


Introduction
CHDs affect approximately 1.1% of newborns, constituting the most common congenital anomalies.Reference Abela1 Advances in surgical techniques, interventional procedures, and perioperative care have significantly improved survival, enabling many children with CHD to reach adulthood.Reference Apitz2,Reference Banks, Rosenthal and Manlhiot3 However, these individuals face elevated risks of metabolic disorders, cerebrovascular events, and coronary heart disease.Reference Banks, Rosenthal and Manlhiot3 Regular physical activity is essential to mitigate these risks, yet participation is often curtailed by real and perceived safety concerns.Reference Blanchard, McCrindle and Longmuir4
Physical activity enhances cardiovascular health and quality of life.Reference Blanchard, McCrindle and Longmuir4 Despite rare instances of sudden cardiac events during exertion in those with CHD, overprotective caregivers and healthcare providers frequently restrict activity.Reference Dua, Cooper and Fox5,Reference Brudy, Hock and Häcker6 Due to secondary to activity restrictions and symptoms, patients with CHD often fail to reach the recommended World Health Organization exercise guidelines of at least 60 minutes of daily moderate-to-vigorous physical activity for children.Reference Brudy, Hock and Häcker6–Reference Gierat-Haponiuk, Haponiuk and Szalewska7 What is noteworthy is that most physical activity studies in CHD have been performed in North America or Europe and thus may not be generalised in other countries. In Oman, cultural and healthcare contexts may shape unique barriers to participation.Reference Dua, Cooper and Fox5,Reference Andreo, Crespo and Lloret8
The primary aims of this study were (a) to quantify physical activity levels in a cohort of Oman children with CHD, (b) to identify potential influencing factors in physical activity promotion, and (c) to assess awareness of physical activity patterns and barriers among caregivers and healthcare professionals in Oman.
Materials and methods
This cross-sectional study was conducted at Sultan Qaboos University Hospital and the National Heart Centre in Oman. Participants were children aged 5–18 years with CHD attending paediatric cardiology clinics from January 2019 to January 2023, identified via TrackCare® and Al-Shifa 3+® healthcare systems. Basic demographic data were collected from the chart review. Exclusion criteria included children with mental disabilities, cardiomyopathies, single ventricle patients, those who were unoperated or within three months post-surgery, and those with physical disabilities precluding activity.
Parents provided informed consent and completed a validated questionnaire via telephone interviews, assessing physical activity levels, influencing factors, and awareness of benefits and risks. The questionnaire consists of multiple-choice and yes/no responses, without any open-ended or narrative questions. (Appendix-1). The questionnaire was reviewed by a paediatric cardiology expert for content validity and piloted for 20 patients before the final approval. Data were securely stored at Sultan Qaboos University Hospital, accessible only to the principal investigator. Ethical approval was obtained from the Medical Research Ethics Committee (MREC#3088) and NHC (MoH/CSR/23/27601).
Statistical analysis
Descriptive Statistics: Continuous variables (e.g., age and activity hours) were summarised using means and standard deviations, while categorical variables (e.g., gender and CHD type) were reported as percentages. Inferential Statistics: Chi-square tests evaluated associations between categorical variables (e.g., residence type and activity participation). Linear regression assessed relationships with continuous variables, and multiple regression identified predictors, adjusting for confounders. A p-value < 0.05 denoted significance. Analyses were performed using SPSS version 27.0.
Results
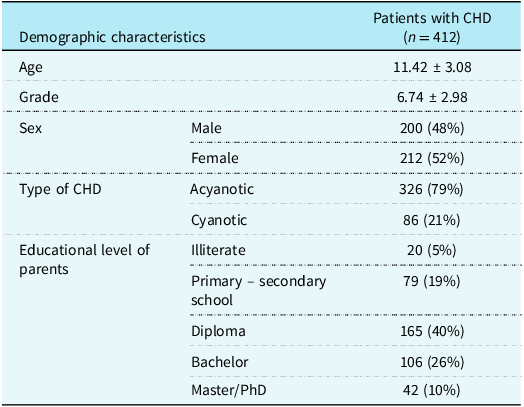
Of 412 enrolled children, 79% had acyanotic CHD, primarily atrial septal defects (15%) and ventricular septal defects (12%) (Table 1). Sex distribution was balanced. Parents permitted 68% of boys and 61% of girls to engage in physical activity, but this difference was not significant (p = 0.18).
Demographic and clinical characteristics of Omani children with CHD (n = 412)
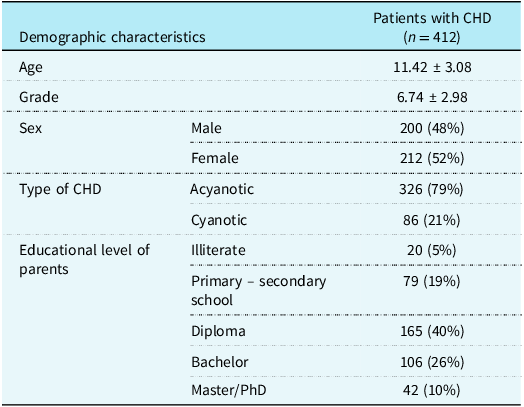
Values are given as mean ± SD or number (percentage).
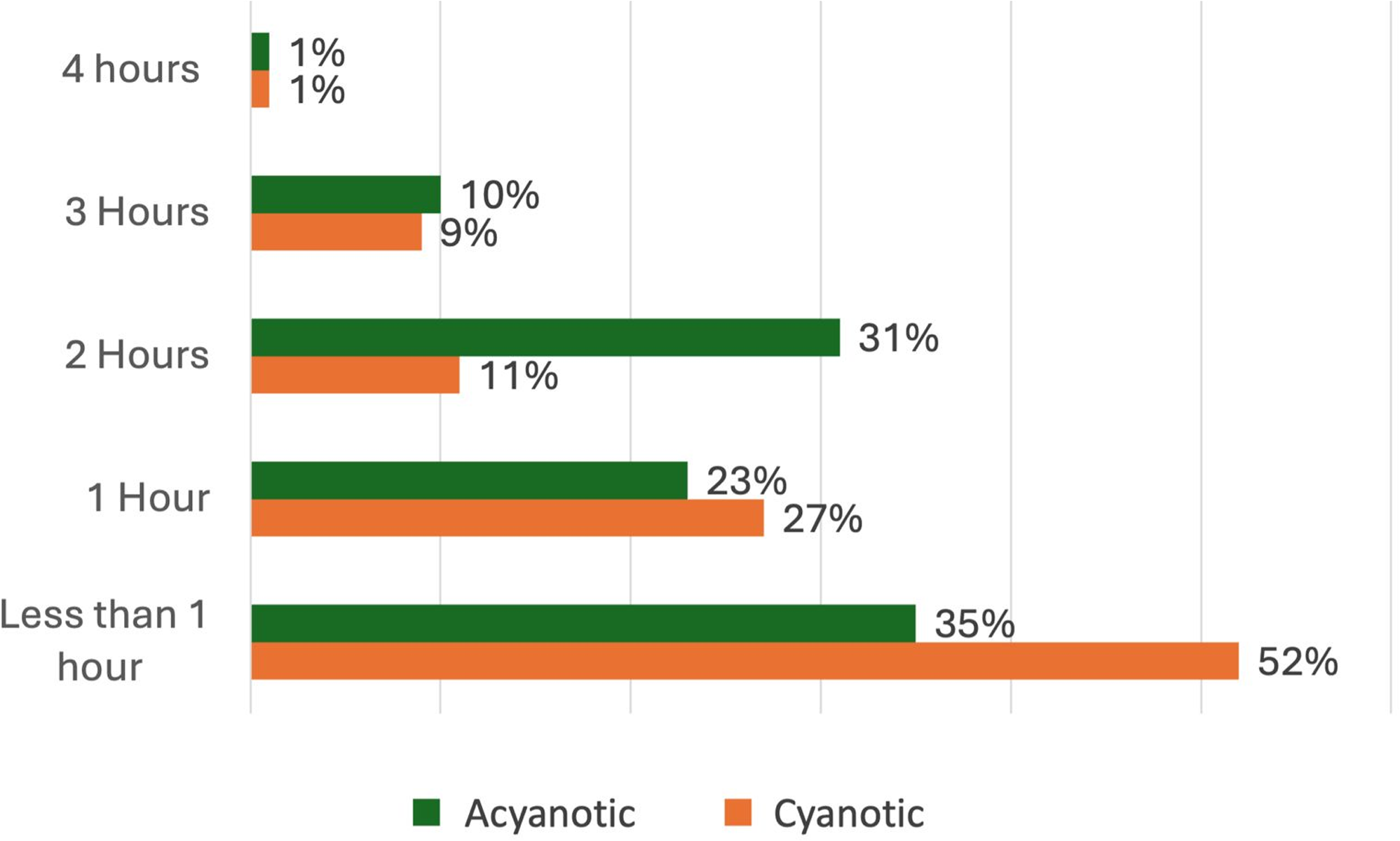
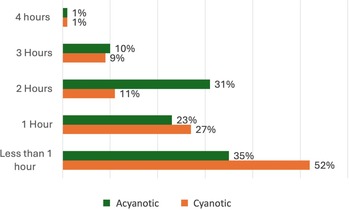
Mean weekly physical activity was 2.18 hours, with <1% achieving WHO’s 60-minute daily recommendation (Figure 1). Shortness of breath was the primary barrier to participation (5%), while concerns about sudden cardiac events were minimal (1%). Children with acyanotic CHD participated more (66%) than those with cyanotic CHD (45%), though this was not statistically significant.
Weekly physical activity duration (hours) among Omani children with congenital heart disease.
Children in houses (83% of sample, 64% active) were more active than those in apartments (17% of sample, 34% active; p = 0.004). Common activities included walking (65%), football (46%), cycling (39%), swimming (34%), running (29%), basketball (19%), and volleyball (4%).
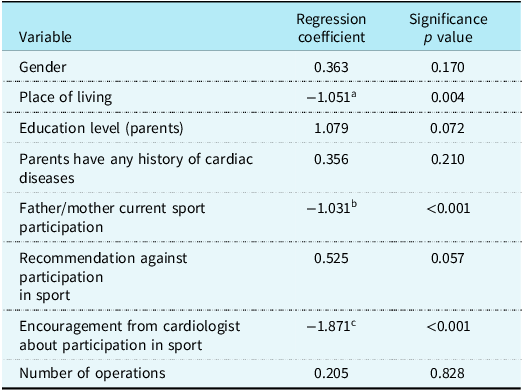
Multiple regression revealed that parental participation in physical activity (β = 0.42, 95% CI: 0.31–0.53, p < 0.001) and cardiologist encouragement (β = 0.38, 95% CI: 0.27–0.49, p < 0.001) significantly increased activity levels. Residence type was also significant (β = 0.22, p = 0.004). Sex, parental education, CHD type, and surgical history were not significant predictors (Table 2).
Multiple regression analysis of factors influencing physical activity levels in Omani children with CHD
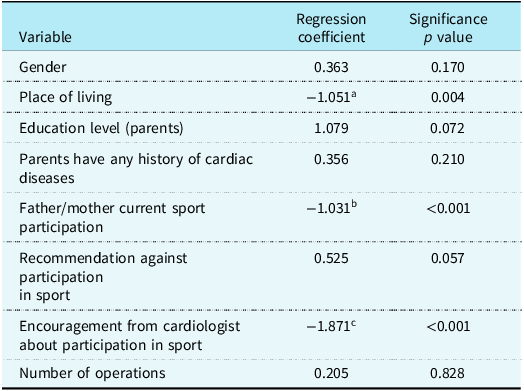
a Reduction of physical exercise in apartment living.
b Reduction of physical exercise in parents who do not participate in sport.
c Reduction of physical exercise in patients who are not encouraged by cardiologist to participate in sports.
Discussion
This study reveals that Omani children with CHD engage in an average of 2.18 hours of physical activity per week, significantly below the World Health Organization’s recommended 60 minutes of daily moderate-to-vigorous activity.Reference Gierat-Haponiuk, Haponiuk and Szalewska7 This finding underscores a critical public health challenge, as physical activity is essential for mitigating long-term risks of metabolic disorders, cardiovascular complications, and reduced quality of life in this population.Reference Banks, Rosenthal and Manlhiot3,Reference Blanchard, McCrindle and Longmuir4 The key facilitators—parental participation in physical activity and cardiologist encouragement (p < 0.001)—highlight the pivotal roles of family and healthcare systems, while residence type (house vs apartment, p = 0.004) introduces a novel environmental influence. These results align with global research but also reflect Oman-specific barriers, necessitating tailored interventions. In Oman, most of the apartments are not equipped with the necessary equipment for sport participation, while the houses are spacious, and the neighbourhoods most of the time are accessible for sport.
Facilitators of physical activity
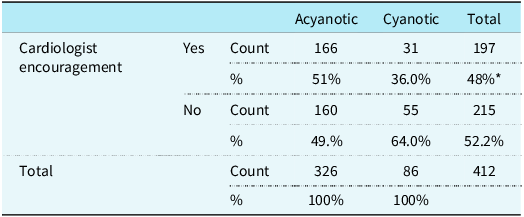
The significant influence of parental participation in physical activity (β = 0.42, p < 0.001) corroborates evidence that family lifestyle shapes children’s behaviours.Reference Abela1,Reference Andreo, Crespo and Lloret8,Reference Zumpf, Järvinen and Hager21 Parents who engage in physical activity likely model active lifestyles, fostering a supportive environment that encourages participation. This is particularly relevant given the finding that sedentary parental behaviours correlate with reduced activity in children with CHD.Reference Apitz2,Reference Murphy, Berrisford and Harris17 Similarly, cardiologist encouragement (β = 0.38, p < 0.001) emerged as a strong predictor, consistent with studies emphasising healthcare providers’ role in alleviating parental fears (Table 3).Reference Liem, Bink-Boelkens and Gatzoulis11,Reference Thomas, Barr and Berman14 For instance, Liem et al.Reference Liem, Bink-Boelkens and Gatzoulis11 noted that clear medical guidance significantly increases participation by dispelling misconceptions about exercise risks. In Oman, where traditional concerns about exertion in children with medical conditions persist,Reference Iommi, Pini and Comastri10 cardiologists’ proactive counselling could bridge knowledge gaps, particularly for parents hesitant due to perceived risks.
Relationship between cardiologist encouragement and CHDs (acyanotic vs cyanotic)
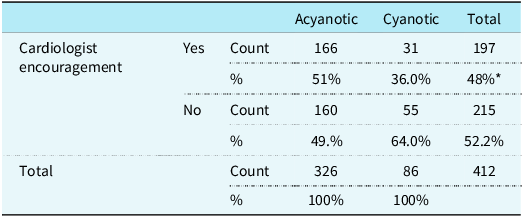
* Statistically significant < 0.001.
The higher participation among children living in houses (64%) compared to apartments (34%, p = 0.004) suggests environmental factors play a critical role. Houses in Oman often provide access to private yards or nearby open spaces, facilitating safe, unstructured activities such as walking or cycling. In contrast, apartment dwellers may face constraints such as limited indoor space or unsafe outdoor areas, a finding not widely reported in CHD literature. This aligns with broader research on environmental determinants of physical activity, which highlights the importance of accessible, safe spaces for children with chronic conditions.Reference Williams, Hicks and Tuncer12,Reference Chen, Zhao and Yu19 Future studies should explore whether urban planning or community infrastructure (e.g., parks, recreational facilities) could enhance activity levels in this population.
Barriers to participation
The study found that children with acyanotic CHD participated more (66%) than those with cyanotic CHD (45%), though this difference was not statistically significant. Shortness of breath, cited as the primary barrier, underscores the need for tailored activity plans that accommodate varying CHD severities. Notably, concerns about sudden cardiac events were minimal (1%), aligning with evidence that such events are exceedingly rare during exertion in CHD patients but somewhat surprising based on previous studies into kinesiophobia in this population.Reference Brudy, Hock and Häcker6,Reference Giannakoulas, Karatzis and Karanasios9,Reference Blake, Gough and Thomas16 For example, Giannakoulas et al.Reference Giannakoulas, Karatzis and Karanasios9 and Blake et al.Reference Blake, Gough and Thomas16 emphasise that with appropriate medical clearance, most children with CHD can safely engage in physical activity without heightened risk. This finding challenges overprotective attitudes, which remain a significant barrier in Oman, driven by cultural misconceptions about the safety of exertion.Reference Iommi, Pini and Comastri10,Reference Charbonnel, Martin and Paillot18
The predominance of community-based activities (e.g., walking 65%, football 46%) over structured school programmes suggests systemic barriers in educational settings. Although the study did not directly quantify school participation, global research indicates that school sports are often restricted for children with CHD due to policies prioritising safety, lack of tailored programmes, or teachers’ fear of liability.Reference Abela1,Reference Williams, Hicks and Tuncer12 In Oman, where physical education may not be fully integrated into school curricula for children with medical conditions, families may turn to community activities as a more accessible alternative. Williams et al.Reference Williams, Hicks and Tuncer12 advocate for inclusive school programmes that incorporate medical guidance to ensure safe participation, a strategy that could be adapted in Oman to reduce reliance on informal settings.
Psychological and social implications
Insufficient physical activity may exacerbate psychological challenges in children with CHD, such as impaired physical self-perception and reduced self-efficacy, as noted by Hall et al.Reference Hall, Stewart and Varela20 A sedentary lifestyle can lead to social isolation and diminished quality of life, particularly in adolescence when peer interactions are critical.Reference Abela1,Reference Brudy, Hock and Häcker6 Structured physical activity, even low-impact options like swimming (34% participation), can improve physical fitness and mental well-being, mitigating these effects.Reference Hall, Stewart and Varela20 The low participation rates in team sports like basketball (19%) and volleyball (4%) suggest missed opportunities for social engagement, potentially due to perceived risks or lack of CHD-specific coaching. Interventions should prioritise activities that balance safety with social benefits, fostering both physical and emotional health.
Cultural and policy considerations
Oman’s cultural context, where physical activity is less embedded in paediatric healthcare compared to Western settings, amplifies participation barriers.Reference Iommi, Pini and Comastri10 Unlike regions with proactive health-seeking behaviours, Omani parents often prioritise caution, influenced by traditional beliefs about exertion in children with medical conditions.Reference Liem, Bink-Boelkens and Gatzoulis11,Reference Charbonnel, Martin and Paillot18 This cultural nuance necessitates targeted, culturally sensitive interventions, such as community-based education campaigns that address specific fears (e.g., sudden cardiac events) with evidence-based reassurance. Charbonnel et al.Reference Charbonnel, Martin and Paillot18 and Chen et al.Reference Chen, Zhao and Yu19 highlight the efficacy of culturally adapted rehabilitation programmes, which could serve as a model for Oman.
From a policy perspective, the findings underscore the need for systemic changes. Oman’s healthcare system could integrate routine exercise counselling into paediatric cardiology visits, ensuring cardiologists are trained to provide clear, evidence-based recommendations. Schools should adopt inclusive physical education frameworks, supported by medical guidelines, to accommodate children with CHD. Additionally, urban planning initiatives could prioritise accessible recreational spaces, particularly in high-density apartment areas, to address environmental disparities. These strategies align with global calls for comprehensive CHD management that prioritises long-term health and quality of life.Reference Tran, Maiorana and Ayer13,Reference Marks, Memon and Pande15
Limitations
This study has limitations. Telephone interviews may introduce recall bias, as parents may inaccurately report activity levels. The lack of face-to-face interaction risks question misinterpretation, potentially affecting data quality. Excluding children’s and cardiologists’ perspectives limits the findings’ depth. Future studies should use objective measures (e.g., activity trackers) and incorporate diverse viewpoints for greater accuracy.
Future directions
Future research should address this study’s limitations, such as recall bias and the absence of children’s and cardiologists’ perspectives, by incorporating objective measures (e.g., wearable activity trackers) and multi-stakeholder input. Longitudinal studies could explore whether increased physical activity improves clinical outcomes, such as cardiovascular fitness or metabolic health, in Omani children with CHD. Additionally, qualitative research could elucidate cultural barriers, informing the design of effective interventions. Pilot programmes testing educational workshops or school-based initiatives could provide practical insights into scalability and impact.
In conclusion, this study highlights the interplay of familial, medical, and environmental factors in shaping physical activity among Omani children with CHD. By addressing cultural misconceptions, enhancing healthcare guidance, and improving access to safe activity spaces, Oman can foster healthier lifestyles for this vulnerable population, aligning with global standards for CHD care.
Conclusion
Omani children with CHD engage in insufficient physical activity, influenced by parental behaviour, cardiologist guidance, and residence type. To enhance participation, we recommend:
-
• Educational workshops for parents on safe physical activity.
-
• Training programmes for cardiologists to integrate exercise counselling into routine visits.
-
• Inclusive school initiatives to support physical activity for children with CHD.These strategies could improve health outcomes and quality of life for this population.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951125110366.
Acknowledgements
We would like to appreciate the help of the hospital information system in the Sultan Qaboos University and National Cardiac Centre.
Financial support
There was no relevant financial support to disclose.
Competing interests
There were no conflicts of interest to disclose.
Ethical standard
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008, and has been approved by the Medical Research Ethics Committee (MREC#3088) and NHC (MoH/CSR/23/27601).



 Open access
Open access