reduce MH to only stress and emotional control, as one study reported the following: “Mental health is when you are stressed or anxious about certain things (s) in your life. Some learners may be able to handle them, some may not. When they do not, they may not behave well.” (Mukuna, Reference Mukuna2025, p. 15). Another study reported a teacher who confirmed the above narrative when she stated, “sometimes we may mistakenly label the adolescents as ill-disciplined or moody whereas it may be signs of an emotional problem” (Mfidi, Reference Mfidi2017, p.8). When distressed, adolescents usually do not seek help because they do not recognise that something is wrong with them.
Furthermore, adolescents do not often understand MHPs and their development. As a result, when they experience a MH concern, they may interpret these symptoms as personal weakness and feel compelled to manage them independently rather than seek support. This internalisation can interfere with their ability to concentrate and participate in academic activities, as distress remains unaddressed. For example, one study reported that distress can disrupt attention and engagement in classroom settings “:If that child is sitting with that blow… in class… and that teacher is explaining something here on the board and that child’s… attention is here with the pain… or with that person who hurt him…” (Coetzee et al., Reference Coetzee, Gericke, Human, Stallard and Loades2022, p. 194). Similarly, another study reported that limited awareness contributes to dismissive attitudes towards MH: “Learners at my school are nonchalant towards issues like mental health and behavioural problems. They are not well educated or well informed about these issues…” (Nkosi, Reference Nkosi2025, p. 30). In the absence of knowledge about the risk factors and causes, adolescents may fail to understand the gravity of the disorder and the urgent need for help to address it.
Adolescents often do not know where to go or how to help themselves effectively when MH issues arise. One study reported: “If I need some to talk to, I talk to my boyfriend who is always there to offer me advice and comfort when I am stressed, so I don’t think I need a counsellor or a psychologist to deal with my problems” (Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023, P.6). Many would rather seek informal support than recognise and use self-help strategies or professional resources.
One major aspect of MHL is awareness of the professional help available. Many adolescents do not know how to seek help when they need it. One study reported that adolescents often experience uncertainty surrounding the help-seeking experience, stating: “The clinic… they are going to ask too many questions… They would just have told me to ‘just get it out of my mind’… and then told me to go home.” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p. 1092). This lack of knowledge and subsequent mistrust was further reflected in another study where a participant expressed the following:
I do not trust doctors… They look nice, but no, I do not trust them… I was going toward a social worker, a real social worker. Not doctors. Even if they come with a social worker, I would ask them what company you are working for. I am going to ask her a question… If I have to Google about it, I will Google. I must make sure where I am” ( van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018 , p. 5).
The lack of knowledge about available professionals contributes to adolescents’ unwillingness to seek prompt help due to a lack of understanding and trust. Adolescents often remain hindered by negative attitudes from both themselves and providers and an inability to recognise signs and symptoms of MHPs. Most adolescents blamed their MHPs on themselves instead of considering them a medical issue. One study reported, “…they will try for a day or two, like I said, but their attitude is already ‘it’s [the programme] not going to work, the children are broken, they come broken from home, so what should I now fix?’” (Coetzee et al., Reference Coetzee, Gericke, Human, Stallard and Loades2022, p. 193).
Adolescents require further guidance when searching for correct MH information. One school administrator indicated that teachers and other staff lacked knowledge about MH in general: “Some teachers are unable to recognise and seek help for their learners’ MHPs due to lack of specific training on mental health” (Mfidi, Reference Mfidi2017, p. 10). Another study reported, “I may have studied psychology, but at times we are not skilled to deal with some of these social, emotional, and behavioural problems. We just have to refer them” (Mfidi, Reference Mfidi2017, p. 7). This perception is further illustrated by the following statement by a participant in another study: “The thought of talking about my life might bring up some problems I thought I had overcome, and that could increase my stress. So, whenever I hear about mental health issues, I just avoid them” (Abdulsalam et al., Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023, p. 8).
This lack of awareness about existing MHPs applies to the school environment as well. Usually, teachers are the first point of contact for students experiencing MHPs, but teachers often do not receive adequate MH training. For example, in one study, a teacher noted, “I can help. I just do not know what it looks like when a child needs help” (Meza et al., Reference Meza, Kiche, Soi, Khairuzzaman, Nales, Whetten, Wasonga, Amanya and Dorsey2020, p. 8). Similarly, another teacher remarked, “I feel unprepared to handle mental health issues among students because I haven’t received any training in this area” (Mfidi, Reference Mfidi2017, p.8). This lack of awareness from teachers, who are often the first critical point of contact for struggling students, further hinders student awareness, “I have never been to counselling before, so I never knew what counselling was about” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p. 1093).
This MHL gap also applies to parents who may not be equipped to help, depending on their MHL. For example, A teacher in one study described that some caregivers are “…people who do not know how to handle their emotions themselves so they cannot help children…” (Coetzee et al., Reference Coetzee, Gericke, Human, Stallard and Loades2022, p. 6). Some adolescents and their parents may also not fully appreciate the usefulness of MH services. A study reported a participant who indicated a reluctance to seek professional help, stating: “…I don’t want to hear about psychological issues or having to go and see a counsellor, it really makes me sick.” (Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023, p.5).
Many adolescents further believe that if their friends or partners support them, they do not need to seek help from professionals. This is reflected in one study: “I talk to my boyfriend…so I don’t think I need a counsellor” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p. 8), further illustrating the preference for informal support over professional help.
Collectively, these studies revealed that participants associated seeking help for MHPs from a MH practitioner with inferiority or weakness. These perceptions and the lack of knowledge and awareness collectively inhibit effective help-seeking behaviours, indicating a need for more MHL.
Theme 4: Privacy, trust and confidentiality concerns with mental health professionals
Concerns about privacy and confidentiality are significant barriers to adolescents seeking MH services in SSA (Mutahi et al., Reference Mutahi, Larsen, Cuijpers, Peterson, Unutzer, McKay, John-Stewart, Jewell, Kinuthia, Gohar, Lai, Wamalwa, Gachuno and Kumar2022; Hlophe et al., Reference Hlophe, Tamuzi, Shumba and Nyasulu2023). Adolescents frequently express fear that their disclosures might be revealed to others, such as teachers, parents or peers (Yao et al., Reference Yao, Li, Wang and Hui2021). For example, one study documented the following “:I know the school has a counselling unit. But ahhh… I will not go there. I am shy of the teachers” (Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021, p. 12).
The physical setting of counselling offices exacerbates these problems. Open or poorly designed spaces are perceived as unsafe, discouraging help-seeking behaviours. Inadequate infrastructure, such as counselling offices divided by plywood, creates an environment where adolescents feel exposed. One study documented the following: “Our counselling office is too open. They used plywood to divide the library and the office; I feel people hear what I discuss. To me, the place is not ok; it is not worth it” (Abdulsalam et al., Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023, p. 10). Another study further described the experience of exposure: “It’s like the whole world is watching me; I feel I was doing something wrong… worried since the room is not hiding” (Abdulsalam et al., Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023, p. 10). Alarmingly, these concerns are not unwarranted, as adolescents report a general lack of privacy related to MHP help-seeking: “They would call our names on the intercom, and all of the kids would be like ‘where are you going, what’s going on there?’” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p. 1094).
Trust in the MH care provider is another critical issue. Adolescents often report negative experiences with professionals, leading to a lack of faith in counselling services. One study presented the following account:
……I do not trust anyone. If I do not trust my mom and dad, why would I trust someone I am not even related to? I have been disappointed by people I trust in my life and trusting someone I do not know is not something I will ever do. I tell my stories to God whenever I face challenges… (Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023, p.5).
A professional in one study confirmed the above by stating “From my encounter with those who came to me, initially, they were hesitant because of some previous experiences that students would share; they went to see a counsellor, and the next moment, somebody had heard their issues.” (Panford-Quainoo et al., Reference Panford-Quainoo, Oppong Asante and Osei-Tutu2024, p. 190). Another shared how a breach of confidentiality during group therapy destroyed their trust:
…I have been to group therapy before, and a few days after I attended a session, I heard people in the community whispering my name about something I had said in the session, I will never trust anyone in the counselling session, including the counsellor… (Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023, p.5).
Adolescents also doubt counsellors’ capacity to understand their issues: “I do not believe the counsellors understand our problems; they just follow a script” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p. 1091). One study provided the following account related to counsellors providing services internally within the schools: “I don’t think it should be internal because it helps them if it’s someone from outside… it’s delicate… not something that children [are] necessarily going to share with a teacher” (Coetzee et al., Reference Coetzee, Gericke, Human, Stallard and Loades2022, p. 195). This reveals another layer, such that students doubt that school counsellors will keep their MHPs private. Another study provided the following account of a student’s concerns related to counsellors sharing information: “She is going to speak about it with… other counsellors” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p. 1091). Such perceptions, combined with stigma, encourage students to “sneak in” for counselling, as observed by one teacher–counsellor in another study: “Students who come for counselling don’t feel at ease… more like sneaking in, watching when to come… like it’s a taboo” (Abdulsalam et al., Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023, p.10).
According to the adolescents, such perceptions of confidentiality breaches profoundly impact their trust in MH services (Haraldsson et al., Reference Haraldsson, Pingel, Nordgren, Johnsson, Kristiansson and Tindberg2022; Kip et al., Reference Kip, Udedi, Kulisewa, Go and Gaynes2022). Thus, it is imperative to ensure that counselling takes place in a secluded location and that the counsellor faithfully adheres to confidentiality rules to build and keep trust with adolescent clients. Students must be informed about these confidentiality protocols ahead of sessions.
Theme 5: Lack of accessibility and availability of mental health services
Lack of access to MH services is another major barrier to help-seeking behaviours among adolescents, particularly in rural SSA (Sarikhani et al., Reference Sarikhani, Bastani, Rafiee, Kavosi and Ravangard2021; Mindu et al., Reference Mindu, Mutero, Ngcobo, Musesengwa and Chimbari2023). Owing to geographic proximity, adolescents in rural educational institutions often lack access to qualified MH professionals, such as counsellors or counselling psychologists. An administrator from one study stated, “Many rural schools have difficulty adopting and implementing school mental health systems… This is caused by insufficient specialised mental and behavioural health personnel such as school counsellors, psychologists, and social workers” (Nkosi, Reference Nkosi2025, p. 27). Similarly, an administrator from another school stated, “During the rainy season, heavy rain significantly increased transportation fees and made roadways to school impassable, posing a barrier to students and their parents’ attendance” (Meza et al., Reference Meza, Kiche, Soi, Khairuzzaman, Nales, Whetten, Wasonga, Amanya and Dorsey2020, p.8).
In addition to issues associated with counselling accessibility at rural schools, another study reported institutional capacity constraints: “Well, I think the challenges, one is the fact that you’re playing a double role; you’re a counsellor, you’re a teacher. So, when you are in the classroom, and somebody needs you for counselling and you’re not available” (Panford-Quainoo et al., Reference Panford-Quainoo, Oppong Asante and Osei-Tutu2024, p. 190).
Financial constraints further exacerbate accessibility-related hurdles. Low-income communities and their respective schools sometimes experience substantial economic adversity, leading to a focus on meeting essential requirements such as food and school expenses rather than prioritising MH care. As one study reported, “We used to go together with health promoters… But now the transport we use cannot accommodate them” (Mfidi, Reference Mfidi2017, p. 8). Similarly, a participant from another study reported, “Currently they [school counsellors] are full to the ears… I just feel those children—I think some of our parents do not have the means to get professional help for them.” (Coetzee et al., Reference Coetzee, Gericke, Human, Stallard and Loades2022, p. 193). Many adolescents cannot afford MH services because of the costs involved, whether for the service itself or for the related expenses, such as transport. Many colleges also do not have adequate counselling facilities, nor educated professionals to ensure a standard of MH care for students. One study illustrated this by stating, “You could sit in the queue the whole day but not get the help you needed.” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p. 1095). Thus, accessibility and availability issues prevent MH help-seeking among adolescents despite their intentions to do so.
Theme 6: Family and parental attitudes, peer influence and alternative support
It has been well-established that family and parental attitudes can serve as barriers to the MH help-seeking behaviour of adolescents. The attitudes of some parents become a barrier, blocking their children from seeking support. For instance, one study reported a participant who remarked, “Pressure from our peers can impact us negatively, including the abuse from guardians, parents… Abuse from our parents impacts us a lot, and it is not easy to talk about it…” (Nkosi, Reference Nkosi2025, p. 30). Despite the potential for negative attitudes, parents and families still provide alternative sources of emotional and financial support for adolescents, who often seek comfort from family instead of MH professionals. This is reflected in the following quote: “Parents are the first source of life to the child in terms of love and care. This is why students are homesick when they need advice… to discuss their problems closely, a kind of allegiance.” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p.6). Similarly, another study reported, “They feel it is their duty, a natural duty… they feel they are more obliged as parents or family to advise and guide the student. This perspective affects the sensitivity of the child; nearly in everything, including getting help” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p.6).
Siblings and extended families also play a significant role in help-seeking activities. Adolescents often discuss issues with their older siblings when they do not wish to reveal perceived confidential information to their parents. According to one study, older siblings counselled younger ones on choosing a career, higher institution and gender-related issues such as relationships and social expectations (Abdulsalam et al., Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023). However, judgement from parents about MH can discourage treatment: “I don’t think parents truly understand what mental health issues entail. Mine don’t,” an adolescent remarked (Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021, p. 8).
During adolescence, when we rely on our social networks, peers may also have considerable influence over one another, as they have established trusting relationships. Some peers function as a barrier to help-seeking; for example, as one participant shared, “I was embarrassed to go to therapy, especially when my school friends asked about it” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p. 1092), whereas other peers function as an informal help-seeking pathway. For instance, one adolescent reported, “My boyfriend is the one who comforts me because I do not trust anybody” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p.1092). According to Khombo et al. (Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023), most adolescents prefer informal support systems over professional services. One of the main reasons for this is the stigma associated with using professional services.
A preference for familiar connections may subsequently result in reduced engagement with supportive services (Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023). As one participant noted, “If I need some to talk to, I talk to my boyfriend who is always there to offer me advice and comfort… I don’t think I need a counsellor or a psychologist to deal with my problems.” (Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023, p.6).
Some parents prioritise academic and other responsibilities over MH, which may further discourage adolescents from seeking help for MHPs. As reported in one study, a student presented the following account, “Because some of them are the ones who ill-treat us. If they knew that we are getting help somewhere, they might even hate us. That would become a disadvantage to us.” (Mushonga et al., Reference Mushonga, Jopling, Glozah, Kamvura, Dodd, Gudyanga, Maramba, Dambayi, Ayuure, Bere, Achana, Owusu, Chibanda, Abas, Weobong and Kumwenda2025, p. 10). Such an attitude of overlooking MHPs can fuel the notion that one’s problems may not be serious, so the adolescent avoids professional help. Another study reported a student’s account who shared their experience of their parents’ hurtful and unsupportive behaviour during a traumatic incident, stating:
[Parents] do not expect the bad from their family … they do not really care. So, it was difficult for me to speak to people about [the traumatic incident] … My daddy went to confront [the perpetrator], and then he denied everything, and my mummy said “ I must not press charges because it is my auntie’s only child” … It felt like no one cared … [when I told my mom and gave the forms and stuff] she just looked at me and then she was like, are you sure it was him? ( van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018 , p.1092).
Religious beliefs and practices are another factor affecting the help-seeking behaviours of school-going adolescents. Some students draw upon their religious communities or spiritual tools instead of counselling for support. According to one study, a participant stated, “ students seek spiritual guidance if they sense the matter is between them and God… strictly spiritual “(Abdulsalam et al., Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023, p. 1305). This sentiment was echoed by another study which reported, “When you start hearing voices, it’s only the spiritualists like fetish priests who can help you” (Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021, p. 12).
Facilitators of mental health help-seeking behaviours
The reported facilitators of MH help-seeking among adolescents included supportive family dynamics, positive peer influence, accessible informal networks and cultural or community resources (see Table 5).
Facilitators of mental health help-seeking

Table 5. Long description
The table consists of four columns: an index number, Facilitator theme, Sub-themes, and Number of studies.
* Row 1: Mental health education and literacy enhancement. Sub-themes include promotion of mental health literacy, access to information and resources, integration into the school curriculum, and parental mental health education. Supported by 12 studies.
* Row 2: Supportive school environment or climate. Sub-themes include school mental health initiatives, school mental health policies, and institutional commitment. Supported by 10 studies.
* Row 3: Improved professional services. Sub-themes include availability of trained and specialized mental health professionals, and confidential, gender-sensitive, and culturally appropriate care. Supported by 8 studies.
* Row 4: Family, community involvement and peer support. Sub-themes include family communication and emotional support, peer support and shared coping, and community-based support and outreach. Supported by 8 studies.
* Row 5: Improved service accessibility and affordability. Sub-themes include policy and financial investment in mental health services, and school-based integration of mental health services. Supported by 6 studies.
Theme 1: Mental health education and literacy enhancement
All 12 studies identified increased awareness and MH education as the main driver of help-seeking behaviours among school-going adolescents in SSA. When adolescents receive MH information that is both clear and culturally relevant, they display higher rates of early symptom recognition and are more willing to pursue help while talking openly about their MHPs. Adolescents are also more likely to seek help when MH education is integrated into life skills training by teachers and when peer leaders facilitate open discussions with students. Promotion of MHL at the school and community level was identified as an important facilitator for enhancing help-seeking behaviour among school-going adolescents (Meza et al., Reference Meza, Kiche, Soi, Khairuzzaman, Nales, Whetten, Wasonga, Amanya and Dorsey2020; Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021; Coetzee et al., Reference Coetzee, Gericke, Human, Stallard and Loades2022). To illustrate this, one participant (female caregiver) noted:
I am of the view that if all the stakeholders in the school could be sensitized—what do I mean by the stakeholders? The parents, the children themselves, the teachers, and the people who manage the school—about how children can be handled. I think it can help the children to have good mental health. (Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021 , p.6).
Another study noted the benefits of MHL, stating that “Learning about mental health in school made it easier to talk about my problems” (Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021, p. 7). Similarly, interdisciplinary collaboration within school settings was also identified as a mechanism for strengthening MH support, particularly through coordinated involvement of teachers, parents and school leadership. As one school stakeholder emphasised, “The promotion of mental health through interdisciplinary collaboration in schools was also deemed essential” (Mfidi, Reference Mfidi2017, p. 8).
In addition to increasing MHL as a facilitator of help-seeking, visibility of MH services for adolescents helps to clarify available resources and enhance the likelihood of their utilisation (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018). For example, flyer distribution, community programming and information dissemination through the internet may enhance awareness of MH services for school-going adolescents. As one student indicated, “It was through the support and information I received during the trial that I learned about PTSD and the available treatments. This knowledge motivated me to seek help when my symptoms worsened” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p. 1091). Another participant remarked on the helpfulness of peer education, “Peer education programme undertaken by the provincial department is not regularly done, but it does help” (Mfidi, Reference Mfidi2017, p. 7). Integrating MH education into the school curriculum was noted as another critical facilitator of help-seeking (Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021; Coetzee et al., Reference Coetzee, Gericke, Human, Stallard and Loades2022). Incorporating MH education into the curriculum gives adolescents a platform to express themselves and encourages them to seek help for MHPs. One study reported, “School counsellors recommended that the content of such a programme should be psychoeducational and in-line with the current school-curriculum.” (Coetzee et al., Reference Coetzee, Gericke, Human, Stallard and Loades2022, p. 195).
One study provided the following account of a teacher who stated that MH education could be beneficial in preventing suicide ideation and behaviours, suggesting the following: “Just like we have this sex education thing, I think it [mental health education] should be added because of the way people are even committing suicide today because of some trivial issues” (Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021, p. 13). Another adolescent noted the benefits of MHL in school, stating “Learning about mental health in school showed me it’s important to seek help” (Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021, p. 8). Therefore, introducing MH education into the school curriculum can help enhance the students’ knowledge and outlook towards MH, which in turn encourages them to ask for help when needed (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018; Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021; Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023).
Despite issues related to the lack of MH education and literacy, findings showed that education programmes can help families and parents understand the mental wellness needs of adolescents. Workshops and seminars for parents, for example, can create a bridge between home and school activities that further facilitate a positive environment for adolescents. As a study reported, “The workshops assisted my parents in understanding what I am facing and how I could be assisted” (Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021, p. 13). Another participant remarked, “The only way you can get most of the parents is usually when there is a PTA meeting. So that is a way that you can get them and give them that education concerning mental health issues.” (Mushonga et al., Reference Mushonga, Jopling, Glozah, Kamvura, Dodd, Gudyanga, Maramba, Dambayi, Ayuure, Bere, Achana, Owusu, Chibanda, Abas, Weobong and Kumwenda2025, p. 6). These educational programmes for parents can equip families with the skills to identify and deal with MHPs.
Theme 2: Supportive school environment or climate
The second facilitator theme that emerged from the QES was a supportive school climate, which can motivate school-going adolescents from SSA to seek help for their MH. A school’s climate is defined as the socio-cultural, psychological, safety and educational environment that stimulates learning, social growth and emotional well-being (Wang & Degol, Reference Wang and Degol2016). Across studies, participants noted that programmes designed to support student MH would be beneficial: “Teachers and school counsellors explained that a programme like this would help them meet the demand for mental health and behavioural support in the schools” (Coetzee et al., Reference Coetzee, Gericke, Human, Stallard and Loades2022, p. 193). Among studies of schools where such programmes have been implemented, participants generally report positive feedback, with one noting that it was “a surprise to find ‘someone out there that cares’” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p. 1094).
Our review further found that a positive school climate is reflected in the fair implementation of rules and regulations, the promotion of norms and values, student engagement, attachment to school and teaching activities that enhance learner agency (Thapa et al., Reference Thapa, Cohen, Guffey and Higgins-D’Alessandro2013). Schools that offer counselling services and maintain a positive environment can help students to deal with their MHPs (Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021; Coetzee et al., Reference Coetzee, Gericke, Human, Stallard and Loades2022). Involving MH experts in providing support for students, such as counsellors and educational psychologists, rather than relying solely on teachers, is highly effective (Coetzee et al., Reference Coetzee, Gericke, Human, Stallard and Loades2022). Teachers and parents should serve as the first point of contact and a referral pathway to these specialists.
Our findings also demonstrated that to develop a positive school climate that encourages adolescents to seek help, policies surrounding MH must be created (Coetzee et al., Reference Coetzee, Gericke, Human, Stallard and Loades2022). In schools, where guidance and counselling units are well established, students and teachers understand the importance of strong support systems in promoting adolescent MH (Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021). One participant in a study stated, “For me, I see them having a positive view about counselling in general… the trust has been built; freshers learn from those who are already in the system, and those in that system speak well about my office” (Panford-Quainoo et al., Reference Panford-Quainoo, Oppong Asante and Osei-Tutu2024, p. 191). According to another teacher, providing a source of support by actively listening to students’ concerns is also helpful in enhancing school climate:
…where a child is listened to, whenever a child has a problem, there must be someone to listen even if you cannot act, but just giving a child time makes that child have [better] feelings and will be free with whatever problem will not keep any challenge the child has, he will be able to always to speak out whenever he has a problem” (Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021 , p. 4).
Theme 3: Improved professional services
Schools require the presence of trained MH professionals, such as counsellors and psychologists, to take care of the MH of adolescents. Students should not receive counselling services from teachers. Rather, teachers should refer students to a MH professional, who can refer them to proper interventions (Panford-Quainoo et al., Reference Panford-Quainoo, Oppong Asante and Osei-Tutu2024; Nkosi, Reference Nkosi2025). Support for counselling services was noted across studies. For example, a participant from one study noted: “Having a professional counsellor at school makes me feel like my problems are taken seriously” (Abdulsalam et al., Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023, p. 1202). This is similarly reflected in another study, “It was a surprise to find ‘someone out there that really cares’” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p. 1093). These perceptions speak to the faith students have in MH professionals working within school settings, as well as the positive outcomes for students with access to these professionals.
One of the most important components of MH services offered in schools involves the assurance of confidentiality. Our review revealed that assured confidentiality enhances trust, as users feel less at risk of negative judgement, stigma or exposure to their peers and family (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018; Meza et al., Reference Meza, Kiche, Soi, Khairuzzaman, Nales, Whetten, Wasonga, Amanya and Dorsey2020). For instance, one participant from van de Water et al. (2018) remarked: “I was relieved to share my secret with the nurse counsellor because she’s not my friend and she’s not part of my family” (van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018, p. 1094). Similarly, another study reported, “I can speak about my issues easily because our school keeps everything private.” (Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021, p. 7).
Theme 4: Family, community involvement and peer support
Family, community and peer involvement encourage school-going adolescents in SSA to seek help for their MHPs (Coetzee et al., Reference Coetzee, Gericke, Human, Stallard and Loades2022). These types of involvement include open communication, peer support and encouragement and community outreach. Open communication within the family was important in helping adolescents to seek MH help. Regular and open discussions within families about MH can be effective in reducing stigma and encouraging adolescents to seek help. As one study reported,
Where I come from, we do not tell anyone who is outside of the family anything we are going through, both on a personal and family level. Whenever we have challenges in life, we find someone we are close to in the family, we tell them, and we get help…. (Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023 , p.5).
In addition to family, a peer participant described offering sustained emotional support:
If you need somebody to talk to, I am here for you… Even if you go through bad things …. I can help you … Cause me too I was in a very bad space. I will go with you until you finish your counselling ( van de Water et al., Reference van de Water, Rossouw, van der Watt, Yadin and Seedat2018 , p. 1095).
Similarly, a teacher highlighted the positive role of families in adolescents’ help-seeking, stating, “Parents are the first source of life to the child in terms of love and care. This is why students are homesick when they need advice … to discuss their problems closely, a kind of allegiance (Abdulsalam et al., Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023, p. 5).
Student-led peer support groups and peer counselling initiatives are also powerful facilitators of MH help-seeking. Specifically, help-seeking programmes facilitate and motivate a culture of seeking help among adolescents and further create a conducive environment for them to relate to and empathise with each other. For instance, a teacher from a study conducted in Uganda revealed:
For the groups, when they come together and they talk about the problems, first, they will know that they are not alone. Other people have the same problem and then they will also learn how they can be able to handle that problem. [They will] learn from the other friends. When this one happens, what do you do? They can also learn how to cope with their problem from their friends (Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021 , p. 5).
In addition to family and peer support, organisations within the community offer outreach programmes to make MH services accessible. These initiatives help link formal MH services with the community. A representative of one of the local schools revealed in a study how local Non-Government Organisations (NGOs) have been helpful to them by providing free services to students: “Local organisations run mental health workshops that are helpful to our students, especially to our schools, who are still struggling with having mental health budgets” (Abdulsalam et al., Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023, p. 8). Culturally appropriate MH services must be ensured through outreach services and appropriate community programmes. These programmes allow adolescents and their families to access the necessary help in their communities, reducing barriers to help-seeking.
Theme 5: Improved service accessibility and affordability
Adolescents showed increased readiness to seek MH help when they could access affordable services. This QES revealed that students showed increased participation in MH programmes, which were located near their schools or communities, when these services had reduced or no associated costs. Research demonstrated that school-based MH programmes significantly affected students’ willingness to pursue MH support (Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021; Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023; Panford-Quainoo et al., Reference Panford-Quainoo, Oppong Asante and Osei-Tutu2024). Adolescents encountered fewer logistical and financial obstacles when MH services were integrated into their school environments. We found that policies developed to increase the funding available for MH initiatives in schools and communities have the potential to significantly improve services. Despite this, a lack of focus on the funding of MH interventions limits their success and hinders progress. However, it has been revealed that communities where the government has deliberately supported MH initiatives have yielded positive MH outcomes.
A viable strategy for improving accessibility and affordability of MH services is through their integration into schools. If MH specialists are integrated into schools, they could provide counselling to the students as well as the community. This approach addresses accessibility issues with on-site services, which are cost-effective and easier to use. A participant from one study emphasised the importance of accessible support within schools, stating, “It’s very necessary… because they don’t have support at home… they need someone or a programme like that to help them.” (Coetzee et al., Reference Coetzee, Gericke, Human, Stallard and Loades2022, p. 193).
Discussion
Adolescent MH help-seeking presents a persistent global public health challenge, with evidence across regions indicating that stigma, limited MHL and structural access constraints impede timely engagement with support services. In high-income settings, barriers often centre on individual attitudes, concerns about confidentiality within formal systems and service accessibility. In contrast, help-seeking behaviours in SSA are more deeply embedded within sociocultural norms, family authority structures, religious interpretations of distress and institutional resource limitations. This QES situates SSA-specific findings within the broader global literature while foregrounding the contextual realities that shape how school-going adolescents interpret distress and navigate formal and informal support offered by or in educational settings or systems.
Our extraction of themes identified six barriers to MH help-seeking, including: pervasive stigma, MHL (knowledge gaps, misconceptions and limited awareness of services), gender differences, privacy, trust and confidentiality concerns, lack of accessibility and availability of services and family and parental disapproval. For clarity, the theme “MHL (knowledge, misconceptions and awareness gaps)” is used consistently throughout this manuscript to capture deficits in symptom recognition, misunderstanding of causes and treatment and limited awareness of available services. The term “low MHL” refers specifically to this broader construct and does not represent a separate barrier. Overall, perceived stigma emerged as the most robust barrier to school-going adolescent help-seeking behaviour, which took the form of social stigma as well as self-stigma and anticipated discrimination (Mfidi Reference Mfidi2017; Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021; Abdulsalam et al., Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023).
The second most prevalent barrier was low MHL, encompassing knowledge deficits, misconceptions, awareness gaps, along with privacy, trust and confidentiality concerns (Meza et al., Reference Meza, Kiche, Soi, Khairuzzaman, Nales, Whetten, Wasonga, Amanya and Dorsey2020; Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021; Coetzee et al., Reference Coetzee, Gericke, Human, Stallard and Loades2022; Panford-Quainoo et al., Reference Panford-Quainoo, Oppong Asante and Osei-Tutu2024; Mushonga et al., Reference Mushonga, Jopling, Glozah, Kamvura, Dodd, Gudyanga, Maramba, Dambayi, Ayuure, Bere, Achana, Owusu, Chibanda, Abas, Weobong and Kumwenda2025). These factors contributed to the delayed recognition of symptoms and a lack of awareness of available services. Boys were less inclined to pursue professional help, as gender norms related to masculinity functioned as an influential factor (Mfidi Reference Mfidi2017; Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021). The fear of confidentiality breaches among professionals further prevented adolescents from seeking help (Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021; Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023; Panford-Quainoo et al., Reference Panford-Quainoo, Oppong Asante and Osei-Tutu2024; Nkosi, Reference Nkosi2025). Adolescents also encountered structural barriers, including geographical distance to services and financial constraints.
On the other hand, key themes involving facilitators of MH help-seeking included school-based MH programmes (Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021), family and community support, peer networks (Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021; Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023; Nkosi, Reference Nkosi2025) and increased MHL through school-based education (Mfidi Reference Mfidi2017; Meza et al., Reference Meza, Kiche, Soi, Khairuzzaman, Nales, Whetten, Wasonga, Amanya and Dorsey2020; Panford-Quainoo et al., Reference Panford-Quainoo, Oppong Asante and Osei-Tutu2024; Mukuna, Reference Mukuna2025). Supportive school environments with trained counsellors and MH education initiatives encourage help-seeking. Family and community support, particularly from parents, teachers and peers, plays a crucial role in promoting MH awareness and normalising help-seeking behaviours.
In a few instances, supportive school MH environments in this QES were linked to policies derived from national MH plans or school health legislation. However, where counselling services and psychoeducational interventions were described, most studies reflected implementation at institutional or externally supported levels rather than through formally operationalised, legally enforced policy mechanisms. This implies that MH policies are often present across SSA contexts but are typically weakly enacted, poorly resourced and fail to regularly adhere to international models (e.g., the World Health Organization Health Promoting Schools framework)(Meza et al., Reference Meza, Kiche, Soi, Khairuzzaman, Nales, Whetten, Wasonga, Amanya and Dorsey2020; Freeman, Reference Freeman2022; Panford-Quainoo et al., Reference Panford-Quainoo, Oppong Asante and Osei-Tutu2024). Therefore, supportive school environments would seem to develop organically via grassroots/local mandates or external intervention, as opposed to operating as structured systems.
However, these facilitators did not operate independently. Improved MHL appeared to strengthen the impact of peer support and school-based services, as adolescents who recognised symptoms were more likely to utilise trusted peers and available professionals. Similarly, supportive school climates amplified the effects of confidentiality assurance, suggesting that structural and relational elements jointly shape help-seeking behaviour.
Although presented as distinct themes for analytical purposes, several of these themes overlap bidirectionally. The facilitators and barriers were not mutually exclusive and affected help-seeking behaviour both positively and negatively. For example, family and parental authority functioned as barriers when imposed through discouragement or negativity towards help-seeking but as facilitators when built on trust and open communication. Similarly, peer relationships, school climate and religious influence changed from risk factors to protective factors based on experiences. These results show that identical structural and sociocultural factors can facilitate or hinder adolescent use of MH care.
Compared to previous reviews conducted in other geographic regions, our findings corroborate previous evidence in low- and middle-income countries (LMICs), where stigma and a lack of knowledge about MH are significant problems (Aguirre Velasco et al., Reference Aguirre Velasco, Cruz, Billings, Jimenez and Rowe2020; Barrow and Thomas, Reference Barrow and Thomas2022; van den et al., Reference van den Broek, Gandhi, Sureshkumar, Prina, Bhatia, Patel, Singla, Velleman, Weiss, Garg, Sequeira, Pusdekar, Jordans and Nadkarni2023). The studies included in this review reaffirm that perceived stigma, fear of discrimination and low awareness of MH services deter adolescents from seeking formal help (Mfidi, Reference Mfidi2017; Meza et al., Reference Meza, Kiche, Soi, Khairuzzaman, Nales, Whetten, Wasonga, Amanya and Dorsey2020; Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021; Abdulsalam et al., Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023). Evidence from qualitative reviews of school-based interventions in high-income settings shows that targeted support often triggers anticipated stigma and peer judgement (Gronholm et al., Reference Gronholm, Nye and Michelson2018). This aligns with the evidence in this synthesis, where fear of labelling and visibility influenced adolescents’ reluctance to seek support.
Similar patterns of stigma and discrimination have been observed in LMICs in Southeast Asia and Latin America in countries such as Haiti, Honduras and Nicaragua (González Moller et al., Reference González Moller, Heaphy and Urrutia Ortiz2021; Javed et al., Reference Javed, Lee, Zakaria, Buenaventura, Cetkovich-Bakmas, Duailibi, Ng, Ramy, Saha, Arifeen, Elorza, Ratnasingham and Azeem2021; Lien et al., Reference Lien, Chen, Cai, Y-H and Liu2024), where traditional beliefs and misinformation about MHPs compounded these barriers (Saade et al., Reference Saade, Parent-Lamarche, Khalaf, Makke and Legg2023). Unlike high-income settings, where MH education and awareness campaigns have played a significant role in promoting help-seeking behaviour (Newlove-Delgado et al., Reference Newlove-Delgado, McManus, Sadler, Thandi, Vizard, Cartwright and Ford2021; Adams et al., Reference Adams, Gringart and Strobel2022; Westberg et al., Reference Westberg, Nyholm, Nygren and Svedberg2022; Habgood et al., Reference Habgood, Gandhi, Smith, Hearps, Hiscock, Oberklaid, Raniti and Darling2024), SSA continues to face challenges in implementing school-based MH interventions because of limited resources, a lack of trained professionals and inadequate policy frameworks (Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021; Brits, Reference Brits2021; Aboagye et al., Reference Aboagye, Ahinkorah, Seidu, Okyere, Frimpong and Kumar2022).
Furthermore, while prior research underscores the significance of implementing professional MH services (Abdulsalam et al., Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023; Adams et al., Reference Adams, Gringart and Strobel2022; Breslin et al., 2022), this QES reveals that adolescents in SSA frequently depend more on informal support systems, such as teachers and religious leaders, rather than on formal MH professionals (Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021; Panford-Quainoo et al., Reference Panford-Quainoo, Oppong Asante and Osei-Tutu2024; Mushonga et al., Reference Mushonga, Jopling, Glozah, Kamvura, Dodd, Gudyanga, Maramba, Dambayi, Ayuure, Bere, Achana, Owusu, Chibanda, Abas, Weobong and Kumwenda2025). This reliance on informal networks is evident in studies such as Carlson et al. (Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021) and Khombo et al. (Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023), in which adolescents reported seeking guidance from family members or school staff rather than engaging with trained professionals. Stigma, low MHL and structural access barriers in high-income contexts have been described elsewhere as barriers to MH help-seeking (Jörns-Presentati et al., Reference Jörns-Presentati, Napp, Dessauvagie, Stein, Jonker, Breet, Charles, Swart, Lahti, Suliman, Jansen, van den, Seedat and Groen2021; Hlophe et al., Reference Hlophe, Tamuzi, Shumba and Nyasulu2023; van den et al., Reference van den Broek, Gandhi, Sureshkumar, Prina, Bhatia, Patel, Singla, Velleman, Weiss, Garg, Sequeira, Pusdekar, Jordans and Nadkarni2023).
However, these barriers operate differently in SSA settings, where help-seeking tends to rely more on family authority figures, religious beliefs and informal or community support systems (Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021; Panford-Quainoo et al., Reference Panford-Quainoo, Oppong Asante and Osei-Tutu2024). MH symptoms in SSA settings are more likely to be attributed to spiritual causes, personal weakness or family dishonour and driven by concealment behaviour (Mayston et al., Reference Mayston, Frissa, Tekola, Hanlon, Prince and Fekadu2020; Asiimwe et al., Reference Asiimwe, Racheal, Dwanyen and Kasujja2023; Hlongwane and Juby, Reference Hlongwane and Juby2023). In higher-income settings, findings on adolescents’ help-seeking have more commonly pointed to individual-level attitudinal barriers or perceptions of dissatisfaction with services (Gulliver et al., Reference Gulliver, Griffiths and Christensen2010; Radez et al., Reference Radez, Reardon, Creswell, Lawrence, Evdoka-Burton and Waite2021), rather than contextualised explanations of distress shaped by culture or community. Findings from SSA expand upon previous theoretical models of help-seeking globally by highlighting the embeddedness of help-seeking behaviour within adolescents’ families, cultural backgrounds and religious practices (Rickwood and Thomas, Reference Rickwood and Thomas2012). This signals a need for global MH theory to expand upon individualistic, cognition-based models of help-seeking behaviour to better integrate structural and sociocultural barriers.
This finding contrasts with findings from high-income countries, where adolescents are more likely to access formal psychological support within schools or community-based services (Rickwood and Thomas, Reference Rickwood and Thomas2012; Heerde and Hemphill, Reference Heerde and Hemphill2018; Lauzier-Jobin and Houle, Reference Lauzier-Jobin and Houle2022). The preference for informal networks suggests that interventions in SSA should leverage these existing support structures while simultaneously strengthening access to professional services through policy changes and infrastructure development.
Strengths and limitations
There are a number of notable strengths associated with this QES. First, we implemented a systematic and rigorous search strategy, and multiple reviewers independently conducted both the study selection and data extraction while complying with predefined inclusion and exclusion criteria. The study performed a critical appraisal and thematic synthesis according to established methodologies, which maintained methodological rigour.
Despite its strengths, the breadth of perspectives captured in the findings remains limited, as only eight qualitative studies met the inclusion requirements. Research shows a high concentration of studies in South Africa and West Africa, which may limit the generalisability of findings to other SSA regions. Most of the findings depended on barriers reported by individuals, which might obscure true institutional and systemic limitations. In addition, our review only included studies published in English, which again may limit generalisability. Future studies should focus on conducting qualitative research in regions that lack representation while examining structural and policy-level influences on adolescent MH service use.
Implications for future research and policy
The findings of this QES have critical implications for research, policy and practice. From a research perspective, future research should include longitudinal studies designed to track how adolescent help-seeking behaviours evolve over time (Eigenhuis et al., Reference Eigenhuis, Waumans, Muntingh, Westerman, van Meijel, Batelaan and van Balkom2021; Abdulsalam et al., Reference Abdulsalam, Ahmed Tharbe and Mohd Jaladin2023). Research should further investigate the sustained effects of current MH interventions (van den Broek et al., Reference van den Broek, Gandhi, Sureshkumar, Prina, Bhatia, Patel, Singla, Velleman, Weiss, Garg, Sequeira, Pusdekar, Jordans and Nadkarni2023; Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021) while evaluating new methods that aim to improve adolescent engagement with MH services (Barrow and Thomas, Reference Barrow and Thomas2022; Mabrouk et al., Reference Mabrouk, Mbithi, Chongwo, Too, Sarki, Namuguzi, Atukwatse, Ssewanyana and Abubakar2022). Research urgently requires randomised controlled trials (RCTs) to examine specific factors impacting help-seeking behaviour, especially in settings that remain unexplored (O’Dea et al., Reference O’Dea, Han, Batterham, Achilles, Calear, Werner-Seidler, Parker, Shand and Christensen2020; Radez et al., Reference Radez, Reardon, Creswell, Lawrence, Evdoka-Burton and Waite2021; O’Neill et al., Reference O’Neill, Stapley, Rehman and Humphrey2023).
Policymakers must prioritise the integration of MHL into school curricula within the broader education system (Addy et al., Reference Addy, Agbozo, Runge-Ranzinger and Grys2021; Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021; Khombo et al., Reference Khombo, Khombo, Stoddart, Sifelani and Sibanda2023). This approach requires the creation and dissemination of educational materials suitable for adolescents to learn about identifying MHPs and developing stress management skills while understanding how to access support systems (Mushonga et al., Reference Mushonga, Jopling, Glozah, Kamvura, Dodd, Gudyanga, Maramba, Dambayi, Ayuure, Bere, Achana, Owusu, Chibanda, Abas, Weobong and Kumwenda2025; Nkosi, Reference Nkosi2025). School-based MH services, like counselling, must be implemented so adolescents can obtain confidential treatment in a familiar setting (Azfredrick, Reference Azfredrick2015; Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021). This proposed service model holds significant potential for rural and underserved areas due to the current shortage of specialised care options. Achieving this goal requires essential investment in school counsellor training programmes and infrastructure development (Azfredrick, Reference Azfredrick2015; Panford-Quainoo et al., Reference Panford-Quainoo, Oppong Asante and Osei-Tutu2024).
From a practice standpoint, school MH professionals must focus on building trust and maintaining confidentiality in their practice with adolescents (Carlson et al., Reference Carlson, Namy, Nakuti, Mufson, Ikenberg, Musoni, Hopson, Anton-Erxleben, Naker and Wainberg2021; Yao et al., Reference Yao, Li, Wang and Hui2021). Establishing clear communication about privacy and consent can alleviate the fear of seeking help for MHPs (Yao et al., Reference Yao, Li, Wang and Hui2021; Haraldsson et al., Reference Haraldsson, Pingel, Nordgren, Johnsson, Kristiansson and Tindberg2022). Schools and communities should also collaborate to actively combat MH stigma through awareness campaigns that aim to normalise seeking support (Chinawa et al., Reference Chinawa, Manyike, Obu, Aronu, Odutola and Chinawa2015; Bella-Awusah et al., Reference Bella-Awusah, Ani, Ajuwon and Omigbodun2019; Cefai et al., Reference Cefai, Simões and Caravita2021). A multi-sectoral approach involving healthcare providers, educators and policymakers is essential for creating a holistic, adolescent-centred support system that addresses the full spectrum of MH needs (van den Broek et al., Reference van den Broek, Gandhi, Sureshkumar, Prina, Bhatia, Patel, Singla, Velleman, Weiss, Garg, Sequeira, Pusdekar, Jordans and Nadkarni2023; Iswanto and Ayubi, Reference Iswanto and Ayubi2023; Lien et al., Reference Lien, Chen, Cai, Y-H and Liu2024).
Conclusion
Overall, our findings revealed that schools offer a powerful yet often overlooked platform for the cost-effective adolescent MH services. The synthesis further provides insight into adolescents’ experiences and barriers to develop foundational guidance for context-sensitive and inclusive school MH programmes. The data demonstrate a pressing requirement for qualitative research which takes context into account to direct policy and practice while transforming schools into accessible hubs for MHL, early intervention and normalisation of help-seeking for MHPs.
In addition to institutional reforms, school-based MH programmes in SSA should also be mindful of the social context in which adolescents reside. Aspects that may influence whether adolescents seek help include parental hierarchy and authority, community attitudes about sharing problems and spiritual beliefs about mental illness. Behavioural interventions that do not consider these relational factors may be ineffective if adolescents are unable or unwilling to access help. Culturally appropriate engagement efforts at school and community levels, such as family sensitisation and engaging religious/community leaders, could build goodwill towards school-based MH programmes.
Notably, the QES reveals significant gaps in our knowledge of adolescent help-seeking behaviours within school environments in SSA. Quantitative studies dominate the field, limiting our understanding of adolescents lived experiences and help-seeking behaviours within school settings. While some subgroups, such as pregnant adolescents or those with substance use issues, have received focused attention, the broader spectrum of adolescent voices in SSA remains underexplored. Future research should further integrate qualitative methods, which are sensitive to context and accurately capture the range of school environments, to examine MH help-seeking in SSA adolescents. Strengthening school-based MH systems in SSA, therefore, represents not only a response to unmet need, but also a strategic investment in the long-term social, educational and psychological well-being of future generations.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10250.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/gmh.2026.10250.
Data availability statement
Data sharing does not apply to this article as no new data were created or analysed.
Acknowledgements
The authors gratefully acknowledge the University of Dundee Africa Doctoral Fellowship Scheme (UoD-ADFS) for providing PhD funding support for the lead author (AIK).
Author contribution
The authors’ contributions to this QES reflect their collective expertise and collaboration.
Adrian Ivan Kakinda conceptualised the review, led the article screening, conducted the formal analysis, synthesised the data and prepared the manuscript draft. Tim J. Croudace supervised the methodological framework, contributed to the article screening and guided the analysis. Rachel A. Plouffe supervised the review, contributed to article screening, ensured analytical rigour and edited the manuscript. Kennedy Amone-P’Olak supervised the study, participated in article screening and provided contextual insights on adolescent mental health in Sub-Saharan Africa.
Financial support
This work was supported by the University of Dundee Africa Doctoral Fellowship Scheme (ADFS) studentship.
Competing interests
The authors declare no conflicts of interest.
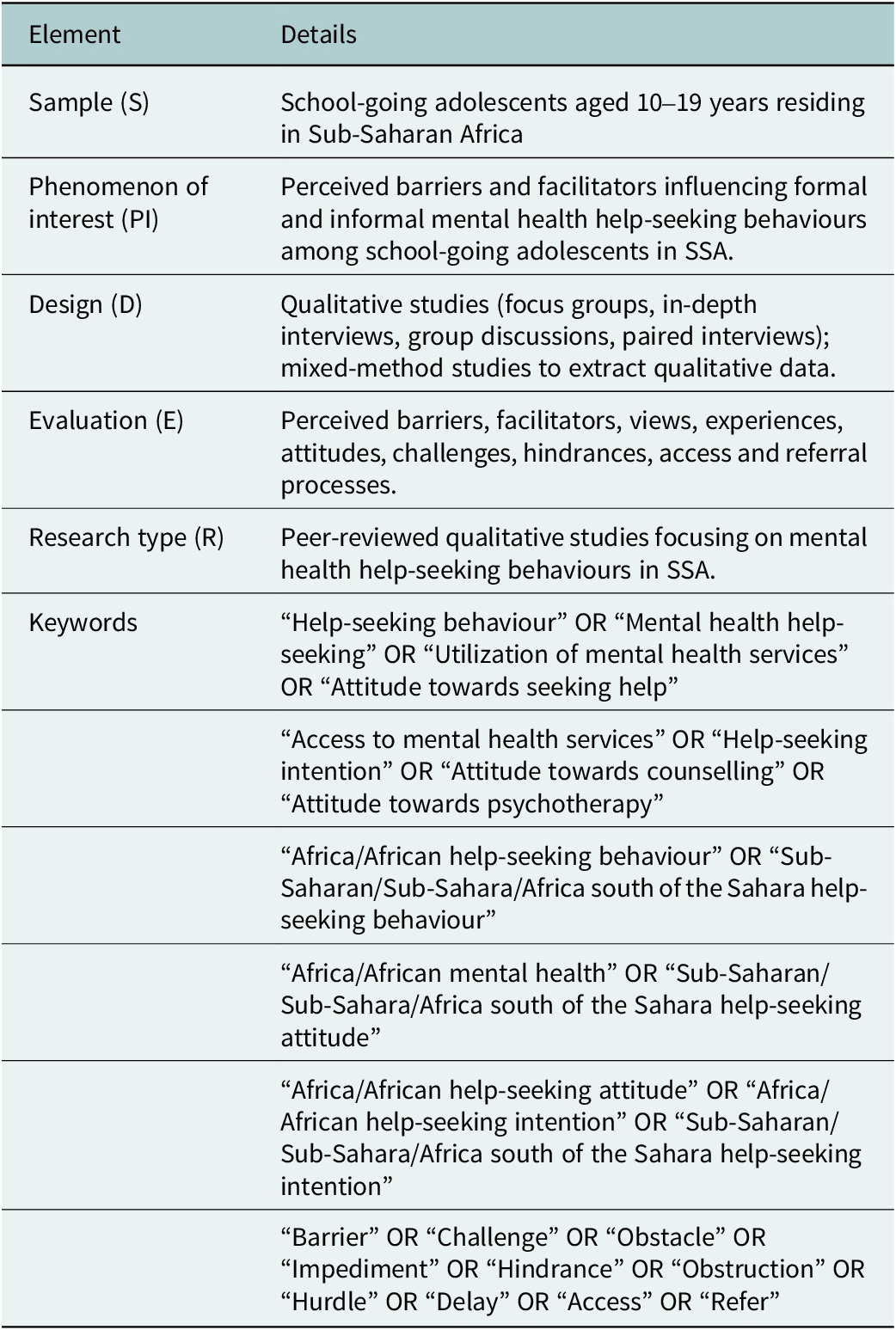
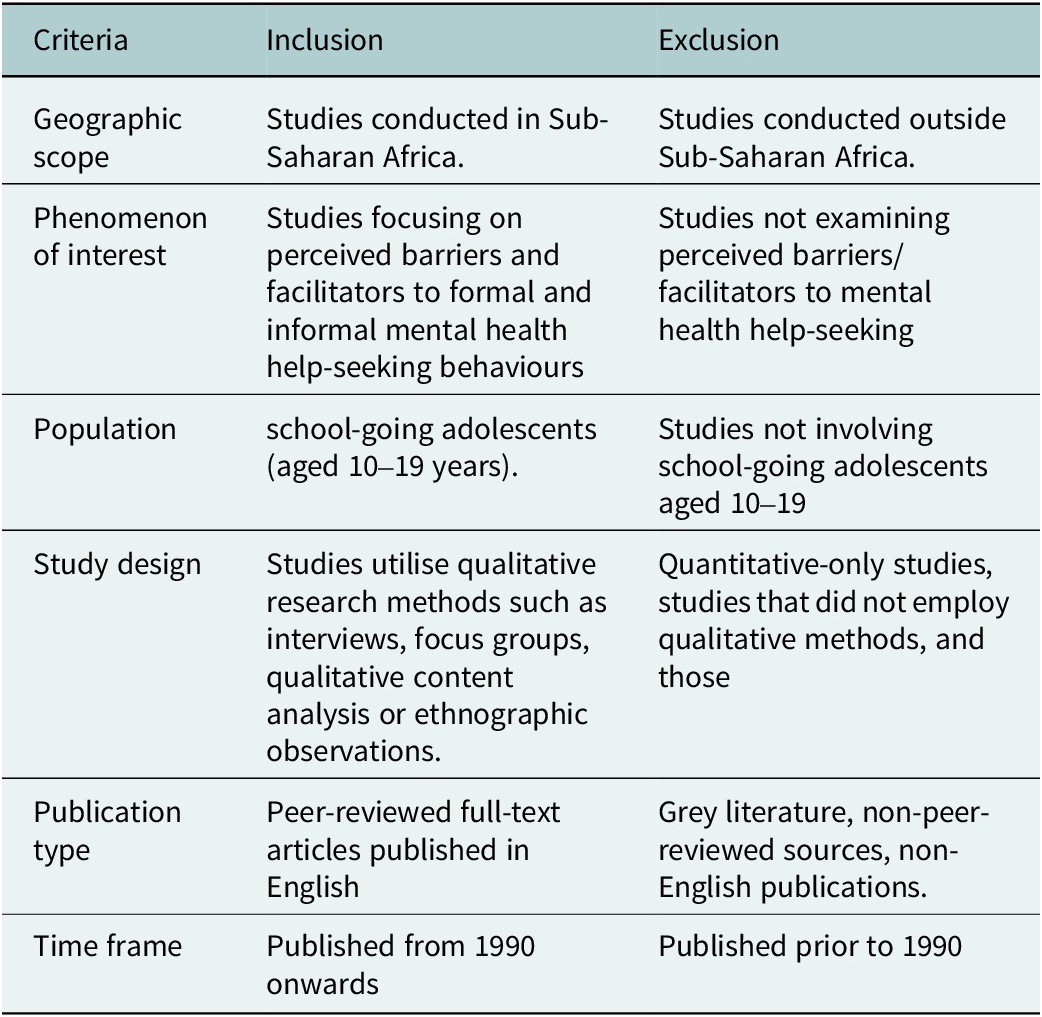
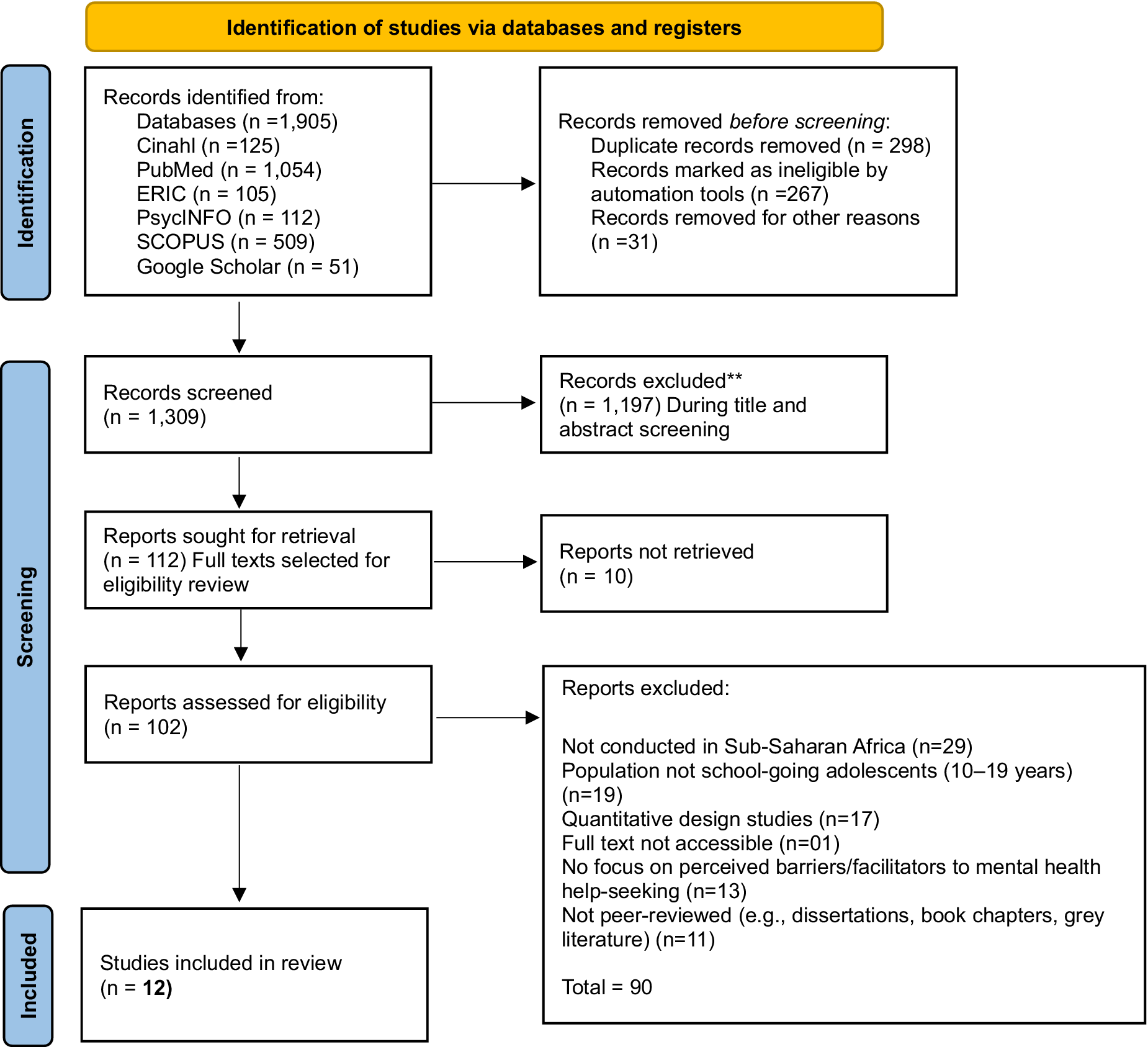
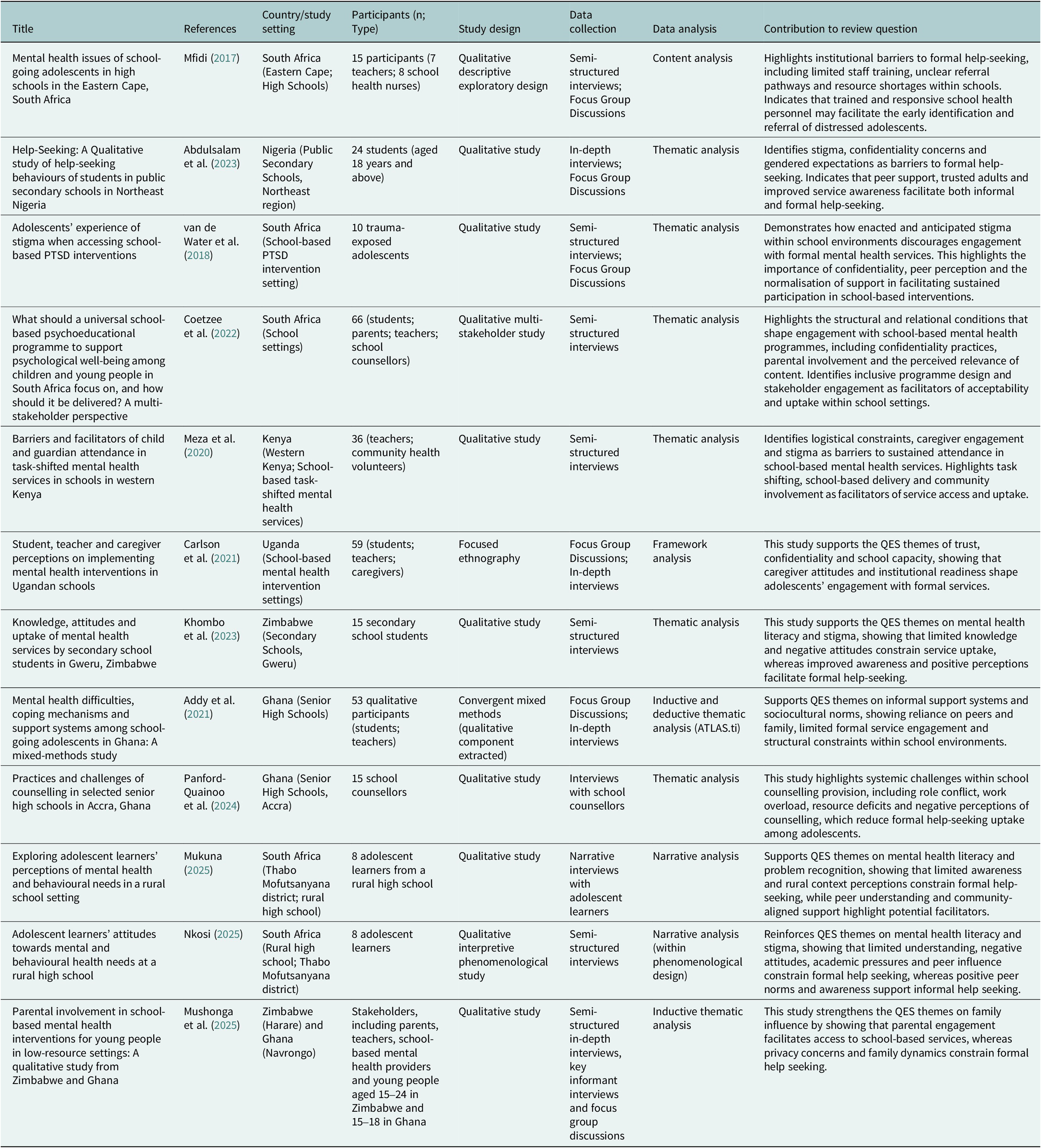
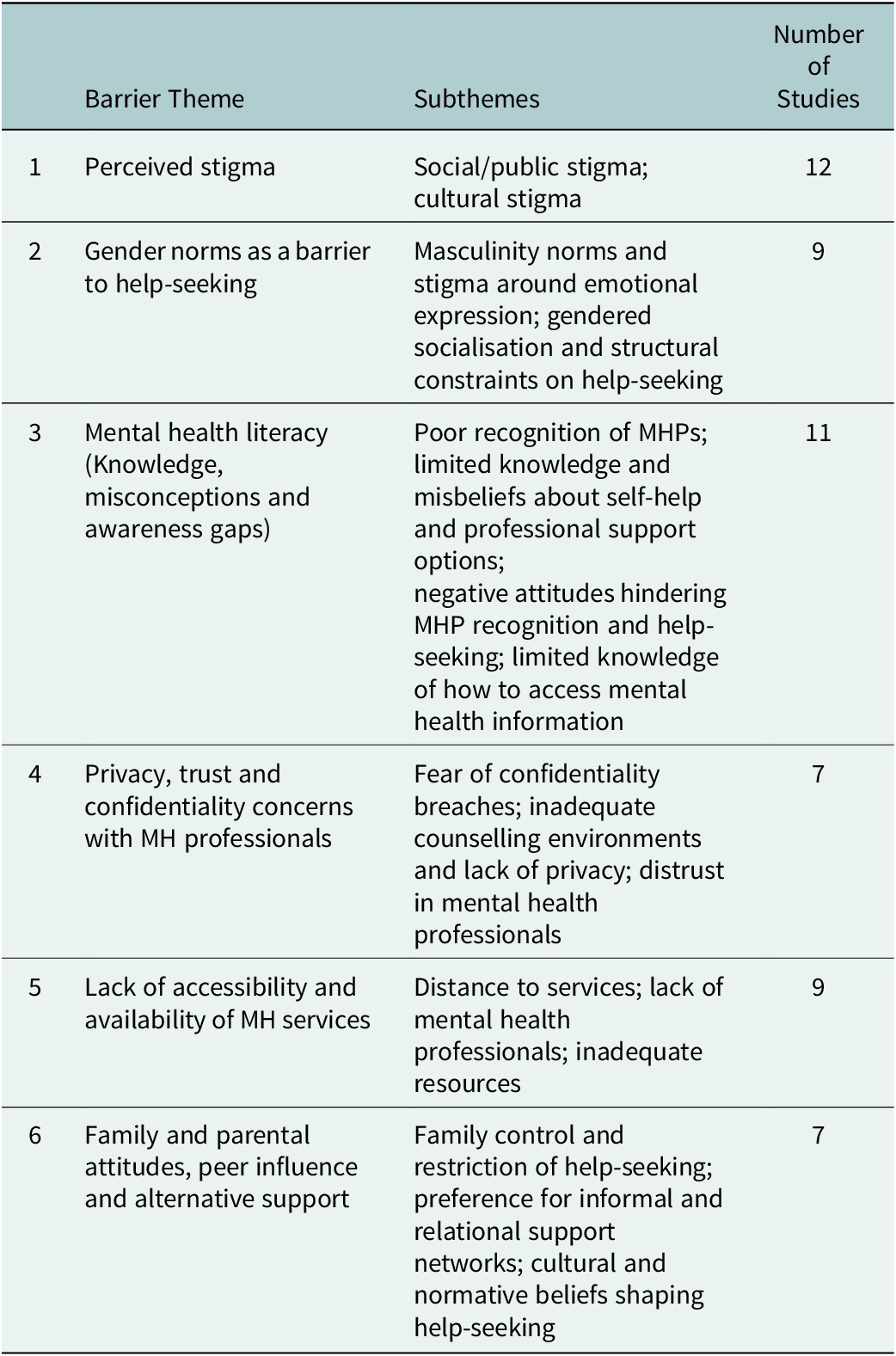
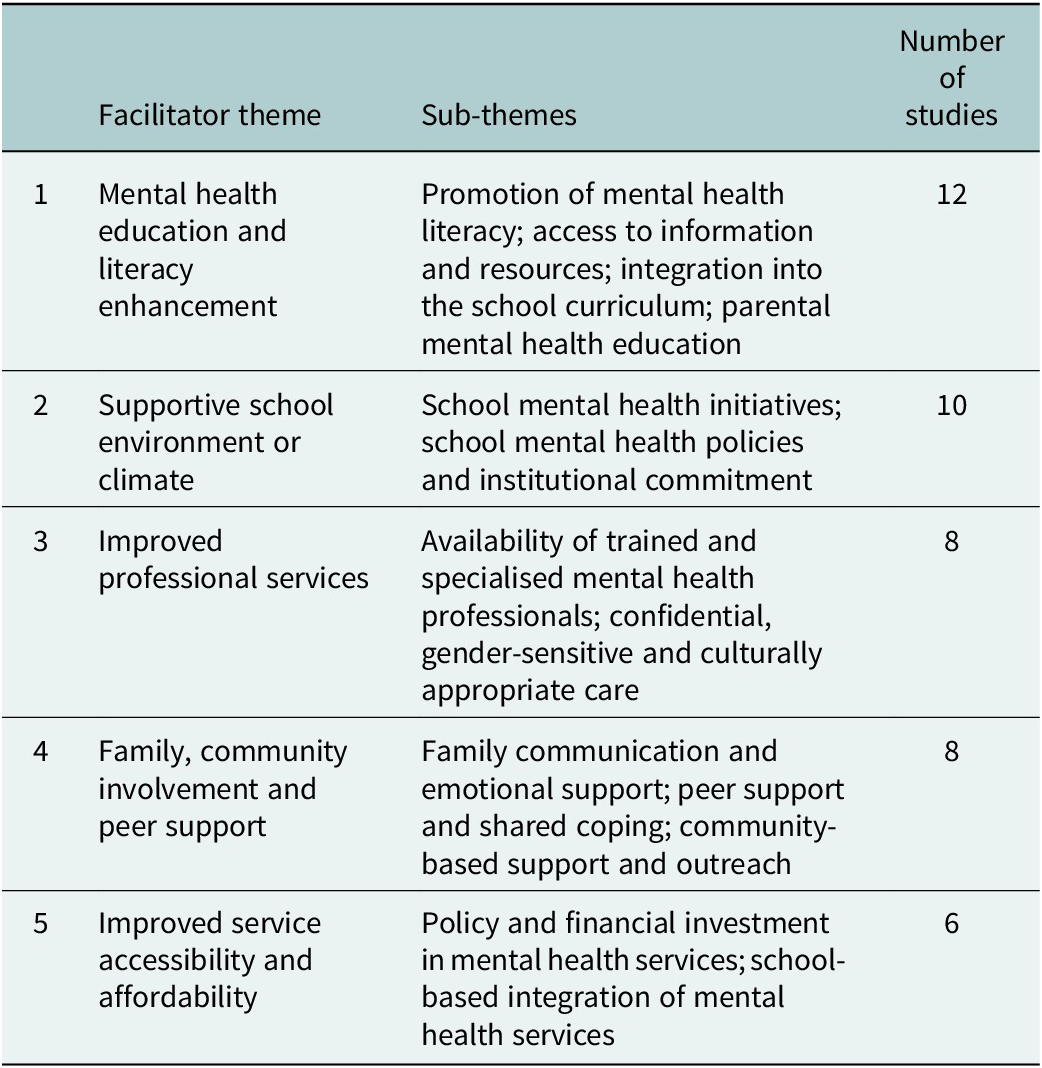



 Open access
Open access
Comments
Adrian Ivan Kakinda
PhD Candidate, Psychology
School of Humanities, Social Sciences and Law
University of Dundee
Nethergate, Dundee DD1 4HN, Scotland
2612662@dundee.ac.uk
08/01/2026
Professor Judy Bass
Editor-in-Chief
Cambridge Prisms: Global Mental Health
Johns Hopkins Bloomberg School of Public Health in Maryland, USA,
Dear Prof. Bass,
I am pleased to submit the manuscript titled “Barriers and Facilitators of mental health help-seeking behaviours among school-going adolescents in Sub-Saharan Africa: A qualitative evidence synthesis” for consideration in Cambridge Prisms: Global Mental Health.
This manuscript presents a rigorous qualitative evidence synthesis of mental health help-seeking behaviours among school-going adolescents in Sub-Saharan Africa. Mental health challenges among adolescents remain a neglected priority in the region, despite growing demand for contextually grounded interventions. Our synthesis integrates findings from eight qualitative studies conducted across multiple Sub-Saharan countries, using thematic synthesis to identify common barriers, cultural dynamics, and pathways influencing school going adolescents’ willingness and ability to seek help for mental health problems.
The study addresses a pressing gap in global adolescent mental health literature by focusing on underrepresented populations. It offers analytical clarity on the role of stigma, informal care systems, gendered perceptions of vulnerability, and structural school-level influences. Our synthesis contributes to knowledge translation by highlighting locally informed strategies for improving adolescent engagement with mental health support systems.
We believe Cambridge Prisms: Global Mental Health is the most appropriate venue for this work given its global readership, commitment to evidence-based psychological science, and relevance to both clinical and public health practice. Our manuscript presents a timely and policy-relevant contribution to ongoing conversations on mental health equity and access in low-resource settings.
The manuscript has not been published or submitted elsewhere. All authors have reviewed and approved the final version and agree to its submission to Cambridge Prisms: Global Mental Health. There are no conflicts of interest to declare.
Thank you for considering our work. We welcome the opportunity for it to contribute to the critical discourse on adolescent mental health and help-seeking.
Sincerely,
Adrian Ivan Kakinda
PhD Candidate, Psychology
School of Humanities, Social Sciences and Law
University of Dundee
(on behalf of all co-authors)