


Anxiety disorders are a heterogeneous group of conditions characterised by excessive fear, anxiety and associated behavioural disturbances. They have among the highest prevalence rates of all psychiatric disorders worldwide. The DSM-5-TR recognises seven primary anxiety disorders: generalised anxiety disorder (GAD), panic disorder, agoraphobia, specific phobia, social anxiety disorder (SAD), separation anxiety disorder and selective mutism. This editorial reviews the development of anxiolytic medications, that is, agents used to treat symptoms of anxiety or specific anxiety disorders. Psychological interventions are first-line treatments for mild to moderate anxiety disorders but are outside the remit of this paper. Many patients with moderate to severe anxiety disorders respond best to combined psychological and pharmacological treatment.
History of anxiolytics
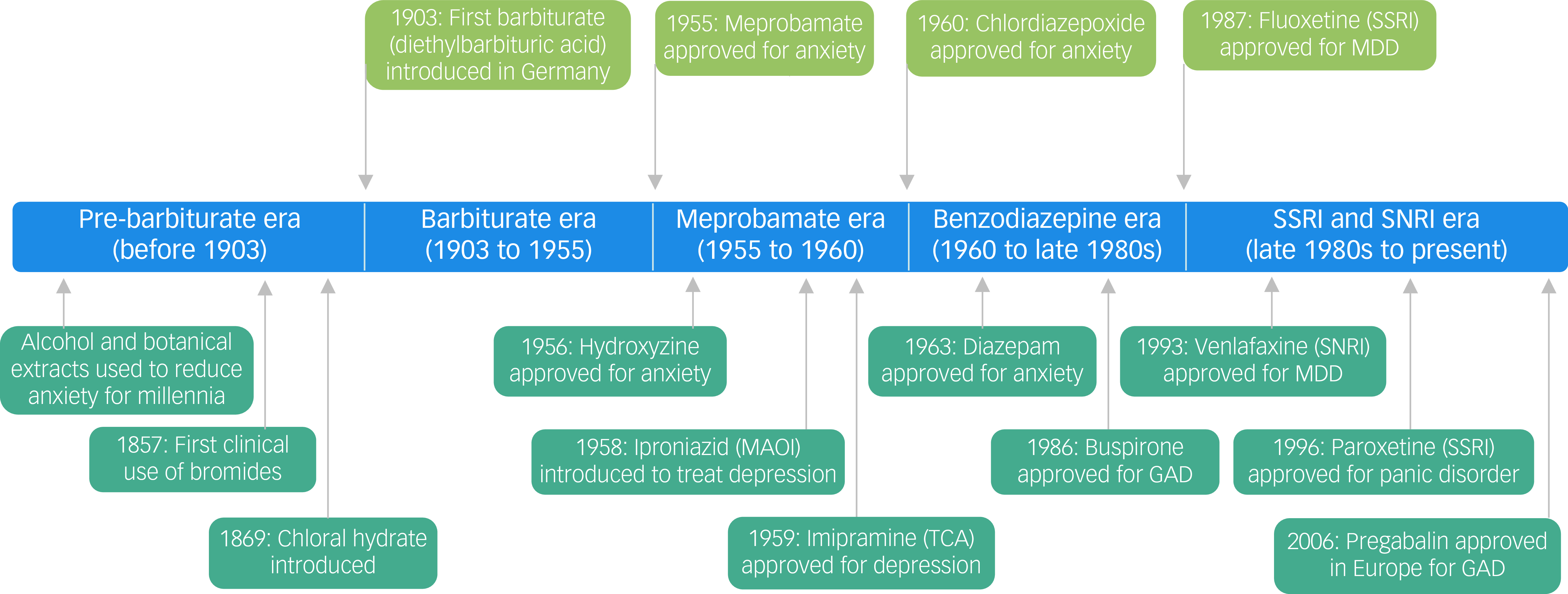
The history of anxiolytic drugs can be viewed as a series of eras defined by the dominant agents of the time (Fig. 1).
Key milestones in the history of anxiolytic drugs (unless otherwise indicated, the year indicates when the drug received FDA approval). FDA, Food and Drug Administration; GAD, generalised anxiety disorder; MAOI, monoamine oxidase inhibitor; MDD, major depressive disorder; SNRI, selective serotonin and noradrenaline reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic antidepressant.

The pre-barbiturate era (before 1903)
For millennia, naturally occurring sedative–hypnotics, including alcohol, opium and cannabis, have been used to relieve symptoms of anxiety. Bromide salts were first used clinically in 1857 for their sedative effects. However, chloral hydrate, introduced in 1869, is generally regarded as the first synthetic organic sedative–hypnotic to enter clinical practice. Paraldehyde followed in the early 1880s. Chloral hydrate was associated with dependence, whereas bromides had long elimination half-lives (9–12 days), which could lead to accumulation and toxicity (‘bromism’). Recognition of these problems was delayed.
The barbiturate era (1903 to 1955)
In 1902, German chemists Emil Fischer and Joseph von Mering synthesised the first barbiturate, diethylbarbituric acid (barbital). It was marketed in 1903 under the brand name Veronal. More than 50 barbiturates entered clinical practice. Barbiturates were widely used as sedatives and hypnotics in the first half of the 20th century. Their narrow therapeutic index resulted in a high risk of fatal overdose. Case reports of barbiturate dependence and withdrawal appeared in American medical journals in the 1920s, but widespread clinical and public health recognition did not occur until the 1950s.
The meprobamate era (1955 to 1960)
Meprobamate (Miltown) is neither a barbiturate nor a benzodiazepine. It was approved by the U.S. Food and Drug Administration (FDA) in 1955 and was the first drug marketed as a ‘tranquilliser’ to treat anxiety. It was promoted as less sedating than barbiturates but shared many of their adverse effects, including a substantial misuse and dependence potential and a high risk of fatal overdose. Meprobamate became the first psychiatric ‘blockbuster’ drug and by 1957 was the fastest-growing medication in history. Its success paved the way for the development and marketing of the benzodiazepines.
The benzodiazepine era (1960 to late 1980s)
Chlordiazepoxide (Librium), the first benzodiazepine, was synthesised by Leo Sternbach in 1955 and entered clinical use in 1960. Other benzodiazepines followed, including diazepam (Valium) in 1963 and alprazolam (Xanax) in 1981. Benzodiazepines vary in potency and half-life and in their indications, which include treatment of anxiety, insomnia, seizures and alcohol withdrawal. They rapidly replaced barbiturates and meprobamate as they were less sedating and carried a markedly lower risk of fatal overdose. Use peaked in the mid-1970s, when they were among the most widely prescribed psychotropic agents worldwide. Barbiturates, meprobamate and benzodiazepines have the same anxiolytic mechanism, acting as positive allosteric modulators of the γ-aminobutyric acid subtype A (GABAA) receptor. The narrower therapeutic index of barbiturates reflects their additional ability to directly activate the GABAA receptor at high concentrations.
Dependence and withdrawal were reported soon after benzodiazepines entered clinical use, but the full extent of these was only recognised years later. In 1988, the UK’s Committee on Safety of Medicines highlighted these risks and recommended that benzodiazepines only be used for short-term treatment of anxiety (2–4 weeks).1 Other drawbacks include cognitive and psychomotor impairment. Despite their limitations, benzodiazepines remain valuable for short-term management of severe anxiety.Reference Baldwin, Aitchison, Bateson, Curran, Davies and Leonard2
The 1950s saw the first tricyclic antidepressants (TCAs) and monoamine oxidase inhibitors (MAOIs) introduced to treat depression. Certain TCAs and MAOIs are effective in some anxiety disorders, but both classes are limited by side-effects. MAOIs also require dietary restrictions.
The SSRI and SNRI era (late 1980s to the present)
DSM-III (1980) introduced operational criteria for discrete anxiety disorders, replacing earlier, less specific classifications and profoundly influencing anxiolytic research and drug licensing. The advent of selective serotonin reuptake inhibitors (SSRIs) and serotonin–noradrenaline reuptake inhibitors (SNRIs) marked a major milestone in anxiety treatment, offering a lower side-effect burden compared with TCAs and MAOIs and more robust evidence of efficacy. The FDA approval of fluoxetine in 1987 is widely regarded as marking the start of the SSRI era. Venlafaxine, approved in 1993, was the first SNRI.
All SSRIs and SNRIs were initially approved for the treatment of major depressive disorder. In 1996, paroxetine became the first SSRI to receive FDA approval for an anxiety disorder (panic disorder). Extended-release venlafaxine (venlafaxine XR) became the first SNRI with FDA approval for an anxiety disorder (GAD) in 1999. Since then, various SSRIs and SNRIs have gained approval for GAD, panic disorder and SAD, with indications varying by drug and country.
Most authorities, including the UK Committee on Safety of Medicines,Reference Weller, Ashby, Chambers, Chick, Drummond and Ebmeier3 do not regard SSRIs and other antidepressants as being associated with a dependence syndrome. However, antidepressants can cause withdrawal symptoms, which are usually mild and self-limiting but can be severe in a minority of patients, making discontinuation difficult.Reference Henssler, Schmidt, Schmidt, Schwarzer, Bschor and Baethge4 Other limitations of SSRIs and SNRIs include delayed onset of therapeutic effect, initial anxiety and sexual dysfunction.
Current pharmacological treatments
SSRIs and SNRIs remain first-line pharmacological treatments for a broad range of anxiety disorders.Reference Baldwin, Anderson, Nutt, Allgulander, Bandelow and den Boer5 Buspirone, a serotonin 1A (5-HT1A) receptor partial agonist with no sedative or dependence potential, was approved by the FDA for GAD in 1986. Pregabalin (Lyrica), a gabapentinoid, was approved in Europe for GAD in 2006. It reduces calcium influx at presynaptic nerve terminals, which reduces release of the excitatory neurotransmitter glutamate. Although pregabalin was initially considered to have a low risk of misuse, post-marketing experience revealed significant misuse and dependence liability, leading to tighter prescribing controls. Pregabalin is the drug most recently approved by the European Medicines Agency (EMA) for an anxiety disorder, whereas the last FDA-approved treatment was the SNRI duloxetine for GAD, approved in 2007.
Some, but not all, anxiolytic drugs demonstrate efficacy across several anxiety disorders. For example, paroxetine and venlafaxine XR have FDA and EMA approvals for GAD, panic disorder and SAD.Reference Baldwin, Anderson, Nutt, Allgulander, Bandelow and den Boer5 By contrast, buspirone is only approved for GAD, with clinical trials showing a lack of efficacy in SAD and panic disorder.Reference Baldwin, Anderson, Nutt, Allgulander, Bandelow and den Boer5
Off-label medications are often used to treat anxiety disorders when approved first-line agents are ineffective or unsuitable. Examples include second-generation antipsychotics (SGAs), beta-blockers, antidepressants outside the SSRI and SNRI classes (e.g. agomelatine and mirtazapine) and first-generation antihistamines (H1 receptor antagonists), although hydroxyzine has FDA approval for anxiety. Among the SGAs, low-dose quetiapine has the most robust evidence for efficacy in GAD, but side-effects include sedation and weight gain.Reference Slee, Nazareth, Bondaronek, Liu, Cheng and Freemantle6 No SGA is currently approved by either the FDA or EMA for any anxiety disorder.
Beta-blockers, particularly propranolol, are widely prescribed off-label for anxiety disorders but have limited evidence of efficacy. They are effective for performance-only SAD, reducing peripheral autonomic symptoms, but are not effective for generalised SAD, panic disorder or GAD.
Acute-phase trials dominate the evidence base for pharmacological treatment of anxiety disorders. Although clinical guidelines recommend continuation of agents with demonstrated maintenance efficacy to reduce relapse risk, there is no clear consensus on the optimal duration. Recommendations generally include at least 6 months of medication after remission, but longer treatment may be appropriate, with decisions to continue or taper being individualised and based on patient factors and tolerability.Reference Baldwin, Anderson, Nutt, Allgulander, Bandelow and den Boer5 Further research is needed to define optimal long-term strategies for specific agents.
Drugs in development
In the past decade, anxiolytic research has expanded beyond conventional treatment paradigms, exploring both novel targets and innovative approaches to established neurotransmitter systems. Investigational compounds include neuropeptide modulators (e.g. corticotropin-releasing factor antagonists and oxytocin agonists), endocannabinoid system modulators, neuroactive steroids and glutamatergic agents (e.g. ketamine).Reference Garakani, Murrough, Freire, Thom, Larkin and Buono7 Despite this diversification, many clinical trials have yielded negative or inconclusive results. Two areas with potential are PH94B and psychedelic-assisted psychotherapies.
PH94B is a neuroactive steroid that is administered as a nasal spray and is currently undergoing phase 3 trials as an ‘as-needed’ (p.r.n.) anxiolytic for SAD, targeting situational anxiety (e.g. public speaking). It exerts its effects via activation of nasal chemosensory neurons leading to modulation of limbic circuits.
The strongest evidence for psychedelics in treating anxiety disorders relates to anxiety associated with life-threatening illness (e.g. cancer), although research is also addressing GAD and SAD. Preliminary findings suggest that psychedelic-assisted therapies may be effective in patients with treatment-resistant anxiety, as well as having a relatively rapid onset of action and producing sustained effects after only a small number of administrations. However, much of the evidence remains of low or very low certainty owing to small sample sizes, risk of bias and challenges with blinding in trials.Reference Højlund, Kafali, Kırmızı, Fusar-Poli, Correll and Cortese8 No psychedelic is currently approved by the EMA or FDA for any psychiatric indication.
Psychedelics are thought to reduce anxiety partly by enhancing structural and functional neural plasticity in circuits involved in threat processing and emotional regulation. Classic serotonergic psychedelics, such as psilocybin and LSD (lysergic acid diethylamide), are 5-HT2A receptor agonists. Their action is believed to activate downstream cortical signalling pathways that enhance psychological flexibility and reduce anxiety. By contrast, MDMA (3,4-methylenedioxymethamphetamine) increases synaptic release of serotonin, noradrenaline, dopamine and oxytocin. These changes are thought to contribute to reduced defensiveness and increased feelings of safety.
A meta-analysis found that both serotonergic psychedelics and MDMA reduced anxiety symptoms in patients with anxiety disorders, with serotonergic psychedelics also improving quality of life.Reference Højlund, Kafali, Kırmızı, Fusar-Poli, Correll and Cortese8 In a phase 2 trial, a single dose of an LSD formulation (MM120) produced a dose-dependent reduction in anxiety in adults with moderate-to-severe GAD at 4 weeks.Reference Robison, Barrow, Conant, Foster, Freedman and Jacobsen9 This result prompted the FDA to grant the compound ‘breakthrough therapy’ designation for GAD.
In addition to research involving emerging compounds, other strategies are being explored to revitalise drug development across psychiatry. These include stratified biomarker-driven approaches, high-throughput screening, drug repurposing, computational modelling, and artificial-intelligence-driven drug discovery.
Themes and future outlook
Several themes emerge from the history of anxiolytic drug development. Approved agents act via diverse mechanisms, including GABAergic, serotonergic and noradrenergic mechanisms, whereas investigational compounds also target additional systems. This suggests that anxiety arises from dysregulation across multiple overlapping neural circuits rather than a single pathway. The variable efficacy of anxiolytics across specific anxiety disorders further indicates distinct yet partially overlapping pathophysiological processes.
Some anxiolytics carry risks of dependence and misuse, whereas others do not. Agents not associated with these risks include buspirone, hydroxyzine and antidepressants across multiple classes. The delayed recognition of dependence with older drugs (barbiturates, meprobamate and benzodiazepines) reflected several factors at the time, including less stringent drug approval systems, limited post-marketing surveillance and an incomplete understanding of dependence. Today, pre-approval assessment of misuse and dependence potential is required for central nervous system-active drugs. The delay in recognising the misuse and dependence liability of pregabalin illustrates that some risks may only emerge with wider clinical use. These examples underscore the importance of both rigorous pre-approval evaluation and post-marketing surveillance in ensuring drug safety.
The blockbuster status of meprobamate, diazepam and SSRIs indicates a substantial public demand for anxiolytic medications. This demand needs to be balanced with appropriate prescribing and education for both the public and healthcare professionals, as some drug classes have historically been overused in the treatment of anxiety disorders. Psychological interventions, particularly cognitive–behavioural therapy, are recommended as first-line treatments for mild to moderate anxiety disorders, as they provide efficacy comparable with that of pharmacotherapy but with a more favourable risk–benefit profile.
Anxiety disorders are highly prevalent and disabling, yet current pharmacological treatments have limited efficacy and significant side-effects. Anxiolytic drug development has largely stalled over the past two decades, with no new approvals in Europe or the USA for nearly 20 years, reflecting a mismatch between clinical need and therapeutic innovation. This stagnation extends across much of psychiatry and partly reflects incomplete understanding of disease mechanisms. Despite this, a range of agents for anxiety disorders are in development, reflecting diversification of therapeutic approaches. Psychedelic-assisted therapies are of particular interest and show preliminary promise. New treatments are needed to reduce disability and improve quality of life.
Funding
This study received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
P.M.H. has received a lecture fee from Lundbeck and is a member of the British Journal of Psychiatry editorial board but did not take part in the review or decision-making process for this paper.

eLetters
No eLetters have been published for this article.