


Introduction
Hypoplastic left heart syndrome represents about 3% of all patients with congenital cardiac disease. Reference Grossfeld, Nie, Lin, Wang and Anderson1 In the United States, approximately 2000 infants are born with hypoplastic left heart syndrome every year. Reference Grossfeld, Nie, Lin, Wang and Anderson1 This heart problem is one of the most expensive of all birth defects, with estimated neonatal hospitalisation charges of approximately $200,000. 2,Reference Hansen, Madsen, Bishop, Morales and Anderson3
Management of infants with hypoplastic left heart syndrome is a complex and resource-intensive process. Most neonates with hypoplastic left heart syndrome undergo intervention with a Stage 1 palliation in the neonatal period to establish unobstructed systemic outflow with a restrictive pulmonary blood supply. This is commonly achieved via either the Norwood procedure with modified Blalock Tausig Thomas shunt (NmBT) (introduced in 1981), Reference Norwood, Lang, Casteneda and Campbell4 the Norwood procedure with a right ventricle to pulmonary artery conduit (NRVPA), also known as a Sano shunt (introduced in 2004), Reference Sano, Ishino, Kawada and Honjo5 or the hybrid procedure (introduced in 2002). Multiple reviews have been published to assess the consideration of the three techniques in the setting of single ventricle disease and overall outcomes, with little consensus on optimal choice, as this is patient- and centre-dependent. Reference Karamlou and Najm7–Reference Roeleveld9 Large studies comparing Stage 1 Norwood to Stage 1 hybrids identified higher early mortality in hybrid patients, similar interstage mortality, and hybrid patients require more re-interventions. Reference Cao10,Reference Rogers11
Several studies have described survival rates of infants with hypoplastic left heart syndrome treated with various management techniques. For example, the Single Ventricle Reconstruction Trial, published in 2010, showed that transplant-free survival by 12 months of age was 59% among patients who received the NRVPA and 54% among patients who received the NmBT. Reference Goldberg, Trachtenberg and William Gaynor12 In addition, this trial found that 1-year transplant-free survival rates were better for patients who underwent the NRVPA. Reference Goldberg, Trachtenberg and William Gaynor12 However, by the time patients reached 6 years of age, there were no significant differences between the NRVPA and NmBT cohorts in risk of death and/or transplant and catheter interventions. Reference Goldberg, Trachtenberg and William Gaynor12
While some longitudinal, multi-centre trends in initial Stage 1 procedure choice have been described within registry data, Reference Wirth, Heydarian, Marcuccio, Tepe, Stein and Hill13 the association among procedure choice, hospital costs, and patient outcomes such as in-hospital mortality and length of stay is unknown. Understanding procedure choice and outcome over time can help us determine modifiable factors to optimise patient survival, reduce hospital stay, and reduce hospital cost improving value delivered to our patients. We aim to describe the trends in initial Stage 1 procedure choice over time and to evaluate the association between procedure choice and patient health outcomes and costs using a multi-centre administrative database.
Methods
This study was considered exempt from human subjects research by the Johns Hopkins All Children’s Hospital Institutional Review Board (IRB #00325083).
Study design and data source
This retrospective multi-centre cohort study is reported according to the guidelines of the Strengthening the Reporting of Observational Studies in Epidemiology statement. Reference Cuschieri14
The data were obtained from the Paediatric Health Information System® maintained by the Children’s Hospital Association. This database collects encounter-level administrative and billing data from more than 40 non-profit paediatric hospitals that provide tertiary care in the United States. Reference O’Byrne, Song and Huang15,16 The quality of the data is assured through a joint effort between the Paediatric Health Information System, Children’s Hospital Association, and participating hospitals. Data are de-identified at the time of data submission and subject to several reliability and validity checks. Reference O’Byrne, Song and Huang15,16
Study cohort
The study included infants with hypoplastic left heart syndrome discharged from a Paediatric Health Information System centre between 1 January 2004 and 31 December, 2022, following admission for an initial Stage 1 palliation at age less than 30 days with either a Norwood operation or a hybrid procedure. Patients were identified using International Classification of Diseases versions 9 and 10 codes (ICD-9/10). For example, a patient who underwent a NRVPA was identified by the code for hypoplastic left heart syndrome and codes for a conduit between the right ventricle and the pulmonary artery. Similarly, a patient who underwent a hybrid procedure was identified by the code for hypoplastic left heart syndrome and codes for stenting of the ductus arteriosus as well as the restriction of pulmonary artery branches Reference Malik, Bird, Jaquiss, Morrow and Robbins17 [Supplementary Table 1]. If patients had more than one Stage 1 procedure, the chronologically first procedure was considered as the primary. Exclusion criteria were having had a primary heart transplant, more than one Stage 1 procedure on the same day, missing or implausible data for the day of service, and/or a qualifying procedure after the 30th day of life. Patients undergoing Stage 1 procedure after the 30th day of life may fundamentally differ from patients undergoing this procedure in the early neonatal period, making these groups unsuitable for comparison. Factors that may systematically differ between the two groups include late diagnosis, unclear diagnosis, other congenital heart anomalies, or extremes of gestational age and birth weight.
Study variables
The primary study exposure was the initial Stage 1 procedure, as defined by a categorical variable grouped according to whether the patient had the NmBT, the NRV-PA, or the hybrid procedure. The primary study outcome was the prevalence of initial Stage 1 procedures performed annually between 2004 and 2022. Secondary outcomes included in-hospital mortality, hospital length of stay (days), hospitalisation costs (dollars), and the presence of any complications. The Paediatric Health Information System® database estimates hospitalisation costs by converting charges transferred from hospitals’ billing records using a hospital-specific ratio of costs to charges. Reference McHugh, Pasquali, Hall and Scheurer18 Estimated hospitalisation costs were adjusted to 2022 dollars by multiplying the nominal estimated hospitalisation cost by the ratio of the 2022 Consumer Price Index (CPI-U) for all urban consumers to the CPI-U of the year in which the patient’s discharge occurred. Common initial Stage 1 procedure postoperative complications described in previous literature were identified using respective ICD-9/10 codes. Reference Ohye, Sleeper and Mahony19,Reference Tadphale, Tang, ElHassan, Beam and Prodhan20 Complications were categorised into organ systems as follows: neurologic, cardiac, pulmonary, gastrointestinal, renal, infectious, and haematologic complications [Supplementary Table 1]. A yes/no binary variable was constructed to indicate the presence of any of these complications.
Statistical analysis
Patient demographics and clinical characteristics were summarised by initial Stage 1 procedure choice with medians and interquartile ranges for continuous variables and frequencies and percentages for categorical variables. Study outcomes were pooled across discharge years and compared by Stage 1 palliation choice using χ2 or Fisher’s exact tests for categorical variables and Kruskal–Wallis tests for continuous variables. Mann–Kendall tests determined the presence of monotonic upward or downward linear trends over the duration of the study. Generalised linear multivariable mixed models were used to evaluate the adjusted association between initial Stage 1 procedure choice and study outcomes. A binomial distribution was used for outcomes of in-hospital mortality (yes/no), and the presence of any complications (yes/no), while a log-normal distribution was used for continuous outcomes of hospital length of stay in days and hospitalisation costs in dollars. Race and ethnicity, sex, discharge year, age at admission (days), birthweight (grams), and the presence of non-cardiac complex chronic conditions were hypothesised a priori to be associated with the outcomes and therefore included in the final multivariable models. Version 2.0 of the complex chronic conditions in the Paediatric Health Information System® database was used. Reference Feudtner, Feinstein, Zhong, Hall and Dai21 To assess the change in patient complexity over time, the average number of complex chronic conditions per patient was assessed over time. For each model, an interaction term of initial Stage 1 procedure choice by discharge year was included to test whether the association between initial Stage 1 procedure choice and study outcomes varied according to the discharge year. A Bonferroni adjustment was applied to the resulting P-values to adjust for Type 1 error. Interaction terms with an adjusted P-value ≥ 0.05 were removed from the final models. Missing data were not imputed. Two-sided P-values <0.05 were considered statistically significant. All analyses were conducted with Stata/SE Version 17.1 (StataCorp LLC, College Station, TX).
Results
Patient cohort
The Paediatric Health Information System® report was created on 6 April 2023. Overall, 7701 patients from 45 hospitals met the study inclusion criteria; 55 patients were excluded due to negative day of service. Study population characteristics according to the initial Stage 1 procedure type are displayed in Table 1. Among the included patients, 67.5% (n = 5194) underwent a NmBT, 22.1% (n = 1699) underwent NRVPA, and 10.5% (n = 808) underwent a hybrid procedure. The study population characteristics are displayed in Table 1. Among the total cohort, 62.1% of patients were male, 61% were born at or after 37 weeks of gestational age, 77.3% measured between 2500 and 4000 g, and 9.5% had a genetic or non-cardiac congenital defect.
Demographic and clinical characteristics of the overall cohort and by type of initial Stage 1 procedure

Percentages may not add exactly to 100% due to rounding.
Prevalence of procedure choice
The annual prevalence of NmBT decreased from 84.8% in 2004 to 29.9% in 2022 (P < 0.001 for trend), while the annual prevalence of NRV-PA surpassed the annual prevalence of NmBT in 2017 (53.6% vs. 42.4%, respectively). The sharpest observed decline in the annual prevalence of NmBT occurred between 2014 and 2017 [Figure 1]. In-hospital mortality prevalence for NmBT, NRVPA, and hybrid was 16.4%, 11.2%, and 27.2%, respectively. There were no observed trends in mortality over time (P > 0.05 for trend, for all procedure choices); however, the mean number of complex chronic conditions per patient increased consistently over the study period (p < 0.001, Supplementary Figure 1)
Annual prevalence of initial Stage 1 palliation type from 2004 to 2022. NmBT = Norwood with modified BT shunt, NRV-PA—Norwood with RV-PA conduit (Sano modification).

Hospital costs
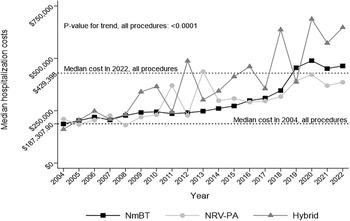
The median hospitalisation cost increased for all procedure types (P < 0.0001 for trend) [Figure 2] across the study period. In the pooled analyses, median hospitalisation cost for NmBT was $250,183.0 (Interquartile range (IQR) $159,463.0 to $425,285.0), while the cost for the NRVPA was $335,406.0 (IQR $208,624.0 to $583,322.0), and the cost for hybrid was $328,428.0 (IQR $169,224.0 to $662,385.0). The NRVPA was costlier than the other two options during its adoption period between 2011 and 2015. However, it has had the least median hospitalisation cost since 2016.
Median hospitalisation costs in adjusted USD 2022 dollars, from 2004 to 2022. NmBT = Norwood with modified BT shunt, NRV-PA—Norwood with RV-PA conduit (Sano modification).

Procedural complication
Table 2 illustrates the prevalence of complications according to the initial Stage 1 procedure choice pooled across the study period. Among the entire cohort, 77.3% of patients had at least one defined post-operative complication. The three most common types of complications were cardiac (50.5%), pulmonary (28.5%), and infectious (27.7%). The hybrid procedure had more cardiac complications (55.6%) than the other two procedure choices (P = 0.009). In comparison to the other two types of procedures, the NRVPA procedure had the lowest rate of pulmonary (22.3%; P < 0.0001) and infectious complications (21.8%; P < 0.0001).
Study outcomes for the overall cohort and by initial Stage 1 palliation choice

Percentages may not add exactly to 100% due to rounding.
Multivariable analyses
We did not observe any statistically significant interactions between procedure choice and discharge year in any of the adjusted models (adjusted P ≥ 0.05 for all). Given that the association between procedure choice and study outcomes was statistically similar across all discharge years, we pooled data from the study discharge years (2004–2022) and applied the multivariable models to these data. Results are shown in Supplementary data Figures 2–4.
Hospital cost
After adjustment for covariates, we found a significant association between procedure type and hospital cost. Specifically, in comparison to the NmBT procedure, the hybrid procedure was associated with higher costs (Exponentiated beta coefficient: 1.2, 95% confidence interval: 1.1 to 1.2), while the NRVPA procedure was associated with lower costs (Exponentiated beta coefficient: 0.9, 95% confidence interval: 0.8 to 0.9). In comparison to non-Hispanic White race and ethnicity, non-Hispanic Black (Exponentiated beta coefficient: 1.2, 95% confidence interval: 1.2 to 1.3) race and ethnicity was associated with higher hospitalisation costs. More recent discharge years (Exponentiated beta coefficient: 1.1, 95% confidence interval: 1.1 to 1.1) and higher age at hospital admittance (Exponentiated beta coefficient: 1.0, 95% confidence interval: 1.0 to 1.0) were associated with higher hospitalisation cost, whereas higher birthweight in grams was associated with lower hospitalisation cost (Exponentiated beta coefficient: 0.9, 95% confidence interval: 0.9 to 0.9). In comparison to having no non-cardiac complex chronic conditions, having 1 (Exponentiated beta coefficient: 1.5, 95% confidence interval: 1.4 to 1.6), 2 (Exponentiated beta coefficient: 2.0, 95% confidence interval: 1.9 to 2.2), or 3 (Exponentiated beta coefficient: 3.0, 95% confidence interval: 2.8 to 3.2) complex chronic conditions was associated with higher hospitalisation costs.
In-hospital mortality
In comparison to the NmBT procedure, the adjusted odds for in-hospital mortality were nearly twice as high for the hybrid procedure (adjusted odds ratio: 1.8, 95% confidence interval: 1.5 to 2.2), whereas the adjusted odds for in-hospital mortality for the NRVPA procedure were 30% less (adjusted odds ratio: 0.7, 95% confidence interval: 0.5 to 0.8). In comparison to Non-Hispanic White race and ethnicity, other race and ethnicity (adjusted odds ratio: 1.9, 95% confidence interval:1.5 to 2.5) was associated with higher odds for mortality. Discharge year (adjusted odds ratio: 0.9, 95% confidence interval: 0.9 to 1.0), male sex at birth (adjusted odds ratio: 0.8, 95% confidence interval: 0.7 to 0.9), having 1 (adjusted odds ratio: 1.5, 95% confidence interval: 1.3 to 1.8), 2 (adjusted odds ratio: 2.4, 95% confidence interval: 2.0 to 3.0), or 3 (adjusted odds ratio: 3.1, 95% confidence interval: 2.5 to 3.8) non-cardiac complex chronic conditions in comparison to none, and birthweight (adjusted odds ratio: 0.9, 95% confidence interval: 0.9 to 1.0) were also associated with in-hospital mortality.
Presence of any post-operative complications
In relation to the NmBT procedure, we observed that the adjusted odds for any complications were lower in the NRV-PA procedure (OR: 0.7, 95% confidence interval: 0.6 to 0.9). In comparison to non-Hispanic White patients, Hispanic patients of any race had 1.2 times greater odds for any complications (95% CI: 1.0 to 1.5). In comparison to having no non-cardiac complex chronic conditions, having 1 (adjusted odds ratio: 2.2, 95% confidence interval: 1.9 to 2.6), 2 (adjusted odds ratio: 3.4, 95% confidence interval: 2.7 to 4.2), or 3 (adjusted odds ratio: 5.7, 95% confidence interval: 4.2 to 7.9) complex chronic conditions was associated with higher odds for complications.
Discussion
Our data show that since 2017, NRVPA has emerged as the preferred initial Stage 1 procedure choice. Hybrid procedure rates have remained comparatively low throughout the study period, while since 2016, NRVPA had the lowest median estimated hospitalisation cost. NmBT patients had the lowest median length of hospitalisation during the entire study period. An increase in median estimated hospitalisation cost was observed across time for all procedure types, despite appropriate inflation-adjustment of the reported costs. Overall, NRVPA had the lowest mortality. While no significant temporal trend in mortality was observed, the prevalence of comorbid chronic conditions has increased over the same time period suggesting that patient complexity has increased while mortality has remained stable. This suggests that for some portions of the cohort, mortality has likely improved.
Our results support the results of the 2010 Single Ventricle Reconstruction trial that showed a 10.1% reduction in death or transplant by 12 months of age in the NRVPA group. Reference Ohye, Sleeper and Mahony19 It is also most likely that the increase in the NRVPA use as the preferred most of initial Stage 1 palliation is directly attributable to this landmark study. The sharp increase in the use of NRVPA in 2014 is consistent with the widely accepted axiom that it takes years for published research to change medical practice. Reference Morris, Wooding and Grant22
In-hospital mortality remained lowest for the NRVPA group in our study, as well as others in the literature. Reference Tadphale, Tang, ElHassan, Beam and Prodhan20 However, soberingly, our data show that the in-hospital mortality for these patients did not change over time. While it is possible that this reflects sobering odds despite ongoing advancements in cardiac surgery, cardiac anaesthesia, and paediatric cardiac intensive care, it is more likely that this reflects, at least in part, the increased patient complexity suggesting that for some subsets of this population, in-hospital mortality is likely improving. Similarly, it supports that as a field, we are taking on increased patient complexity without increasing the overall risk of mortality. Further study would be needed with more clinical granularity to better assess the risk factors for in-hospital mortality in these patients.
In-hospital mortality and total hospital cost in the patients with a hybrid procedure as the initial choice in Stage 1 palliation was the highest, likely related to the comorbidities that were more present in this population. Prior publications have found that infants who underwent the hybrid procedure had a higher prevalence of prematurity and chromosomal anomalies/syndromes compared to those who underwent traditional surgical Norwood operations. Overall, preoperative risk factors such as prevalence of shock, sepsis, mechanical circulatory support, and stroke were higher in this population. In addition, median weight at operation was lower among infants undergoing hybrid palliation versus infants undergoing Norwood palliation. Reference Karamlou, Overman and Hill23 Similar effects likely explain why outcomes were worse in the hybrid palliation group in our study.
As with any retrospective study, there is a possibility for residual confounding. Capturing patients with hypoplastic left heart syndrome and their initial Stage 1 palliation procedures and complications utilising International Classification of Diseases codes has inherent limitations in terms of data entry and data query. Any inaccuracy of the diagnostic codes may have resulted in misclassification of patients within the cohort. Moreover, the inaccuracy of time stamps necessary to classify the first palliation procedure may have similarly resulted in the misclassification of patients with more than one procedure performed. Costs were expressed by using estimated hospitalisation costs without further analysis of overall cost components such as clinical, imaging, laboratory, pharmacy, supplies, other, and unmapped costs. Given the limitations of administrative data, we do not have specific data regarding what might make particular patients higher risk for complications, morbidity, or mortality. Finally, we have no information within the database regarding what other patient-specific and institutional factors were considered in the decision-making process for each patient.
Conclusions
Our study shows that NRVPA has become the most frequently performed and lowest cost initial Stage 1 procedure for infants with hypoplastic left heart syndrome, as well as the safest. The cost of any index admission for a Stage 1 palliation procedure outpaced inflation. In the setting of increasing patient complexity, the in-hospital mortality rate did not significantly change for any palliation procedure during the 18-year study period. Additional studies to evaluate the most modifiable drivers of in-hospital mortality as complexity increases are needed in these patients.
Supplementary material
To view the supplementary material for this article, please visit https://doi.org/10.1017/S1047951125109992.
Financial support
This research received no specific grant from any funding agency, commercial entity, or not for profit organisation.
Competing interests
The authors declare none.
Ethical standards
No human or animal experimentation was conducted during the course of this research.






 Open access
Open access