


Introduction
Worldwide, an estimated 1.5 billion deaf and hard-of-hearing (DHH) people live with hearing loss, which ranks among the leading contributors to years lived with disability (GBD 2019 Hearing Loss Collaborators, 2021; GBD 2021 Diseases and Injuries Collaborators, 2024). In this review, we use ‘deaf and hard of hearing (DHH)’ as an inclusive umbrella term referring to people with hearing loss. Capitalised ‘Deaf’ denotes the cultural–linguistic community, whereas lowercase ‘deaf’’ is widely used when referring broadly to all deaf people, particularly when cultural affiliation is unknown (National Association of the Deaf, n.d.). The World Health Organization (WHO) classifies DHH as ranging from mild (20–35 decibels [dB] in the better ear) to profound or total hearing loss (>95 dB in the better ear) (Humes, Reference Humes2019; World Health Organization, 2021). Of the total DHH population, approximately 1.16 billion (or 77%) have mild hearing loss, while 430 million (or 23%) experience moderate (35–50 dB) or higher levels of hearing loss (World Health Organization, 2021). Across the lifespan, the global prevalence of moderate or higher levels of hearing loss is around 2% for those with early onset (in childhood or adolescence), increases gradually to 2.8% in those aged 40–44 years, and rises more sharply to 8.4% in people aged 55–59 years. Notably, around one-third of DHH people with moderate or higher levels of hearing loss are adults between 18 and 60 years old (GBD 2019 Hearing Loss Collaborators, 2021; Guo et al., Reference Guo, Ji, Song, Zhao, Yan, Zou, Bai, Wu, Guo and Song2024).
These DHH adults may face challenges in daily functioning, such as discrimination, accessing information, and stigmatisation, which can increase their vulnerability to mental health problems (de Graaf and Bijl, Reference de Graaf and Bijl2002; Fellinger et al., Reference Fellinger, Holzinger and Pollard2012; Mousley and Chaudoir, Reference Mousley and Chaudoir2018). Barriers to effective communication, both early in life and in adulthood, can also contribute to long-term psychosocial and health vulnerabilities among DHH adults, including Deaf signing populations (Kushalnagar et al., Reference Kushalnagar, Moreland, Simons and Holcomb2018, Reference Kushalnagar, Ryan, Paludneviciene, Spellun and Gulati2020; Rogers et al., Reference Rogers, Rowlandson, Harkness, Shields and Young2024). Furthermore, navigating a predominantly hearing world may lead to acculturative stress as DHH adults have to adapt to differing cultural environments (Aldalur et al., Reference Aldalur, Pick and Schooler2021; Aldalur and Pick, Reference Aldalur and Pick2023). Additionally, accessing mental health care remains a significant challenge due to service inaccessibility, lack of cultural sensitivity and limited health literacy (McKee et al., Reference McKee, Paasche-Orlow, Winters, Fiscella, Zazove, Sen and Pearson2015; Smith and Samar, Reference Smith and Samar2016; Morisod et al., Reference Morisod, Malebranche, Marti, Spycher, Grazioli and Bodenmann2022).
Given these challenges, several systematic reviews and meta-analyses have examined whether the prevalence, incidence or severity of mental disorders is higher among DHH people than among hearing people. Throughout this review, when referring to two or more of these collectively, we use the umbrella term ‘mental disorder outcomes’. Most of these reviews focused on a single mental disorder and reported higher mental disorder outcomes for depression, anxiety disorders, psychotic disorders and overall psychopathology among DHH children, adolescents and older adults (Theunissen et al., Reference Theunissen, Rieffe, Netten, Briaire, Soede, Schoones and Frijns2014; Linszen et al., Reference Linszen, Brouwer, Heringa and Sommer2016; Shoham et al., Reference Shoham, Lewis, Favarato and Cooper2019; Jiang et al., Reference Jiang, Kubwimana, Eaton, Kuper and Bright2020; Lawrence et al., Reference Lawrence, Jayakody, Bennett, Eikelboom, Gasson and Friedland2020; Trott et al., Reference Trott, Smith, Xiao, Veronese, Koyanagi, Jacob, Lopez-Sanchez, Barnett and Pardhan2021). While two of these reviews included studies covering the entire lifespan, the majority of the included studies focused on samples of older adults (60 +) or children, yielding limited and only indirect evidence for adults aged 18–60 years (Linszen et al., Reference Linszen, Brouwer, Heringa and Sommer2016; Shoham et al., Reference Shoham, Lewis, Favarato and Cooper2019). This highlights a significant gap in the literature regarding the mental health of DHH adults compared to hearing adults. This gap is particularly concerning because employment declines rapidly from age 60, and many adults leave the workforce well before the pension eligibility age (OECD, 2025). Therefore, adults aged 18–60 years represent the majority of the working-age population, for whom mental disorders not only affect individual well-being, functioning and mortality, but also result in significant economic and societal costs, including but not limited to reduced labor market participation and productivity losses (Walker et al., Reference Walker, McGee and Druss2015; Christensen et al., Reference Christensen, Lim, Saha, Plana-Ripoll, Cannon, Presley, Weye, Momen, Whiteford, Iburg and McGrath2020; Arias et al., Reference Arias, Saxena and Verguet2022).
Therefore, in the present systematic review, our objective was to compare the prevalence, incidence and severity of mental disorders between DHH and hearing adults aged 18–60 years. We aimed to be the first systematic review to examine the full spectrum of mental disorders as defined by any mental, developmental or behavioural disorder included in the DSM-5-TR or ICD-11 (World Health Organization, 2019; American Psychiatric Association, 2022). By synthesising the overall findings, alongside a disorder-specific breakdown, we aimed to offer a broad evidence base on potential disparities, helping to guide future research, inform policy, support service adaptation, and enable the development of targeted interventions and preventive strategies for DHH adults.
Methods
The current systematic review was reported according to the PRISMA guidelines, with the checklist provided in Supplement A (Page et al., Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann, Mulrow, Shamseer, Tetzlaff, Akl, Brennan, Chou, Glanville, Grimshaw, Hróbjartsson, Lalu, Li, Loder, Mayo-Wilson, McDonald, McGuinness, Stewart, Thomas, Tricco, Welch, Whiting and Moher2021). The protocol was registered in PROSPERO (CRD42023474624), with four amendments presented in Supplement B.
Identification and selection of studies
We conducted systematic searches in Ovid Medline, Embase.com, APA PsycInfo (Ebsco) and Web of Science (Core Collection) from inception to 13 December 2025, in collaboration with a medical information specialist (R.d.V.). Search terms (including synonyms and related words) were used as index terms or free-text words: ‘Deaf’, ‘Hard of hearing’, ‘Hearing Disorders’, ‘Persons with Hearing Impairments’, ‘Mental Disorders’, ‘Mental Health’, ‘Prevalence’, ‘Incidence’, ‘Severity’. Publications in all languages were included. Duplicates were removed using Endnote X20.0.1 (Clarivate™), following the Amsterdam Efficient Deduplication (AED) and Bramer methods (Bramer et al., Reference Bramer, Giustini, de Jonge, Holland and Bekhuis2016; Otten et al., Reference Otten, de Vries and Schoonmade2019). The full search strategies are presented in Supplement C. All records were first screened based on title and abstract independently by two researchers (N.d.P. and K.D.) using Rayyan (Ouzzani et al., Reference Ouzzani, Hammady, Fedorowicz and Elmagarmid2016). Records identified as potentially eligible by either researcher were retrieved for full-text review. Full-text studies were then assessed for inclusion by the same researchers. Disagreements were resolved through discussion, involving a third researcher (C.v.K., I.C., or E.H.) if needed. No language restrictions were applied during the search. During full-text screening, five potentially eligible studies could not be assessed because they were written in a language not understood by the research team. All five were Chinese-language publications.
Eligibility criteria
We included studies that (a) used a case-control, cohort, or cross-sectional design; (b) examined adult samples with a mean or median age of 18–60 years, at least half the participants within this range, or explicitly described the sample as adults; (c) compared DHH adults with bilateral hearing loss (20–95 dB + in the better ear) with a hearing group. In practice, many primary studies did not report the exact degree of hearing loss, so being DHH could be identified through any method used in the original study; (d) reported differences in the prevalence, incidence, or severity of any mental, behavioural or developmental disorder corresponding to DSM-5-TR or ICD-11 categories, or examined suicidal outcomes such as ideation or attempts (World Health Organization, 2019; American Psychiatric Association, 2022). Clinical diagnosis was not required, and studies were eligible regardless of the type of mental health measure used; no minimum severity threshold was applied. No restrictions on publication date were applied.
Studies were excluded if (a) the DHH group did not meet the age criteria; (b) statistical significance was not reported or effect sizes could not be calculated from the provided data; (c) the comparison group consisted exclusively of people with disabilities (e.g., comparing DHH people only to people with a visual impairment); (d) focused exclusively on neurocognitive disorders; or (e) duplicate use of the same sample for the same outcome to avoid including the same participants across multiple studies reporting on the same outcomes (e.g., the Netherlands Longitudinal Study on Hearing) (Nachtegaal et al., Reference Nachtegaal, Smit, Smits, Bezemer, van Beek, Festen and Kramer2009; Stam et al., Reference Stam, Smit, Twisk, Lemke, Smits, Festen and Kramer2016; Bosdriesz et al., Reference Bosdriesz, Stam, Smits and Kramer2018). In such cases, we retained one study per sample and outcome, prioritising longitudinal over cross-sectional designs, clearer age range reporting, larger sample sizes or most outcomes.
Risk of bias assessment
The potential RoB of the included studies was assessed using a modified version of the CLARITY tool (CLARITY Group at McMaster University, n.d.; van der Ven et al., Reference van der Ven, Olino, Diehl, Nuñez, Thayer, Bridgwater, Ereshefsky, Musket, Lincoln, Rogers, Klaunig, Soohoo, DeVylder, Grattan, Schiffman, Ellman, Niendam and Anglin2024). This tool is structured across seven domains: (a) sample representativeness of the general population; (b) selection of exposed and non-exposed cohorts; (c) assessment of the exposure; (d) assessment of the outcome; (e) consideration of confounding factors; (f) assessment of confounding factors; and (7) handling missing data. Each domain was rated as either low risk, high risk, or unclear based on the tool’s explanation document (Supplement D). Two raters (N.d.P. and K.D.) independently conducted the assessments, resolving disagreements through discussion.
Data extraction
Two researchers (N.d.P. and K.D.) independently extracted data, with disagreements resolved through discussion or, if needed, involving a third researcher (C.K., I.C., or E.H.). Extracted data included study characteristics, participant characteristics and empirical findings. Study characteristics included study design (i.e., cross-sectional, case-control, or cohort), publication year, country and continent, recruitment strategy (e.g., schools/universities, register data), sample size per group, examined disorder (e.g., depression, anxiety) and disorder assessment measure (e.g., validated self-report questionnaire, diagnostic interview). Participant characteristics included group descriptions, sample age (range, mean, standard deviation), gender/sex distribution and tinnitus status. For the DHH group, we also extracted the type of audiometric test, preferred language, hearing device usage, pre- or post-lingual onset (as defined in the primary study) and education setting (e.g. mainstream or special education).
Empirical findings included outcome type (i.e., prevalence, symptom severity or incidence), effect direction (e.g., higher prevalence for DHH, no difference), statistical test used (e.g., t-test, logistic regression) and reported effect size, or if not reported, data to calculate odds ratios. Prevalence was defined as group differences in the proportion of individuals meeting diagnostic criteria or thresholds; severity as differences in symptom severity questionnaire scores or regression analyses with continuous variables; and incidence as new cases of mental disorders.
Data synthesis
Odds ratios were calculated for studies without reported effect sizes, using the number of cases in the DHH (exposed) and hearing (control) groups with positive (presence of disorder) and negative (absence of disorder) outcomes (Altman, Reference Altman1990; MedCalc Software Ltd., n.d.).
We synthesised the results using two complementary approaches, each aggregating findings at the study level so that every study contributed one overall direction of effect. Firstly, the summary-direction approach categorised studies as reporting higher, lower, no difference or mixed mental disorder outcomes for DHH compared to hearing groups, based on statistical significance of the effect direction. Studies were classified as mixed if they reported multiple outcome types, more than one disorder, or subgroup-specific results (e.g., by age or hearing loss degree) with varying directions. Secondly, to address the ambiguity introduced by mixed findings, the majority-direction approach classified studies by the most frequently reported effect direction. When outcomes were evenly split, studies were conservatively reclassified as no difference.
We applied both approaches across all studies (overall effects). Additionally, we conducted separate sensitivity and subgroup syntheses based on study RoB, with lower risk defined as 4–7 low-risk domains (50–100%) and higher risk as 0–3 low-risk domains (0–50%), age groups (younger adults: mean age <40 years or more than 50% of the sample under 40 years; older adults: mean age ≥40 years or more than 50% of the sample over 40 years), and outcome type (prevalence, incidence, and severity). This age distinction was based on global data indicating that hearing loss prevalence increases more sharply after age 40, suggesting that older samples likely include more later-onset hearing loss (GBD 2019 Hearing Loss Collaborators, 2021; Guo et al., Reference Guo, Ji, Song, Zhao, Yan, Zou, Bai, Wu, Guo and Song2024). Lastly, we conducted separate syntheses for each mental disorder, again aggregating results at the study level using both synthesis approaches.
Results
Selection and inclusion of studies
After removing duplicates, we screened a total of 14 089 records, excluding 13 384 based on titles and abstracts. Full texts were retrieved for the remaining 705 records, of which 645 were excluded. The PRISMA flowchart (Fig. 1) details the inclusion process and reasons for full-text exclusions. In total, 60 studies were included for narrative synthesis (full references in Supplement E).
PRISMA flowchart of study identification and selection.

Study characteristics
Selected characteristics of the 60 included studies are presented in Table 1, and full study-level details for each study are provided in Supplement F. In total, the studies included 8 578 466 participants (median = 3321), of whom 351 707 were DHH adults (median = 269) and 8 226 759 were hearing adults (median = 2489.5). Four studies did not report group-specific numbers. Most studies were cross-sectional (45; 75.0%) and half were published from 2020 onward (30; 50.0%; range: 1989–2025). Geographically, studies were mostly conducted in North America (28; 46.7%) and Europe (19; 31.7%). Terminology used to describe DHH groups varied: 14 studies (23.3%) used terms such as ‘deaf’ or ‘hard of hearing’, while 46 (76.7%) used ‘hearing loss’ or ‘hearing impairment’. Type of audiometric test also varied, with self-report used in 28 studies (46.7%) and audiological assessments such as pure tone audiometry (PTA) in 19 (31.7%). Most studies examined prevalence (40; 66.7%), fewer focused on severity (15; 25.0%) or both (3; 5.0%), and only two (3.3%) focused on incidence. Mental disorder outcomes were typically assessed using validated questionnaires (32; 53.3%). Some characteristics were infrequently reported, limiting further classification: tinnitus status (9; 15.0%), language use (11; 18.3%), hearing device usage (13; 21.7%) and pre- or post-lingual onset (8; 13.3%).
Selected study characteristics

a This included samples from three studies in Russia and Türkiye, and one study conducted in five countries spanning three continents (Africa, Asia and North America).
b Within the same study.
Risk of bias
The complete RoB assessment for all seven domains is presented in Supplement G. For studies with outcome-specific variation in RoB, the highest risk rating was retained within domains and for the overall assessment. In Domain 1, over half of the studies (31; 51.7%) had high RoB due to voluntary participation, while 28 (46.7%) had low RoB based on representative sources such as national registries. Most studies showed low RoB in Domain 2 (52; 86.7%), as exposed and unexposed groups were generally comparable in source and time frame. In Domain 3, 30 studies (50.0%) had low RoB based on objective or validated hearing loss assessments, while the remaining 30 (50.0%) had high RoB due to self-report measures or insufficient reporting. Most studies (45; 75.0%) had low RoB in Domain 4, using validated questionnaires or registry diagnoses. More than half (35; 58.3%) had low RoB in Domain 5 due to statistical adjustment for confounders. In Domain 6, 40 studies (66.7%) assessed confounding factors with confidence. Over half (36; 60.0%) had unclear RoB in Domain 7, as missing data or response rates were unreported, while 11 studies (18.3%) had low RoB. Overall, 3 studies (5.0%) had low RoB in 0–25% of domains, 15 (25.0%) in 25–50%, 35 (58.3%) in 50–75% and 7 (11.7%) in 75–100%.
Differences in mental disorder outcomes between DHH and hearing adults
Main synthesis
Table 2 presents the results of the summary-direction and majority-direction synthesis approaches, including the overall synthesis and sensitivity syntheses. In the overall effects synthesis using the summary-direction approach, over half of the 60 included studies (35; 58.3%) reported a higher prevalence, incidence, or severity of mental disorders for DHH compared to TH, while the remaining studies found either no difference (13; 21.7%) or mixed findings (12; 20.0%). Similar patterns were found for the majority-direction approach, with increases in both higher for DHH to 65.0% (39), as well as in no differences to 35.0% (21) for the remainder of studies. Therefore, mixed findings consisted of higher for DHH and no difference findings. Notably, not a single study in either synthesis approach reported lower aggregated mental disorder outcomes for DHH groups.
Differences in mental disorder outcomes between DHH and hearing adults

Note: Results are aggregated at the study level; N = Number of studies; RoB = Risk of Bias; Lower age = mean age lower than 40 years or more than 50% of sample under 40; Higher age = mean age higher than 40 years or more than 50% of sample over 40). Studies with equal findings were regarded as no difference per outcome in the majority-direction synthesis: overall effects (N = 2), only prevalence (N = 1), Only incidence (N = 1), Lower RoB (N = 2), Younger adults (N = 1) Older adults (N = 1); Three studies did not report data for age group classification, all reported mixed results (majority-direction: all three no difference).
In the sensitivity analysis by RoB, studies with higher RoB more frequently reported higher mental disorder outcomes for DHH (summary: 66.7%—majority: 72.2%) than lower RoB studies (54.8%—61.9%). Mixed findings were more frequent among lower RoB studies (23.8%) than higher RoB studies (11.1%), reflecting higher and no difference mental disorder outcomes with two ties regarded as no difference. In the subgroup analysis by age, over half of studies in both younger (mean age < 40) and older (mean age ≥ 40) adult samples showed higher mental disorder outcomes for DHH, with majority-direction results of 71.4% (younger adults) and 66.7% (older adults), while the remaining studies showed no difference. Lastly, in the sensitivity syntheses by outcome type, we observed similar patterns for prevalence and severity as the overall synthesis. Most studies reported higher prevalence (62.8%—72.1%) and severity (61.1%) of mental disorders for DHH in both syntheses approaches. For prevalence, 25.6% of studies showed mixed findings; these reflected combinations of higher prevalence for DHH and no difference. For severity, findings were identical across approaches due to the absence of mixed results. Incidence was reported in only two studies, one showing no difference and one mixed (treated as no difference in majority-direction synthesis). Consistent with the overall effects, across all sensitivity and subgroup syntheses, no study reported lower aggregated mental disorder outcomes for DHH groups compared to hearing groups.
Disorder-specific synthesis
Table 3 presents the disorder-specific results of both synthesis approaches. Six mental disorders were examined in at least five studies: depression (33 studies), anxiety (15 studies), psychotic disorders (11 studies), suicidal outcomes (8 studies), general mental disorders (7 studies), and post-traumatic stress disorder (PTSD; 5 studies). In the majority-direction synthesis, all mixed findings from the summary-direction approach were reclassified as either higher for DHH or no difference (including ties). Across disorders, PTSD (80.0%), suicidal outcomes (75.0%), and psychotic disorders (72.2%—81.8%) showed the greatest tendency towards higher mental disorder outcomes for DHH. Moreover, for anxiety (53.3%) and general mental disorders (57.1%), more than half of the studies indicated higher mental disorder outcomes for DHH. Lastly, for depression, just under half of the studies (48.5%) reported higher mental disorder outcomes for DHH, while the remaining studies indicated no difference. Across all six disorders, none showed lower aggregated mental disorder outcomes for DHH groups.
Disorder-specific synthesis
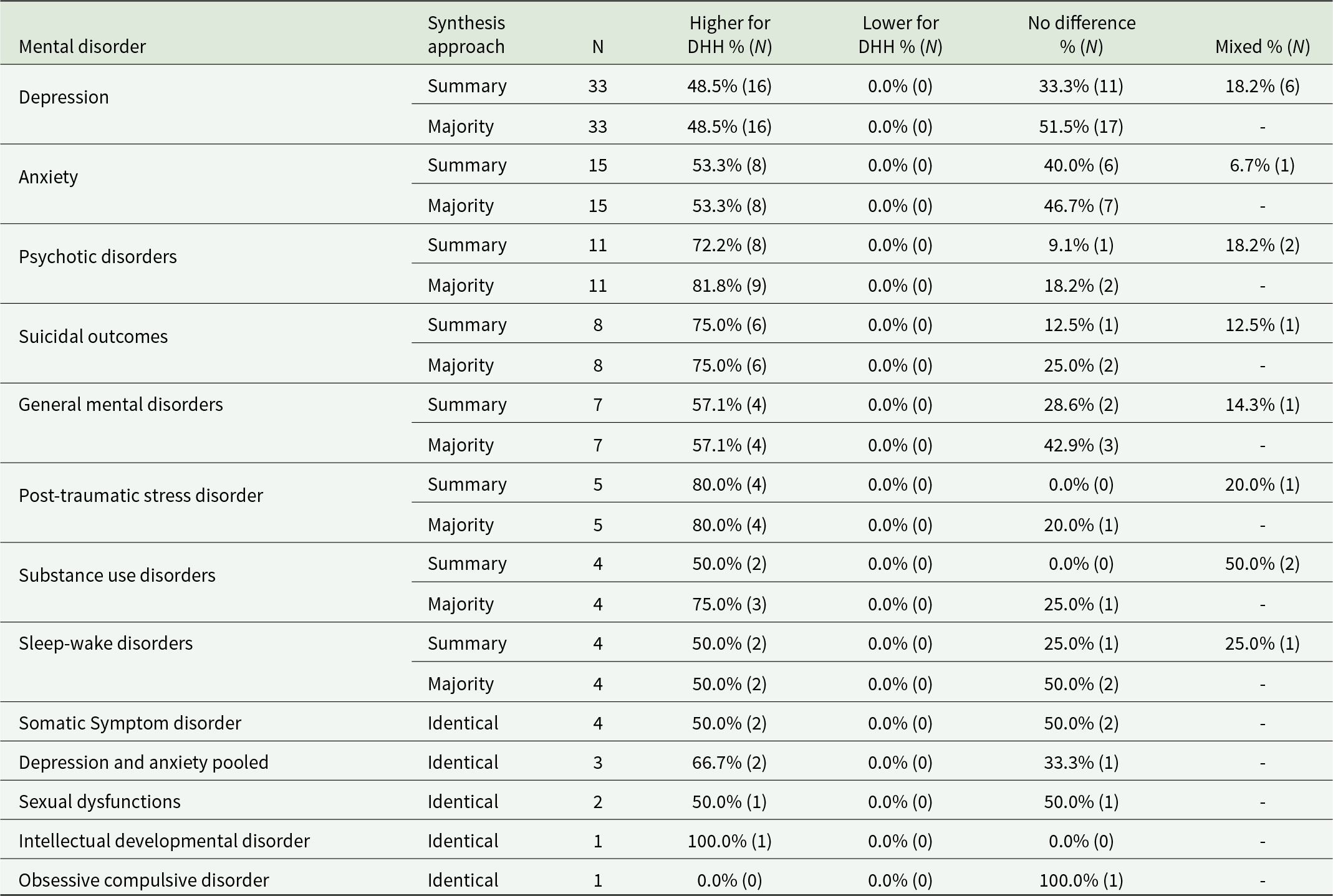
Note: Results are aggregated at the study level; N = number of studies; Identical = Summary and Majority effect directions were the same (i.e., no mixed findings were present within the study); Equal findings studies regarded as no difference per outcome in the majority-direction synthesis: Depression (N = 2), General mental disorders (N = 1), Post traumatic stress disorder (N = 1), Substance use disorders (N = 1).
Other disorders were examined in fewer than five studies each, including somatic symptom disorder, substance use disorders, and sleep–wake disorders (4 studies each), depression and anxiety pooled (3 studies), sexual dysfunctions (2 studies), and intellectual developmental disorder and obsessive compulsive disorder (1 each). For most disorders, the predominant effect was higher mental disorder outcomes for DHH, followed by no difference. Consistent with all earlier syntheses, no disorder-specific synthesis showed lower aggregated mental disorder outcomes for DHH.
Discussion
In this systematic review covering 60 studies, we aimed to synthesise the existing evidence for differences in mental disorder prevalence, incidence, or severity between DHH and hearing adults aged 18 to 60. Most studies (58.3%–65.0%) reported higher mental disorder outcomes for DHH adults, while the remaining studies primarily reported no differences. Notably, not a single study showed lower mental disorder outcomes for DHH in any synthesis approach. These patterns were consistent across prevalence and severity outcomes. Only two studies examined incidence, both finding no group differences in the majority-direction synthesis. In studies with lower risk of bias, around 60% reported higher mental disorder outcomes for DHH adults, compared to around 70% in higher-risk studies; yet both patterns broadly aligned with the overall synthesis. Results were also consistent across age groups, with approximately 60%–70% of studies reporting higher mental disorder outcomes for both younger and older DHH adults. Disorder-specific syntheses aligned with the overall synthesis, with no aggregated effect direction resulting in lower mental disorder outcomes for DHH. For the more commonly studied disorders, depression, anxiety, psychotic disorders, suicidal outcomes, general mental disorders, and post-traumatic stress disorder, the proportion of studies reporting higher mental disorder outcomes for DHH adults ranged from 48.5% for depression to 72.2%–81.8% for psychotic disorders. Other disorders, such as sleep–wake disorders and substance use disorders, were examined in fewer than five studies each, limiting the reliability of conclusions for these categories.
These findings align with previous systematic research on depression, anxiety, psychotic disorders, and general psychopathology, which also indicates a potential higher prevalence or severity of mental disorders for DHH people compared to hearing people, particularly for children, adolescents, and older adults (Theunissen et al., Reference Theunissen, Rieffe, Netten, Briaire, Soede, Schoones and Frijns2014; Linszen et al., Reference Linszen, Brouwer, Heringa and Sommer2016; Shoham et al., Reference Shoham, Lewis, Favarato and Cooper2019; Jiang et al., Reference Jiang, Kubwimana, Eaton, Kuper and Bright2020; Lawrence et al., Reference Lawrence, Jayakody, Bennett, Eikelboom, Gasson and Friedland2020; Trott et al., Reference Trott, Smith, Xiao, Veronese, Koyanagi, Jacob, Lopez-Sanchez, Barnett and Pardhan2021). Our findings indicate that elevated mental health risks are not confined to early developmental stages, but may arise or persist throughout adulthood. A separate question concerns the influence of age of onset of hearing loss. Few studies reported this information, limiting firm conclusions about its potential impact on mental health (de Graaf and Bijl, Reference de Graaf and Bijl2002; Ciesla et al., Reference Ciesla, Lewandowska and Skarzynski2016; Linszen et al., Reference Linszen, Brouwer, Heringa and Sommer2016). Still, our comparison of younger and older adult samples suggested broadly similar patterns in mental disorder outcomes. Given that the prevalence of hearing loss remains relatively stable before age 40, it is plausible that a sizeable portion of younger adults in these samples experienced earlier-onset hearing loss, which provides suggestive evidence that mental disorder outcomes are broadly similar for people with both early and later onset hearing loss (GBD 2019 Hearing Loss Collaborators, 2021; World Health Organization, 2021). However, this interpretation remains speculative and should be approached with caution.
This systematic review had several strengths. First, it addressed a key gap in the literature by focusing specifically on adults aged 18 to 60, a substantial proportion of the working-age population whose mental health is critical not only for individual well-being but also for broader societal and economic functioning (Walker et al., Reference Walker, McGee and Druss2015; Christensen et al., Reference Christensen, Lim, Saha, Plana-Ripoll, Cannon, Presley, Weye, Momen, Whiteford, Iburg and McGrath2020; Arias et al., Reference Arias, Saxena and Verguet2022). Second, it is the first to synthesise mental disorder outcomes across the full diagnostic spectrum in adults. By including studies on prevalence, incidence, and severity for a wide range of disorders, we provide a comprehensive overview of current evidence on mental health disparities between DHH and hearing adults. Third, applying two complementary synthesis approaches reduced ambiguity from within-study variation. Finally, Subgroup analyses by outcome type, risk of bias, and age enabled a more nuanced understanding of how patterns vary across methodological approaches and subgroups.
This systematic review also has some limitations. First, there was considerable heterogeneity between studies, including differences in study design, exposure and outcome measurement, and control for confounding. Many studies relied on non-validated, single-item self-report measures of hearing loss, often lacking detail on severity or laterality, possibly leading to misclassification (Tremblay et al. Reference Tremblay, Pinto, Fischer, Klein, Klein, Levy, Tweed and Cruickshanks2015; Musiek et al. Reference Musiek, Shinn, Chermak and Bamiou2017; World Health Organization, 2021). Second, over three quarter of the studies were conducted in North America and Europe, potentially limiting generalisability to global DHH populations. Third, age of onset of hearing loss was rarely reported, restricting direct examination of whether early or late onset DHH may explain differences in mental disorder outcomes. Fourth, a proportion of studies reported no statistically significant group differences, yet many of these studies had small sample sizes or many subgroup analyses, thereby increasing the risk of Type II error. These findings should therefore be interpreted with caution, as the absence of detected differences may reflect limited statistical power rather than a true absence of disparities.
Given the findings, several recommendations can be made for future research, policy, and practice. First, differences in mental disorder outcomes between DHH and hearing people remain unknown for many disorders. For example, differences in eating disorders and personality disorders have not been studied, and several others (e.g., OCD, sleep-wake disorders) have only been minimally explored. These gaps need to be filled, as understanding the full scope of mental health disparities across all mental disorders is crucial to ensuring comprehensive care and targeted prevention efforts for the DHH population. Secondly, future research could benefit from employing longitudinal and population-based designs to better track mental health trajectories over time. Additionally, quasi-experimental approaches, such as matching studies, can help improve causal inference by accounting for confounding factors. Thirdly, sample diversity and representativeness should be prioritised, as key DHH characteristics (e.g., degree of hearing loss, language preference, age of onset, type of education) are rarely reported, limiting the generalisability of findings. Finally, there is an urgent need for mental health intervention research. Only a few RCTs have been conducted to date, primarily in children or older adults, leaving working-age DHH adults underrepresented (Trott et al., Reference Trott, Koblitz and Pardhan2025). Future interventions, such as psychotherapy, should be accessible, culturally and linguistically appropriate, and developed in collaboration with the DHH community (Fellinger et al., Reference Fellinger, Holzinger and Pollard2012; James et al., Reference James, Argenyi, Guardino, McKee, Wilson, Sullivan, Griest Schwartzman and Anderson2022a).
In terms of policy and practice, our findings highlight the importance of ensuring adequate and equitable access to mental health care for DHH adults, who may face more elevated risks for mental disorders. Yet, significant barriers remain, including communication challenges, cultural mismatches, and stigma, which often hinder access to appropriate care (Kuenburg et al., Reference Kuenburg, Fellinger and Fellinger2016; Mousley and Chaudoir, Reference Mousley and Chaudoir2018; James et al., Reference James, Coady, Stacciarini, McKee, Phillips, Maruca and Cheong2022b). To address these issues, mental health services ought to be adapted to better meet the needs of DHH adults through more accessible, culturally sensitive, and linguistically appropriate approaches (Sheppard, Reference Sheppard2014; Kuenburg et al., Reference Kuenburg, Fellinger and Fellinger2016; James et al., Reference James, Coady, Stacciarini, McKee, Phillips, Maruca and Cheong2022b). In addition, routine screening for symptoms of mental disorders should be implemented during healthcare encounters, including in settings where hearing loss is assessed, to ensure not only identification of those with elevated symptoms, but also early identification of those at elevated risk (Sheppard, Reference Sheppard2014; Dethmers et al., Reference Dethmers, Knoors, Vissers, van Gelder and Hermans2025). But, without integrated and inclusive support, the mental health needs of DHH adults will continue to go unmet (World Health Organization, 2021). Policies should therefore prioritise investment in tailored, evidence-informed services that are co-designed with DHH communities.
To conclude, this review shows that the majority of the current evidence indicates higher prevalence or severity of mental disorders for DHH adults aged 18–60 years compared to hearing adults, while evidence on incidence remains too limited to draw firm conclusions. Notably, none of the aggregated findings suggested lower mental disorder outcomes for DHH adults. Addressing these persistent disparities will require intervention research, along with more population-based, longitudinal and quasi-experimental designs, incorporating comprehensive reporting of participant characteristics. This would substantially advance understanding, support the development of tailored interventions, and ultimately contribute to improved mental health and quality of life for DHH adults.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S2045796026100511
Availability of data and materials
All data and information supporting this study are presented in the main text, tables and supplementary materials. Additional information can be requested from the corresponding author (n.de.ponti@vu.nl).
Acknowledgements
During the preparation of this manuscript, the first author used ChatGPT for language editing and refinement to enhance clarity and readability. All authors subsequently reviewed and revised the content and take full responsibility for the final version of the publication.
Financial support
This work was funded by a grant from ZonMw, represented by Deelkracht (Grant number: 10840302210002).
Competing interests
The authors declare no competing interests.
Ethical standards
Not applicable to this study.






 Open access
Open access