


Introduction
Parkinson’s disease (PD) is a progressive neurodegenerative disorder diagnosed based on motor symptoms like bradykinesia, resting tremor, and rigidity (Hussein et al. Reference Hussein, Guevara, Del Valle, Gupta, Benson and Huntley2023). Of note, over 30% of people living with PD experience anxiety, 35% depression, and up to 50% report sleep disturbances (Saadat et al. Reference Saadat, Faramarzi, Salimkhani and Khafri2020; Szatmá et al. Reference Szatmá, Ajtay, Oberfrank, zs Dobi, niel Bereczki and Szentágothai2020). PD is part of the Lewy body disease (LBD) spectrum, including cognitive disorders such as mild cognitive impairment due to PD (PD-MCI), dementia in PD (PDD), and dementia with Lewy bodies (DLB). The cognitive, behavioural and psychological aspects of the LBD spectrum remain often undiagnosed, even though they are linked to negative outcomes like longer hospital stays, poorer functional outcomes, higher institutionalisation rates, and increased mortality (Borda et al. Reference Borda, Brønnick, Garcia-Cifuentes, Jaramillo-Jimenez, Reyes-Ortiz, Patricio-Baldera, Ocampo-Chaparro, Baena, Cano and Lopera2023; Spears et al. Reference Spears, Besharat, Monari, Martinez-Ramirez, Almeida and Armstrong2019). Up to 48% of respondents in a survey considered non-motor symptoms more detrimental to their own and their care partner’s quality of life than motor symptoms (Hermanowicz et al. Reference Hermanowicz, Jones and Hauser2019). Addressing this, health services should enable access for service users with PD-related neuropsychiatric and cognitive difficulties to specialised mental and cognitive health diagnostic and post-diagnostic care (Carney Reference Carney2018). Such services should ideally relate to memory services for comprehensive care of cognitive impairment and dementia.
While no prevalence studies have been conducted specifically in the Irish context, Parkinson’s Ireland estimates that approximately 18,000 individuals are living with PD in the Republic of Ireland (Parkinson’s Association of Ireland n.d.). Similarly, the Alzheimer’s Society of Ireland reports that around 64,000 people are living with dementia (Alzheimer’s Society of Ireland 2023) and LBD accounts for approximately 10–25% of all dementia cases in Ireland (Alzheimer’s Society of Ireland 2024). Thus, between 6400 and 16,000 individuals in Ireland may be affected by LBD. Consequently, there is a substantial need for support for cognitive, behavioural and psychological symptoms developing in the context of PD. Presently, there is limited integration of mental and cognitive health services for individuals and their caregivers.
In 2018, the UK’s All Party Parliamentary Group (APPG) on mental health in PD highlighted the shortage of mental health services for people with PD, emphasising difficulties in accessing psychiatric care, often provided separately. APPG testimonials described experiences with mental health services as ‘poor’ and ‘limited’. A comparable situation exists in Ireland, evident in a survey of 1,400+ people with PD, where access to cognitive or mental health services was not mentioned, and only 20% of individuals with PD had access to the services provided by a PD nurse specialist (O Shea et al. Reference O’ Shea, Rukundo, Foley, Wilkinson and Timmons2024). Satisfaction was lowest for nonmotor symptom support, especially psychological support. A European survey across 25 countries showed limited cognitive and mental health support for PD patients, with physiotherapy (68%), PD nurse specialist (45%), dietetics (28%), and counselling (38%) being the main non-motor services which were considered alongside standard PD care focused on motor symptoms (Bloem and Stocchi Reference Bloem and Stocchi2012).
In response to the UK APPG findings emphasising the need for comprehensive, multidisciplinary support for Parkinson’s-related disorders, the ‘Mind and Movement’ (M&M) Clinic at St James’s Hospital in Dublin was established in 2020. The clinic aims to address the cognitive, behavioural, and psychological needs of patients from both the Parkinson’s and memory clinics. While both clinics incorporated elements of multidisciplinary practice, the specific needs of individuals with movement-related symptoms in the memory clinic, or with cognitive, behavioural, and/or psychological symptoms in the Parkinson’s clinic, were not fully met, leading patients and their families to feel underserved. Additionally, there was a concern that the diagnosis of PD-MCI, PDD and DLB was potentially under-recognised due to a focus on motor symptoms and Alzheimer-like cognitive symptoms in the Parkinson’s and memory clinics, respectively, along with a lack of dedicated subspecialty expertise in LBD.
Here, we present the sociodemographic and cognitive-neuropsychiatric profiles, referral patterns, and clinical services provided to the first 99 patients at the newly established M&M clinic at St James’s Hospital. The clinic integrates Memory Assessment Service and Parkinson’s disease service, combining medical gerontology and neurology with mental and cognitive health. Gaining insights into the (i) demographic- and (ii) clinical characteristics of the first users of a new clinical service, (iii) the symptoms that prompted their referral, (iv) the components of the diagnostic workup and the therapeutic plans that have been developed, as well as (v) the patient care pathway to and beyond the new service form a solid foundation for identifying strengths, gaps, and areas for improvement. To this end, the present study employed descriptive and between-group analyses to characterise demographic, clinical, cognitive, neuropsychiatric, pharmacological, and care pathway features across diagnostic subgroups. Such data are essential to inform ongoing development, resource allocation, and policy decisions. In the context of novel or specialised services addressing under-recognised conditions, these findings may provide foundational evidence to support scalability and sustainability.
Methods
Study design
This study employed a retrospective study design conducted as part of a service improvement project at the M&M clinic during the period 2020–2023.
Setting
The M&M clinic is led by a geriatric psychiatrist specialising in the cognitive, behavioural and psychological aspects of Parkinson ’s-related disorders, with support from a junior doctor. All patients undergo a standard ‘new patient’ or ‘follow-up’ neuropsychiatric assessment, either by the geriatric psychiatrist or the junior doctor who is supervised by the former. New assessments include a comprehensive physical, cognitive, and mental state examination, screening neuropsychological evaluation, care partner burden checklist, and a review of neuroimaging and relevant investigations. Multidisciplinary support derives from specific referrals to linked services, arising from the neuropsychiatric assessment. This includes professionals in the memory clinic (neuropsychologist for in-depth assessment, medical social worker, speech and language therapist), the Parkinson’s Clinic (nurse specialist, occupational therapist, physiotherapist), and the broader medical gerontology service (social prescriber, counselling psychologist). These medical and non-medical professionals are involved in the diagnostic workup and/or the post-diagnostic care of patients based on their individual needs, as clinically indicated. Two clinics operate weekly, one for new assessments and one for follow-ups. All cases are discussed at the weekly multidisciplinary team meetings of the Parkinson’s Clinic or the Memory Clinic or at both, depending on the origin of each referral and/or the individual post-diagnostic care needs of each user. Both team meetings take place once per week. Patients and the physician who referred them to the M&M Clinic receive a report after the completion of the diagnostic workup with the assessment findings and care recommendations. Semi-annual follow-ups resemble the initial assessment in thoroughness, and a report is sent to both the referring physician and the patient. Follow-up assessments taking place at shorter intervals commonly include a pragmatic review of changes in the physical, cognitive, and mental state of the patient and their care plan. At such follow-ups, if changes in the care plan are recommended and/or the patient is referred to other services or specialities, reports are sent to both the patient and the physician who referred them to the Clinic.
The M&M Clinic operates at St James’s Hospital, a 1,028-bedded hospital in Dublin, and serves the people of the south inner-city Dublin. This densely populated catchment has double the Irish national average of people aged 65 and above. Of note, the Parkinson’s Clinic is catchment area-based, while the memory Clinic is not. Based on clinic activity from 2021 to mid-2025, the Parkinson’s (Neurology) service receives an average of approximately 75 new and 320 return referrals per year, totalling around 395 referrals annually. The Memory (Geriatric) service receives an average of 50 new and 150 return referrals per year, totalling approximately 200 referrals annually.
Participants
Participants’ data were retrospectively extracted from clinic proformas and electronic and paper medical records for the first 99 consecutive individuals referred to the M&M service. Of these, 93 individuals were included in the current analyses and classified into two diagnostic groups: (1) the LBD group, including individuals with DLB and PDD (n = 48), and (2) the non-dementia group, including individuals with PD-MCI or cognitively unimpaired PD (n = 45). Specifically, the LBD group comprised 37 individuals with DLB and 11 with PDD, while the non-dementia group comprised 36 individuals with PD-MCI and 9 with cognitively unimpaired PD.
Diagnostic criteria
Diagnostic classifications were established according to international diagnostic criteria. DLB was diagnosed according to the 2017 Fourth Consensus Report of the DLB Consortium (McKeith et al. Reference McKeith, Boeve, Dickson, Halliday, Taylor, Weintraub, Aarsland, Galvin, Attems, Ballard, Bayston, Beach, Blanc, Bohnen, Bonanni, Bras, Brundin, Burn, Chen-Plotkin, Duda, El-Agnaf, Feldman, Ferman, ffytche, Fujishiro, Galasko, Goldman, Gomperts, Graff-Radford, Honig, Iranzo, Kantarci, Kaufer, Kukull, Lee, Leverenz, Lewis, Lippa, Lunde, Masellis, Masliah, McLean, Mollenhauer, Montine, Moreno, Mori, Murray, O’Brien, Orimo, Postuma, Ramaswamy, Ross, Salmon, Singleton, Taylor, Thomas, Tiraboschi, Toledo, Trojanowski, Tsuang, Walker, Yamada and Kosaka2017). PDD was diagnosed in line with the Movement Disorder Society clinical criteria for dementia associated with Parkinson’s disease (Emre et al. Reference Emre, Aarsland, Brown, Burn, Duyckaerts, Mizuno, Broe, Cummings, Dickson, Gauthier, Goldman, Goetz, Korczyn, Lees, Levy, Litvan, McKeith, Olanow, Poewe, Quinn, Sampaio, Tolosa and Dubois2007). PD-MCI was defined using the Movement Disorder Society Task Force criteria (Litvan et al. Reference Litvan, Goldman, Tröster, Schmand, Weintraub, Petersen, Mollenhauer, Adler, Marder, Williams‐Gray, Aarsland, Kulisevsky, Rodriguez‐Oroz, Burn, Barker and Emre2012). Diagnostic groups classification was also supported by cognitive assessment, including ACE-III Addenbrooke’s Cognitive Examination III (Hsieh et al. Reference Hsieh, Schubert, Hoon, Mioshi and Hodges2013).
PD without cognitive impairment was identified, where a diagnosis of Parkinson’s disease was present, and no cognitive deficits were reported or detected clinically. All diagnoses were supported by neuropsychiatric assessment, cognitive evaluation using the ACE-III, and multidisciplinary case review to ensure diagnostic accuracy.
Diagnostic reclassification following M&M clinic assessment
Of the 60 patients referred to the M&M Clinic with a diagnosis of PD, final diagnoses following assessment included PD-MCI (n = 33), PDD (n = 8), DLB (n = 9), MCI-AD (n = 1), and cognitively unimpaired PD (n = 9). Of the three patients referred with a diagnosis of PDD, one was reclassified as PD-MCI. Among the 29 patients referred with a diagnosis of DLB, two were reclassified as PD-MCI and one as PDD.
Data capture and analysis
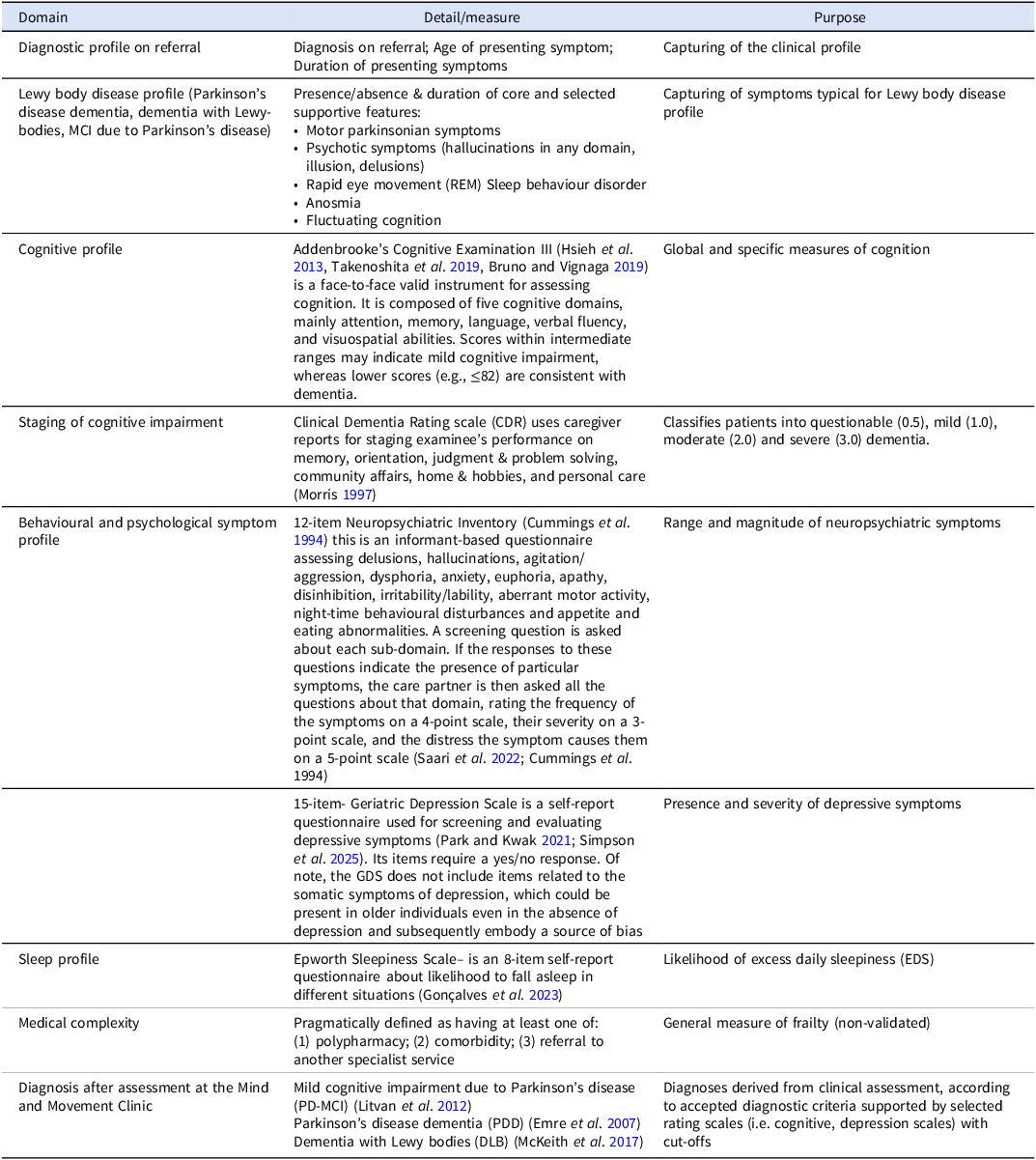
To ensure a comprehensive cognitive-neuropsychiatric assessment, the Clinic proforma was based on the domains outlined in the consensus set of outcomes for PD (De Roos et al. Reference de Roos, Bloem, Kelley, Antonini, Dodel, Hagell, Marras, Martinez-Martin, Mehta, Odin, Chaudhuri, Weintraub, Wilson and Uitti2017) developed in collaboration with the International Consortium for Health Outcomes Measurement (ICHOM). These outcomes were designed to be pragmatic and to address the range of motor and non-motor aspects of PD; however, since the Clinic’s focus was on cognitive, behavioural and psychological symptoms, we expanded the assessment tools used to capture these aspects of the clinical phenotypes. The domains that were captured included (1) service user profile, i.e. cognitive and psychiatric symptoms/functioning, non-motor functioning, motor functioning, demographic characteristics and diagnostic criteria for PD-related cognitive, behavioural and psychological syndromes; (2) referral diagnosis and diagnosis made following the M&M assessment. The tools to assess these domains are outlined in Table 1. Next, we recorded the therapeutic plan agreed upon during the assessment, noting both pharmacologic and non-pharmacologic interventions. Finally, to ascertain the care pathway to and beyond the clinic, we captured the referral source and reason for referral. Data were inconsistently captured due to the pragmatic nature of the report and the real-life setting of the clinic.
Domains and tools used to assess the clinical profiles of the first 99 patients of the Mind and Movement clinic

Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics version 30. Analyses focused on comparing demographic, clinical, cognitive and neuropsychiatric characteristics across Lewy body–associated parkinsonian disorders, including PD with normal cognition, PD-MCI, PDD, and DLB. These groups were analysed either as three diagnostic categories (PD-MCI, PDD and DLB) or dichotomised into non-dementia PD (i.e., PD with or without MCI) vs. LBD (i.e., PDD/DLB).
Continuous variables were evaluated for normality using histograms, Q–Q plots and the Shapiro–Wilk test. Homogeneity of variance was assessed with Levene’s test. Parametric methods were applied only when both assumptions were met; otherwise, non-parametric procedures were used.
Between-group comparisons of continuous variables were conducted using independent-samples t-tests when comparing two groups and one-way ANOVA when comparing three groups. For significant omnibus ANOVA effects, Bonferroni-corrected post-hoc tests were performed. For continuous or ordinal variables violating normality assumptions (e.g., ACE-III domain scores), Mann–Whitney U tests (two groups) or Kruskal–Wallis H tests (three groups) were applied, followed by Bonferroni-adjusted post-hoc pairwise comparisons as appropriate.
Categorical variables – including gender, medication use and prevalence of clinically significant neuropsychiatric symptoms – were analysed using χ2 (chi-square) tests when expected frequencies permitted; otherwise, Fisher’s Exact Test was used.
Statistical significance was defined as two-tailed p < 0.05. Test statistics, degrees of freedom, and adjusted p-values (where applicable) are reported within each table. Confidence intervals and effect size estimates are presented for parametric outcomes when suitable. No additional corrections for multiple testing were applied beyond post-hoc adjustments after significant omnibus effects.
Results
Demographics and medication characteristics of individuals with Lewy body dementia (LBD) (i.e., PDD/DLB) versus Non-LBD dementia (i.e., PD/PD-MCI)
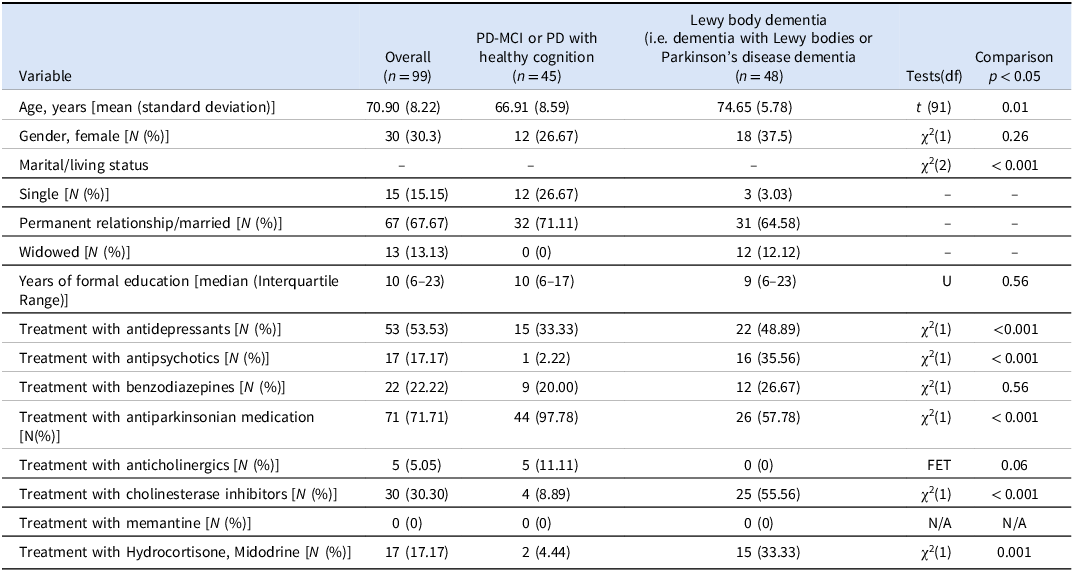
Demographic and medication characteristics for the first 99 consecutive referrals to the M&M Clinic are presented in Table 2. For the current analyses, 93 individuals were classified into two diagnostic groups: (1) the LBD group, including individuals with DLB and PDD (n = 48), and (2) the non-LBD dementia group, including individuals with PD-MCI or PD with healthy cognition (n = 45).
Demographic and medication profile of individuals with Lewy body dementia (LBD) (i.e., PDD/DLB) versus non-LBD dementia (i.e., PD/PD-MCI)

Note: All statistical analyses compare participants with dementia due to LBD (i.e., DLB and PDD) versus those without dementia (i.e., PD and PD-MCI). Continuous variables were analysed using parametric (Independent samples t-test; t) or non-parametric (Mann–Whitney U test; U) tests depending on distribution characteristics. Categorical variables were analysed using Chi-square tests (χ2) or Fisher’s Exact Test (FET) when expected cell counts were insufficient. Test statistics and degrees of freedom (df), when applicable, are reported in the table. N/A = not applicable; statistical comparison could not be performed as no cases were observed in any group.p < 0.05 was considered statistically significant.
A small subset of referrals (n = 6) received alternative diagnoses – Alzheimer’s disease pathology (n = 3), multisystem atrophy (n = 1), progressive supranuclear palsy (n = 1), or vascular mild cognitive impairment (n = 1). Although these individuals are included in the total sample (n = 99), they were not considered in the two-group statistical comparison presented in Table 2.
Across the full cohort, the mean age was 70.90 years (SD = 8.22). Individuals with LBD were significantly older than those with PD-MCI/PD (74.65 ± 5.78 vs 66.91 ± 8.59 years; t (91) = 2.45, p = .01).
Overall, 30.3% of the total cohort were female, with no significant sex-distribution difference between groups [χ2(1) = 1.25, p = 0.26]. Most individuals lived with a spouse or partner (67.67%), with living status distributions differing significantly across diagnostic groups [χ2(2) = 17.38, p < 0.001]. Years of formal education did not differ significantly between groups (median = 10 years, IQR 6–23) (U = 546.0, Z = 0.59, p = 0.56).
Regarding medication exposure, antidepressant use was present in 53.5% of the total sample, with a significantly higher prevalence among individuals with LBD than among those without dementia [χ2(1) = 11.67, p = 0.001]. Antipsychotic use was reported in 17.17% of the full sample and occurred almost exclusively in those with LBD [χ2(1) = 15.05, p < 0.001]. Benzodiazepine use was documented in 22.22% of the cohort, with similar proportions across groups [χ2(1) = 0.33, p = 0.56]. Use of anti-Parkinsonian medication was common (71.71%), with significantly greater frequency in individuals with PD-MCI/PD than in those with LBD [χ2(1) = 23.73, p < 0.001]. Anticholinergic prescriptions were uncommon, occurring only in those without LBD (11.11%) (FET, p = 0.06). Cholinesterase inhibitor prescriptions were documented in 30.30% of the full sample and most frequently in the LBD group [χ2(1) = 20.19, p < 0.001]. Hydrocortisone or midodrine was prescribed in 17.17% of the cohort (4.44% without LBD; 33.33% LBD; [χ2(1) = 11.17, p = 0.001].
No participants were receiving memantine at the time of referral.
Symptoms leading to referral and clinical presentation of individuals with Lewy body dementia (LBD) (i.e., PDD/DLB) versus Non-LBD dementia (i.e., PD/PD-MCI)
Data are based on the first 99 consecutive cases assessed at the M&M Clinic (Table 3). In the whole sample (n = 99), the main symptoms comprising the diagnostic core criteria for DLB (McKeith et al. Reference McKeith, Boeve, Dickson, Halliday, Taylor, Weintraub, Aarsland, Galvin, Attems, Ballard, Bayston, Beach, Blanc, Bohnen, Bonanni, Bras, Brundin, Burn, Chen-Plotkin, Duda, El-Agnaf, Feldman, Ferman, ffytche, Fujishiro, Galasko, Goldman, Gomperts, Graff-Radford, Honig, Iranzo, Kantarci, Kaufer, Kukull, Lee, Leverenz, Lewis, Lippa, Lunde, Masellis, Masliah, McLean, Mollenhauer, Montine, Moreno, Mori, Murray, O’Brien, Orimo, Postuma, Ramaswamy, Ross, Salmon, Singleton, Taylor, Thomas, Tiraboschi, Toledo, Trojanowski, Tsuang, Walker, Yamada and Kosaka2017), which prompted referral to the clinic, were cognitive difficulties (64.65%), visual hallucinations (30.30%), and depression or anxiety-related complaints (35.35%). During clinical assessment of the entire sample, cognitive impairment was identified in 83.84%, recurrent visual hallucinations in 42.42%, REM sleep behaviour disorder in 56.57%, and spontaneous parkinsonian features in 90.91%.
Symptoms prompting referral and symptoms endorsed at assessment in Lewy body dementia (LBD) (i.e., PDD/DLB) versus non-LBD dementia (i.e., PD/PD-MCI)

Note: *Additional dementia with Lewy bodies symptoms that are part of the supportive features of the diagnostic criteria McKeith et al. (Reference McKeith, Boeve, Dickson, Halliday, Taylor, Weintraub, Aarsland, Galvin, Attems, Ballard, Bayston, Beach, Blanc, Bohnen, Bonanni, Bras, Brundin, Burn, Chen-Plotkin, Duda, El-Agnaf, Feldman, Ferman, ffytche, Fujishiro, Galasko, Goldman, Gomperts, Graff-Radford, Honig, Iranzo, Kantarci, Kaufer, Kukull, Lee, Leverenz, Lewis, Lippa, Lunde, Masellis, Masliah, McLean, Mollenhauer, Montine, Moreno, Mori, Murray, O’Brien, Orimo, Postuma, Ramaswamy, Ross, Salmon, Singleton, Taylor, Thomas, Tiraboschi, Toledo, Trojanowski, Tsuang, Walker, Yamada and Kosaka2017) were not assessed for: antipsychotic sensitivity, hyperosmia, syncope or transient loss of consciousness.
Within diagnostic subgroups, cognitive impairment was present in 64.44% of individuals in the non-dementia group (PD/PD-MCI; n = 45) and in 100% of those with LBD (DLB/PDD; n = 48). Recurrent visual hallucinations were documented in 15.56% of the non-dementia group compared with 72.92% of the LBD group. REM sleep behaviour disorder was identified in 48.89% of individuals in the non-dementia group and 60.42% of those with LBD. Cognitive fluctuations were relatively uncommon, present in 16.16% of the total cohort, occurring in 2.22% of the non- dementia group versus 31.25% of the LBD group.
Regarding supportive diagnostic features, dopaminergic abnormalities on SPECT/PET were identified in 26.3% of the overall cohort, occurring in 22.2% of individuals without LBD and 31.3% of those with LBD. Postural instability or falls were reported in 79.80% of individuals, including 86.67% of the non-dementia group and 81.25% of the LBD group. Autonomic dysfunction was present in 51.52% of the total cohort, occurring in 35.56% of the non-dementia group and 66.67% of the LBD group. Hyposmia occurred in 23.23% of the entire cohort, with 26.67% in the non-dementia group and 20.83% in the LBD group. Systematised delusions were recorded at referral in 23.23% of individuals and clinically documented in 17.17%; at assessment, they were noted in 4.44% of the non-dementia subgroup and 31.25% of the LBD group. Apathy was reported in 30.30% of the full sample and at similar rates across subgroups (28.89% in the non-dementia group; 35.42% in the LBD group). Depression and/or anxiety were identified in 48.48% of the total cohort, including 51.11% of individuals in the non-dementia group and 45.83% of those in the LBD group.
Additional supportive DLB features – antipsychotic sensitivity, hyperosmia, syncope, and transient loss of consciousness – were not systematically assessed.
Demographics and cognitive profile in individuals with Parkinson’s Disease-Mild Cognitive Impairment (PD-MCI) and Lewy body dementia (i.e., PDD and DLB)
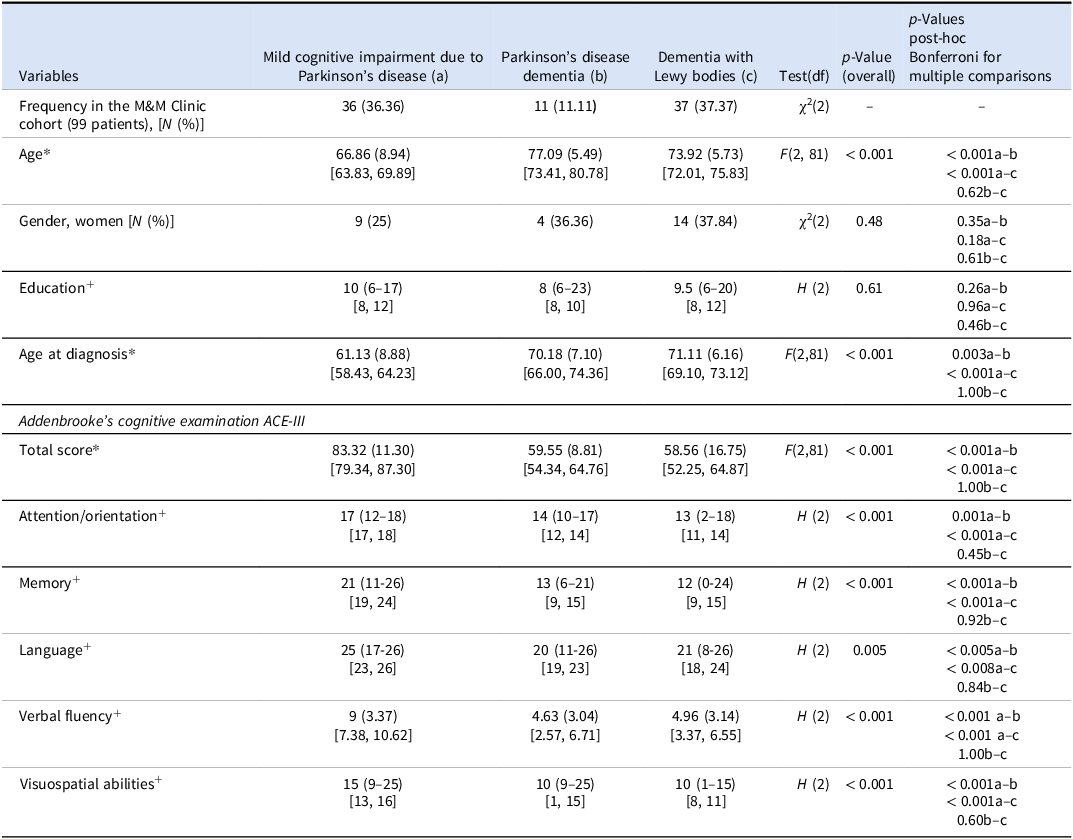
The demographic characteristics and cognitive profiles of individuals with PD-MCI, PDD and LBD are summarised in Table 4. PD-MCI and DLB were diagnosed with similar frequency (36.36% and 37.37%, respectively), whereas PDD was diagnosed less frequently (11.11%).
Demographic characteristics and Addenbrooke’s cognitive examination III (ACE-III) domain scores across mild cognitive impairment due to Parkinson’s disease (a), Parkinson’s disease dementia (b), and dementia with Lewy Bodies (c)

Note: *Mean (standard deviation) [CI = 95% Confidence Interval]; +Median (range) [CI = 95% Confidence Interval; df = degrees of freedom.
Comparisons were conducted between Mild Cognitive Impairment due to Parkinson’s Disease (PD-MCI) (a), Parkinson’s Disease Dementia (PDD) (b), and Dementia with Lewy Bodies (DLB) (c). Continuous variables were analysed using one-way ANOVA (F) or Kruskal–Wallis tests (H), and categorical variables using Chi-square tests (χ2). Bonferroni-adjusted p-values are reported for post-hoc pairwise comparisons. Significance threshold set at p < 0.05.
Post-hoc codes: a–b = PD-MCI vs PDD; a–c = PD-MCI vs DLB; b–c = PDD vs DLB.
Significant between-group differences in age were identified [F(2, 81) = 12.59, p < 0.001]. Individuals with PDD (mean 77.09 yrs ± 5.49) and DLB (mean = 73.92 yrs ± 5.73) were significantly older than those with PD-MCI (mean 66.86 yrs ± 8.49; both p < 0.001), with no age difference between the PDD and DLB groups (p = 0.62). A similar pattern was observed for age at diagnosis [F(2, 81) = 16.30, p < 0.001], with both PDD and DLB individuals diagnosed significantly later than those with PD-MCI (p = 0.003 and p < 0.001, respectively).
No significant group differences were observed in education level [H(2) = 1, p = 0.61] or gender distribution [χ2(2) = 1.48, p = 0.48].
As expected, ACE-III total scores differed significantly across groups [F(2) = 28.38, p < 0.001]. Individuals with PD-MCI scored significantly higher than those with PDD (p < 0.001) and DLB (p < 0.001), while PDD and DLB groups did not differ (p = 1.00). The same pattern was observed across the other ACE-III subscale (domain) scores – including attention/orientation [H(2) = 30.82, p < 0.001], memory [H(2) = 26.83, p < 0.001], language [(H(2) = 10.64, p = 0.005], verbal fluency [H(2) = 19.41, p < 0.001], and visuospatial abilities [H(2) = 28.69, p < 0.001]. Overall, individuals with PD-MCI performed significantly better than those with PDD and DLB (all ps < 0.005). No differences were found between PDD and DLB groups in any ACE-III domain (all ps > 0.45).
Although these results are consistent with established cognitive patterns across LBD subtypes, comparisons should be interpreted with caution due to the smaller number of PDD cases (n = 11).
Neuropsychiatric profile across Mild Cognitive Impairment due to Parkinson’s Disease (PD-MCI), Parkinson’s Disease Dementia (PDD), and Dementia with Lewy Bodies (DLB)
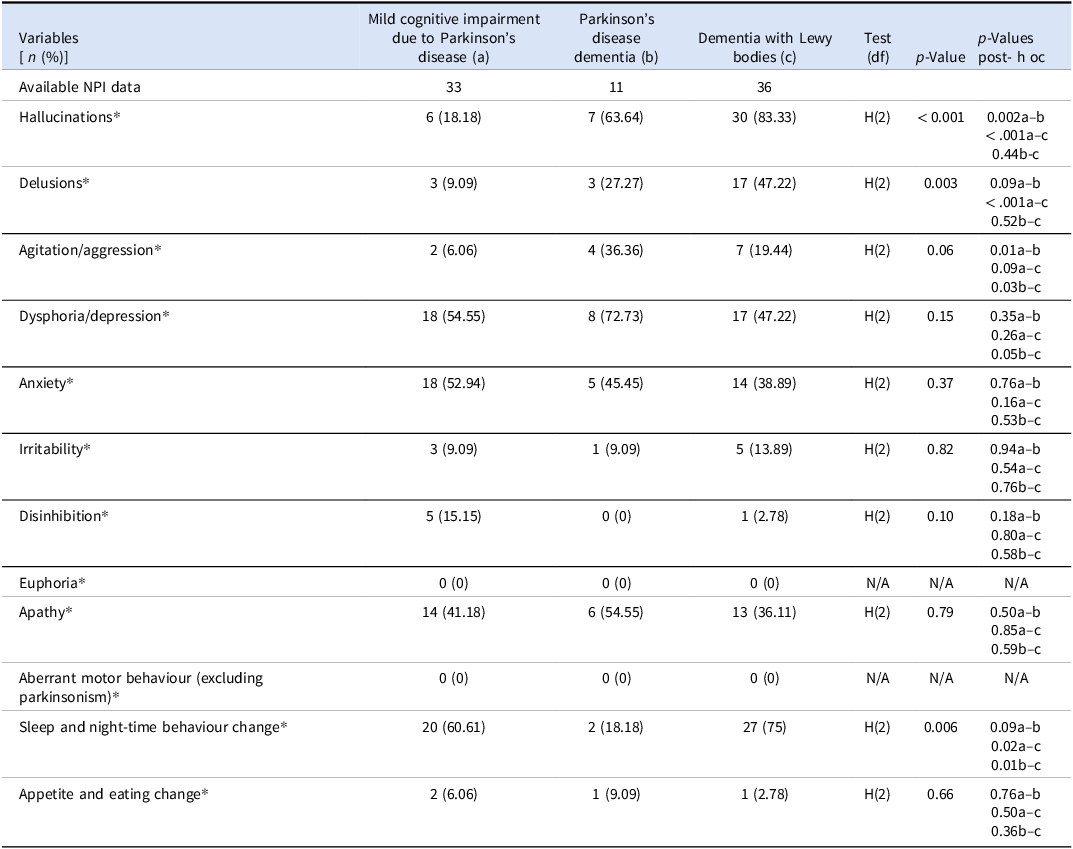
Data on Neuropsychiatric Inventory (NPI) symptoms and between-group comparisons in individuals with PD-MCI, PDD, and DLB are presented in Table 5.
Neuropsychiatric Inventory (NPI) symptoms across Mild cognitive impairment due to Parkinson’s disease (PD-MCI), Parkinson’s disease dementia (PDD), and Dementia with Lewy bodies (DLB)

Note: Comparisons were conducted between Mild Cognitive Impairment due to Parkinson’s Disease (PD-MCI) (a), Parkinson’s Disease Dementia (PDD) (b), and Dementia with Lewy Bodies (DLB) (c). *Neuropsychiatric Inventory (NPI) domain scores are shown as n (%) and reflect clinically significant symptoms (score ≥ 4), based on the combined frequency × severity rating. H = NPI domain scores were compared across the three groups using the Kruskal–Wallis H test with Bonferroni-adjusted post-hoc comparisons; df = degrees of freedom. Post-hoc group codes: a–b = PD-MCI vs PDD; a–c = PD-MCI vs DLB; b–c = PDD vs DLB.
N/A = not applicable; statistical tests were not performed as no cases were observed in any group.
Behavioural and psychological symptoms were assessed using the informant-rated 12-item NPI, with a domain score ≥ 4 (frequency × severity) considered clinically significant.
A Kruskal–Wallis H test (df = 2) demonstrated a significant overall group difference for hallucinations [H(2) = 28.11, p < 0.001]. Post-hoc analyses showed that individuals with PDD (63.64%) and DLB (83.33%) exhibited significantly higher rates than those with PD-MCI (18.18%; p = 0.002 and p < 0.001, respectively), whereas no significant difference was observed between PDD and DLB groups (p = 0.44). Notably, in the total sample (n = 99), the most frequently observed hallucinations were visual (n = 40, 40.40%), which in six patients (6.06%) also experiencing hallucinations in other sensory modalities (e.g., auditory, tactile).
Delusions also differed significantly across groups [H(2) = 11.96, p = 0.003]. The DLB group exhibited the highest prevalence (47.22%), followed by the PDD group (27.27%) and the PD-MCI group (9.09%). Post-hoc analyses confirmed significantly higher rates of delusion in DLB compared with PD-MCI (p < 0.001), with no statistically significant differences between PD-MCI and PDD (p = 0.09) or between PDD and DLB (p = 0.52). Across the entire cohort, delusional misidentification was the most common subtype, occurring in 13 individuals (13.13%), followed by delusions of jealousy, delusional infestation, and persecutory/paranoid delusions, each observed in one individual (1.01%).
Sleep and night-time behavioural changes differed significantly between diagnostic groups [H(2) = 10.27, p = 0.006], occurring more frequently in individuals with DLB (75.0%) than in those with PD-MCI (60.61%; p = 0.02) and PDD (18.18%; p = 0.01).
No significant between-group differences were observed for agitation/aggression [H(2) = 5.82, p = 0.06], dysphoria/depression [H(2) = 3.81, p = 0.15], anxiety [H(2) = 2, p = 0.37], or irritability [H(2) = 40, p = 0.82]. Similarly, disinhibition [H(2) = 4.59, p = 0.10], apathy [H(2) = 0.47, p = 0.79] and appetite and eating changes [H(2) = 0.84, p = 0.66] did not reach statistical significance following correction.
Investigations and therapeutic plans
All patients whose assessment might have benefited from structural neuroimaging had already had a brain MRI or CT scan prior to their evaluation at the M&M Clinic. Of the 32 patients who underwent DAT imaging, 26 (81.3%) already had a positive (i.e., abnormal) scan. A DAT scan was recommended to three additional patients (3.03%) who had not already undergone DAT imaging. Alzheimer-disease-related CSF biomarkers were elicited in only two individuals with DAT-scan-supported DLB, which unveiled amyloid pathology, prompting a diagnosis of comorbid Alzheimer’s disease and DLB. Additionally, detailed neuropsychological assessments were requested for five patients, following the initial M&M cognitive evaluation.
Following assessment, treatment plans including medication and non-medication related interventions were offered. Medication interventions were recommended to 71 (71.72%) patients, which included initiation and/or dose alterations, including three who required a dose change to their dopaminergic medications. Cholinesterase inhibitors were prescribed to 23 patients (23.23%), with rivastigmine transdermal patches being the most common. Antidepressants were prescribed in 69 patients (69.70%), with the most common being duloxetine, followed by mirtazapine. Other medications prescribed included melatonin (for rapid eye movement sleep behaviour disorder, RBD) and memantine, which was prescribed to four patients (4.04%). Combination therapy of cholinesterase inhibitor and memantine was prescribed in one patient (1.01%). Benzodiazepines (clonazepam or lorazepam) were prescribed in two patients only, while 22 were on benzodiazepines prior to referral to the M&M Clinic (22.22%). No medication cessation was recommended to the first 99 service users. Non-medication interventions included referrals to cognitive stimulation therapy, cognitive rehabilitation, speech therapy, and peer support in only 14 patients (14.14%) (see below ‘patient care pathway’). Additionally, within the M&M clinic, non-specific support such as education about the condition was offered to all patients.
Patient care pathway to and beyond the Mind and Movement clinic
Most patients were referred from the Parkinson’s clinic (n = 61, 61.62 %), followed by the memory clinic (n = 20, 20.20%) and the psychiatry of older age service (n = 6, 6.06%). The remaining 12 (12.12%) were referred directly from primary care (n = 2, 2.02%, memory clinic referrals redirected to M&M prior to assessment) or self-referrals (n = 10, 10.10%). A second opinion regarding a suspected diagnosis of PD-MCI, PDD or DLB was requested for 21 patients (21.21%), support for ongoing management of cognitive, behavioural and psychological symptoms for 46 patients (46.46%), and the need for possible additional diagnosis related to cognitive, behavioural and psychological symptoms for 32 patients (32.32%).
Following the assessment, 49 (49.49%) patients were referred to 16 separate services aimed at helping them with a variety of concerns. The patient care pathway is shown in Figure. 1, demonstrating a high degree of intersectionality across services to support the complex needs of these patients. Services within the St James’s Hospital included: occupational therapy (n = 9, 9.09%), Falls and Syncope Unit (FASU) (n = 5, 5.05%), physiotherapy (n = 5, 5.05%), neuropsychological assessment (n = 5, 5.05%), Social Prescribing Service (n = 5, 5.05%), medical social work (n = 5, 5.05%), Geriatric Day Hospital (n = 4, 4.04%), hearing assessment (n = 4, 4.04%), Cognitive Rehabilitation (n = 2, 2.02%), Older Adult Psychiatric Day Hospital (n = 2, 2.02%), Cognitive Stimulation Therapy (n = 1, 1.01%), medical nutritionist (n = 1, 1.01%); speech and language therapy (n = 1, 1.01%). Beyond St James’s Hospital, two referrals to the public health nurse were made (2.02%), and five individuals were referred to a driving assessment (5.05%).
Patient care pathway.

Additionally, ten people (10.10%) with DLB were referred to the monthly online peer support group ‘Teatime with Lewy’ supported by the third sector organisations, Lewy Body Ireland (LBI; www.lewybodyireland.org) and Lewy Body Society, UK (LBS; www.lewybody.org), and two (2.02%) were referred to the Lewy Body Admiral Nurse online support service offered from the UK. For patients (4.04%), given a diagnosis of LBD, information about relevant third sector organisations (LBI, LBS in the UK and Alzheimer Society Ireland) was given. Notable services not available were psychology.
Discussion
The M&M clinic embodies a cognitive and mental health service bridging the already well-established memory assessment, movement disorder and medical services (i.e. Falls and Syncope Unit) dedicated to older people with motor disturbances, cognitive decline and dysautonomia. This study aimed to profile the first 99 referrals to the M&M clinic as a service improvement project. Gaining insights into the demographic and clinical characteristics of users of a new service and their care pathways is valuable for further shaping and developing the service, ensuring it is tailored to users’ needs and complementary to, and well-integrated into, the network of available health and social care services.
Our findings underscore the broad scope and clinical utility of the M&M Clinic in delivering specialised assessments, optimising pharmacological management, and addressing cognitive and psychiatric symptoms in individuals with PD and related conditions. The clinic also complements the services provided by the memory clinic, particularly for patients presenting with psychosis. Cognitive deficits, recurrent visual hallucinations, and REM sleep behaviour disorder (RBD) were the most common referral symptoms. Notably, these were more frequently identified during M&M assessments than at the point of referral.
Of the total cohort, cognitive impairment was primarily a referral concern in 64 patients (65%) but detected in 83 (84%), including 48 (49%) with LBD; hallucinations were cited in 30 (30%) but found in 42 (42%); and RBD was noted in 9 (9%) but identified in 56 (57%) as part of broader sleep disturbances.
In some cases, these co-morbid features were not explicitly stated as the primary referral question but were likely recognised and documented elsewhere in the referral correspondence (e.g., within the body of the letter). These findings emphasise the clinic’s role in identifying under-recognised or secondary symptoms and facilitating more accurate diagnoses and tailored interventions.
Taken together, these findings indicate that observed symptom frequencies align with existing literature and highlight the need for multidisciplinary care in LBD spectrum disorders.
Visual hallucinations – a core diagnostic feature of DLB – affect up to 60% of individuals with PD over 12 years (Takenoshita et al. Reference Takenoshita, Terada, Yoshida, Yamaguchi, Yabe, Imai, Horiuchi, Miki, Yokota and Yamada2019), typically emerging in later stages and contributing to reduced quality of life and increased institutionalisation risk. Consistent with prior research33, misidentification delusions were most common in DLB, contrasting with the persecutory delusions more typical of other psychotic disorders34. Visual hallucinations and night-time disturbances were also more prevalent in DLB compared to PD-MCI. REM sleep disturbances were present in 60% of individuals with parkinsonism and dementia, versus 49% without dementia – highlighting a potential association with disease progression that warrants further study35 36. Agitation and aggression were more frequently observed in DLB and PDD than in PD-MCI, aligning with reports that such behaviours affect up to 70% of individuals with dementia, especially in moderate-to-severe stages37.
Cognitive impairment is a hallmark of DLB, while the point prevalence of PDD ranges from 22% to 48%; longitudinal studies report an annual dementia incidence of ∼10% in PD (Bruno and Vignaga, Reference Bruno and Vignaga2019). REM sleep behaviour disorder (RBD), present in 33–46% of individuals with PD (Morris Reference Morris1997) and up to 40% with DLB (Cummings et al. Reference Cummings, Mega, Gray, Rosenberg-Thompson, Carusi and Gornbein1994), is strongly associated with cognitive and functional decline. Idiopathic RBD is also a key predictor for developing parkinsonism and dementia (Saari et al. Reference Saari, Koivisto, Hintsa, Hänninen and Hallikainen2022).
In our cohort, cognitive performance was significantly lower in individuals with PDD and DLB than in those with PD-MCI, with no significant differences between PDD and DLB. As expected (Hsieh et al. Reference Hsieh, Schubert, Hoon, Mioshi and Hodges2013), PD-MCI patients scored higher across attention/orientation, memory, language, verbal fluency, and visuospatial domains (ACE-III). The performance gap in language was more pronounced between DLB and PD-MCI than between PDD and PD-MCI, though small sample sizes – particularly in the PDD group – limit interpretation. While previous studies suggest greater deficits in DLB than in PDD, especially in attention, visuospatial, and language functions32, such differences were not evident in our data. These findings should be interpreted cautiously, and a more detailed assessment or a larger sample may help clarify these trends. This report, however, offers a pragmatic overview of the first 99 patients seen at the new outpatient clinic rather than an exhaustive neurocognitive analysis.
The complex clinical phenotype of LBD has necessitated the implementation of a multidisciplinary team (MDT) approach at St James’s Hospital. MDT interventions have been shown to improve quality of life and reduce depressive symptoms in people with PD (Cummings et al. 1994). Referrals to the M&M Clinic, along with the collaborative diagnostic efforts between the Parkinson’s Clinic, Memory Clinic, and M&M Clinic, highlight the adaptability of the MDT model in addressing the multifaceted symptoms, side effects, and comorbidities associated with LBD. The newly established M&M Clinic represents a vital addition to the care pathway, focusing specifically on symptoms that are often overlooked or inadequately managed within existing services.
Medication profiles differed significantly between patients with and without dementia. Those with dementia were more frequently prescribed antidepressants, antipsychotics, cholinesterase inhibitors, and hydrocortisone/midodrine. Antiparkinsonian medication use was also higher in this group – an unexpected finding that may reflect the small sample size or the predominance of DLB (n = 37, 77%) over PDD (n = 11, 23%) in the dementia cohort. In DLB, parkinsonism is often less severe at diagnosis (Simpson et al. Reference Simpson, Wyman-Chick and Daniel2025), and antiparkinsonian drugs are generally less effective and more likely to worsen symptoms such as hallucinations and sedation (Gonçalves et al. Reference Gonçalves, Malafaia, Moutinho dos Santos, Roth and Marques2023) 26. The higher rate of antipsychotic use in dementia aligns with the central role of psychosis in DLB, though it raises concerns given DLB patients’ heightened sensitivity to antipsychotic side effects. The increased use of antidepressants may reflect either chance variation or greater symptom severity, despite similar rates of depressive and anxiety symptoms across PD-MCI, PDD, and DLB based on NPI subscores27–29. Cholinesterase inhibitors (primarily rivastigmine and donepezil), approved for both PDD and DLB30, were more commonly prescribed in the dementia group, with 23 patients (19%) initiated on treatment following M&M Clinic assessment. Increased fludrocortisone/midodrine use in this group supports growing evidence linking synucleinopathy-related dementia, particularly DLB, with dysautonomia and orthostatic hypotension31.
Post-diagnostically, patients were referred to ten different hospital-based services, and 21 (21%) were directed to community or peer-support services. These individualised care plans reflect the heterogeneity of care needs in LBD. The management of LBD is clinically complex due to poly-symptomatic presentation, heightened sensitivity to medication side effects, and functional decline across physical, cognitive, neuropsychiatric, and autonomic domains. LBD care necessitates coordination across disciplines and services, including frequent transitions such as hospitalisations38,39. A German inpatient multimodal treatment programme for PD has shown success in combining pharmacological and non-pharmacological interventions – including physiotherapy, occupational and speech therapy – with attention to post-discharge community care40. Similarly, the synergies between the Parkinson’s Clinic, Memory Clinic, and M&M Clinic at St James’s Hospital embody a local integrated care pathway41, addressing the multifaceted symptoms and comorbidities associated with LBD and warranting further evaluation and refinement. If proven effective, such a model could be scaled nationally, particularly in light of the high and escalating care costs associated with LBD compared to other dementias like AD42. Such integrated services should ideally be embedded within Ireland’s developing memory service network (under the National Dementia Service) and integrated with local movement disorder services. Access to post-diagnostic care – occupational therapy, speech therapy, falls clinics, ICPOP, psychiatry, neurology, gerontology, and emergency services – should be safeguarded.
Finally, to further enhance understanding of the phenotypic and endophenotypic spectrum of LBD, the development of a Core Outcome Set (COS) is essential. It would facilitate harmonisation of outcome measures, improve cross-study comparability, support clinical implementation, and ultimately guide more informed healthcare decision-making (Park and Kwak, Reference Park and Kwak2021).
This real-world, retrospective report has certain limitations. The sample was small and imbalanced, particularly with few PDD cases, and data completeness varied43. Additionally, while diagnoses followed international criteria and were supported by biomarkers (e.g., cMRI, DAT scans), they were not confirmed at autopsy, leaving room for diagnostic uncertainty. These factors limit generalisability. Nonetheless, the study`s strengths include its real-world setting and consecutive referral, and it provides invaluable evidence supporting the development and upscaling of speciality clinics such as the M&M Clinic.
Conclusion
The M&M Clinic at St James’s Hospital in Dublin provides specialised cognitive and mental healthcare for individuals with neuropsychiatric and cognitive manifestations of LBD spectrum disorders disease spectrum disorders. Through diagnostic clarification and tailored post-diagnostic care, the clinic supports the development of an integrated local care pathway addressing the complex and variable needs of this population. Ongoing evaluation of service structure, effectiveness, and patient experience will be essential to guide future expansion.
Funding statement
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors report no competing interests.
Ethical consideration
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The service has ethical approval to analyse routinely collected clinical data for entry to an anonymised database for the purpose of service appraisal and development. The study was conducted as a service improvement project in accordance with local governance procedures, and further formal research ethics committee approval was not required.



 Open access
Open access