

Introduction
Clinical trials are critical to advance medical treatments from the laboratory to the bedside. However, this process is lengthy and costly, costing up to 10 to 15 years and as much as $2 billion [Reference Chaudhari, Ravi, Gogtay and Thatte1–Reference Bower, Brueton and Gamble3]. Nearly 40% of trial sites face under-recruitment, and delays in recruitment can extend the study duration by 1 to 6 months, making trials less effective and efficient [Reference Desai2,Reference Wandile4]. In addition, traditional recruitment methods are not only labor-intensive but also often biased; studies have shown that older adults, women, and minority ethnic groups are frequently underrepresented, undermining the external validity of trial results [Reference Ford, Howerton and Lai5–Reference Yang, Nair and Ke9]. These challenges can delay new therapies, incur economic losses, and raise ethical concerns about equitable trial access.
Advances in artificial intelligence (AI) have begun to transform the healthcare industry in recent years. AI tools encompass various categories, including machine learning (supervised, unsupervised, reinforcement), robotic, and rule-based approaches [Reference Muthazhagu, Surendiran and Arulmurugaselvi10,Reference Shi, Yang, Yang and Zhou11]. Machine learning-based AI excels with large, unstructured data and complex tasks, while rule-based and robotic AIs perform better with structured data and simple tasks [Reference Ompusunggu, Sensuse, Wahbi and Mahdalina12–Reference Liu, Gegov and Cocea14]. From early predictive modeling to complex algorithms involving natural language processing (NLP), large-scale language models, and interactive chatbots, developments in AI have opened new avenues for addressing long-standing challenges in clinical trials. The application of AI in diagnostic imaging, dose management, and clinical decision-making has yielded promising results [Reference Talati15–Reference Bajwa, Munir, Nori and Williams17].
However, integrating AI into clinical trial program workflows remained a challenge. Issues of interoperability, clinician trust, adoption, and the risk of embedding or exacerbating bias through AI algorithms remained serious concerns. These challenges are critical given the need for diverse and inclusive patient populations in clinical trials [Reference Lu, Yang, Liang, Hu, Zhong and Jiang18–21]. While AI has been credited for its ability to optimize the clinical trial process [Reference Prabhakar22–Reference Harrer, Shah, Antony and Hu25], relatively few studies have explored the role of AI in improving early-stage trial efficiency, particularly through improved recruitment and retention.
We conducted a comprehensive scoping review to evaluate the role, effectiveness, and limitations of AI-powered tools in clinical trial recruitment and retention. By synthesizing existing evidence, we highlight both the promise and challenges of current applications, aiming to inform future strategies for effective and equitable implementation.
Methods
We conducted a comprehensive scoping review to investigate the use of AI technologies in enhancing the recruitment and retention process in clinical trials. To accomplish this, this review followed the methodological framework outlined by the Joanna Briggs Institute (JBI). It was reported using the Preferred Reporting Items for Systematic Reviews of Scoping Reviews (PRISMA-ScR) guidelines to ensure transparency and compliance with reporting standards [Reference Peters, Marnie and Tricco26–28]. The paper screening process was described by the PRISMA-ScR flowchart. The included papers were carefully categorized. The performance of the AI models was then analyzed using a comprehensive meta-analysis. Details of the methodological framework for the beginning phase can be found in Supplementary Material 1 (Appendix A: Extra Details of Methods of the Appendix.additional content).
Developing the search strategy
A comprehensive search strategy was developed for each database with the help of an experienced librarian to identify relevant studies. The search strategy combined keywords and database-specific controlled vocabulary using “OR” and filtered papers on AI and trial participant terms/keywords using “AND.” Searches were conducted in multiple databases, including comprehensive searches in Medline (via Ovid), Cochrane Library, Embase (Elsevier), CINAHL Complete (EBSCOhost), and Scopus (Elsevier) using controlled vocabulary and keywords. Only publications written in English were included to ensure feasibility, and comments, editorials, letters, and conference abstracts were excluded from the search. The literature search was limited to publications from January 1, 2018, to June 28, 2024, coinciding with the emergence of new AI tools and techniques. The search strategy was adapted to match different formats from different databases. An experienced librarian assisted throughout the construction, conversion, and implementation of the search strategy, ensuring the robustness of the search and the comprehensive identification of relevant studies. Details of our search strategy can be found in Supplementary Material 1 (Appendix B: Search Strategy of the Appendix.additional content).
Paper screening and source of evidence selection
The paper screening process followed a structured approach [Reference Peters, Marnie and Tricco26,Reference Tricco, Lillie and Zarin29] to ensure comprehensive and unbiased inclusion of relevant evidence. Titles and abstracts were initially screened using Covidence, followed by full-text review, with all studies assessed by at least two independent reviewers. Discrepancies were resolved through group discussion with an additional reviewer. Reviewers (YC, ZR, JCKL, YR, EM, ZG) received training and completed a 100-title pilot to ensure consistency. Dual independent screening was applied to all records, with conflicts resolved by third reviewers (HF, CH). Screening results are detailed in the results section and illustrated in the PRISMA-ScR flowchart.
Large language model-based assistance (ChatGPT, OpenAI) was used to improve the efficiency of title and abstract screening. We applied the predefined inclusion criteria to generate a relevance score (0–100). These scores were used to prioritize the order of human review (≥58 indicating likely to meet, 40–58 ambiguous, <40 unlikely to meet). All results were subsequently manually checked and verified by reviewers (YC, ZR, JCKL, YR, EM, ZG). Further methodological details are provided in Supplementary Material 1 (Appendix A: Extra Details of Methods of the Appendix.additional content). The detailed description of our AI-assisted methodological construction is discussed in Liu et al [Reference Liu, Yang and Liew30].
Charting the evidence and data extraction
We extracted key information from each included study, including demographic features, AI tool details, and AI model performance. Study characteristics included study purpose, publication date, duration, country of author affiliation, cohort description, inclusion and exclusion criteria, and dataset sources. AI tool implementation was assessed across four aspects: (1) tool timing (retrospective analysis vs. real-time alert system); (2) tool implementation (theoretical framework vs. real-world clinical setting); (3) type of tool (recruitment AI vs. retention AI); and (4) type of AI technology (e.g., electronic health record (EHR)-based models, chatbot-based recruitment, NLP for eligibility screening, or machine learning-based patient stratification). AI model performance was documented using clinical outcome metrics (e.g., time saved, percentage of participants retained, trial efficiency) and standard metrics: precision, recall, positive predictive value (PPV), negative predictive value (NPV), area under the receiver operating characteristic curve (AUC-ROC), and F1-score.
Paper categorization by recruitment and retention workflow
To enhance interpretability and facilitate subsequent meta-analysis, we categorized each study according to the specific stage of the clinical trial recruitment and retention workflow that the AI tool aimed to enhance. The included studies were grouped into 10 categories. The first category includes AI tools that extract, structure, and interpret eligibility criteria. The second focuses on classifying free-text eligibility into structured formats. The third involves identifying potential patient cohorts, followed by tools for direct patient screening that assess trial eligibility. Next, AI tools focused on patient-trial matching systematically pair patient profiles with suitable clinical trials or arms. Upon completion of the recruitment stage, the retention phase begins with AI tools that enhance patient adherence during retention. Two additional categories include AI tools for evaluating and optimizing past trial eligibility rules and AI-driven digital platforms that enhance trial processes or deliver clinical information to stakeholders. Beyond the categorization, studies were also classified by (1) timing, (2) implementation, and (3) tool type, as previously described.
Meta-analysis
We conducted a meta-analysis stratified by clinical trial categories to quantitatively assess the AI model’s performance at different stages of the recruitment and retention workflow. Each meta-analysis used performance metrics, including sensitivity, specificity, precision, accuracy, F1 score, and AUC. A random-effects model was employed to account for heterogeneity among studies, and weighted averages were calculated for pooled performance estimates. Forest plots were generated for each model’s performance to visualize individual study contributions and overall effect sizes. The between-study heterogeneity was quantified using k, τ 2, and I 2 for each task–metric stratum, and results were interpreted. The full stratum-level table could be referred to Supplementary Material 2 (Appendix Table 1. heterogeneity assessment).
Detailed code and data tables are provided in the accompanying GitHub repository: https://github.com/yinz33/Artificial-Intelligence-in-Clinical-Trial-Participant-Recruitment-and-Retention.git
Results
Applications of artificial intelligence across the clinical trial workflow
Study identification and screening summary
21,573 records were initially identified through our database searches (Embase, Medline [via Ovid], CINAHL, CENTRAL, and Scopus). After removing duplicates, 18,741 unique records underwent title and abstract screening. The low inclusion rate of 1.01% reflects our deliberate use of broad search terms to ensure comprehensive coverage of this emerging field, combined with rigorous inclusion criteria requiring demonstrated AI implementation rather than theoretical discussions. Many retrieved studies addressed AI in clinical settings generally, but relatively few specifically focused on recruitment and retention processes within clinical trial workflows. This stringent approach ensures our findings represent the current evidence base of practically implemented AI solutions in clinical trials. 18,552 articles were excluded during title and abstract screening. 194 disagreements (1.04%) from independent double-screenings were reconciled on multiple occasions. Table 1 outlines the key features of studies that utilize AI tools to screen and recruit eligible patients. Details of addressing disagreement can be referred to Supplementary Material 3 (Appendix Table 2. screening and resolution). Subsequently, 189 articles were assessed in full text, and 68 were excluded. Ultimately, 121 articles were included in this review (Figure 1).
Brief summary of included studies

PRISMA-ScR flowchart for the scoping review process. Out of 189 full-text articles that passed the title and abstract screening, 68 were excluded primarily because they were review papers, lacked AI application, or did not focus on recruitment or retention.

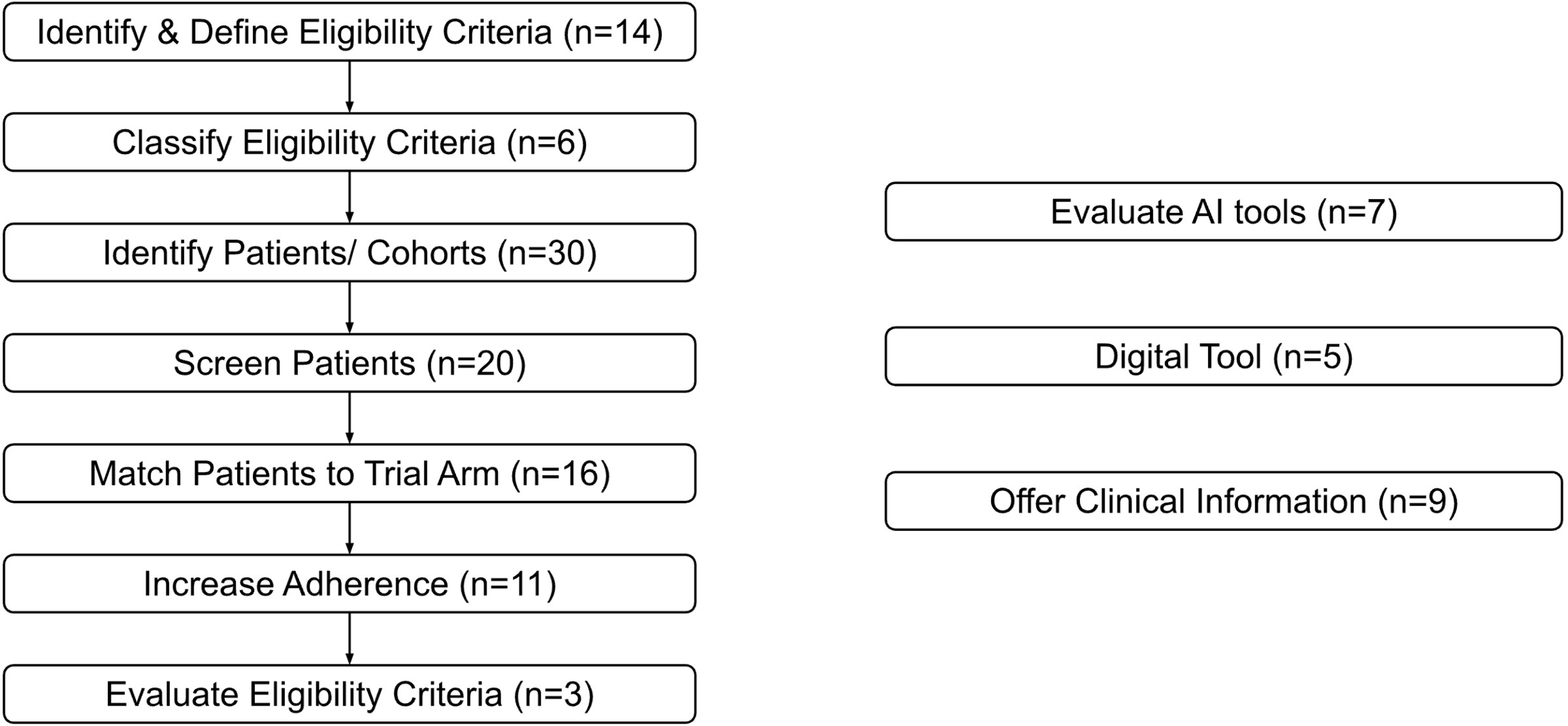
Figure 2 illustrates a comprehensive, multi-step clinical trial recruitment and retention workflow based on the reviewed studies. The workflow begins with identifying and defining eligibility criteria (n = 14), where AI tools extract, structure, and interpret requirements from various sources. Six studies focused on classifying these criteria by converting free text into structured formats. Thirty studies applied AI to identify potential patient cohorts, and 20 used AI for direct patient screening to find individuals likely to meet trial criteria. Patient-trial matching was addressed in 16 studies, using AI to align patient profiles with suitable trials. For retention, 11 studies employed AI to support adherence by addressing barriers. Three studies evaluated past eligibility rules, while eight focused on subprocesses across the trial workflow. Additionally, five studies developed AI-based digital tools to streamline trial processes, and nine used AI to deliver relevant clinical or medical information to stakeholders. Figure 2 summarizes how studies addressed the full recruitment and retention process in clinical trials. Details are in Supplementary Material 4 (Appendix Table 3.summary of AI tasks, data, evaluation metrics).
Clinical trial recruitment and retention workflow. The included studies were grouped into ten categories based on the workflow stage targeted by the AI tool.

AI for eligibility assessment
The AI tools for identifying eligibility criteria are designed to extract, structure, and interpret eligibility requirements. These tools commonly take as input the free-text eligibility criteria from ClinicalTrials.gov [Reference Jung, Jain, Sinha and Gaudioso31–Reference Tian, Erdengasileng and Yang40] and unstructured or structured data from electronic health records (EHRs) [Reference Tun, Luo, Xie, Wibowo and Hao41–Reference Karystianis, Florez-Vargas, Butler and Nenadic43]. The AI approaches in this category frequently rely on NLP techniques such as rule-based logic [Reference Jung, Jain, Sinha and Gaudioso31,Reference Yuan, Ryan and Ta33,Reference Tun, Luo, Xie, Wibowo and Hao41–Reference Karystianis, Florez-Vargas, Butler and Nenadic43], lexicon-enhanced pipelines [Reference Jung, Jain, Sinha and Gaudioso31], named entity recognition (NER) [Reference Jung, Jain, Sinha and Gaudioso31,Reference Fang, Idnay and Sun32,Reference Bompelli, Li and Xu34–Reference Tian, Yin, Zhang, Erdengasileng, Bian and He38,Reference Tian, Erdengasileng and Yang40], the concept normalization to standardized vocabularies like OMOP CDM or UMLS [Reference Yuan, Ryan and Ta33,Reference Bompelli, Li and Xu34,Reference Sun and Tao36,Reference Fang, Kim and Idnay39], and other tools like Apache UIMA, CLAMP, Criteria2Query [Reference Jung, Jain, Sinha and Gaudioso31,Reference Yuan, Ryan and Ta33,Reference Bompelli, Li and Xu34,Reference Sun and Tao36,Reference Fang, Kim and Idnay39,Reference Meystre, Heider, Kim, Aruch and Britten42] for better structured annotation and entity mapping. Nevertheless, the transformer-based models, including BERT, SciBERT, PubMedBERT, and SapBERT, are also used for entity recognition and relation extraction tasks [Reference Dobbins, Mullen, Uzuner and Yetisgen35,Reference Sun and Tao36,Reference Tian, Yin, Zhang, Erdengasileng, Bian and He38,Reference Tian, Erdengasileng and Yang40]. These approaches typically yield structured outputs such as computable cohort definitions [Reference Yuan, Ryan and Ta33,Reference Fang, Kim and Idnay39], entity-attribute relations [Reference Dobbins, Mullen, Uzuner and Yetisgen35], condition-drug-procedure mappings [Reference Sun and Tao36–Reference Tian, Yin, Zhang, Erdengasileng, Bian and He38], annotated named entities or eligibility criteria tokens [Reference Jung, Jain, Sinha and Gaudioso31,Reference Dobbins, Mullen, Uzuner and Yetisgen35,Reference Sun and Tao36,Reference Tian, Erdengasileng and Yang40], and alerts from user interfaces [Reference Fang, Idnay and Sun32,Reference Meystre, Heider, Kim, Aruch and Britten42].
The AI tools that classify eligibility criteria are designed to categorize free-text eligibility statements into structured, interpretable formats. These models typically leverage transformer-based NLP architectures, such as BERT-family variants with ensemble frameworks to improve classification performance [Reference Zeng, Xu, Lin, Liang and Hao44–Reference Yang, Jayaraj, Ludmir and Roberts46]. Some tools integrate more advanced machine learning algorithms like LightGBM [Reference Zeng, Pan, Xu and Qu45] or custom preprocessing pipelines with word embeddings (Word2Vec and FastText) for better phrase detection and classification [Reference Bustos and Pertusa47]. This yielded a wide variety of outputs. Some generate predicted category labels spanning dozens of predefined eligibility-related classes [Reference Zeng, Xu, Lin, Liang and Hao44,Reference Bustos and Pertusa47] or binary exclusion indicators for predefined conditions, like prior malignancy, autoimmune disease, or infections [Reference Yang, Jayaraj, Ludmir and Roberts46]. Some other tools convert eligibility text into structured clinical concepts mapped to standardized vocabularies, such as OMOP CDM [48,Reference Li, Liu and Kury49], and offer user interfaces for further manual classification, including editing, reviewing, or querying eligibility logic.
AI for patient identification and trial matching
AI tools used for direct patient screening aim to efficiently identify individuals or cohorts who are likely to meet key clinical trial eligibility criteria. These tools apply a wide spectrum of methodologies, ranging from classical statistical models like logistic regression [Reference Yang, Watach, Varrasse, King and Sawyer50–Reference Ansart, Epelbaum and Gagliardi52], ensemble learning methods such as random forests, LASSO, and gradient-boosted trees [Reference Cai, Cai and Dahal51,Reference Widera, Welsing and Danso53–Reference Ni, Bermudez, Kennebeck, Liddy-Hicks and Dexheimer56], to more advanced NLP pipelines incorporating NER, rule-based logic, TF-IDF, and transformer-based architectures like GPT-4 or hybrid models with retrieval-augmented generation (RAG) [Reference Vinod Vydiswaran, Strayhorn and Zhao57–Reference Ansoborlo, Gaborit, Grammatico-Guillon, Cuggia and Bouzille62]. The AI approaches in this category include diverse input sources, including structured and unstructured EHR data such as progress notes, lab values, and ICD codes [Reference Yang, Watach, Varrasse, King and Sawyer50–Reference Ansart, Epelbaum and Gagliardi52,Reference Kanbar, Wissel and Ni54,Reference Ni, Bermudez, Kennebeck, Liddy-Hicks and Dexheimer56–Reference Meystre, Heider and Cates61,Reference Haddad, Helgeson and Pomerleau63–Reference Calaprice-Whitty, Galil, Salloum, Zariv and Jimenez65], the patient self-reported or survey data [Reference Bustos and Pertusa47,Reference Yang, Watach, Varrasse, King and Sawyer50,55], and the medical image or scanning [Reference Widera, Welsing and Danso53,Reference Juan Ramon, Parmar and Carrasco-Zevallos66]. The outputs from these tools are typically binary classification of eligible or ineligible [Reference Yang, Watach, Varrasse, King and Sawyer50–Reference Ansart, Epelbaum and Gagliardi52,Reference Kanbar, Wissel and Ni54,Reference Ni, Bermudez, Kennebeck, Liddy-Hicks and Dexheimer56–Reference Meystre, Heider and Cates61,Reference Haddad, Helgeson and Pomerleau63–Reference Calaprice-Whitty, Galil, Salloum, Zariv and Jimenez65] and predicted eligibility scores [Reference Yang, Watach, Varrasse, King and Sawyer50–Reference Widera, Welsing and Danso53,55,Reference Meystre, Heider and Cates61].
AI tools for patient-trial matching are designed to systematically pair patient profiles with appropriate clinical trials. These tools typically input structured and unstructured EHR data [Reference Kaskovich, Wyatt and Oliwa67–Reference Wang, Cui and Zhu81] with explicitly defined eligibility criteria [Reference Lu, Yang, Liang, Hu, Zhong and Jiang18,Reference Stemerman, Bunning, Grover, Kitzmiller and Patel58,Reference Ott, Rinner and Duftschmid98,Reference Mellem, Kollada, Tiller and Lauritzen136] or free-text eligibility criteria description directly derived from ClinicalTrials.gov or curated trial protocols [Reference Murcia, Aggarwal and Pesaladinne68,Reference Nievas, Basu, Wang and Singh70–Reference Alexander, Solomon and Ball73,Reference Yuan, Tang, Jiang and Hu75–Reference Jin, Wang and Floudas77,Reference Chang, Yuan and Ding79–Reference Wang, Cui and Zhu81]. Methodologies in this category span several AI and machine learning strategies, including transformer-based models [Reference Nievas, Basu, Wang and Singh70,Reference Yuan, Tang, Jiang and Hu75,Reference Jin, Wang and Floudas77,Reference Chang, Yuan and Ding79,Reference Beattie, Neufeld and Yang80], the NLP-enhanced rule-based pipelines [Reference Murcia, Aggarwal and Pesaladinne68,Reference Kusa, Mendoza, Knoth, Pasi and Hanbury71–Reference Alexander, Solomon and Ball73,Reference Hassanzadeh, Karimi and Nguyen76,Reference Xu, Liu and Sun78,Reference Wang, Cui and Zhu81], the semantic similarity approaches [Reference Kusa, Mendoza, Knoth, Pasi and Hanbury71,Reference Yuan, Tang, Jiang and Hu75,Reference Hassanzadeh, Karimi and Nguyen76], and other machine learning classifiers, including gradient boosting machines and logistic regression [Reference O’Regan, Hoskins and Grave69,Reference Kehl, Mazor and Trukhanov74,Reference Chang, Yuan and Ding79]. These AI tools typically generate binary eligibility decisions indicating whether a patient is eligible for each potential trial [Reference Murcia, Aggarwal and Pesaladinne68,Reference Nievas, Basu, Wang and Singh70,Reference Kehl, Mazor and Trukhanov74,Reference Jin, Wang and Floudas77,Reference Chang, Yuan and Ding79,Reference Beattie, Neufeld and Yang80]; some are more quantitatively advanced with matching scores [Reference Nievas, Basu, Wang and Singh70,Reference Kehl, Mazor and Trukhanov74,Reference Hassanzadeh, Karimi and Nguyen76,Reference Chang, Yuan and Ding79]. Some tools yield ranked trial lists for each patient as output, with confidence levels or visual explanations of inclusion/exclusion features [Reference Murcia, Aggarwal and Pesaladinne68,Reference Kusa, Mendoza, Knoth, Pasi and Hanbury71–Reference Alexander, Solomon and Ball73,Reference Xu, Liu and Sun78,Reference Wang, Cui and Zhu81].
AI for trial retention and workflow support
AI-driven digital tools can enhance the clinical trial recruitment and retention process at any stage of the workflow. These tools typically operate as front-end systems, such as chatbots [Reference Chuan and Morgan82], digital research assistants [Reference Cesario, Simone and Paris83], and telemedicine [Reference Hardy-Abeloos, Karp and Xiao84]/patient tracking platforms [Reference Do, Elbers and Fillmore85]. These tools’ inputs vary based on different tasks, including unstructured free-text eligibility criteria extracted from clinical trial databases [Reference Chuan and Morgan82] and structured and unstructured EHR data [Reference Cesario, Simone and Paris83–Reference Do, Elbers and Fillmore85]. The AI approaches are typically NLP and deep learning techniques, such as word2vec embeddings and convolutional neural networks (CNN) for chatbot interfaces [Reference Chuan and Morgan82], and the hybrid NLP pipeline for interaction support [Reference Cesario, Simone and Paris83,Reference Do, Elbers and Fillmore85].
The AI tools that are designed for increasing patient adherence during the retention stage usually employ a wide range of methodologies to overcome different adherence barriers, including tailored interventions [Reference Chen, Houston and Faro86–Reference Castillo, Alexander and Rubiano89], predictive scoring for worsening conditions [Reference Getz, Smith, Shafner and Hanina90–Reference Abiodun, Okunbor and Osamor93], and engagement real-time monitoring [Reference Abiodun, Okunbor and Osamor93–Reference Shafner96]. This type of AI tools includes diverse input sources, depending on different tasks, including self-reported data and survey responses from patients [Reference Chen, Houston and Faro86,Reference Adams, Long and Fleury87,Reference Getz, Smith, Shafner and Hanina90,Reference Craig, Ji and Zhang92,Reference Abiodun, Okunbor and Osamor93], structured and unstructured EHR data [Reference Lauffenburger, Yom-Tov and Keller88,Reference Craig, Ji and Zhang92–Reference DeLozier, Speltz and Brito95], the data tracked by mobile app [Reference Roy, Zhu, Guan, Feng, Daniels and Sand91,Reference Shafner96], and so on. The key methodologies also span widely depending on the tasks, such as rule-based alert systems [Reference Oluoch, Cornet and Muthusi94], computer vision-powered platforms and mobile AI apps for real-time dose tracking and fraud detection [Reference Roy, Zhu, Guan, Feng, Daniels and Sand91,Reference Shafner96], and more advanced predictive modeling [Reference Chen, Houston and Faro86,Reference Getz, Smith, Shafner and Hanina90,Reference Abiodun, Okunbor and Osamor93] and an NLP system that flags suspected adverse reactions [Reference DeLozier, Speltz and Brito95].
AI tools for evaluating eligibility criteria are designed to assess, validate, and optimize how trial eligibility rules are constructed or applied in past clinical trials. The approaches include rule-based logic systems [Reference Liu, Rizzo and Whipple97], NLP pipelines [Reference Ott, Rinner and Duftschmid98], and predictive modeling frameworks [Reference Gulden, Landerer, Nassirian and Andrae99]. The evaluate AI models category validates or enhances the performance, generalizability, and fairness of AI tools used when enhancing the effectiveness of clinical trial recruitment and retention. The clinical trial databases [Reference Beaulieu, Berry and Paganoni100–Reference Ismail, Al-Zoubi, El Naqa and Saeed102], structured EHR data [Reference Beaulieu, Berry and Paganoni100,Reference Kempf, Vaterkowski and Leprovost101,Reference Theodorou, Glass, Xiao and Sun103–Reference Idnay, Liu and Fang106], unstructured notes [Reference Ismail, Al-Zoubi, El Naqa and Saeed102,Reference Idnay, Liu and Fang106], and medical images/scans [Reference Iyer, Pokkalla and Biddle-Snead104] would generally be used depending on the tool’s focus. Their outputs are either predictive accuracy metrics [Reference Beaulieu, Berry and Paganoni100–Reference Ismail, Al-Zoubi, El Naqa and Saeed102,Reference Iyer, Pokkalla and Biddle-Snead104–Reference Idnay, Liu and Fang106] or fairness metrics like demographic parity and equal opportunity [Reference Theodorou, Glass, Xiao and Sun103].
Lastly, AI tools that offer clinical information support and enhance recruitment and retention decision-making by delivering actionable insights to clinicians, researchers, or patients. These AI tools’ input depends on the type of information they offer, often including EHR-derived medical profiles [Reference Jordan, Jahreiss and Kasi107–Reference Ma, Lowe and Berkowitz110], free-text clinical reports [Reference Borno, Duffy and Zhang111], structured eligibility criteria [Reference Jordan, Jahreiss and Kasi107], or self-reported medication data [Reference Marcath, Coe and Shakeel112]. More details can be found in Supplementary Material 4 (Appendix Table 3.summary of AI tasks, data, evaluation metrics).
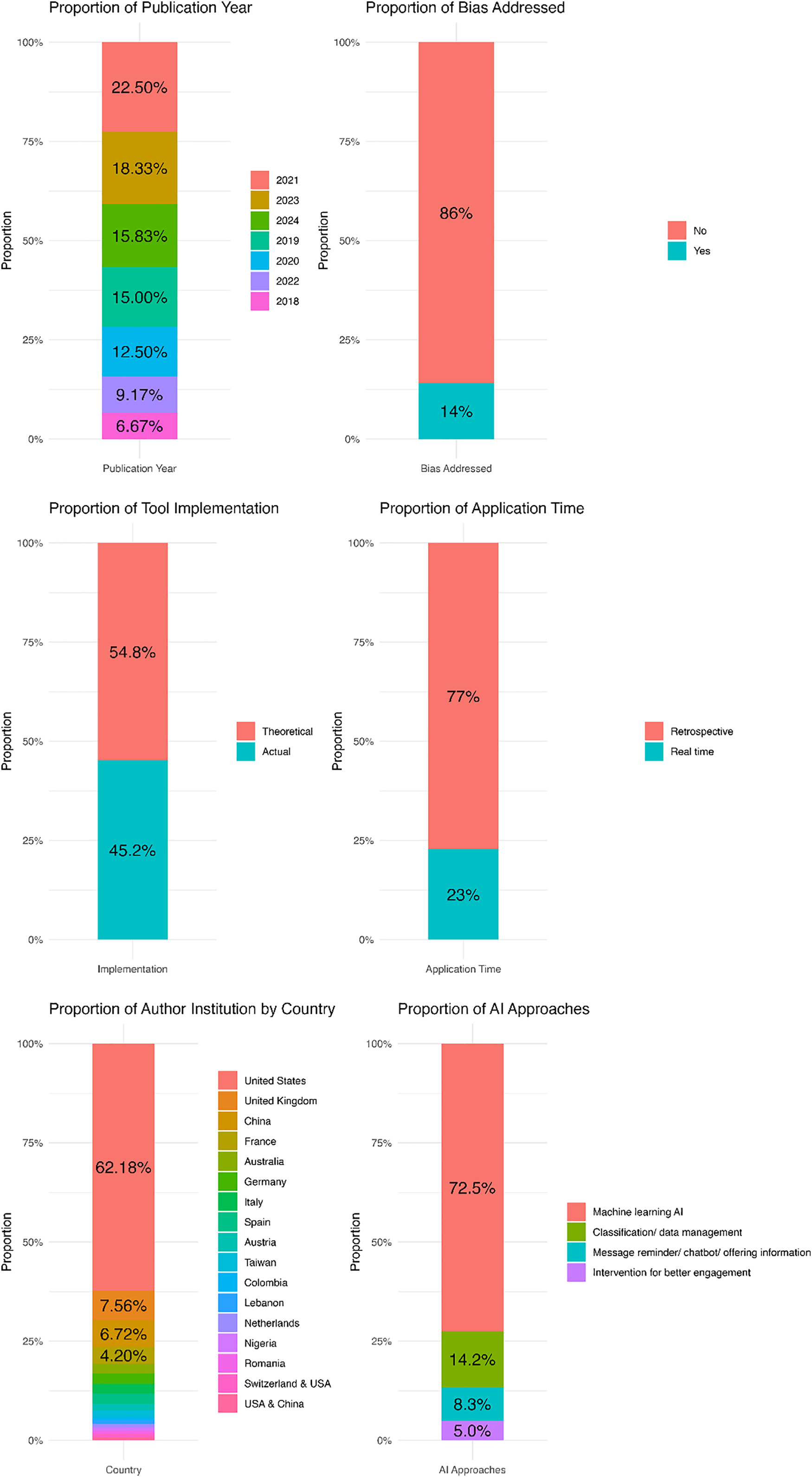
Figure 3 summarizes key study characteristics, including country, year, disease focus, AI approach, and bias consideration. Most studies were retrospective (77%) and published after 2019 (93.33%), with peaks in 2021 (22.5%), 2023 (18.33%), and 2024 (15.83%). The USA led in publications (62.18%), followed by the UK (7.56%) and China (6.72%). Only 14% addressed bias, and fewer than half (45.2%) applied to actual clinical trials. Most used general machine learning (72.5%), while others relied on rule-based methods. Full details are in Supplementary Material 1 (Appendix D: Others of the Appendix.additional content).
Clinical subject area & publication information. Most of the studies included came from institutions in the USA, and many did not explicitly address biases or disparities. Retrospective and theoretical AI applications predominated among these studies. Machine learning was the most commonly used AI approach.

Model performance
Primary endpoints
Different clinical trial recruitment and retention stages employed distinct endpoints for evaluating AI models. For patient screening, the true/false positives and negatives are usually defined based on whether the AI tool’s patient eligibility predictions match those determined by manual review or a clinical standard. For identifying eligibility criteria, the true/false positives often refer to whether correctly identified entities match reference annotations. For classifying eligibility criteria, the true positives and negatives usually reflect the correct classification of patient trial arm predictions, while false positives and negatives represent incorrect predictions compared against a manually annotated or gold-standard reference. For patient identification or cohort identification, the true/false positives and negatives are often based on whether the model’s predictions correctly or incorrectly match the manual annotations of potential eligible patients or cohorts.
These results were often reported in papers through model performance metrics, including sensitivity, specificity, accuracy, precision, F-1 score, and AUC. Among the studies we reviewed, for the screen patient category, sensitivity was the most frequently reported metric, appearing in 40% of included papers; however, other performance metrics were less common, with fewer than 30% of papers reporting F1 or AUC. For identifying and defining eligibility criteria, the endpoints usually consisted of the number of records or documents processed during criteria extraction. Sensitivity, specificity, accuracy, precision, F-1 score, and AUC were also commonly used to evaluate this type of AI tool; among these, precision was the most frequently reported metric at 57.1%. Studies focusing on identifying eligible patients or cohorts report the raw number of patients identified alongside model performance measures as a primary endpoint. For this category, sensitivity (30%) was the most frequently reported metric. Similarly, for classifying eligibility criteria, precision (66.7%) and the F-1 score (66.7%) were the most commonly reported endpoints for model evaluation. Details in Supplementary Material 1 (Appendix D: Others of the Appendix.additional content). Given that studies targeting different recruitment and retention stages prioritized various performance metrics, we have chosen to present the following metrics in the main text: the sensitivity of screening patients, the precision of identifying eligibility criteria, the sensitivity of identifying patients, and the precision and F-1 score of classifying eligibility criteria.
Patient screening
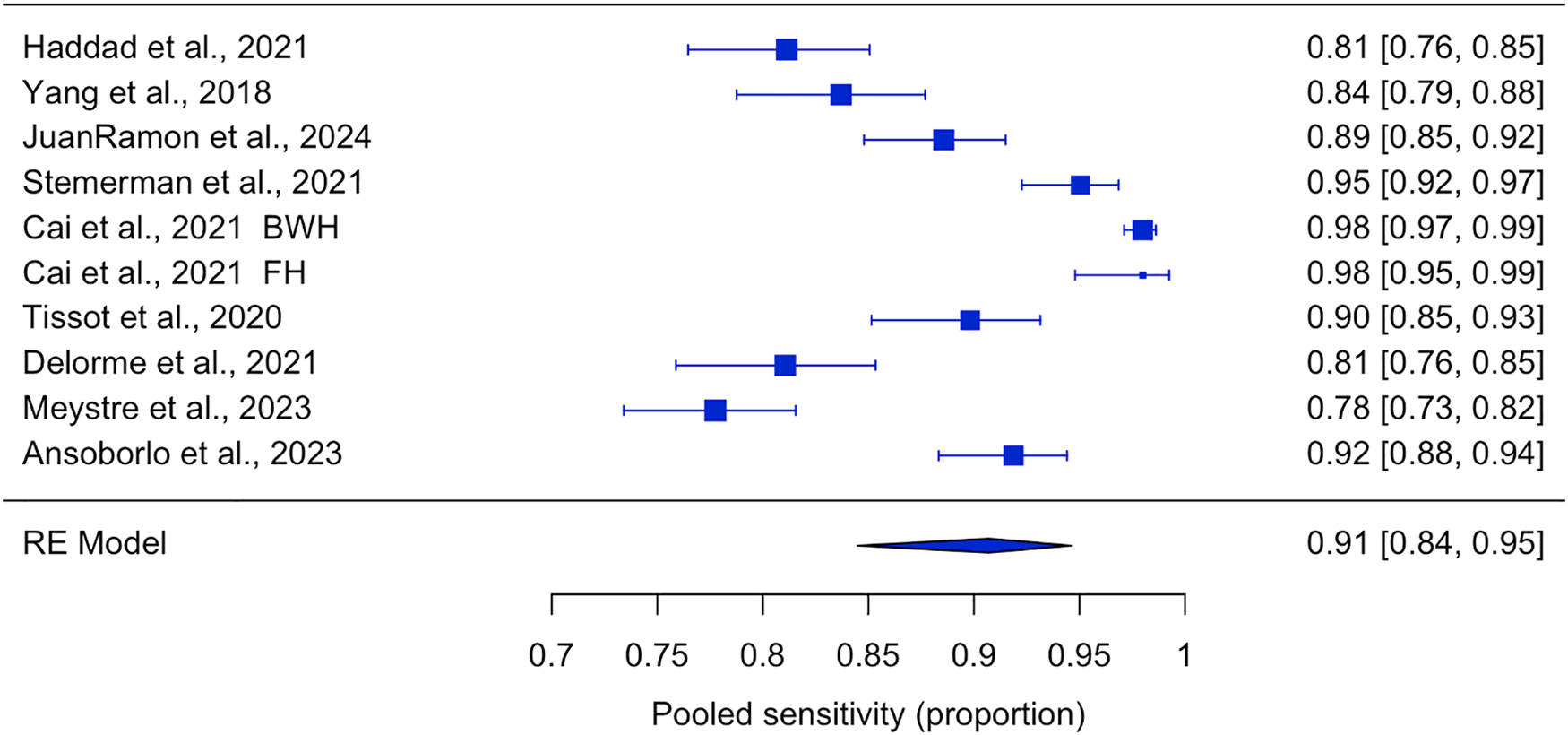
For patient screening, AI tools analyze health data and automatically enroll patients in suitable clinical trials. The efficacy of these tools was assessed through aggregated estimates of key metrics, including specificity, sensitivity, precision, accuracy, F1 score, and AUC. The sensitivity was relatively high, with a pooled estimate of 0.91 [0.85, 0.95] (Figure 4). The pooled specificity was 0.74 [0.33, 0.94]. Precision varied significantly across studies, ranging from 0.22 to 1.00. The pooled F1 score was 0.90 [0.85, 0.94], and the overall classification performance, represented by the area under the ROC curve (AUC), was 0.79 [0.72, 0.85]. The overall pooled accuracy consistently remained high at 0.95 [0.86, 0.98]. Details of all forest plots for the screening patients’ meta-analysis can be found in Supplementary Material 1 (Appendix C: Additional Figures of the Appendix.additional content).
Sensitivity meta-analysis for papers using machine learning for patient screening, with estimates represented by pooled proportions and 95% confidence intervals.

Identify eligibility criteria
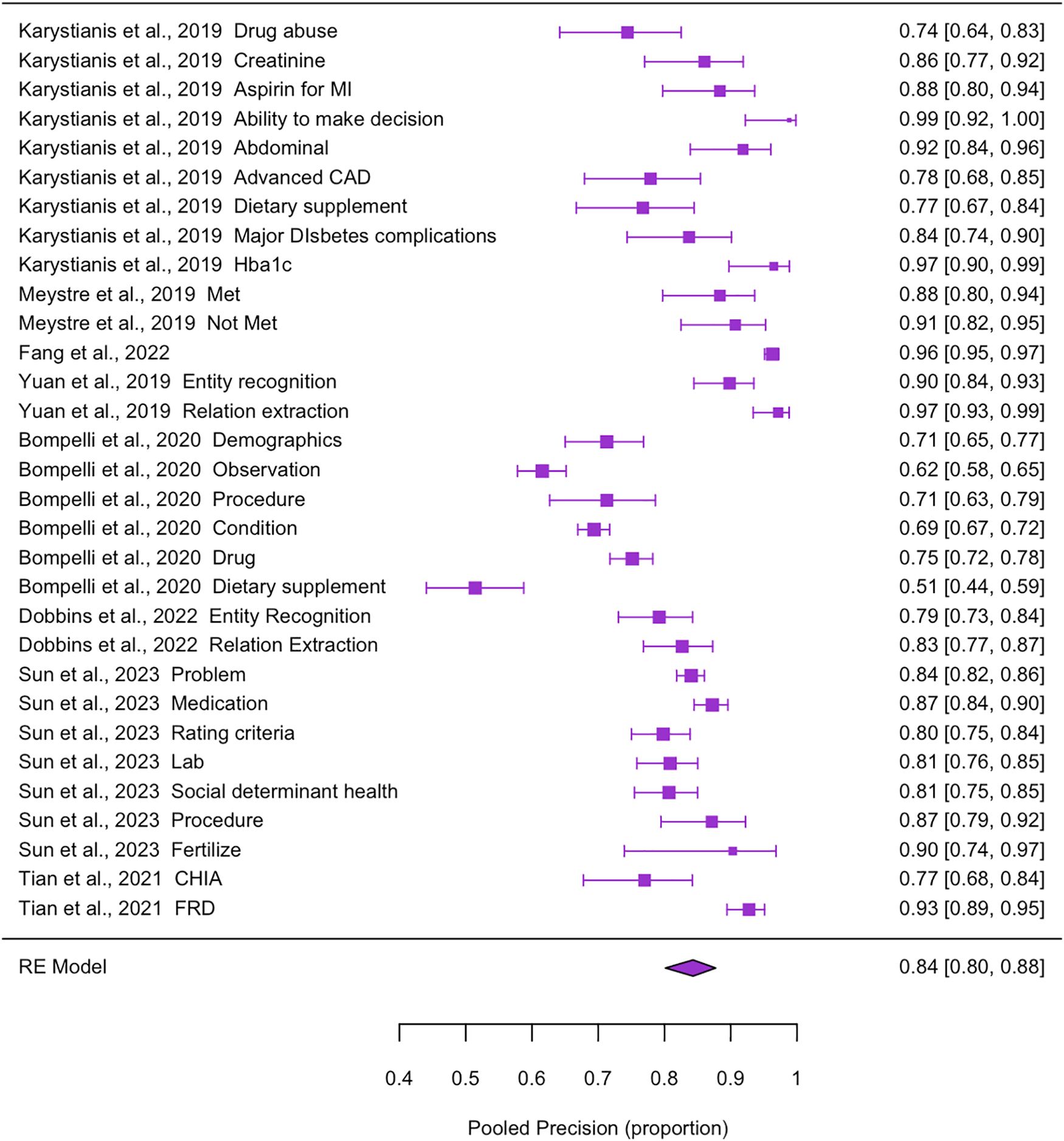
To identify and define eligibility criteria, AI tools analyze patients’ clinical records and automatically pinpoint the key medical attributes that align with the trial’s inclusion and exclusion criteria. The model’s performance was also assessed by aggregating key metrics from the included studies. The overall sensitivity was 0.80 [0.76, 0.84]. Pooled precision was relatively higher, with an estimated 0.84 [0.80, 0.88] (Figure 5). Overall accuracy reached 0.93 [0.89, 0.95]. The pooled F1-score was 0.80 [0.77, 0.83]. These results indicate that AI-based tools can systematically and reliably extract eligibility criteria. Detailed forest plots for the meta-analysis of identifying eligibility criteria can be found in Supplementary Material 1 (Appendix C: Additional Figures of the Appendix.additional content).
Precision meta-analysis for papers using machine learning to identify eligibility criteria, with estimates represented by pooled proportions and 95% confidence intervals.

Classify eligibility criteria
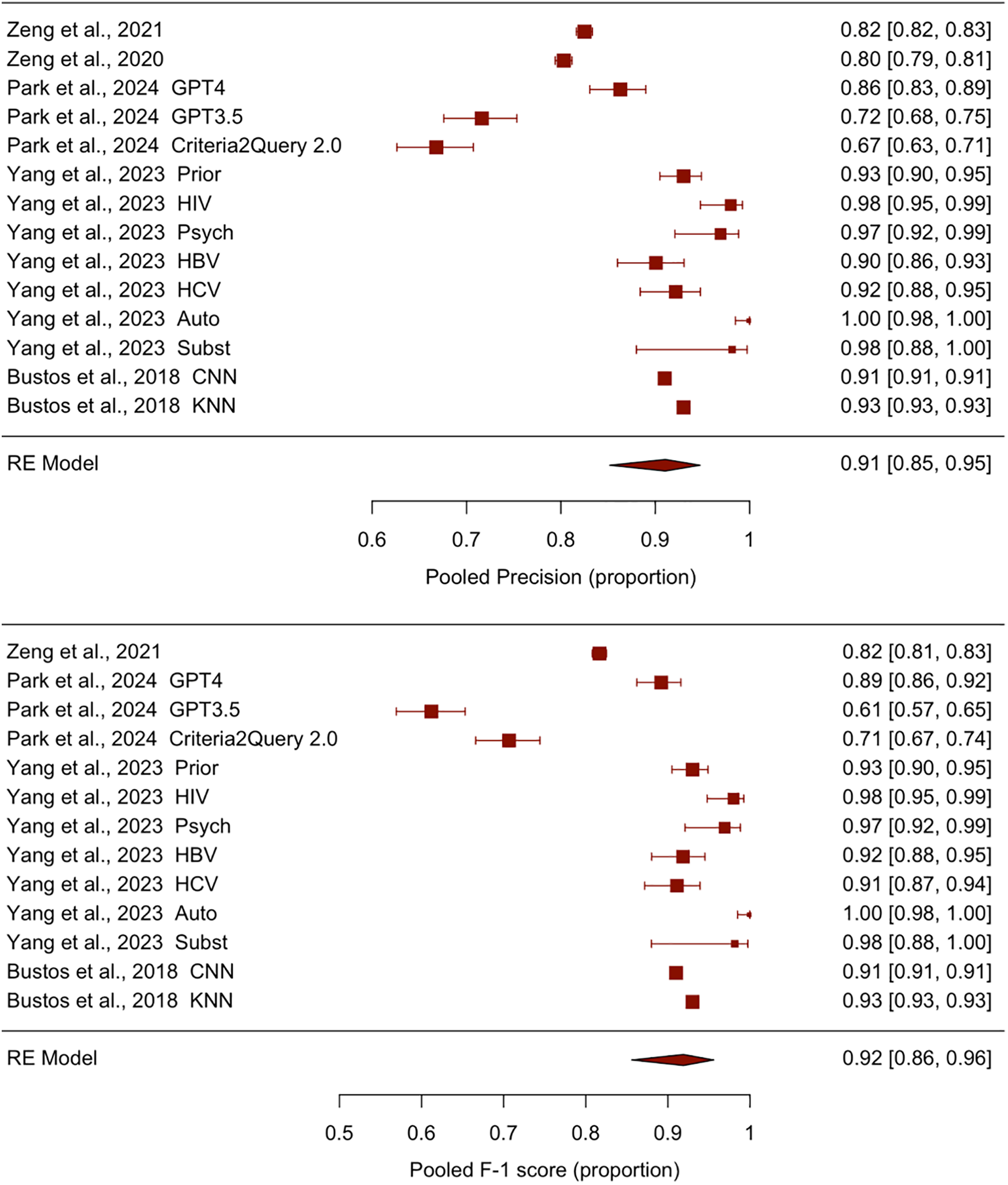
For classifying eligibility criteria, AI tools categorized clinical statements by distinguishing inclusion and exclusion criteria from standard clinical statements and organizing them into various domains. Among the included studies, the performance was encouraging. The pooled sensitivity reached 0.92 [0.84, 0.96], and the aggregated precision was similarly high at 0.91 [0.85, 0.95] (Figure 6). The overall accuracy was 0.94 [0.89, 0.97], and the F1-score was 0.92 [0.86, 0.96] (Figure 6). Ultimately, these findings suggested that the criteria were rarely misclassified, and the AI methods for automating classification proved valuable tools for enhancing clinical trial workflows due to their high reliability and effectiveness. Details of all forest plots for classifying eligibility criteria in the meta-analysis can be found in Supplementary Material 1 (Appendix C: Additional Figures of the Appendix.additional content).
Meta-analysis results for studies using machine learning methods to classify clinical trial eligibility criteria. The upper plot indicates the performance measured using precision, with estimates represented by pooled proportions and 95% confidence intervals. The lower plot indicates the performance measured using F-1 score, with estimates represented by pooled proportions and 95% confidence intervals.

Patient identification (identify patients/cohorts)
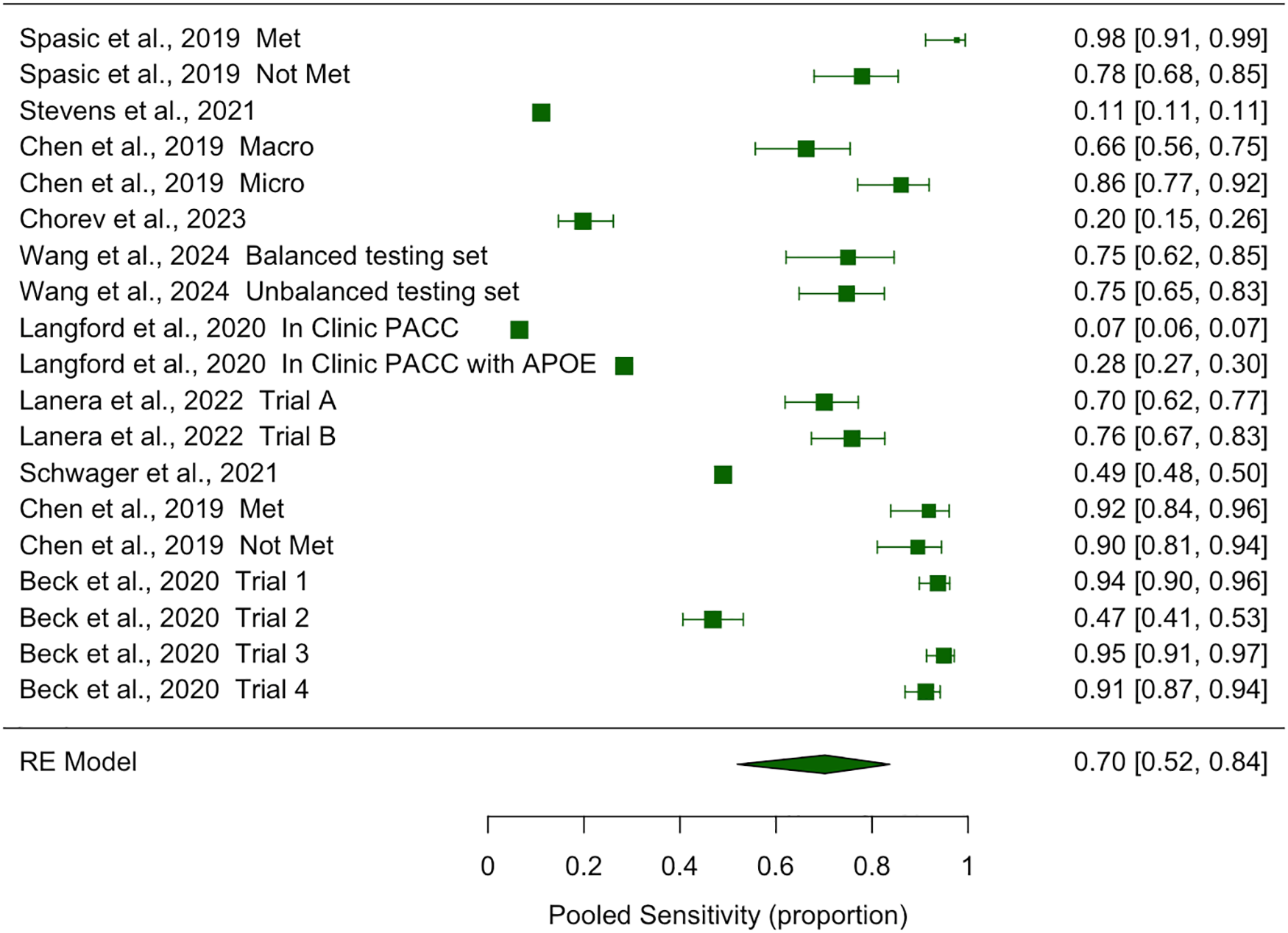
In studies utilizing machine learning techniques to identify eligible patient cohorts, the pooled sensitivity was 0.70 [0.52, 0.84] (Figure 7). The specificity was 0.79 [0.59, 0.95], and the precision was 0.69 [0.55, 0.80]. The pooled estimation and confidence intervals of sensitivity, specificity, and precision were lower compared to AI models managing other recruitment tasks, with the lower boundary of the interval nearing 0.5, indicating the relatively poor performance of AI-powered techniques in identifying patients and patient cohorts. Overall accuracy reached 0.81 [0.75, 0.86], and the aggregated AUC was 0.74 [0.61, 0.84], with an F1-score of 0.69 [0.32, 0.91]. Collectively, these findings reflect moderate discriminative performance. Details of all forest plots for identifying patients in the meta-analysis can be found in Supplementary Material 1 (Appendix C: Additional Figures of the Appendix.additional content). The detailed data for the subsequent recruitment and retention stages that have not undergone meta-analysis can be found in the Supplementary Material 5 (Appendix Table 4.categorization).
Sensitivity meta-analysis for papers using machine learning to identify patients/cohort, with estimates represented by pooled proportions and 95% confidence intervals.

Matching patients
Among the included studies, the accuracy ranges from 0.75 to 0.98, about one third of the studies [Reference Murcia, Aggarwal and Pesaladinne68,Reference Kusa, Mendoza, Knoth, Pasi and Hanbury71,Reference Gardner, Halligan and Fontana72,Reference Hassanzadeh, Karimi and Nguyen76,Reference Xu, Liu and Sun78] (5/16) output ranked list of clinical trials; and among these five studies, two of them [Reference Kusa, Mendoza, Knoth, Pasi and Hanbury71,Reference Hassanzadeh, Karimi and Nguyen76] evaluated the output relevance with information retrieval (IR) metrics. The included studies proved to solve patient matching barriers. For example, in the study by Jin et al. [Reference Jin, Wang and Floudas77], the TrialGPT (a patient labeling model built on GPT-4 and GPT-3.5), along with NLP and rule-based methods, resulted in significant time savings (42.6% overall, with the highest close to 95%). Another FairPM studies [Reference Chang, Yuan and Ding79] addressed fairness concerns by including sensitive attributes such as race and gender in their models. For both patient-criterion matching performance and patient-trial matching performance, FairPM demonstrated drastically reduced demographic parity and equal opportunity values while maintaining slightly reduced accuracy and F1-score compared to the baseline-biased model.
Evaluating AI tools
Seven studies developed AI tools that support various stages of the clinical trial recruitment and retention workflow through methods distinct from conventional approaches. For example, the study by Gligorijevic et al. (2019) [Reference Gligorijevic, Gligorijevic and Pavlovski105] developed a system to rank clinical investigators according to their projected enrollment performance, boosting recruitment efficiency by matching eligible investigators instead of participants. The study by Beaulieu et al. [Reference Beaulieu, Berry and Paganoni100] used structured clinical trial datasets from PRO-ACT and Answer ALS to evaluate a net penalized Cox proportional hazards model, which was developed for survival prediction for neurodegenerative diseases and the potential of trial admission. Overall, these seven AI approaches introduced novel approaches for streamlining clinical trial processes and demonstrated the potential to enhance recruitment effectiveness.
Digital tools
Digital tools were also applied to facilitate recruitment and retention workflows. For example, the chatbot-based eligibility assistants developed by Chuan et al. [Reference Chuan and Morgan82] demonstrated impressive performance (over 94% accuracy) and greater perceived usability and interactivity in addressing patients’ needs compared to traditional websites. Telemedicine platforms developed by Hardy–Abeloos et al. [Reference Hardy-Abeloos, Karp and Xiao84] conducted descriptive and comparative analyses for telemedicine’s impact on clinical trial enrollment odds, offering an alternative option to in-person visits, and the study indicated no significant difference in patient enrollment between Telemedicine and in-person consultations. Another study by Do et al. [Reference Do, Elbers and Fillmore85] built the MPACT platform for the Veterans Health Administration, integrating structured data from the Corporate Data Warehouse, unstructured clinical notes via NLP, and real-time patient schedules, resulting in a considerable reduction in patient data processing time (from 6 hours to under 1 hour). These studies collectively emphasized the potential of digital tools to increase the efficiency of clinical trial operations.
Offering clinical trial information
Providing additional clinical trial information to potential patient candidates has enhanced both clinical trial recruitment and retention. For instance, in Borno et al.’s study, the online platform Trial Library used ePath to enhance underrepresented patients’ interest in participating in cancer trials; a notable percentage of contacted patients completed trial surveys and were enrolled. In a study by Ma et al. [Reference Ma, Lowe and Berkowitz110], the EHR notification system for patient-provider communication increased recruitment by 10.1% through automatic notifications and referrals. Furthermore, AI-driven tools and educational platforms aimed at improving clinical trial literacy could lead to positive shifts in patient attitudes, including a greater willingness to participate in future trials.
Increase adherence and reduce loss
AI tools designed to improve adherence in clinical trials and minimize unwanted loss of follow-up are also essential tools that could enhance clinical trial retention. For example, a recommender system developed by Chen et al. [Reference Chen, Houston and Faro86] for smoking cessation and telehealth/video visits has been associated with an improved retention rate of between 60% and 85%. A real-time text processing system built by Delozier et al. [Reference DeLozier, Speltz and Brito95] could reduce the time required for drug events and study consent, cutting down follow-up time by 35% by simplifying the procedures between adverse events and patient consent. With the alert system in place, the monthly rate of diTdP enrollment was 4.15 times higher compared to traditional recruitment methods. Furthermore, a remote patient monitoring platform designed by Shafner et al. [Reference Shafner96] in a 2018 schizophrenia trial demonstrated improved adherence rates, with non-adherence ranging from 8.3% to 10.4% – a significant reduction from the 39%–50% non-adherence rates observed in clinical trials and real-world settings. Collectively, these examples illustrate the potential of AI tools in boosting clinical trial retention.
Heterogeneity assessment
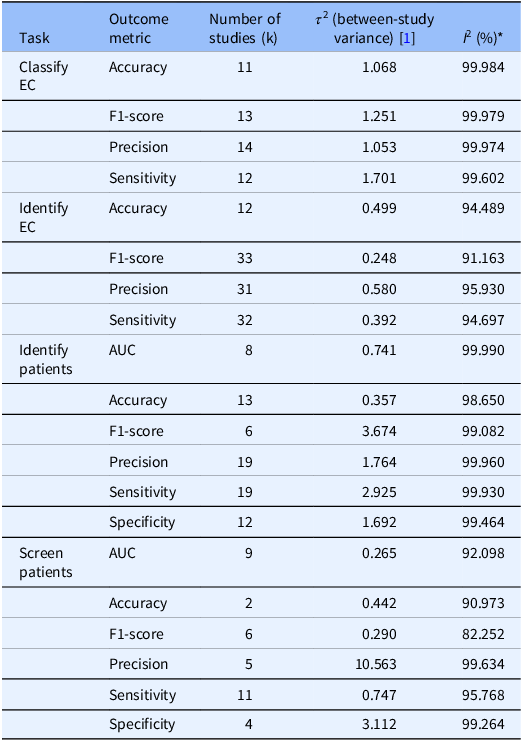
Heterogeneity is substantial across all task-metric strata, based on Table 2. The I 2 is consistently over 90%, indicating that most of the variability reflected real between-study differences rather than sampling error. There was dispersion expected; thus, the pooled means should be carefully read as descriptive summaries. Several strata have small k, which might inflate the heterogeneity; however, the persistently high I 2 and τ 2, even where k is large, confirm the between-study heterogeneity. Possible underlying reasons for the large between-study heterogeneity include differences in task definitions regarding different clinical trials, different underlying data sources, variation in model families/training, and the study design. Full details can be found in the Supplementary Material 2 (Appendix Table 1.heterogeneity assessment).
Between-study heterogeneity by task and metric: for each task–metric stratum, the number of studies (k), τ 2 (between-study variance), and I 2 (% variability due to heterogeneity) were reported. Consistently high I 2 indicates substantial cross-study dispersion in reported performance

* τ 2 and I 2 are rounded to 3 decimal places.
Discussion
Our analysis evaluated various AI tools used in clinical trial recruitment and retention, including patient screening, eligibility criteria extraction, and cohort identification. Overall, AI tools showed strong potential to enhance efficiency and reduce manual workload and costs. Studies reported high accuracy in pre-screening and exclusion of ineligible patients, reliable precision in extracting and defining eligibility criteria, and strong performance in classifying criteria with high sensitivity, precision, and accuracy. Cohort and site identification showed moderate discriminative performance, highlighting areas for further model refinement.
Limited coverage of preprint repositories
An important limitation of our search strategy is the lack of explicit querying of preprint-specific databases, such as arXiv, medRxiv, and OpenAlex. Even though our study covered an extensive scope of peer-reviewed studies, they didn’t reflect a systematic or exhaustive search of the broader preprint landscape. As preprints are increasingly relevant in fast-moving fields such as AI in healthcare, future reviews may benefit from incorporating dedicated preprint sources to ensure more comprehensive coverage.
Different focus of different models
Throughout all clinical workflow stages and performance metrics, the observed variability in plots was not solely determined by model reliability but also reflected differing model priorities. For example, some models were designed to avoid missing critical information, while others focused on minimizing the risk of enrolling ineligible patients. This divergence in prioritizing metrics led to a wide range in certain reported values (e.g., the specificity of screening patients varied from 0.46 to 0.95).
Heterogeneity of sample size
In our meta-analysis, sample sizes varied significantly across four categories. In the patient screening category, the number of patients evaluated ranged from fewer than 100 to tens of thousands. Similarly, in the patient identification category, datasets ranged from as few as 86 patients to as many as 72 million. In the eligibility criteria category, there was a notable heterogeneity in sample size, although it was less severe compared to the screening and identification categories, with a minimum of 86 annotated records and a maximum of 1600 entities. In the eligibility criteria classification category, sample sizes ranged from as small as 54 annotations to as large as 600,000 text-based samples, indicating significant variability.
Two primary factors likely contributed to this heterogeneity. First, the study design and the target disease can significantly influence variations in sample size. For example, under patient screening studies, Widera et al. [Reference Widera, Welsing and Danso53] had a sample size of 74 patients and focused on the progression of knee osteoarthritis, a more narrowly defined condition, while Shi et al. [Reference Shi, Kelsey and Sullivan113] evaluated nine different diseases, with a sample size of 86,292 patients. Second, data access could also be a potential reason for the sample size heterogeneity. For example, in the 2019 study by Chen et al. [Reference Chen, Warikoo, Chang, Chen and Hsu114], the investigators were assigned only 86 pre-annotated patient records, whereas investigators in the 2023 study by Hassan et al. [Reference Hassan, Ravi, Desai, Saei, Mckennon and Tekle115] had access to an entire structured EHR patient record. The large variability in sample size across models might affect the pooled outcome of the meta-analysis, and the estimates might not represent the underlying true effect, leading to reduced statistical power in the results.
Insufficient report of model performance
Most (n = 104, 83.2%) of the papers did not report all 5 metrics (sensitivity, specificity, precision, F1-score, and AUC) in the included studies. The details on how many models reported each performance matrix can be found in Supplementary Material 1 (Appendix D: Others of the Appendix.additional content). This inconsistency in reporting hindered the ability to generate comprehensive pooled estimates across all performance dimensions. Furthermore, some studies did not provide explicit sample sizes, which further diminished the statistical power and limited the robustness of pooling. Future research would benefit from integrating the existing guidelines [Reference Sounderajah, Ashrafian and Golub116,Reference Collins, Moons and Dhiman117] with an additional section for standardized performance reporting to ensure that all relevant metrics and sample sizes are consistently documented.
Fairness concerns
Only a small portion (16.8%, n = 21) of the studies in our review directly addressed concerns about bias. For example, models designed specifically to address disparities in transgender recruitment and the recommendation to exercise caution regarding the potential introduction of bias and decreased generalizability when utilizing synthetic cohorts in leukemia studies [Reference Kaskovich, Wyatt and Oliwa67,Reference Chen, Warikoo, Chang, Chen and Hsu114]. The details of the papers discussing bias have been documented in the Supplementary Material 5 (Appendix Table 4.categorization). Though rarely discussed, bias in AI tools for recruitment and retention is evident and stems from data and algorithmic processes. Unchecked, it risks being perpetuated. Addressing fairness is vital for credibility and progress in clinical trials.
Publication bias
Publication-bias signals were present in several task–metric pairs. Full details in the Supplementary Material 6 (Appendix Table 5.publication bias assessment). It indicated possible small-study effects and selective reporting, thus the related unadjusted pooled performances might be inflated. Full details of funnel plots are in Supplementary Material 1 (Appendix D: Others of the Appendix.additional content). The results should be interpreted cautiously and future studies should prioritize larger samples and complete metric reporting.
Preprints and evidence inclusion
Though our search strategy did not explicitly query standalone preprint repositories (e.g., arXiv, medRxiv), it is possible that a small number of preprint records were retrieved incidentally through databases we searched (e.g., PubMed Central, which has begun indexing select NIH preprints: https://pmc.ncbi.nlm.nih.gov/about/nihpreprints/). In this review, we did not include preprints in the final evidence base in order to minimize the risk and focus on peer-reviewed literature. Readers who wish to incorporate preprints can further expand the search to dedicated preprint repositories and then re-run the same screening workflow.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/cts.2026.10743.
Author contributions
Ziran Yin: Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Visualization, Writing-original draft, Writing-review & editing; Yun-Chung Liu: Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Visualization, Writing-original draft; Jonathan Chong Kai Liew: Data curation, Formal analysis, Investigation, Methodology, Validation, Visualization, Writing-original draft, Writing-review & editing; Rui Yang: Data curation, Formal analysis, Writing-original draft; Stephanie Hendren: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Writing-original draft, Writing-review & editing; Elisa Ma: Data curation, Formal analysis, Visualization; Zhaomei Geng: Data curation, Formal analysis; Jiahan Wang: Data curation, Formal analysis; Henry Foote: Conceptualization, Data curation, Formal analysis, Methodology, Supervision, Validation, Writing-review & editing; Christopher Lindsell: Conceptualization, Methodology, Supervision, Writing-review & editing; Chuan Hong: Conceptualization, Investigation, Methodology, Supervision, Validation, Writing-original draft, Writing-review & editing.
Funding statement
This research received no external funding.
Competing interests
The authors have no conflicts of interest to disclose.





 Open access
Open access