


Introduction
Restraint is sometimes used in hospital settings to facilitate the treatment of agitated patients, to prevent self-harm, and to protect staff and other patients.Reference Cannon1 Though used to avoid injury and decrease agitation,2 restraint may cause physical and psychological harm to the restrained patient and staff involved.Reference Butterworth, Spivakovsky and Oster3 Consequently, restraint is often perceived by staff as a “necessary evil.”Reference Wilson4 Impacting and infringing the interests and rights of patients — their dignity and autonomy — its use is ethically controversialReference Oster5 and divisive.Reference Cannon, Wilson, McSherry, Perez, Obasogie and Zaret6
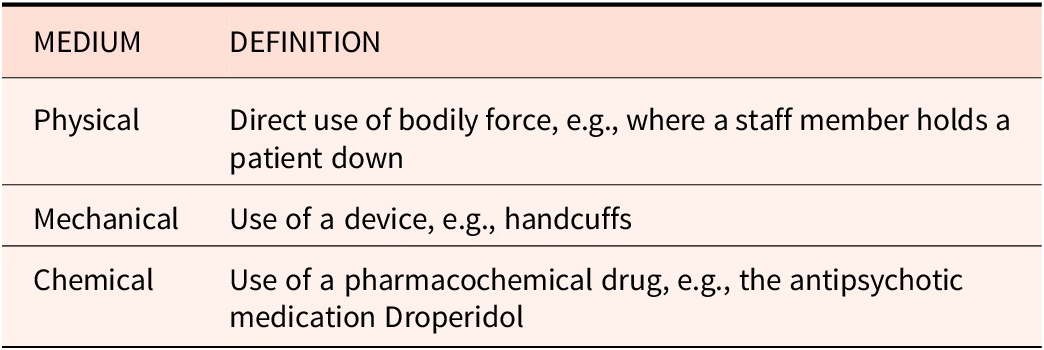
Restraint is defined as a “measure[] limiting a person in his or her freedom.”Reference de Bruijn7 It is used internationallyReference Spivakovsky and Savage8 and across a variety of hospital settings including psychiatric, geriatric, emergency, and intensive care.Reference Cannon, Conely, Campbell, Knott, Nirmalan, Smithard and Randhawa9 In the hospital context, overt restraint is administered using one of three “types” of medium — physical, chemical, or mechanical (see Table 1). Restraint rates, and the medium used, vary widely between countries,Reference Cannon and Oster10 hospitals, and individual wards within hospitals.Reference Oster11
Definitions of restraint mediums

Precise estimates of the prevalence of restraint, particularly outside psychiatric settings, are difficult to obtain.Reference Savage12 However, recent international research reports prevalence in psychiatric settings between 3.8% and 20% of patients.Reference Oster13 In Australia, only physical and mechanical restraint rates in acute specialized mental health services are currently reported.14 Recent national data in this setting indicates that in 2022–23, the physical restraint rate was 10 events per 1000 bed days and the mechanical restraint rate was 1 event per 1000 bed days.15 Data concerning the use of restraint in other hospital settings (i.e., emergency departments and intensive care) is not centrally collected or reported. However, studies suggest that restraint is regularly used in Australian intensive care unitsReference Perez and Perez16 and emergency departments, where it is estimated that the rate is 3.3 events per 1000 presentations.Reference Cannon17 It is difficult to accurately assess where Australia sits among other similar (i.e., high-income) countries internationally due to differences in definition and reporting requirements, as well as in the methods used to collect and report data.Reference Belayneh, Lepping and Janssen18
The purpose of restraint and the methods employed also vary considerably within and between hospitals.Reference Oster19 For example, in intensive care restraint is often used to prevent therapy interruption or self-harmReference Cannon20 — patients may be mechanically restrained (e.g. using [soft] wrist restraints) to prevent them from removing uncomfortable medical equipment.Reference Perez21 In psychiatric settings, chemical, physical, and (rarely) mechanical restraints may be used to manage “challenging [patient] behaviors,”Reference Block22 including high-risk and/or dangerous behavior.Reference Butterworth, Spivakovsky and Block23 The most common indications for restraint in emergency settings are violence, psychosis, and behaviors related to acute brain trauma.Reference Knott24 In this setting, patients are generally chemically restrained.Reference Cannon and Knott25 Restraint is also reported to be implemented in response to staff shortagesReference Butterworth, Block and Smithard26 and poor ward administration and management.Reference Perez and Block27
The effectiveness of restraint is contested.Reference Spivakovsky, Cortinhal, Dafny, Muller, Marangos-Frost, Wells, Méndez, McSherry and Maker28 It is reported that, appropriately managed, restraint can be used safely and achieve positive results,Reference Perez and Carr29 allowing hospital staff to provide necessary care and restore health.Reference Jansen30 Its use, however — particularly in psychiatric settings — is associated with both direct and indirect physical and psychological adverse outcomes for the patient,Reference Butterworth, Perez and Evans31 their caregivers,Reference Perez32 and staff involved.Reference Block and Jansen33 Hospital staff, particularly nurses, also regularly experience feeling “shame,” “guilt,”Reference Lamoureux34 and internal conflict about the use of restraint. This is often referred to as moral distress.Reference Perez35 The risk of adverse outcomes increases when restraints are applied without appropriate oversight.Reference Perez36 There is overwhelming consensus that, particularly outside mental health care settings, restraint is under or poorly regulated,Reference Thomann and Perez37 and otherwise that its use “should be minimize[d]”Reference Perez38 or eliminated.39 However, despite these risks to patients and themselves, staff — particularly in managing patients with challenging behaviors — report “significant fear[s]”Reference Muir-Cochrane40 about the potential elimination of the practice.Reference Block, Jansen and Kodua41
The use of restraint in hospital settings runs counter to international law,Reference Spivakovsky, McSherry, Pértega and Holmberg42 its use perceived by some as a violation of the right to liberty and security, the right to be free from violence and abuse, the right to integrity of the person, and the right to privacy43 — all rights protected at international law.44 Its use in mental health care settings is particularly condemned, with the United Nations Special Rapporteur on torture and other cruel, inhuman or degrading treatment or punishment calling for an “absolute ban”Reference Méndez45 on the practice, declaring its use to be akin to torture and a breach of human rights.Reference Spivakovsky46 Calls for the elimination of restraint in healthcare settings are gaining momentum internationally.Reference McSherry, Roper and Borckardt47 This sentiment is reflected in Australia, including in the state of Victoria. For example, one of the key recommendations of the 2021 Royal Commission into Victoria’s Mental Health System (Royal Commission) was that the Victorian Government “act immediately to [end] the use of … restraint.”Reference Armytage48
Largely the purview of state regulation in Australia, restraint is the subject of disparate legislative arrangements. Commencing in September 2023, Victoria’s Mental Health and Wellbeing Act 2022 (MHWA) is the most recent Australian legislation defining and regulating restraint — including, for the first time, chemical restraint — in hospital settings. Part 3.7 of the MHWA regulates the use of restraint, and confines its use to circumstances where it is necessary to
-
1. prevent imminent and serious harm to the person or other persons; or
-
2. in the case of bodily restraint, to administer treatment or medical treatment to the person.
Where restraint is used pursuant to the MHWA, the Chief Psychiatrist must be notified.49 Reflecting the recommendations of the Royal Commission,Reference Chesterman50 an express objective of the MHWA is: “[t]he reduction in the use of … restraint with the aim of eliminating its use within 10 years” (s.12(c)(ix)). This objective ignores the challenges evidenced in the experiences of hospital staff who feel compelled, at times, to restrain patients to facilitate treatment and otherwise protect themselves and others.Reference Marangos-Frost, Wells and Lind51 Anecdotally, Victorian hospital staff are concerned about the implications of the MHWA for staff and patient safety, and ultimately the quality of care provided.Reference Ore52
Given the level of international concern expressed about the use of restraint in hospital settings — both from a clinical perspective (i.e., its likelihood to cause harm) and a moral or ethical perspective (i.e., tension between the competing interests of the patient and others) — it is unsurprising that there is a substantial body of literature investigating the where, when, and how of restraint in hospital settings.Reference Cannon, Chesterman, McSherry, Perez, Pértega and Holmberg53 This literature addresses practical or descriptive questions about the practice, including its prevalenceReference Cannon and Knott54 and impact on patients and staff,Reference Butterworth, Perez, Perez, Marangos-Frost, Wells, Jansen, Evans, Lamoureux, Kodua, Lind and Chavulak55 in a variety of settings. There is a particularly rich body of literature describing the use and regulation of restraint in psychiatric, senior care, and disability settings.Reference Spivakovsky and Chesterman56 However, there have been few systematic attempts to examine the conceptual and normative dimensions of the practice, particularly in general hospital settings.Reference Hall and Smithard57 Instead, the ethics literature tends to consider the practice in specific contexts, predominantly psychiatric and geriatric settings.Reference Obasogie, Zaret, Conely, Campbell, Cortinhal, Marangos-Frost, Wells, Chavulak, Sashidharan and Chieze58
The tension between an elimination policy and the perception held by many hospital staff of restraint as a “necessary evil”Reference Wilson59 necessitates consideration of the underlying ethics of patient restraint in hospitals. In responding to this gap, this paper addresses the following questions from an ethical perspective:
-
1. What is restraint?
-
2. How is restraint best conceptualized for ethical analysis? Specifically, what type of ethical framework should be used in practice to evaluate potential instances of restraint in hospitals?
Our argument is in three parts. In the first, we consider the definition of restraint. We argue that current definitions in the ethics literature are not fit for purpose and suggest that restraint is more usefully conceptualized as a continuum between therapeutic restraint and public-safety restraint. In the second part, we explore the dominant ethical frameworks used to understand restraint in the current literature: human rights and principlism. We argue that, due to their exclusively individualistic foci, neither of these frameworks provides a satisfactory approach to addressing the ethical tensions posed by restraint. In the third part, we suggest that an ethical approach grounded in public health ethics (PHE) may better address these tensions. We suggest that, in certain contexts, the intent and impact of an act of restraint are similar to the intent and impact of a public health intervention (PHI). Given this similarity, and that a PHE framework provides scope to consider third-parties’ interests while safeguarding the interests of individuals, this framework provides a better approach to considering the ethical justifiability of restraint.
Critical Interpretive Review
As a starting point for defining restraint and exploring the ethical justification for its use in hospital settings, we conducted a critical interpretive review (CIR) of the existing ethical literature on the use of restraint in hospital settings. A CIR is a literature review method specific to the discipline of bioethics designed to generate new ideas and theories about ethical justifiability through critical engagement with existing literature.Reference McDougall60
Search Strategy
We identified literature on the ethics of using restraint in hospitals by searching titles, abstracts, and keywords in SCOPUS and MEDLINE Ovid in March 2024. We conducted an additional search using Philosopher’s Index in April 2024, to identify and capture any philosophical literature not referenced in the other databases. We selected these databases with the assistance of a research librarian, to facilitate a comprehensive search of biomedical and philosophical/ethical journals. The search terms are listed in Table 2 and aimed to capture literature at the intersection of ethics, restraint, and hospital care.
Search Terms

We selected these terms after initial searches demonstrated their effectiveness at identifying relevant literature. Other search terms we trialled included “immobilization” and “sedation,” but these were discarded given their tendency to exclusively identify literature considering the use of restraint in contexts outside the scope of our research. We also searched the reference lists of included publications.
Inclusion Criteria
Though primarily interested in the use of restraint in general hospital settings, we did not exclude literature exclusively considering its use in psychiatric settings given the overlap of relevant normative considerations between these settings. For similar reasons, we did not exclude literature addressing specific patient populations. We did, however, exclude literature which concerned the restraint of patients also criminally detained given the overlay of the custodial setting.
To answer our research questions, it was essential that publications use ethical concepts as a tool in their analysis. For example, several qualitative research studies of the experience of nurses administering restraint in hospital settingsReference Marangos-Frost, Wells, Jansen and Muir-Cochrane61 were excluded. Though these publications provided a rich description of the moral experience of nurses administering restraint, they otherwise did not engage with the question of whether the practice was itself ethically justified. For this reason, literature exclusively considering the legal aspects of restraint was also excluded — for example, literature which presented a comparative legal analysis of domestic and international legislation.Reference Chesterman62
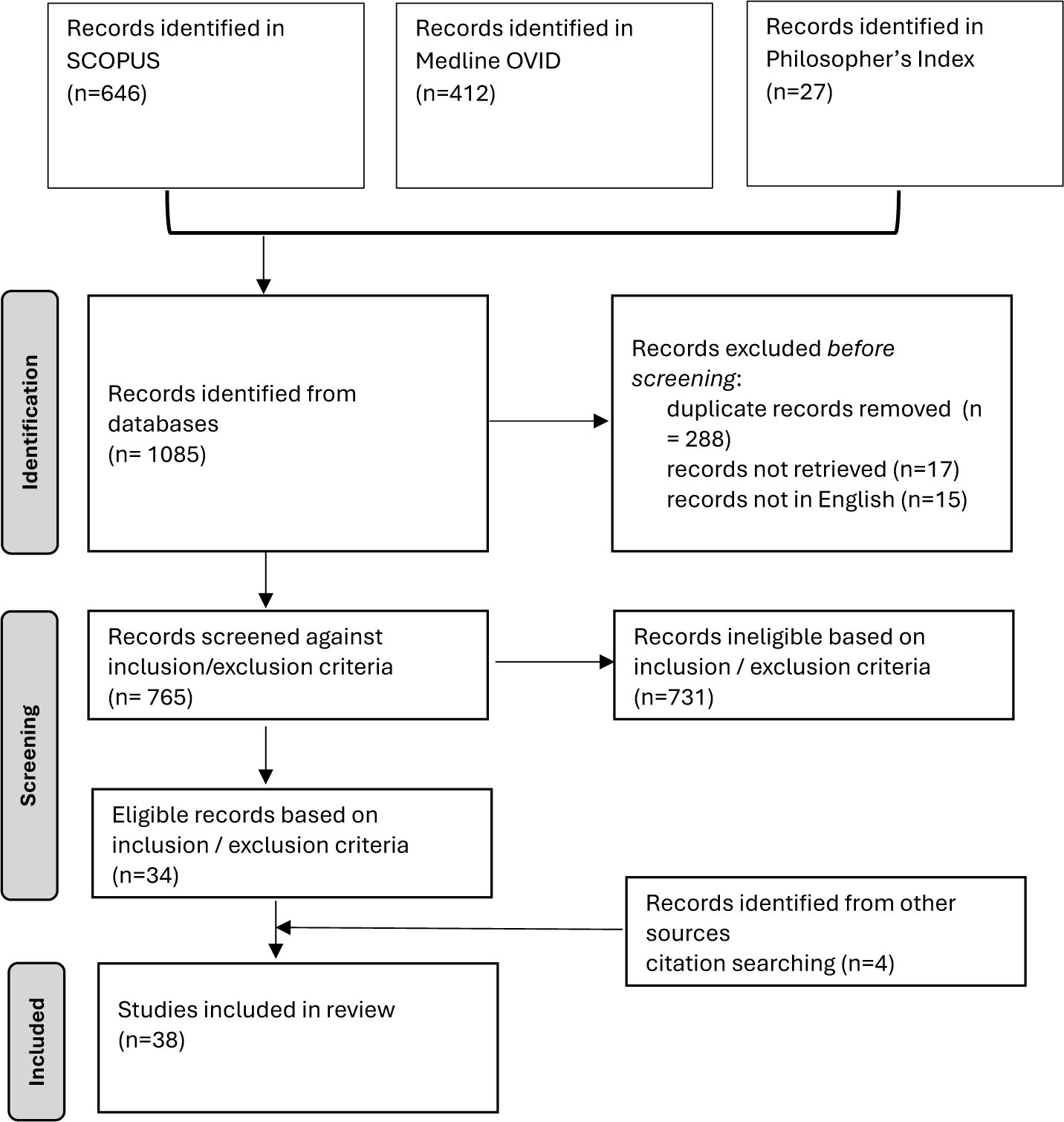
Screening involved two stages. First, Author 1 screened titles and abstracts against the inclusion and exclusion criteria (see Table 3). Author 1 then reviewed the full text of any publications that she had initially been unsure about; any remaining uncertainties were resolved through discussion with Author 2. Consistent with the CIR method, quality assessment was reserved for the analysis stage, forming part of the critical analysis and interpretation of the arguments — which included “judgements and interpretations of [their] credibility and contribution.”Reference Dixon-Woods63 A PRISMA diagramReference Page64 describing the search process is at Figure 1.
Screening Criteria

Prisma Diagram.

Our review identified 38 relevant publications from a range of ethical (n=16) and clinical (n=22) sources. Of these, sixteen were published or considered restraint in North America, twelve in the United Kingdom, four in continental Europe, four in Australia, and two in China. The earliest article was published in 1986,Reference Sclafani65 however the majority were published post-2010. Particularly interesting were the authors’ professional backgrounds, with all but two publicationsReference McSherry and Roper66 including at least one author with a clinical background and/or role; of these the majority were nursing. Details of the 38 publications are included in a supplementary file.
From each paper, Author 1 extracted
-
1. the definition of restraint used;
-
2. criteria and guidance for its use; and
-
3. the ethical framework utilized.
Both authors synthesized these findings and considered the arguments of each publication — both in isolation and in the context of the entire body of literature — identifying any consistencies, inconsistencies, and omissions. This process facilitated the critical analysis and assessment of the literature,Reference McDougall, Williams and Dawson67 which grounded the subsequent consideration of — and answers to — our research questions.
Part I: Defining Restraint
Our searches identified several publications which provide an explicit definition of restraint.Reference Hall, Smithard, Feder, Bray and Fitzgerald68 However, the majority rely on a common understanding of the term and only define the types of restraint as outlined in Table 1. Publications are predominately concerned with the application of either
-
1. physical and mechanical restraint; or
-
2. physical, mechanical, and chemical restraint.
Four papers identify other types of restraint. Priesz and Priesz (2019) refer to, but largely dismiss, the notion that removing access to technology may constitute restraint, and Behrman and Dunn (2010) briefly discuss the use of “environmental” restraints (e.g., bedrails to prevent patients from leaving their beds). By contrast, Gallagher (2011) and Roper et al. (2020) propose broad definitions; for example, Roper et al. suggest that restraint is any act “that restricts a person’s agency.”Reference Roper69 The literature rarely considers physical and mechanical restraint separately, unless ranking “restrictiveness.”Reference Tsu, Sugimoto, De Marco, Crutchfield and Birks70
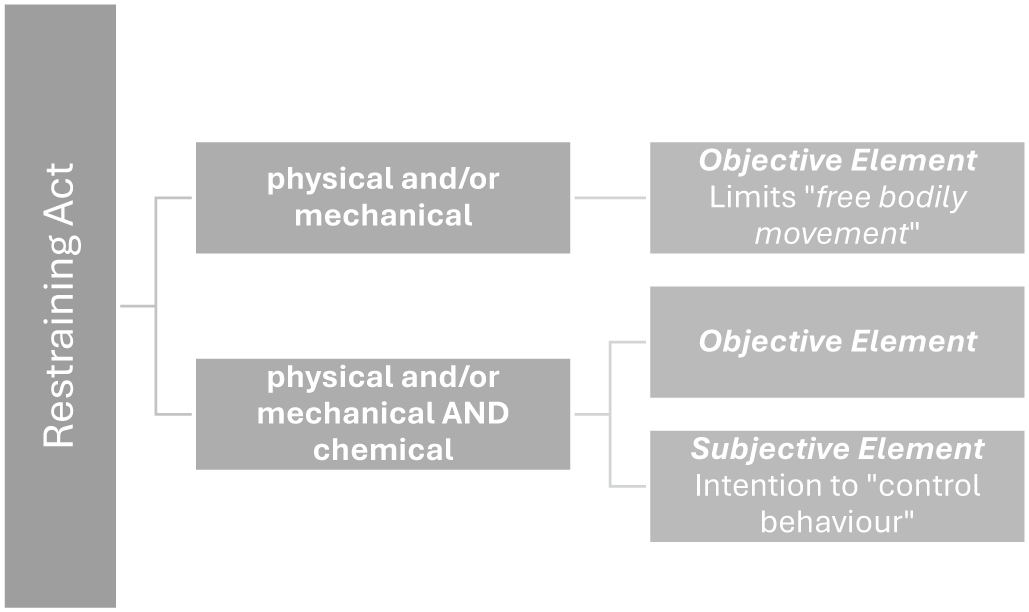
We interpret the literature as positing two essentially different definitions of restraint. One group of publications defines restraint by result and includes only physical and mechanical restraint. The second group of publications defines restraint by the practitioner’s intention and includes chemical methods alongside physical and mechanical methods. These differences are presented in Figure 2.
Definitions of Restraint.

Physical and Mechanical Restraint: Defining Restraint by the Result
Most of the literature considers only physical and mechanical restraint. Proposing a result-oriented definition of restraint, these papers are concerned with the effect of an act on the individual’s free movement of their limbs. The act, the application of the device and/or bodily-force, must “prevent … free bodily movement,”Reference Cheung and Yam71 “limit[ing] freedom.”Reference Hall and Smithard72 The potential use of medication/sedation to restrain is not considered. The reason for this silence is unclear, though it may reflect the assumption, alluded to in the older literature,Reference Moss and La Puma73 that sedation is an ethically permissible precursor to restraint. This understanding reflects the historical regulation of restraint in Australia that has not previously regulated the use of sedating medications as a precursor to, or instead of, physical and/or mechanical restraint.Reference Maker and McSherry74
Physical, Mechanical, AND Chemical Restraint: Defining Restraint by the Intention
By contrast, the more recent and smaller body of literature considering physical, mechanical, and chemical restraint adds a subjective element to the result-oriented definition.Reference Patten, Chaucer and Fitzgerald75 In these articles, applying a medium constitutes restraint where it
-
1. deprives the individual of a relevant “freedom,”Reference Patten and Chaucer76 specifically “bodily”Reference Cheung and Yam77 or “mental state”Reference Birks78; and
-
2. is applied “intentionally”Reference Crutchfield79 to “control behavior and restrict … freedom of movement.”Reference Patten and Chaucer80
It is the “intent, not mechanism [that] determines whether movement restriction is considered restraint.”Reference Quaine, Waisel and Van Norman81 The MHWA adopts this definition, and similarly distinguishes using medication to restrain from using it exclusivelyReference Fitzgerald, Patten, Chaucer, Quaine and Waisel82 or predominatelyReference Roper83 to “treat a medical condition.”Reference Patten and Chaucer84 Though alluded to by Bray (2015), the inherent difficulty in defining restraint by reference to the restrainer’s subjective intent is not clearly articulated or resolved.
Problems with These Definitions of Restraint
Our research identified two definitions of restraint in the literature: a result-oriented definition, and an intent-oriented definition. However, in our view, neither definition draws out all ethically relevant features of the act sufficiently to assist in assessing the ethical justifiability of the breadth of freedom-limiting acts (FLAs) that occur in hospital settings. For example, an FLA to prevent a patient in intensive care from self-extubating is different in an ethically important way from the same FLA to placate an aggressive patient experiencing a psychiatric emergency on a busy ward. In the first, the FLA is solely intended to benefit the patient; in the second, the intended benefit is shared between the patient, the staff, and other patients on the ward. Yet, the result-oriented definition cannot distinguish between them. Tied to the objective effect of the FLA, using the result-oriented definition, these acts are ethically equivalent.
The intent-oriented definition is also problematic for two reasons. First, it requires the impossible: the objective determination of subjective intent. A third party cannot unequivocally or reliably discern the intention of another. In practice, this definition relies on proxy measures of intent, for example the “off-label” use of medication. This is unsatisfactory, given that the distinction between treatment and restraint — particularly in patients presenting with mental health conditions — is often fine and potentially arbitrary. For example, the administration of an antipsychotic to a medically unstable patient with anorexia and comorbid anxiety before commencing nasogastric feeds may have multiple motives, including to facilitate necessary treatment (e.g., nutritional stabilization), and/or to treat the comorbidity. Whether this is an instance of restraint or treatment is unclear when applying the intent-oriented definition. The complexity exposed by this example is compounded where the patient, or their medical condition, is unknown to the prospective restrainer, and an FLA intended to control behavior may ultimately treat an unknown, underlying medical condition.
Second, even if it were possible to accurately identify the restrainer’s intent, this definition remains insufficient for the purpose of assessing ethical justifiability. Knowing the restrainer’s intent does not necessarily differentiate between the examples described above of the FLA in the intensive care unit and the one on the ward. In fact, it is likely that both FLAs were intended to control the patient’s behavior. Even if “intent” does differentiate between these examples, we consider this difference insufficient to warrant either regulating or understanding them differently. It does not capture all ethically relevant differences.
The Importance of Context: A Continuum of Restraint
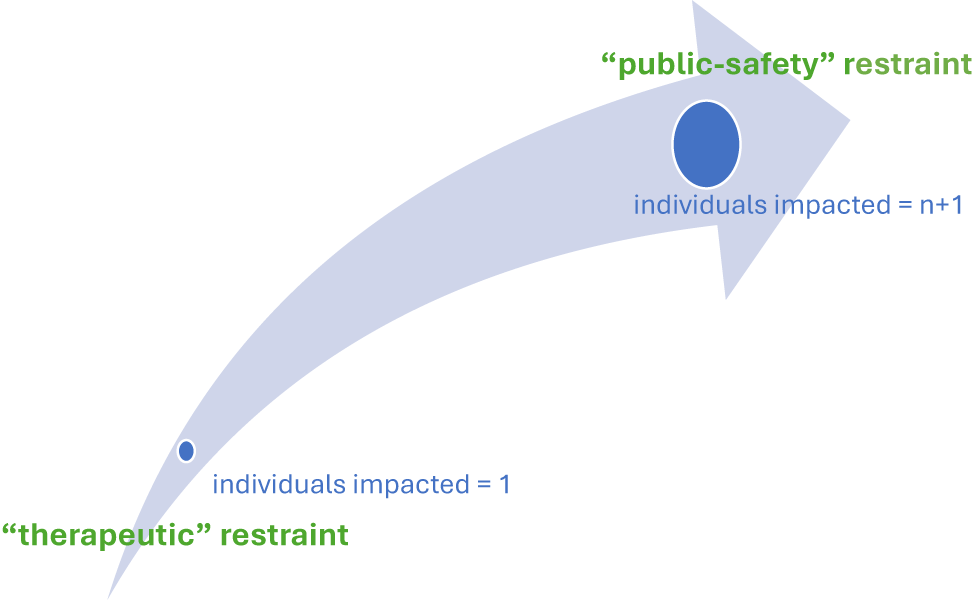
The outcome- and intent-oriented definitions both miss the ethical significance of the context in which the FLA occurs. Considered within its context, it becomes apparent that the key feature differentiating the examples above is the number of people impacted by the FLA. For example, while the consequences of an FLA (e.g., wrist restraints) to prevent a patient in intensive care from self-extubating are largely confined to the patient, the consequences of a similar act to control the behavior of an agitated patient experiencing a psychiatric emergency on a busy ward are potentially spread across many individuals, including proximate patients and staff. These examples demonstrate that FLAs can be understood as occurring along a continuum. At one end of the continuum are FLAs which only impact the patient. We refer to these as “therapeutic restraint.” At the other end are FLAs which impact many people’s interests. This describes the ward scenario, where a patient’s behavior, without intervention, endangers the safety of many. We refer to these instances as “public- safety restraint” (see Figure 3). There is no specific point of demarcation on the continuum between these two types of restraint. Instead, FLAs are understood to be more or less like an act of “therapeutic restraint” or “public-safety” restraint depending on the circumstance/context in which they occur.
Restraint as a Continuum.

When considering an FLA, the applicant’s intent and/or its outcome is less relevant to the question of its ethical justifiability than its impact on the (ethically relevant) interests of those affected by its application. Conceptualizing restraint as occurring along a continuum redirects attention to this (ethically) critical feature, thus facilitating the subsequent ethical analysis.
We argue that, from an ethical perspective, a critical feature of a restraining act is the number of individuals impacted, and thus the current definitions of restraint are inadequate because they fail to consider the ethical relevance of the number of individuals impacted by the act (i.e., its potential public impact). With this understanding, we propose that such acts are better understood as acts occurring along a continuum, from acts which impact the interests of a single individual (e.g., the patient restrained in ICU — “therapeutic restraint”) to those that impact the interests of many (e.g., the use of restraint in a busy ward — “public-safety” restraint). Conceptualizing the act in this way allows for a (gradual) change in the focus of the ethical analysis — that is, the weight different ethical principles are afforded when considering the ethicality of the act.
Part II: Frameworks in the Existing Literature — Principlism vs. Human Rights
Kotalik argues that “every discourse about health care has not only a scientific but also a moral dimension.”Reference Kotalik85 This latter dimension identifies whether, and if so when, the use of restraint is ethically justified in hospital settings. As analytical tools, ethical frameworks facilitate this inquiry, highlighting the ethically relevant values and principles for consideration and the appropriate way of approaching the issue.Reference Zachreson86 There are many frameworks used to assist in resolving ethical challenges — their particular principles, values, and priorities determined by the context of the issue.Reference Wilson87 For example, many of the principles and values of ethical frameworks used in clinical medicine are like those deployed in public health contexts. However, differences in social scale, goals, and the nature and number of interests between the settings require the ethical priorities to differ. While the interests of the individual are prominent in both public health and clinical ethics frameworks, they are afforded primacy in the latter. By contrast, in a public health context individuals’ interests are balanced against the health of the public.Reference Jamrozik, Dawson and Jennings88
The use of ethical frameworks to guide decision-making is a particular feature of clinical medicine. The dominant framework is Beauchamp and Childress’ four principles of biomedical ethics or principlism.Reference Beauchamp and Childress89 A principlist analysis involves considering an issue from the perspective of four principles derived in part from “the obligations and virtues of health professionals”Reference Beauchamp and Childress90 — beneficence, non-maleficence, autonomy, and justice (see Table 4). Having a prima facie nature, a principle can be “justifiably overridden”Reference Beauchamp and Childress91 by another. Where conflicting, the decision-maker must balance the respective weights of the competing interests.Reference Beauchamp, Childress and Beauchamp92 Theoretically, no principle is supreme, and thus the ultimate prioritization is an exercise of discretion.Reference Gillon and Gillon93
Definitions of the Four Principles of Biomedical Ethics

Adapted from Beauchamp and Childress (2001) and Beauchamp (2003).
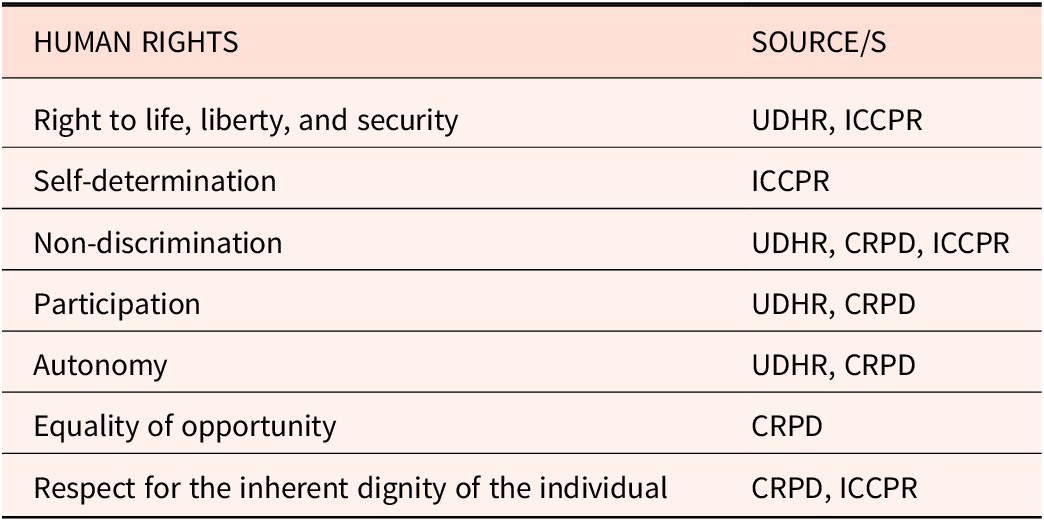
Emerging out of political liberalism, another ethical framework used in health contexts is human rights. Historically used in legal and political contexts,Reference Fuentes-Julio, Ibrahim and Gruskin94 the human rights framework (HRF) proceeds from the ethical principle that individuals have an inherent value, or “dignity.”Reference Langlois and Goodhart95 This value entitles all individuals to a collection of “universal, [and] inalienable”Reference Langlois96 rights and freedoms, many of which are now codified in international law (see Table 5).Reference Peel97 Rights-based approaches are increasingly a feature of health policy and legislation,Reference Gruskin98 and have been a core feature of mental health policy in Australia since the early 1990s.Reference McSherry99 Placing the “person” at the center of the analysis, the HRF considers the ethicality of an act or policy by reference to its interaction with these fundamental (absolute100) rights.Reference Langlois101 Where an act is demonstrated to limit or infringe a human right, it is unethical.Reference Méndez and Langlois102
Examples of Human Rights

UDHR — Universal Declaration of Human Rights; ICCPR — International Covenant of Civil and Political Rights; CRPD — Convention on the Rights of Persons with Disabilities
Justifying the Use of Restraint
Framing the Arguments
Several ethical frameworks are prominent in the literature. Of the publications considered, the majority (n=28) were written by health practitioners/academics and use Beauchamp and Childress’ (2001) four principles approach to frame their ethical analysis of restraint. By contrast, publications which use the HRF are predominately written by legal academics,Reference Roper and McSherry103 which is perhaps reflective of the increasing influence of human rights discourse in health policy. The remaining literature draws upon values from specific professional-ethics frameworksReference Carr, Gallagher and Zeng104 and high-level normative theories.Reference Hopton105 Three articles responding to Crutchfield and Redinger (2024) rely on the notion of basic (negative) libertyReference Tsu, Sugimoto, De Marco and Birks106 — “what is required to live the life of a free person.”Reference Crutchfield107 The choice of ethical framework is significant, determining the ethically relevant interests — and consequently, whether restraint can be ethically justified.
Human Rights: Protecting the Person
Three publicationsReference Roper, McSherry, Hardy and Armitage108 use an HRF, focusing on the experience of restraint by marginalized and/or vulnerable cohorts: children,Reference Hardy and Armitage109 the mentally ill,Reference Roper110 and the disabled.Reference McSherry111 Drawing upon the language and values of international rights instruments, particularly the United Nations Convention on the Rights of Persons with Disabilities (CRPD),Reference Roper112 the primary ethical concern of these publications is the basic, inviolable “human rights and freedoms”Reference Roper113 of “the person.”Reference Roper114 The importance of “personhood” is evidenced by the decision to exclusively use the term “person.” While papers applying other frameworks refer to the restrained individual by their situation (e.g., the principlist literature refers to the restrained individual as a “patient”) those applying the HRF only ever refer to the “person.” The person’s rights — including their right to “freedom of movement,”Reference Roper115 “to make [their] own decisions,”Reference McSherry116 and “respect for [their] inherent dignity”Reference McSherry117 — operate as “essential limit[s] for all human action … [and] must be protected in all circumstances.”Reference Cortinhal118
Concluding that restraint limits these rights, it necessarily follows that restraint violates human rights “whatever terminology is used,”Reference McSherry119 “irrespective of questions of ‘justification,’”Reference Roper120 and is unethical. From this conclusion, an elimination — as opposed to “reduction” — policy is preferred by Roper and colleagues (2020), who argue that “‘reducing’ is not enough”Reference Roper121 given restraint “may be crushing to a person’s sense of self, their dignity and self-respect.”Reference Roper122 The other publications are more equivocal, suggesting longer-term solutions culminating in elimination. This correlation replicates the findings of Chieze et al. (2021). Their research similarly identified the “elimination position” as a minority opinion, justified because restraint is perceived as “violat[ing] fundamental rights.”Reference Chieze123
Principlism: (Peeking) Beyond the Patient
Applying (expressly or implicitly) the principles of biomedical ethics, the majority of the literature concludes, somewhat pragmatically,Reference Mohr, Chieze, Cheung, Yam, Quaine, Waisel, Crutchfield and Herrera124 that using restraint in “exceptional”Reference Carr125 circumstances can be ethically justified — restraint being at times “unavoidable” or “necessary” to ensure therapeutic values are met.Reference Hall and Smithard126 This results in a preference for the “reduction,” not elimination, of restraint. This preference is enabled by the prima facie nature of the principles.Reference Gillon127 In contrast to the absolute rights of the HRF, the principlist frame allows authors, when faced with conflicting principles, to “strike a balance.”Reference Sokol128
However, the principles are not equally weighted. Regardless of place of publication,Reference Cortinhal, Cheung, Yam, Zeng and Ye129 primacy or “sanctity”Reference Cheung and Yam130 is granted to the principle of autonomy — “the ability … to make decisions free from … controlling interference by others.”Reference Cheung and Yam131 The other principles, particularly justice, “giving others their due,… fairness, and equit[y],”Reference Mohr132 receive markedly less attention. The primacy of autonomy correlates with the general movement in clinical practice away from medical paternalism (i.e. “doctor knows best”), itself reflective of the broader sociocultural recognition of the value of self-determination.Reference Murgic133 This approach firmly places the individual’s personal preferences at the core of the ethical analysis.
In evaluating the ethics of restraint, two conflicts emerge. The first, a conflict between patient autonomy and “best interests”Reference Nirmalan, Chieze, Feder, Behrman and Dunn134 (beneficence/non-maleficence), appears most frequently in publications considering restraint in intensive care settings. This conflict is resolved by considering the “relative weights”Reference Feder, Sokol, Gibb and Slomka135 of the harm to be minimized, the patient’s risk to themselves, and the “burdens, risks and harms of the violation.”Reference Gibb136 The second, identified in psychiatric and emergency settings, is a conflict between the interests of “an individual patient versus [those] of others (staff and other patients)”Reference Fitzgerald137 — a “dialectic between individual autonomy and collective safety.”Reference Geen138
Unlike the HRF, which holds that “restraint must be considered from the perspective of people who have experienced [it]”Reference Roper139 and does not considerReference McSherry, Hardy and Armitage140 the interests of others, principlism provides moral scope for considering “third-party” interests.Reference Beauchamp, Childress and Gillon141 However, this scope is limited by principlism’s allegiance to the “fiduciary duty to care and advocate for … individual patients.”Reference Geen142
Justified (Barely)
In both conflicts, ethical restraint requires an “imminent”Reference Cheung, Yam, Petrini, Preisz, Preisz, Schneider and Thompson143 or “immediate”Reference Moss, La Puma, Nirmalan, Ye, Preisz, Preisz, Elcock, Lewis, Völlm and Nedopil144 risk of harm to the patient or “others.” The identity of the “others” lacks consensus. Most authors agree that the safety of other patients and the “therapeutic milieu”Reference Sclafani145 are relevant.Reference Nirmalan and Thompson146 Less common is the recognition of a broader “public welfare” interest.Reference Cortinhal, Cheung, Yam and Geen147 Staff safety is generally considered ethically relevant,Reference Mohr, Bray, Fitzgerald, Cheung, Yam, Geen, Crutchfield, Ye, Thompson, Elcock and Lewis148 though some suggest this is an accepted risk.Reference Slomka149 There is similar ambiguity regarding using restraint to mitigate against the impact of staffing shortages.Reference Cortinhal, Bray, Zeng and Crutchfield150 Ultimately, however, the authors agree that it is “the patient’s best interests [which] should be of prime concern”Reference Nirmalan151 (emphasis added).
Though uncomfortable in doing so, much of the principlist literature conceives of (very) limited circumstances where restraint is ethically justified. Some also suggest criteria for its use, intended either to “safeguard[]”Reference Sclafani152 the patient,Reference Cortinhal, Crutchfield and Schneider153 or guide or support staff in managing its administration.Reference Cheung, Yam, Thompson, Elcock and Lewis154 The criteria proposed can be broadly categorized as requiring respect for the patient, proportionate application, and safe systems (see Table 6).
Criteria for Ethical Restraint

Problems with the Ethical Frameworks in the Literature
Once the ethical importance of the context in which the FLA occurs, and the (ethical) significance of its potential magnitude, are highlighted, the deficiencies for the task at hand of the preferred “person”- and “patient”-centric frameworks prominent in the literature are exposed.
Human Rights: … but Not All Humans
Neither the HRF nor principlism provide sufficient scope to evaluate the legitimacy of FLAs in the variety of contexts in which they are used in hospital settings. Comprised of inviolable rights and freedoms,Reference McSherry155 as applied in the literature,156 the HRF sites “the person” — their “rights” — at the center of the analysis.Reference Roper157 This approach excludes consideration of others’ ethically relevant interests — the inviolable rights of other individuals impacted by the conduct prompting the FLA and/or its application. Evaluated exclusively from the person’s perspective, the objective finding that an FLA limits or infringes an otherwise inviolable right to, for example, “bodily integrity”Reference Roper158 necessitates the conclusion that the FLA is unethical. This is regardless of its potential to enhance others’ interests. As applied, the HRF does not provide any guidance or scope to balance the infringement of the individual’s inviolable rights against its potential to enhance and/or preserve the otherwise inviolable rights of proximate patients or staff.
Principlism: The Pull of the Patient
Compared to the HRF, principlism is better-suited to analyzing the ethical justification of restraint in hospital settings for two reasons. First, because the principles — beneficence, non-maleficence, and particularly justiceReference Mohr, Hall, Smithard and Gillon159 — explicitly recognize the potential ethical importance of the interests of individuals beyond the patient. Second, because the principles, considered prima facie — “binding until meeting conflict with another”Reference Hall and Smithard160 — can, when conflicting, be prioritized one over the other.Reference Beauchamp and Childress161 At least theoretically, “no preeminent principle exists in biomedical ethics,”Reference Beauchamp and Childress162 and the conflict is determined wholly by the circumstances in which it occurs.Reference Gillon163
However, with its biomedical origins,Reference Lee, Petrini and Gainotti164 principlism has an implicit fidelity to the “special”Reference Beauchamp and Childress165 fiduciary relationship between the doctor and patient.Reference Beauchamp, Childress, Lee and Childress166 In practice, particularly when applied in a Western medical setting,Reference Gillon167 this translates to an emphasis on the interests of the patient — (specific) beneficence, non-maleficence, and increasinglyReference Gillon168 their autonomy.Reference Smith, Oderberg, Laing and Callahan169 The principles of justice, and general beneficence and non-maleficence to the extent they incorporate the interests of others,Reference Beauchamp and Childress170 sit at the periphery, identified but rarely explored.Reference Dawson and Jennings171 The centrality of the doctor-patient dyad, and this preference, is reflected in our results. Few articles interrogate in detail the ethical justifiability of an FLA by reference to its impact on justice.Reference Mohr, Hall, Smithard and Geen172 The principlist literature otherwise universally begins its ethical consideration from the patient’s perspective. When considered, the interests of others are an adjunct — noted, but not explored.
It is unsurprising that principlism, given its origins, is well-suited to assessing the ethical justifiability of therapeutic restraint, a classic clinical ethics question. In this context, as intended,Reference Gillon173 a principlist analysis “aid[s] deliberation by making [all] relevant values explicit.”Reference Dawson, Peckham and Hann174 However, its application is challenged by public safety restraint.Reference Lee, Childress and Kass175 When starting the analysis from the patient’s perspective, it is unclear why and how to “take others into account”Reference Dawson and Jennings176 — principlism does not provide the necessary tools or safeguards to manage the fundamentally different roles of the actors, the type of power exerted, and its impact where there is a public component. This is particularly so when an FLA is of questionable benefit to the patient. The implicit understanding of the pre-eminence of the patient’s interests makes the decision to preference the interests of others uncomfortable and potentially untenable. This is particularly because principlism does not otherwise provide a means of “checking” this use of power. This discomfort is evident in the literature. The circumstances required to permit the restraint of an individual for the benefit of others must be most grave,Reference Schneider177 and even then, there must be some benefit derived by the patient from the act (e.g., an ultimate restoration of autonomy).Reference Fitzgerald178
Part III: The Potential of Public Health Ethics
Conceptualizing restraint as occurring along a continuum exposes the difficulties in “reconciling ethical principles across different social scales”Reference Zachreson179 — doctor-patient versus hospital.Reference Zachreson, Lee and Kass180 While applying the principlist framework aids ethical deliberation about therapeutic restraint events, its utility diminishes as we move along the continuum, the “public” component grows, and (potentially) any therapeutic benefit derived by the patient diminishes. What then are the appropriate values and principles to consider?
Public-safety restraint shares many conceptual similarities with public health interventions (PHIs) such as isolation in the setting of infectious disease. Though occurring on different scales, at the most rudimentary level, both public-safety restraint and PHIs like isolation involve the exercise of institutional power to compel behavior-change primarily for the benefit of others. Isolation involves the state or a health authority compelling the behavior of individuals known to pose a public health risk with the expected benefit of preserving or promoting public health.Reference Giubilini and Upshur181 Its implementation is recognized to have consequences for core values — including autonomy, equality, and justiceReference Upshur182 — and causes many of the same ethical tensions observed when considering public-safety restraint.
Because of these ethical tensions, PHIs, like isolation, are increasingly the subject of ethical interrogation to ensure that an appropriate balance between “individual freedom and community-wellbeing”Reference Lee183 is achieved. Although there is no settled framework or approach,Reference Lee, Childress, Kass, Parasidis and Fairchild184 several principles feature prominently in the PHE literature (see Table 7). Sharing many similar principles and values with clinical ethics frameworks, a PHE approach distinguishes itself by incorporating and emphasizing communitarian values.Reference Dawson, Jennings, Kass, Parasidis and Fairchild185 Combined, PHE principles are sensitive to the larger social scale of public health and PHIs, and the need to balance individual freedom and community well-being.Reference Lee186 Specifically, in emphasizing principles of good governance, transparency, and accountability, PHE approaches draw out the relevance of using compulsive public power for the benefit of third-parties to the ethical analysis. These principles operate as safeguards and accommodate the need to balance the interests of individuals with the common good.
Principles of Public Health Ethics

The potential “public” implications of public-safety restraint applied in a hospital setting warrants a more balanced consideration of, on the one-hand, the individual’s interests, and on the other, the others’ interests, than afforded by principlism. However, this necessary dilution of the emphasis on individual autonomy, and the consequent potential to curtail an individual’s interests for the benefit of others, requires mechanisms to ensure this power is exercised appropriately. PHE principles provide these mechanisms, combining the individual or patient-focused principles of principlism (including autonomy) with community or public-oriented principles (i.e., democratic governance). However, if the ethicality of therapeutic restraint is aptly assessed using a principlist framework, the question becomes: at what point along the continuum ought we transition from a principlist to PHE analysis?
We suggest there is no specific “tipping point,” and that PHE principles are applicable at all points along the continuum, albeit with different weighting. Ethical frameworks are not algorithms to be applied didactically to deduce a correct result. Instead, they are tools. Frameworks are intended to direct the decision-maker’s attention to relevant values, and encourage deliberation and specification based on the particular circumstances.Reference Dawson187 The advantage of applying a PHE framework in this context lies in its inclusion of principles that direct attention to the interests of the individual (i.e., those principles that are common to both PHE and principlism), and principles that direct attention to the interests of the community. On this basis, we argue that an application of PHE principles is appropriate regardless of where an FLA falls on the continuum — all that changes is the relative weight afforded to the different principles. For example, when applied to an FLA at the therapeutic-restraint end of the continuum, the principles which accommodate the “public component” of public-safety restraint (i.e., that the FLA is publicly justified) are less relevant, and thus carry less weight in the ethical deliberation. As we move along the continuum towards the public-safety restraint end, the relevance of — and weight afforded to — those uniquely PHE principles increases. The PHE framework is able to recognize and account for the “public” aspect of some FLAs in hospital settings, while at the same time ensuring that the interests of the individual patient involved are also taken into account.
Conclusion
At a hospital level, the key practical question is how to ensure that any and all use of restraint is ethical. Public health ethics principles may provide the necessary tools for this task. Applying a public health ethics lens to the issue both shifts the focus and widens the frame of ethical consideration. Rather than zooming in on the patient and the FLA, a PHE approach, with its emphasis on principles of “good governance,”Reference Thompson188 suggests that the ethical justifiability of the act is partly determined by the broader systems within which it occurs. The precise form that these systems should take is beyond the scope of this paper. We would, however, recommend that further research be carried out in concert with a broad range of involved stakeholders — including hospital staff, patients, and caregiverrs — directed at developing administrative systems and hospital policies and procedures that operate at an institutional level to minimize the use of restraint and otherwise safeguard the interests of all involved. Cultural attitudes towards the use of coercive public power and the role of medicine are likely significant in shaping attitudes towards the use of restraint in hospitals, and the relative weight afforded the ethical principles concerned. Future research that incorporates a broader range of cultural perspectives would provide a more holistic overview of the ethically relevant issues, and is warranted given the level of international concern.Reference Méndez189
Our research is a unique contribution to the field, providing a novel perspective on how to understand and define restraint that highlights the relevance of “social scale” when considering whether, and when, its use in hospital settings can be ethically justified. We have identified that the current definitions do not incorporate all ethically relevant features of restraint in hospital settings. Specifically, the definitions do not capture the potential “public component” of restraint — the ability of its use to impact the ethically relevant interests of multiple individuals. This feature of restraint explains why the current preferred person- and patient-centric ethical frameworks — human rights and principlism — are problematic. Instead, this understanding supports the application of the principles of PHE to ground the future development of policies, practices, and procedures for the ethical application of restraint in hospital settings.
Disclosures
The authors have nothing to disclose.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/jme.2026.10255.








 Open access
Open access