


Introduction
Tetralogy of Fallot is the most common cyanotic congenital cardiac malformation. As an obstructed right ventricular outflow tract is one of the phenotypic features of the lesion, diagnostic evaluation, and clinical decision making often focuses on its different aspects. The one of the most frequently discussed is the size of the so-called valvar “annulus”. Reference Choi, Sung and Kim1–Reference Kasturi, Balaji and Sudhakar6 Other features have been less well discussed or studied. Of those that have been conducted, a high prevalence has been noted of valves having two leaflets, with this feature also associated with worse clinical outcomes. Reference Altrichter, Olson, Edwards, Puga and Danielson7,Reference Liu, Jiang and Peng8 We primarily aimed to characterise the number of leaflets in the pulmonary valve in the setting of tetralogy of Fallot. Secondary aims were to assess other aspects of pulmonary valve morphology.
Methods
Study aims
Our primary aim was to quantify the number of leaflets in the pulmonary valve in the setting of tetralogy of Fallot. Our secondary aims were to assess the leaflet morphology relative to the number of pulmonary valvar sinuses, to assess whether there was evidence of fusion of leaflets, and to describe the direction of the zone of apposition between those hearts with valves having only two leaflets.
Institutional review board approval was waived for this study as there are no patient identifying data utilised.
Heart specimens
We examined the hearts stored in the cardiac registries at Advocate Children’s Hospital, Ann & Robert H. Lurie Children’s Hospital, Johns Hopkins All Children’s Hospital, and the Van Mierop Archive at the University of Florida. All hearts had been preserved in 10% formalin.
Inclusion criteria
We reviewed only hearts with the accepted phenotypic features of tetralogy of Fallot, namely an outlet interventricular communication opening to the right ventricle between the cranial and caudal limbs of the septomarginal trabeculation, pulmonary stenosis produced by the squeeze between the deviated outlet septum and the septoparietal trabeculations, and an overriding aorta. Reference Jacobs, Franklin and Beland9,Reference Jacobs, Franklin and Beland10 We excluded any hearts with pulmonary atresia, along with those in which it provided impossible to assess the anatomy because of previous catheter-based or surgical interventions.
Characteristics of the pulmonary valve (Figure 1)
Inspection of the valve was focused initially on the number of valvar leaflets. We then assessed the number of valvar sinuses supporting the leaflets, combining this with inspection for the presence of any fusion between the leaflets. Fusion was classified as being present or absent. In those valves having two leaflets, we then determined the direction of the zone of apposition between them. This was described either as pointing towards the aorta, or not. When describing the findings, we followed the concepts as used in the recent consensus statement regarding the anatomy, imaging, and nomenclature of the aortic valve. Reference Tretter, Spicer and Franklin11 In brief, we considered the pulmonary root as a three-dimensional structure extending from its virtual basal ring proximally to the sinutubular junction distally. Within the root, the individual valvar leaflets were considered to be supported by the valvar sinuses, usually but not always in semilunar fashion. Individual sinuses were recognised as being separated by interleaflet triangles, which when fully formed extended to the sinutubular junction. The virtual basal ring as defined is not a true anatomic structure, but rather a geometric entity. It is often described by echocardiographers as the valvar “annulus”. It is distinct from the myocardial-arterial junction, which is found at the bases of all sinuses of the pulmonary root (Figure 2).
The drawings show the morphologies noted in the three clusters that resulted from the cluster analysis. The double line outlines the zones of apposition. A dashed line represents fusion of the leaflets. Panel a shows a three-leaflet pulmonary valve with three sinuses and no fusion of leaflets. Panel B is a two-leaflet pulmonary valve with two sinuses and no fusion of leaflets. Panel C is a two-leaflet pulmonary valve with three sinuses and fusion of leaflets.

The upper panel, an intact normal pulmonary valve, shows the virtual basal ring (green dots) created at the nadir of the leaflets. The valvar leaflets are attached in semilunar fashion reaching the sinutubular junction (black dots), with red lines marking the interleaflet triangles between the leaflets. In the lower panel, the leaflets have been removed to demonstrate the myocardial-arterial junction (red dots) between the wall of the infundibulum and the fibrocollagenous wall of the pulmonary trunk. A crescent of myocardium is incorporated into each of the valvar sinsuses. The sinutubular junction (black dots) and the virtual basal ring (green dots) are illustrated.

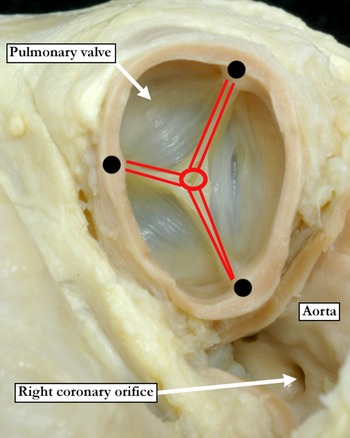
When considered in three dimensions, as with the aortic root, the pulmonary root has an overall crown-like configuration. In the normal root, the crown has three peaks, which can be appreciated during diastole as the distal attachments of the leaflets at the sinutubular junction. These areas are described conventionally as the commissures. The zones of apposition, where the leaflets interface with one another, extend radially from the commissures to the centre of the valvar orifice (Figure 3). In describing our current findings, we have purposely avoided using the term “cusp”. This is because the word is currently used in variable fashion, referring to either the leaflets or the sinuses or sometimes even a combination of both leaflets and sinuses.
This short-axis view of the normal pulmonary valve within the base of the heart shows the valvar attachments (black dots) at the sinutubular junction typically referred to as the commissures. The zones of apposition where one leaflet interfaces with another leaflet (red lines) extend radially from the commissures to the centre of the valvar orifice (red circle).

Statistical analyses
Cluster analysis was performed, using a two-step K-cluster approach, to assess whether the findings segregated into statistically significant groups. The Akaike information criterion was used to determine the optimal number of clusters, noting the characteristics of each cluster. The Akaike information criterion was used as it provides a numeric value that allows for comparison of models, it is associated with lower overfitting and results in fewer but larger clusters.
All other statistical analyses were done using SPSS Version 29.0. A p-value of less than 0.05 was considered statistically significant.
Results
Characteristics of the pulmonary valve
In 97 (63%) of the hearts, the pulmonary valve had two leaflets, whether leaflet fusion resulted in two functional units, or two leaflets were present without leaflet fusion. In 54 (34%), there were three leaflets. A valve with one leaflet, with fusion between all three leaflets and a central orifice, was found in 4 (3%) hearts. Some fusion between the leaflets was found in 44 (28%) hearts. In terms of the sinuses, a trisinuate arrangement was found in 96 (62%) hearts, with a bisinuate arrangement found in 55 hearts (36%). In 3 hearts (2%), we found only one identifiable sinus. When considering the 97 hearts with valves having two leaflets, we observed some degree of fusion between the leaflets in 42 (43%). In 71 of these hearts (73%), the zone of apposition between the leaflets was pointing towards the aorta. In terms of the sinuses, 43 hearts (44%) had three sinuses, with 54 (56%) having only two sinuses. The various combinations of leaflets and sinuses within the roots are summarised in Figure 4.
The diagram shows the breakdown of the number of specimens with various number of leaflets and sinuses. Absolute counts and frequencies are presented. The percentages are based on a denominator one level above in the tree.

Supplemental file 1 contains links to three-dimensional models of heart specimens included in the analyses made from scans produced using a Revopoint Miraco scanner.
Cluster analysis
Using our selected system, we identified three clusters, with the quality of clustering, at 0.80, indicating good statistical discrimination. The most important predictor in differentiating the clusters was the direction of the zone of apposition, with predictive importance of 1.0. With a predictive importance of 0.93, the second most important feature was the number of valvar leaflets, followed by the presence of fusion between the leaflets, with a predictive importance of 0.87. The number of valvar sinuses achieved a predictive importance of 0.83. In Figure 4, we show the different valvar morphologies across our three identified clusters.
The largest cluster contained 61 (40%) of the hearts. In this cluster, with 93% of the hearts having bileaflet valves, 90% also had only two sinuses, with 85% having a zone of apposition pointing towards the aorta. Only 5% of the hearts in this cluster showed any evidence of fusion between the leaflets. This cluster, therefore, was characterised by a bileaflet and bisinuate root, with no leaflet fusion, and a zone of apposition pointing towards the aorta (Figure 5).
Supported by a stenotic subpulmonary infundibulum, the specimen has a pulmonary root made up of two leaflets and two valvar sinuses. There are only two well-formed interleaflet triangles.

The second largest cluster contained 53 (34%) of the hearts. In this cluster, all the hearts had a three-leaflet valve with three sinuses, three distinct zones of apposition, and no fusion between pulmonary valve leaflets (Figure 6).
This pulmonary valve is extremely stenotic and thickened, with three leaflets and three sinuses. The leaflets are fused along the zones of apposition towards the commissures (black dots) leaving a central, tiny opening and a dome-shaped functionally unileaflet valve.

The smallest cluster contained 40 (26%) of the hearts. In this cluster, 57% of the hearts had a zone of apposition pointing towards the aorta, with all hearts having three sinuses, two functional leaflets, with evidence of fusion in one of the functional leaflets (Figure 7).
This pulmonary valve has functionally two leaflets and three sinuses, with only two normally formed interleaflet triangles extending to the sinutubular junction (black dotted line). The third interleaflet triangle is incomplete and rudimentary, resulting from fusion of the valvar leaflets and formation of a raphe (red arrows) that incompletely divides two of the valvar sinuses.

Discussion
Our retrospective study of hearts with tetralogy of Fallot stored in historical archives has shown that the majority have two-leaflet pulmonary valves. Most commonly this occurs in the setting of a bisinuate root without leaflet fusion, with a smaller proportion possessing a functionally bileaflet valve housed within a trisinuate pulmonary root. When seeking to segregate the hearts using cluster analysis, we were able, with good statistical significance, to identify three basic patterns. The largest group was made up of hearts with bisinuate and bileaflet valves. The second group was made up of hearts with trisinuate and trifoliate valves, whilst the smallest group had functional bifoliate valves in a trisinuate root. Previous studies have shown that it is the rule for the hypoplastic pulmonary root in the setting of tetralogy of Fallot to be guarded by a valve with less than three functional leaflets. In one study, just under three-fifths of the cohort were found to have two-leaflet valves. Reference Altrichter, Olson, Edwards, Puga and Danielson7 In another study, using intraoperative inspection, found almost nine-tenths of the roots to have only one or two leaflets. Reference Liu, Jiang and Peng8 Neither of these studies, however, nor any other studies of which we are aware, sought to further clarify the morphology of the abnormal roots in terms of the number of valvar sinuses.
Our current study used specimens from historical archives, which made it impossible for us to make clinical correlations. In this regard, as far as we can establish, it is only the study using intraoperative inspection that has provided such correlations. Reference Liu, Jiang and Peng8 These investigators found that those with other than trisinuate and trileaflet valves were more likely to have lower preoperative arterial saturations, smaller diameters of the virtual basal ring, and greater preoperative right ventricular outflow tract obstruction. The patients, furthermore, were less likely to get a valvar-sparing repair, and more likely to require pulmonary arterioplasty, left pulmonary arterioplasty, and valvar annuloplasty. They also tended to have a longer postoperative duration of mechanical ventilation, and longer postoperative stay in the intensive care unit. In longer-term follow-up, they were also more likely to require reintervention. These findings stress the ongoing need to establish precise valvar morphology during the preoperative work-up. Our findings now indicate that, in addition to the number of functional leaflets, attention is also required regarding the number of valvar sinuses. As we have emphasised, little attention seems to have been paid thus far to the number of sinuses within the hypoplastic pulmonary root.
We have previously demonstrated that, during its development, the outflow tract is best analysed as having distal, middle, and proximal parts. These give rise, respectively, to the intrapericardial arterial trunks, the arterial roots, and the ventricular outflow tracts. Reference Anderson, Lamers and Hikspoors12,Reference Henderson, Eley and Chaudhry13 The components of the aortic and pulmonary valves, therefore, form within the middle part of the developing outflow tract. In the early stages of development, the outflow tract has walls that are exclusively myocardial, and the lumen is lined with cardiac jelly. It is with ongoing development that new non-myocardial cells are added to the outflow tract from the second heart field. With this addition of new material, there is effective proximal regression of the myocardial borders, with the distal myocardium then surrounding the developing arterial roots. At the same time, the initially common lumen is separated into the aortic and pulmonary channels by fusion of the outflow cushions, which extend in a spiralling fashion through the parts of the tract that have retained their myocardial walls. The cushions fuse from distal to proximal, eventually producing complete physical separation of the systemic and pulmonary channels. Reference Anderson, Lamers and Hikspoors12 The distal surfaces of the fused major cushions also excavate so as to produce the valvar leaflets. These components interdigitate with similar excavating aortic and pulmonary intercalated swellings, thus producing two primordiums, each with a trileaflet pattern. Addition of non-myocardial tissues derived from the second heart field then produces the walls of the valvar sinuses. By then, the proximal major cushions have united and muscularised, building a shelf in the roof of the right ventricle so as to commit the aortic root to the developing left ventricle. Tubercles from the atrioventricular cushions then close the persisting aortic-right ventricular communication, producing what will become the membranous part of the septum. At this stage, both the pulmonary and aortic valvar leaflets remain supported entirely by myocardial tissue. It only after the completion of ventricular septation that the inner heart curve within the left ventricle undergoes fibrous conversion, thus producing fibrous continuity between the leaflets of the mitral and aortic valves. Reference Anderson, Lamers and Hikspoors12
On the basis of our knowledge of normal development as described above, we can now infer that tetralogy of Fallot, along with double outlet right ventricle with subaortic interventricular communication and pulmonary stenosis, is the result of incomplete transfer of the developing aortic root to the left ventricle. This is likely the consequence of an abnormal cranial location of the septal attachment of the proximal cushions, which at the same time narrows the subpulmonary outflow tract. This makes it impossible for the tubercles of the atrioventricular cushions to close the aorto-right ventricular communication. As we have also described, the pulmonary and aortic valves form similarly to one another. Their right and left leaflets, along with the septal leaflets of the atrioventricular valves, are derived from the endocardial cushions. Their nonadjacent leaflets, however, are derived from the intercalated valve swellings, sometimes referred to as the intercalated cushions. Reference Henderson, Eley and Chaudhry13 Thus, the leaflets themselves of each valve are not derived from structures with the same developmental origin. Although the intercalated valve swellings eventually appear similar to the endocardial cushions, they are different at a cellular level. Despite these differences, both the leaflets derived from the cushions, and those formed from the intercalated valve swellings, enlarge into the lumen of the developing outflow tracts and ensure one-way flow in the separate outflow tracts. Reference Nomura-Kitabayashi, Phoon and Kishigami14 Through flow-triggered mechanisms yet to be fully delimited, the endocardial cushions and the intercalated valve swellings become smaller, producing the leaflets in a complex process of valvar sculpting. This involves a process of excavation, with the leaflets never “elongating”, as suggested by current conventional wisdom. With the added information of the cellular mechanisms involved, Reference Henderson, Eley and Chaudhry13,Reference Nomura-Kitabayashi, Phoon and Kishigami14 we can now make additional inference regarding the appearance of the different abnormalities we have observed. Presence of only two leaflets in the pulmonary root could imply failure of formation of the pulmonary intercalated valvar swelling. Such a mechanism would account for the commonest pattern we encountered, namely the bisinuate and bileaflet pulmonary root. The findings in the hearts with bileaflet but trisinuate roots imply fusion between the cushions during ongoing development, as would be the case for those having valves with only one leaflet and a central orifice. The varying orientation of the zone of apposition between the leaflets is likely to reflect the specific cushions undergoing fusion.
Clinically, the findings of this study can have clinical implications. This has been highlighted by the study by Liu and colleagues who demonstrated that the presence of an abnormal pulmonary valve was associated with lower preoperative arterial saturations and higher preoperative right ventricular outflow tract gradients. Abnormal pulmonary valves were also associated with increased likelihood of requiring a main pulmonary arterioplasty and left pulmonary arterioplasty. Those with abnormal pulmonary valves were also less likely to undergo a valve sparing repair and undergoing a transannular patch. The findings of the current study may also be associated with similar clinical approaches although this was not investigated in this study. Additional studies applying these criteria to children with tetralogy of Fallot undergoing surgical repair would be of clinical utility. Interest to the surgical technique associated with clusters as well as the future need for reintervention would be of clinical interest.
The features of interest included in this study are able to be assessed by echocardiography. Right ventricular outflow tract dimensions, pulmonary valve leaflet number, and pulmonary valve sinus number can all be assessed with echocardiography. CT can also demonstrate all these features with even greater detail.
We emphasise that our study has been made possible only by access to specimens from historical archives. The use of such specimens has permitted us to make an efficient and thorough evaluation of the overall morphology of the pulmonary root. Thus far, there is a paucity of published data regarding the overall characteristics of the pulmonary root in tetralogy of Fallot, despite it being a major driver of clinical decision-making. In particular, this study highlights the importance of the zones of apposition, pulmonary valve leaflet number, and pulmonary valve sinus number. Clinical evaluation now makes use not only of echocardiography, but increasingly CT and MRI. With care, all of the features we have identified should now be evident to those using these clinical techniques. Thus far, it has been metrics of the so-called pulmonary valvar “annulus”, in reality the virtual basal ring, that have been used to drive decision-making. Our study now provides evidence that other more specific features of the pulmonary root should be taken into consideration. We accept, nonetheless, that whilst our study offers novel data, it has its limitations. It was limited by the availability of specimens in the registries. There may also have been underlying bias in that all our patients had died. Thus, clinically milder phenotypes may not be well represented. This latter fact may well have influenced the proportions of hearts making up our clusters. The specific patterns we have identified, nonetheless, may have clinical significance. Only careful analysis in the clinical setting will show whether this is, indeed, the case. Additionally, it should be mentioned that the ability to discern clinical features is easier when examining a specimen versus examining a heart in situ using echocardiography, However, with the technological and the technical advances in echocardiography, the valve features discussed here should be able to be reproduced echocardiographically. Advanced imaging modalities such as computed tomography can also be utilised.
Conclusion
In two-thirds of our hearts with tetralogy of Fallot, the pulmonary valve had two leaflets. Most frequently, there were three sinuses. In the setting of a valve with two sinuses, the zone of apposition between the leaflets pointing towards the aorta. Cluster analysis permitted statistically sound segregation of the heart and highlights the importance of delineating these features, specifically the leaflet and sinus morphology, with clinical imaging.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951125001398.









 Open access
Open access